Food Addiction, Binge Eating Disorder, and Obesity: Is There a Relationship?



Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Participants
3.2. Food Addiction and Binge Eating
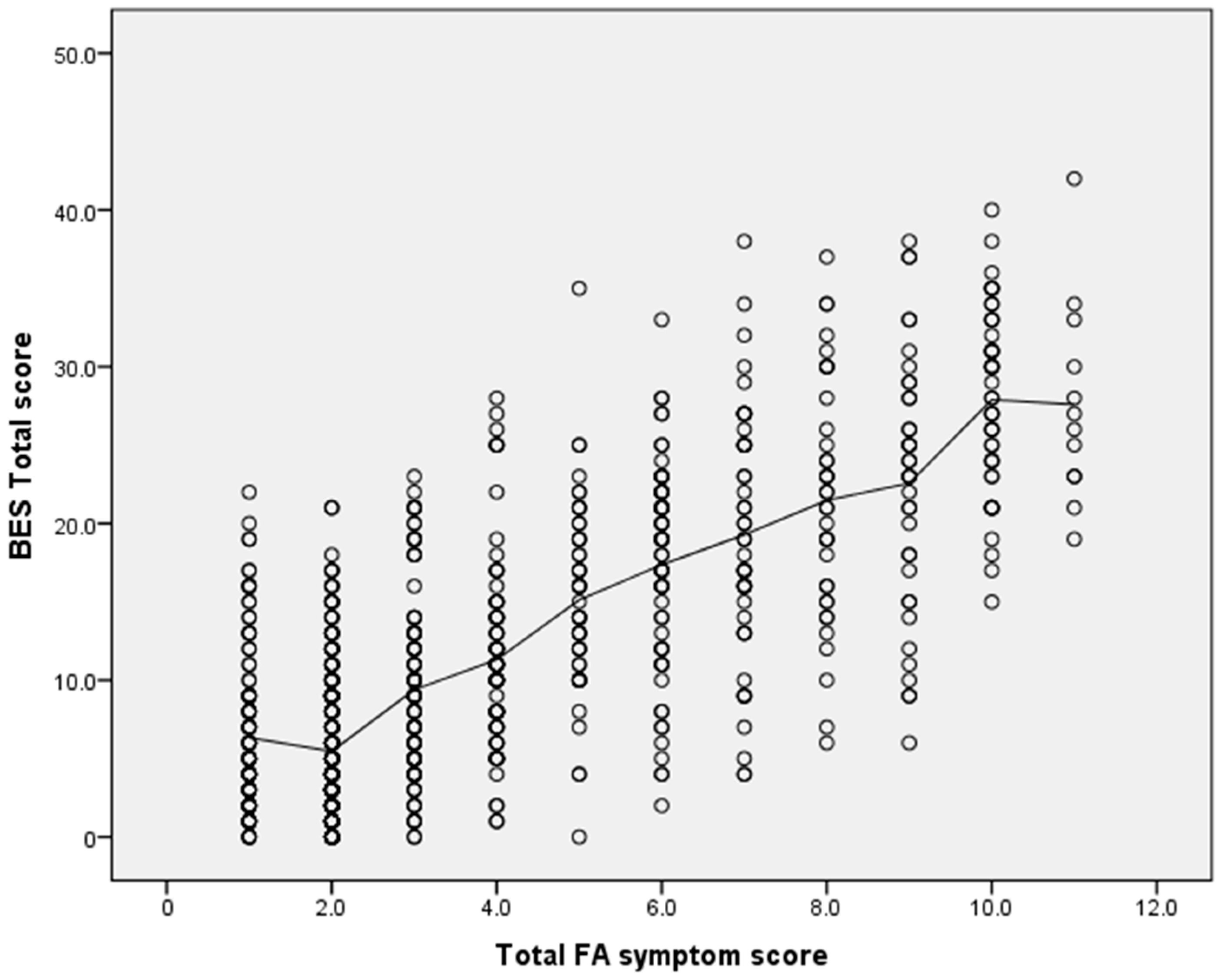
3.3. Relationships between Food Addiction and Binge Eating
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Pursey, K.M.; Stanwell, P.; Gearhardt, A.N.; Collins, C.E.; Burrows, T.L. The Prevalence of Food Addiction as Assessed by the Yale Food Addiction Scale: A Systematic Review. Nutrients 2014, 6, 4552–4590. [Google Scholar] [CrossRef] [PubMed]
- Hebebrand, J.; Albayrak, Ö.; Adan, R.; Antel, J.; Dieguez, C.; de Jong, J.; Leng, G.; Menzies, J.; Mercer, J.G.; Murphy, M.; et al. “Eating addcition” rather than “food addcition” better captures addictive like eating behaviour. Neurosci. Biobehav. Rev. 2014, 47, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.; Corbin, W.; Brownwell, K.D. Preliminary validation of the Yale Food Addiction Scale. Appetite 2009, 52, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N; Corbin, W.R; Brownwell, K.D. Development of the Yale Food Addiction Scale Version 2.0. Psychol. Addict. Behav. 2016, 30, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Davis, C. From Passive Overeating to “Food Addiction”: A Spectrum of Compulsion and Severity. ISRN Obes. 2013, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Schulte, E.M.; Grilo, C.M.; Gearhardt, A.N. Shared and unique mechanisms underlying binge eating disorder and addictive disorders. Clin. Psychol. Rev. 2016, 44, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Hilker, I.; Sánchez, I.; Steward, T.; Jiménez-Murcia, S.; Granero, R.; Gearhardt, A.N.; Rodríguez-Muñoz, R.C.; Dieguez, C.; Crujeiras, A.B.; Tolosa-Sola, I.; et al. Food Addiction in Bulimia Nervosa: Clinical Correlates and Association with Response to a Brief Psychoeducational Intervention. Eur. Eat. Disord. Rev. 2016, 24, 482–488. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, TX, USA, 2013. [Google Scholar]
- Kessler, R.; Berglund, P.A.; Chiu, W.T.; Deitz, A.C.; Hudson, J.I.; Shahly, V.; Aguilar-Gaxiola, S.; Alonso, J.; Angermeyer, M.C.; Benjet, C.; Bruffaerts, R.; et al. The Prevalence and Correlates of Binge Eating Disorder in the World Health Organization World Mental Health Surveys. Biol. Psychiatry 2013, 73, 904–914. [Google Scholar] [CrossRef] [PubMed]
