
“We Dance and Find Each Other”1: Effects of Dance/Movement Therapy on Negative Symptoms in Autism Spectrum Disorder

Abstract
:1. Introduction
1.1. The Development of Social Cognition
1.2. Social Cognition in Autism Spectrum Disorder
1.3. An Embodied Approach to Autism Spectrum Disorder
1.4. Embodied Approaches to Autism Therapy
2. Materials and Methods
2.1. Study Design
2.2. Recruitment Procedure and Randomization
2.3. Intervention
2.4. Clinical Assessment
2.5. Sample
2.6. Statistical Analysis
2.6.1. Missing Data
2.6.2. Main Analysis
3. Results
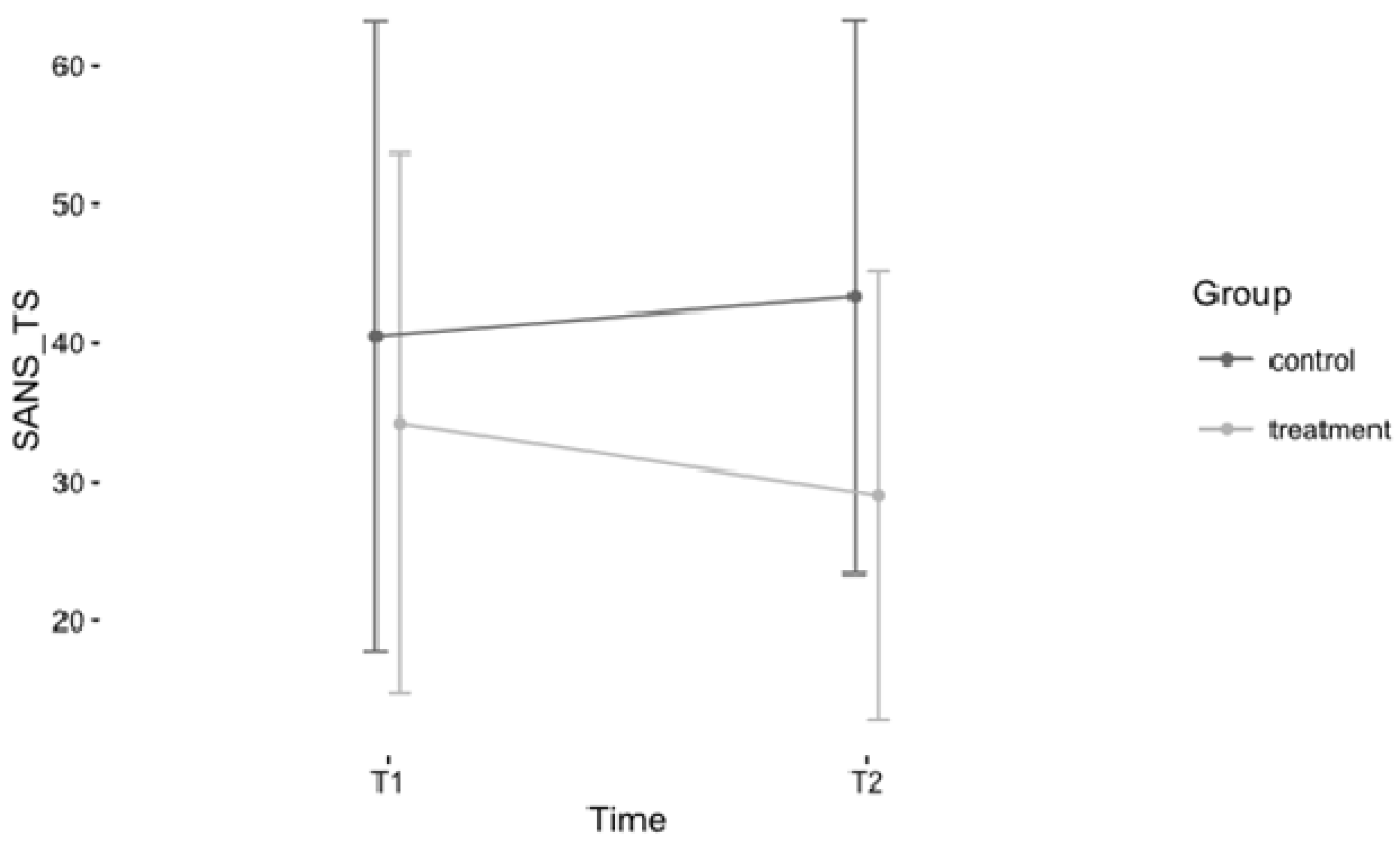
3.1. Changes in Severity of Overall Negative Symptoms
3.2. Changes in Severity of Subdomains
4. Discussion
4.1. Changes in Severity of Negative Symptoms
4.2. Limitations and Further Directions
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A
- We dance
- Everything is dance,
- so one says.