- Preti, A.; de Girolamo, G.; Vilagut, G.; Alonso, J.; de Graaf, R.; Bruffaerts, R.; Demyttenaere, K.; Pinto-Meza, A.; Haro, J.M.; Morosini, P.; et al. The epidemiology of eating disorders in six European countries: Results of the ESEMeD-WMH project RSS. J. Psychiatr. Res. 2009, 43, 1125–1132. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; White, M.A.; Masheb, R.M.; Morgan, P.T.; Crosby, R.D.; Grilo, C.M. An Examination of the food addcition construct in obese patients with binge eating disorder. Int. J. Eat. Disord. 2012, 45, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.; White, M.A.; Masheb, R.M.; Grilo, C.M. An examination of food addiction in a racially diverse sample of obese patients with binge eating disorder in primary care settings. Compr. Psychiatr. 2013, 54, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; Boswell, R.G.; White, M.A. The association of “food addiction” with disordered eating and body mass index. Eat. Behav. 2014, 15, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; von Rezori, V.; Blechert, J. Food addiction and bulimia nervosa. Eur. Eat. Disord. Rev. 2014, 5, 33. [Google Scholar] [CrossRef] [PubMed]
- Burrows, T.; Hides, L.; Brown, R.; Dayas, C.V.; Kay-Lambkin, F. Differences in Dietary Preferences, Personality and Mental Health in Australian Adults with and without Food Addiction. Nutrients 2017, 9, 285. [Google Scholar] [CrossRef] [PubMed]
- Heatherton, T.; Baumeister, R. Binge eating as escape from self-awareness. Psychol. Bull. 1991, 110, 86–108. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.; White, M.; Potenza, M. Binge Eating Disorder and Food Addiction. Curr. Drug Abuse Rev. 2011, 43, 201–207. [Google Scholar] [CrossRef]
- Potenza, M.N.; Grilo, C.M. How relevant is food craving to obesity and its treatment? Front. Psychiatry 2014, 5, 164. [Google Scholar] [CrossRef] [PubMed]
- Pivarunas, B.; Conner, B.T. Impulsivity and emotion dysregulation as predictors of food addiction. Eat. Behav. 2015, 19, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Clark, S.; Saules, K. Validation of the yale Food Addiction Scale among a weight loss surgery population. Eat. Behav. 2013, 14, 216–219. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; Heckel, D. Correlates of food addiction in obese individuals seeking bariatric surgery. Clin. Obes. 2014, 4, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Davis, C. A commentary on the associations among ‘food addiction’, binge eating disorder, and obesity: Overlapping conditions with idiosyncratic clinical features. Appetite 2017, 115, 3–8. [Google Scholar] [CrossRef] [PubMed]
- WHO (The World Health Organisation). BMI Classifcation. Available online: http://apps.who.int/bmi/index.jsp?introPage=intro_3.htm (accessed on 25 July 2017).
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The assessment of Binge Eating Severity among obese. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef]
- Kelly, N.R.; Mitchell, K.S.; Gow, R.W.; Trace, S.E.; Lydecker, J.A.; Bair, C.E.; Mazzeo, S. An evaluation of the reliability and construct validity of eating disorder measures in white and black women. Psychol. Assess. 2012, 24, 608–617. [Google Scholar] [CrossRef] [PubMed]
- Grupski, A.E.; Hood, M.M.; Hall, B.J.; Azarbad, L.; Fitzpatrick, S.L.; Corsica, J.A. Examining the binge eating scale in screening for binge eating disorder with bariatric surgery candidates. Obes. Surg. 2013, 23, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Santor, D.A.; Haggerty, J.L.; Lévesque, J.-F.; Burge, F.; Beaulieu, M.-D.; Gass, D.; Pineault, R. An Overview of Confirmatory Factor Analysis and Item Response Analysis Applied to Instruments to Evaluate Primary Healthcare. Healthc. Policy 2011, 7, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Brunault, P.; Courtois, R.; Gearhardt, A.N.; Gaillard, P.; Journiac, K.; Cathelain, S.; Réveillère, C.; Ballon, N. Validation of the French Version of the DSM-5 Yale Food Addiction Scale in a Nonclinical Sample. Can. J. Psychiatry 2017, 62, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Imperatori, C.; Fabbricatore, M.; Vumbaca, V.; Innamorati, M.; Contardi, A.; Farina, B. Food Addiction: definition, measurement and prevalence in healthy subjects and in patients with eating disorders. Riv. Psichiatr. 2016, 51, 60–65. [Google Scholar] [PubMed]
- Kittel, R.; Brauhardt, A.; Hilbert, A. Hilbert A. Cognitive and emotional functioning in binge-eating disorder: A systematic review. Int. J. Eat. Disord. 2015, 48, 535–554. [Google Scholar] [CrossRef] [PubMed]
- Hauck, C.; Weiß, A.; Schulte, E.M.; Meule, A.; Ellrott, T. Prevalence of ‘Food Addiction’ as Measured with the Yale Food Addiction Scale 2.0 in a Representative German Sample and Its Association with Sex, Age and Weight Categories. Eur. J. Obes 2017, 10, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; Gearhardt, A.N. Food addiction in the light of DSM-5. Nutrients 2014, 6, 3653–3671. [Google Scholar] [CrossRef] [PubMed]
- Ruddock, H.; Hardman, C. Food Addiction Beliefs Amongst the Lay Public: What Are the Consequences for Eating Behaviour? Curr. Addict. Rep. 2017, 4, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Ivezaj, V.; White, M.A.; Grilo, C.M. Examining binge-eating disorder and food addiction in adults with overweight and obesity. Obesity 2016, 24, 2064–2069. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.Y.; Sayed, A.M.; Alshahat, A.A.; Abd Elaziza, E.A. Can food addiction replace binge eating assessment in obesity clinics? Egypt. J. Med. Hum. Genet. 2017, 18, 181–185. [Google Scholar] [CrossRef]
- Long, C.; Blundell, J.; Finlayson, G. A Systematic Review of the Application and Correlates of YFAS-Diagnosed ‘Food Addiction’ in Humans: Are Eating-Related ‘Addictions’ a Cause for Concern or Empty Concepts? Obes. Facts 2015, 8, 386–401. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.M.; Hutson, P.H.; Herman, B.K.; Potenza, M.N. The neurobiological basis of binge-eating disorder. Neurosci. Biobehav. Rev. 2016, 63, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; Yokum, S.; Orr, P.T.; Stice, E.; Corbin, W.R.; Brownell, K.D. Neural correlates of food addiction. Arch. Gen. Psychiatry 2011, 68, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Schrieber, L.; Odlaug, B.; Grant, J. The overlap between binge eating disorder and substance use disorders: Diagnosis and neurobiology. J. Behav. Addict. 2013, 2, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Pursey, K.; Burrows, T.L.; Stanwell, P.; Collins, C.E. How accurate is web-based self-reported height, weight and body mass index in young adults? J. Med. Internet Res. 2014, 16, e4. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographic | NFA Male (n = 176 ) | FA Male (n = 27 ) | p Value | NFA Female (n = 624 ) | FA Female (n = 201 ) | p Value |