- Even atoms
- swing and dance.
- Electrons circle around protons and neutrons.
- Everything swings, all is in harmony.
- Only this way
- the world is kept in an equilibrium
- It is an ancient law.
- And we also
- circle around each other in our dance.
- We dance,
- and the music animates us
- We dance,
- and the rhythms permeates us
- We dance,
- and find each other.
- We dance,
- and are joyful.
- We laugh and dance.
- We dance and are
- …free!
Note: A line of this poem was used in the title of the paper. The participant translated the German version of her poem into English herself. The poem was the result of a voluntary session assignment to the group of participants to reflect their experience in dance movement therapy (DMT) in another art medium, and bring it with them to the last session. The poem is a reprinted from the article “Fixing the mirrors” by Koch et al.[35]
Appendix B

{kind=link}
Intro/Warm-up (approx. 10 min):
| Aim: “Setting the stage”
|
Dyadic mirroring (approx. 15 min):
| Aim: Emotional empathy and interactional reciprocity through nonverbal dyadic sharing.
|
Baum-circle (approx. 25 min):
| Aim: Emotional empathy and improved expression through nonverbal sharing in the group.
|
Verbal processing (approx. 5–10 min *):
| Aim: Empathic emotion (and cognition/perspective taking) and improved expression/interaction through verbal sharing with the group.
|
Appendix C
| Outcome/Time | Treatment NS (T1 = 43; T2 = 30) NA (T1 = 45; T2 = 41) | Control NS (T1 = 21; T2 = 19) NA (T1 = 15; T2 = 20) | ||||||
|---|---|---|---|---|---|---|---|---|
| MS | SDS | MA | SDA | MS | SDS | MA | SDA | |
| SANS-TS | ||||||||
| T1 | 28.72 | 16.06 | 33.51 | 19.27 | 17.48 | 12.92 | 37.93 | 20.89 |
| T2 | 22.37 | 12.11 | 28.37 | 15.63 | 25.16 | 14.43 | 37.45 | 18.94 |
| (1) SANS-BA | ||||||||
| T1 | 9.44 | 6.14 | 13.60 | 7.47 | 5.43 | 7.26 | 12.93 | 9.15 |
| T2 | 7.19 | 5.27 | 9.78 | 6.36 | 8.26 | 5.14 | 12.65 | 9.15 |
| (2) SANS-Al | ||||||||
| T1 | 3.00 | 3.29 | 3.87 | 3.72 | 1.43 | 1.86 | 5.27 | 4.70 |
| T2 | 2.25 | 2.63 | 3.63 | 3.52 | 2.21 | 3.24 | 5.00 | 4.41 |
| (3) SANS-Ab | ||||||||
| T1 | 5.05 | 3.50 | 4.09 | 3.53 | 4.43 | 3.17 | 5.53 | 4.16 |
| T2 | 3.84 | 2.41 | 3.80 | 3.45 | 5.16 | 4.32 | 5.25 | 4.29 |
| (4) SANS-Anh | ||||||||
| T1 | 6.88 | 5.31 | 8.67 | 5.14 | 3.81 | 3.23 | 9.13 | 5.60 |
| T2 | 5.88 | 3.82 | 7.66 | 4.41 | 5.84 | 4.54 | 9.80 | 3.94 |
| (5) SANS-Att | ||||||||
| T1 | 4.35 | 2.84 | 3.73 | 2.96 | 2.38 | 2.13 | 5.07 | 3.26 |
| T2 | 2.63 | 2.43 | 3.49 | 2.98 | 3.68 | 3.30 | 4.75 | 2.79 |
References
- Sheitman, B.B.; Kraus, J.E.; Bodfish, J.W.; Carmel, H. Are the negative symptoms of schizophrenia consistent with an autistic spectrum illness? Schizophr. Res. 2004, 69, 119–120. [Google Scholar] [CrossRef]
- Liemburg, E.; Castelein, S.; Stewart, R.; van der Gaag, M.; Aleman, A.; Knegtering, H.; Genetic Risk and Outcome of Psychosis (GROUP) Investigators. Two subdomains of negative symptoms in psychotic disorders: Established and confirmed in two large cohorts. J. Psychiatr. Res. 2013, 47, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Konstantareas, M.M.; Hewitt, T. Autistic disorder and schizophrenia: Diagnostic overlaps. J. Autism Dev. Disord. 2001, 31, 19–28. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Kirkpatrick, B.; Fenton, W.S.; Carpenter, J.W.T.; Marder, S.R. The nimh-matrics consensus statement on negative symptoms. Schizophr. Bull. 2006, 32, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Hyman, S.L.; Levy, S.E. Autistic spectrum disorders: When traditional medicine is not enough. Contemp. Pediatr. 2000, 17, 101–116. [Google Scholar]
- Fombonne, E. Modern views of autism. Can. J. Psychiatry 2003, 48, 503–505. [Google Scholar] [PubMed]
- Gallagher, S.; Varga, S. Conceptual issues in autism spectrum disorders. Curr. Opin. Psychiatry 2015, 28, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Spaulding, S. Embodied cognition and theory of mind. In The Routledge Handbook of Embodied Cognition; Shapiro, L., Ed.; Routledge/Taylor & Francis Group: New York, NY, USA, 2014; pp. 197–206. [Google Scholar]
- Buccino, G.; Amore, M. Mirror neurons and the understanding of behavioural symptoms in psychiatric disorders. Curr. Opin. Psychiatry 2008, 21, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Gallese, V.; Sinigaglia, C. What is so special about embodied simulation? Trends Cognit. Sci. 2011, 15, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Eigsti, I.-M. A review of embodiment in autism spectrum disorders. Front. Psychol. 2013, 4. [Google Scholar] [CrossRef] [PubMed]
- Théoret, H.; Halligan, E.; Kobayashi, M.; Fregni, F.; Tager-Flusberg, H.; Pascual-Leone, A. Impaired motor facilitation during action observation in individuals with autism spectrum disorder. Curr. Biol. 2005, 15, R84–R85. [Google Scholar] [CrossRef] [PubMed]
- Nishitani, N.; Avikainen, S.; Hari, R. Abnormal imitation-related cortical activation sequences in asperger’s syndrome. Ann. Neurol. 2004, 55, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Belmonte, M.K.; Allen, G.; Beckel-Mitchener, A.; Boulanger, L.M.; Carper, R.A.; Webb, S.J. Autism and abnormal development of brain connectivity. J. Neurosci. 2004, 24, 9228–9231. [Google Scholar] [CrossRef] [PubMed]
- Sutera, S.; Pandey, J.; Esser, E.L.; Rosenthal, M.A.; Wilson, L.B.; Barton, M.; Green, J.; Hodgson, S.; Robins, D.L.; Dumont-Mathieu, T.; et al. Predictors of optimal outcome in toddlers diagnosed with autism spectrum disorders. J. Autism Dev. Disord. 2007, 37, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Conson, M.; Mazzarella, E.; Esposito, D.; Grossi, D.; Marino, N.; Massagli, A.; Frolli, A. ‘Put myself into your place’: Embodied simulation and perspective taking in autism spectrum disorders. Autism Res. 2015, 8, 454–466. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T. Corporealized and disembodied minds: A phenomenological view of the body in melancholia and schizophrenia. Philos. Psychiatry Psychol. 2005, 12, 95–107. [Google Scholar]
- Gallagher, S. Understanding interpersonal problems in autism: Interaction theory as an alternative to theory of mind. Philos. Psychiatry Psychol. 2004, 11, 199–217. [Google Scholar] [CrossRef]
- De Jaegher, H. Embodiment and sense-making in autism. Front. Integr. Neurosci. 2013, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T. Pathologies of intersubjectivity in autism and schizophrenia. J. Conscious. Stud. 2015, 22, 191–214. [Google Scholar]
- Mundy, P.; Gwaltney, M.; Henderson, H. Self-referenced processing, neurodevelopment and joint attention in autism. Autism 2010, 14, 408–429. [Google Scholar] [CrossRef] [PubMed]