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| Age (years) | 42.0 ± 13.2 | 46.0 ± 16.4 | 0.531 | 39.6 ± 13.1 | 40.1 ± 13.0 | 0.407 |
| Height (cm) | 178.8 ± 0.1 | 179.7 ± 0.1 | 0.629 | 166.0 ± 0.1 | 165.9 ± 0.1 | 0.935 |
| Weight (kg) | 87.4 ± 15.4 | 113.7 ± 28.3 | <0.01 | 70.0 ± 16.7 | 88.4 ± 22.9 | <0.01 |
| BMI * (kg/m2) | 27.4 ± 4.8 | 35.4 ± 8.8 | <0.01 | 25.5 ± 6.0 | 32.7 ± 13.1 | <0.01 |
| n = 149 | n = 22 | n = 517 | n = 183 | |||
| BES total | 7.4 ± 5.8 | 20.1 ± 6.1 | <0.01 | 8.5 ± 6.5 | 22.8 ± 8.1 | <0.01 |
| Condition | Underweight (n = 14 ) | Healthy (n = 439 ) | Overweight (n = 263 ) | Obese (n = 286 ) | p Value |
|---|---|---|---|---|---|
| Food Addiction (FA) | % | % | % | % | |
| NFA | 85.7 | 92.5 | 78.7 | 53.8 | <0.001 |
| Mild FA | 0.0 | 0.9 | 0.4 | 0.7 | 0.368 |
| Moderate FA | 7.1 | 1.6 | 3.4 | 3.5 | 0.07 |
| Severe FA | 7.1 | 5.0 | 17.5 | 42.0 | <0.001 |
| Binge Eating (BE) | |||||
| Non-bingeing | 90.0 | 89.3 | 74.8 | 50.6 | <0.001 |
| Moderate | 10.0 | 7.5 | 19.5 | 30.4 | <0.001 |
| Severe | 0.0 | 3.2 | 5.8 | 19.0 | <0.001 |
| Condition | NFA (n = 666 ) | FA (n = 205) | p Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| BES total | 8.23 ± 6.35 | 22.56 ± 7.93 | <0.001 |
| BES emotions | 4.05 ± 3.71 | 12.76 ± 4.44 | <0.001 |
| BES behaviours | 4.72 ± 3.66 | 11.56 ± 4.75 | <0.001 |
| % | % | ||
| Non-bingeing | 90.1 | 27.3 | <0.001 |
| Moderate bingeing | 9.0 | 41.0 | 0.046 |
| Severe bingeing | 0.9 | 31.7 | <0.001 |
| Total | 100.0 | 100.0 |
| Measure | BES Total | BES Emotions | BES Behaviours |
|---|---|---|---|
| Binge Eating | |||
| 1. BES total | - | ||
| 2. BES emotions | 0.95 *** | - | |
| 3. BES behaviours | 0.96 *** | 0.82 *** | - |
| Food Addiction | |||
| 4. Total FA symptoms | 0.76 *** | 0.75 *** | 0.71 *** |
| 5. Consumed more than planned | 0.24 *** | 0.21 *** | 0.25 *** |
| 6. Unable to cut down or stop | 0.61 *** | 0.62 *** | 0.55 *** |
| 7. Great deal of time spent | 0.58 *** | 0.55 *** | 0.56 *** |
| 8. Activities given up or reduced | 0.61 *** | 0.61 *** | 0.56 *** |
| 9. Continued use despite physical/emotional consequences | 0.67 *** | 0.67 *** | 0.60 *** |
| 10. Tolerance | 0.54 *** | 0.54 *** | 0.50 *** |
| 11. Withdrawal | 0.52 *** | 0.52 *** | 0.48 *** |
| 12. Continued use despite social consequences | 0.52 *** | 0.51 *** | 0.48 *** |
| 13. Fail to fulfil roles and obligations | 0.53 *** | 0.53 *** | 0.48 *** |
| 14. Use in physically hazardous situations | −0.49 *** | −0.50 *** | −0.44 *** |
| 15. Craving | 0.65 *** | 0.64 *** | 0.59 *** |
| 16. Impairment or distress | 0.68 *** | 0.70 *** | 0.61 *** |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burrows, T.; Skinner, J.; McKenna, R.; Rollo, M. Food Addiction, Binge Eating Disorder, and Obesity: Is There a Relationship? Behav. Sci. 2017, 7, 54. https://doi.org/10.3390/bs7030054
Burrows T, Skinner J, McKenna R, Rollo M. Food Addiction, Binge Eating Disorder, and Obesity: Is There a Relationship? Behavioral Sciences. 2017; 7(3):54. https://doi.org/10.3390/bs7030054
Chicago/Turabian StyleBurrows, Tracy, Janelle Skinner, Rebecca McKenna, and Megan Rollo. 2017. "Food Addiction, Binge Eating Disorder, and Obesity: Is There a Relationship?" Behavioral Sciences 7, no. 3: 54. https://doi.org/10.3390/bs7030054
APA StyleBurrows, T., Skinner, J., McKenna, R., & Rollo, M. (2017). Food Addiction, Binge Eating Disorder, and Obesity: Is There a Relationship? Behavioral Sciences, 7(3), 54. https://doi.org/10.3390/bs7030054