- Eberhard-Kaechele, M. Von der ko-regulation zur selbstregulation: Spiegelungsphänomene in der tanz-und ausdruckstherapie (from co-regulation to self-regulation. Mirroring in dance and expressive therapy). In Körper—Gefühl—Denken. Körperpsychotherapie und Selbstregulation (Body-Feeling-Thinking. Body Psychotherapy and Self-Regulation); Thiele, M., Ed.; Psychosozial-Verlag: Gießen, Germany, 2009; pp. 251–264. [Google Scholar]
- Eberhard-Kaechele, M. Body memory, metaphor, and mirroring in movement therapy with trauma patients. In Body Memory, Metaphor and Movement; Koch, S.C., Fuchs, T., Summa, M., Ladewig, S., Müller, C., Eds.; John Benjamins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Shai, D.; Belsky, J. When words just won’t do: Introducing parental embodied mentalizing. Child Dev. Perspect. 2011, 5, 173–180. [Google Scholar] [CrossRef]
- Fuchs, T.; Schlimme, J.E. Embodiment and psychopathology: A phenomenological perspective. Curr. Opin. Psychiatry 2009, 22, 570–575. [Google Scholar] [CrossRef] [PubMed]
- Weber, C.M. Tanz- und Musiktherapie zur Behandlung Autistischer Störungen; Verl. für Angewandte Psychologie: Göttingen, Germany, 1999. [Google Scholar]
- Scharoun, S.M.; Reinders, N.J.; Bryden, P.J.; Fletcher, P.C. Dance/movement therapy as an intervention for children with autism spectrum disorders. Am. J. Dance Ther. 2014, 36, 209–228. [Google Scholar] [CrossRef]
- Baudino, L.M. Autism spectrum disorder: A case of misdiagnosis. Am. J. Dance Ther. 2010, 32, 113–129. [Google Scholar] [CrossRef]
- Devereaux, C. Moving into relationships: Dance/movement therapy with children with autism. In Play-Based Interventions for Children and Adolescents with Autism Spectrum Disorders; Gallo-Lopez, L., Rubin, L.C., Gallo-Lopez, L., Rubin, L.C., Eds.; Routledge/Taylor & Francis Group: New York, NY, USA, 2012; pp. 333–351. [Google Scholar]
- Martin, M. Moving on the spectrum: Dance/movement therapy as a potential early intervention tool for children with autism spectrum disorders. Arts Psychother. 2014, 41, 545–553. [Google Scholar] [CrossRef]
- Tortora, S. Dance/movement psychotherapy in early childhood treatment and in pediatric oncology. In The Art and Science of Dance/Movement Therapy: Life is Dance, 2nd ed.; Chaiklin, S., Wengrower, H., Chaiklin, S., Wengrower, H., Eds.; Routledge/Taylor & Francis Group: New York, NY, USA, 2016; pp. 159–181. [Google Scholar]
- Adler, J. Looking for Me. Video Documentation. 1970. Available online: www.adta.org (accessed on 20 June 2016).
- Hartshorn, K.; Olds, L.; Field, T.; Delage, J.; Cullen, C.; Escalona, A. Creative movement therapy benefits children with autism. Early Child Dev. Care 2001, 166, 1–5. [Google Scholar] [CrossRef]
- Koch, S.C.; Mehl, L.; Sobanski, E.; Sieber, M.; Fuchs, T. Fixing the mirrors: A feasibility study of the effects of dance movement therapy on young adults with autism spectrum disorder. Autism 2015, 19, 338–350. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.A.L.; Koch, S.C.; Hirjak, D.; Fuchs, T. Overcoming disembodiment: The effect of movement therapy on negative symptoms in schizophrenia—A multicenter randomized controlled trial. Front. Psychol. 2016, 7, 483. [Google Scholar] [CrossRef] [PubMed]
- Röhricht, F.; Priebe, S. Effect of body-oriented psychological therapy on negative symptoms in schizophrenia: A randomized controlled trial. Psychol. Med. 2006, 36, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Jang, S.H.; Lee, S.Y.; Hwang, K.S. Effectiveness of dance/movement therapy on affect and psychotic symptoms in patients with schizophrenia. Arts Psychother. 2015, 45, 64–68. [Google Scholar] [CrossRef]
- Sandel, S.L.; Chaiklin, S.; Lohn, A. Foundations of Dance/Movement Therapy: The Life and Work of Marian Chace; American Dance Therapy Association (ADTA): Columbia, MD, USA, 1993. [Google Scholar]
- Sandel, S.L. The process of empathic reflection in dance therapy. In Foundations of Dance/Movement Therapy: The Life and Work of Marian Chace; Sandel, S., Chaiklin, S., Lohn, A., Eds.; American Dance Therapy Association (ASDA): Columbia, MD, USA, 1993. [Google Scholar]
- Baum, E.Z. Movement therapy with multiple personality disorder patients. Dissociation Prog. Dissociative Disord. 1991, 4, 99–104. [Google Scholar]
- Andreasen, N.C. Scale for the Assessment of Negative Symptoms; University of Iowa: Iowa City, IA, USA, 1984. [Google Scholar]
- Rabany, L.; Weiser, M.; Werbeloff, N.; Levkovitz, Y. Assessment of negative symptoms and depression in schizophrenia: Revision of the sans and how it relates to the PANSS and CDSS. Schizophr. Res. 2011, 126, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ Br. Med. J. 2009, 339, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Levine, S.Z.; Leucht, S. Identifying clinically meaningful symptom response cut-off values on the sans in predominant negative symptoms. Schizophr. Res. 2013, 145, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Koch, S.C. Arts and health: Active factors of arts therapies and a theory framework of embodied aesthetics. Arts Psychother. 2016. under review. [Google Scholar]
- Wiedenhofer, S.M.; Koch, S.C. Active factors in dance movement therapy: Specifying health effects of non-goal-orientation in movement. Arts Psychother. 2016, 52, 10–23. [Google Scholar] [CrossRef]

| Variable | Demographic Data | Treatment a | Control b |
|---|---|---|---|
| Gender | Female/Male/Missing c | 9/44/2 | 3/19/1 |
| Age | Means (years)/SD | 23.07/8.54 | 21.27/5.32 |
| Treatment Place | Bruchsal | 8 (14.54%) | 0 |
| Karlsruhe | 14 (25.45%) | 4 (17.39%) | |
| Ludwigshafen | 31 (56.36%) | 18 (78.26%) | |
| Missing | 2 (3.64%) | 1 (4.35%) | |
| Nationality | German | 41 (74.55%) | 19 (82.61%) |
| German + one additional | 0 | 1 (4.35%) | |
| Other | 0 | 2 (8.7%) | |
| Missing | 14 (25.45%) | 1 (4.35%) | |
| First Language | German | 39 (70.91%) | 18 (78.26%) |
| Other | 2 (3.64%) | 4 (17.39%) | |
| Missing | 14 (25.45%) | 1 (4.35%) | |
| Education | No degree | 3 (5.45%) | 1 (4.35%) |
| Hauptschule | 9 (16.36%) | 5 (21.74%) | |
| Realschule | 7 (12.73%) | 7 (30.43%) | |
| Abitur | 6 (10.91%) | 2 (8.7%) | |
| Completed formation | 3 (5.45%) | 2 (8.7%) | |
| Completed academic studies | 2 (3.64%) | 0 | |
| Other | 10 (18.18%) | 4 (17.39%) | |
| Missing | 15 (27.27%) | 2 (8.7%) | |
| Clinical Status | Day program | 8 (14.5%) | 4 (17.39%) |
| Inpatient | 1 (1.82%) | 1 (4.35%) | |
| Outpatient | 5 (9.09%) | 1 (4.35%) | |
| Missing | 41 (74.55%) | 17 (72.91%) | |
| Relationship Status | No partner | 33 (60%) | 15 (65.22%) |
| Partner | 3 (5.45%) | 2 (8.7%) | |
| Missing | 19 (34.55%) | 6 (26.09%) | |
| Martial Status | Single | 34 (61.82%) | 18 (78.26%) |
| Wedded | 1 (1.82%) | 0 | |
| Widowed | 1 (1.82%) | 0 | |
| Divorced | 2 (3.64%) | 0 | |
| Missing | 17 (30.91%) | 5 (21.74%) | |
| Children | No children | 34 (61.82%) | 16 (69.57%) |
| Children | 2 (3.64%) | 0 | |
| Missing | 19 (34.55%) | 7 (30.43%) |
| (A) N = 78 | Time of measurement | Treatment | Control | ||||||
|---|---|---|---|---|---|---|---|---|---|
| (Maximal Value) | N | Means | SDc | N | Means | SD | |||
| SANS_TS | T1 | 45 | 33.51 | 19.27 | 15 | 37.93 | 20.89 | ||
| −120 | T2 | 41 | 28.37 | 15.63 | 20 | 37.45 | 18.94 | ||
| SANS_BA | T1 | 13.6 | 7.47 | 12.93 | 9.15 | ||||
| −35 | T2 | 9.78 | 6.36 | 12.65 | 9.15 | ||||
| SANS_Al | T1 | 3.87 | 3.72 | 5.27 | 4.7 | ||||
| −25 | T2 | 3.63 | 3.52 | 5 | 4.41 | ||||
| SANS_Ab | T1 | 4.09 | 3.53 | 5.53 | 4.16 | ||||
| −20 | T2 | 3.8 | 3.45 | 5.25 | 4.29 | ||||
| SANS_Anh | T1 | 8.67 | 5.14 | 9.13 | 5.6 | ||||
| −25 | T2 | 7.66 | 4.41 | 9.8 | 3.94 | ||||
| SANS_Att | T1 | 3.73 | 2.96 | 5.07 | 3.26 | ||||
| −15 | T2 | 3.49 | 2.98 | 4.75 | 2.79 | ||||
| (B) N = 43 | Treatment a | Control b | |||||||
| (Maximal Value) | Means | SD | Means | SD | |||||
| SANS_TS | T1 | 34.26 | 19.42 | 40.5 | 22.69 | ||||
| −120 | T2 | 29.03 | 16.2 | 43.33 | 19.92 | ||||
| SANS_BA | T1 | 13.42 | 7.44 | 14.5 | 9.51 | ||||
| −35 | T2 | 10.03 | 6.83 | 14.67 | 9.16 | ||||
| SANS_Al | T1 | 3.52 | 3.78 | 5.42 | 4.52 | ||||
| −25 | T2 | 3.48 | 3.59 | 5.75 | 4.97 | ||||
| SANS_Ab | T1 | 4.53 | 3.96 | 6.17 | 4.2 | ||||
| −20 | T2 | 3.94 | 3.44 | 7.17 | 4.37 | ||||
| SANS_Anh | T1 | 9.29 | 5.48 | 9.5 | 6.23 | ||||
| −25 | T2 | 8.13 | 4.49 | 10.75 | 4.11 | ||||
| SANS_Att | T1 | 3.52 | 2.68 | 4.92 | 3.45 | ||||
| −15 | T2 | 3.1 | 2.77 | 5 | 2.66 | ||||
| Effect | F | P | η2 |
|---|---|---|---|
| Group | 2.95 | 0.093 | 0.058 |
| Time | 2.03 | 0.162 | 0.006 |
| Group × Time | 2.99 | 0.091 | 0.009 |
| Subscore | Effect | F | P | η2 |
|---|---|---|---|---|
| (1) SANS_BA | Group | 1.42 | 0.241 | 0.027 |
| Time | 5.67 | 0.022 * | 0.023 * | |
| Group × Time | 2.51 | 0.121 | 0.010 | |
| (2) SANS_Al | Group | 2.41 | 0.128 | 0.046 |
| Time | 0.39 | 0.538 | 0.002 | |
| Group × Time | 0.00 | 0.993 | 0.000 | |
| (3) SANS_Ab | Group | 04.5 | 0.04 * | 0.077 * |
| Time | 0.06 | 0.809 | 0.000 | |
| Group × Time | 1.52 | 0.224 | 0.008 | |
| (4) SANS_Anh | Group | 0.84 | 0.365 | 0.016 |
| Time | 0.5 | 0.485 | 0.002 | |
| Group × Time | 2.44 | 0.126 | 0.012 | |
| (5) SANS_Att | Group | 4.15 | 0.048 * | 0.067 * |
| Time | 0.36 | 0.55 | 0.002 | |
| Group × Time | 0.24 | 0.629 | 0.002 |
- 1This quote stems from a poem a female participant in the group intervention wrote for the last session as a reflection of her DMT experience. The complete poem can be found in Appendix A.
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hildebrandt, M.K.; Koch, S.C.; Fuchs, T. “We Dance and Find Each Other”1: Effects of Dance/Movement Therapy on Negative Symptoms in Autism Spectrum Disorder. Behav. Sci. 2016, 6, 24. https://doi.org/10.3390/bs6040024
Hildebrandt MK, Koch SC, Fuchs T. “We Dance and Find Each Other”1: Effects of Dance/Movement Therapy on Negative Symptoms in Autism Spectrum Disorder. Behavioral Sciences. 2016; 6(4):24. https://doi.org/10.3390/bs6040024
Chicago/Turabian StyleHildebrandt, Malin K., Sabine C. Koch, and Thomas Fuchs. 2016. "“We Dance and Find Each Other”1: Effects of Dance/Movement Therapy on Negative Symptoms in Autism Spectrum Disorder" Behavioral Sciences 6, no. 4: 24. https://doi.org/10.3390/bs6040024
APA StyleHildebrandt, M. K., Koch, S. C., & Fuchs, T. (2016). “We Dance and Find Each Other”1: Effects of Dance/Movement Therapy on Negative Symptoms in Autism Spectrum Disorder. Behavioral Sciences, 6(4), 24. https://doi.org/10.3390/bs6040024