
The Impact of Childhood Emotional Abuse and Experiential Avoidance on Maladaptive Problem Solving and Intimate Partner Violence

Abstract
:1. Introduction
1.1. Childhood Emotional Abuse and Physical IPV
1.2. Experiential Avoidance as a Mechanism of CEA-IPV Link
1.3. Social Problem Solving as a Mechanism of CEA-IPV Link
1.4. Summary and Current Study
- After including the influences of experiential avoidance and social problem solving, none of the childhood maltreatment forms would be directly associated with IPV victimization and perpetration.
- Experiential avoidance would be indirectly associated with IPV victimization and perpetration via all three maladaptive social problem solving dimensions.
- After controlling for the effects of CPA and CSA, CEA would remain indirectly predictive of IPV victimization and perpetration via experiential avoidance and social problem solving.
2. Method
2.1. Participants
2.2. Measures
2.2.1. Demographic Questionnaire
2.2.2. Physical Intimate Partner Violence
2.2.3. Social Problem Solving
2.2.4. Childhood Abuse
2.2.5. Experiential Avoidance
2.3. Procedure
3. Results
3.1. Descriptive Characteristics of Study Variables

{kind=link}
{kind=link}
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| N | 221 | 225 | 231 | 230 | 232 | 169 | 230 | 230 | 230 |
| M/SD | 2.05 (2.46) | 3.31 (3.70) | 10.81 (6.16) | 9.23 (5.33) | 8.75 (6.22) | 35.11 (7.07) | 98.17 (16.62) | 97.89 (17.65) | 97.67 (14.19) |
| Min/Max | 0/12 | 0/12 | 5/25 | 5/25 | 5/25 | 16/54 | 73/162 | 74/162 | 78/155 |
| 1. Physical IPV Perpetration | 1 | ||||||||
| 2. Physical IPV Victimization | 0.66 ** | 1 | |||||||
| 3. Childhood Emotional Abuse | 0.16 * | 0.21 ** | 1 | ||||||
| 4. Childhood Physical Abuse | 0.20 ** | 0.24 ** | 0.66 ** | 1 | |||||
| 5. Childhood Sexual Abuse | 0.12 | 0.18 ** | 0.46 ** | 0.47 ** | 1 | ||||
| 6. Experiential Avoidance | 0.24 ** | 0.28 ** | 0.20 ** | 0.14 | 0.04 | 1 | |||
| 7. SPSI-R:S—Impulsivity/Carelessness (IC) | 0.29 ** | 0.33 ** | 0.23 ** | 0.08 | 0.07 | 0.31 ** | 1 | ||
| 8. SPSI-R:S—Negative Problem Orientation (NPO) | 0.03 | 0.03 | 0.25 ** | 0.13 | 0.07 | 0.42 ** | 0.59 ** | 1 | |
| 9. SPSI-R:S—Avoidance Style (AS) | 0.17 * | 0.16 * | 0.21 ** | 0.07 | 0.09 | 0.34 ** | 0.65 ** | 0.66 ** | 1 |
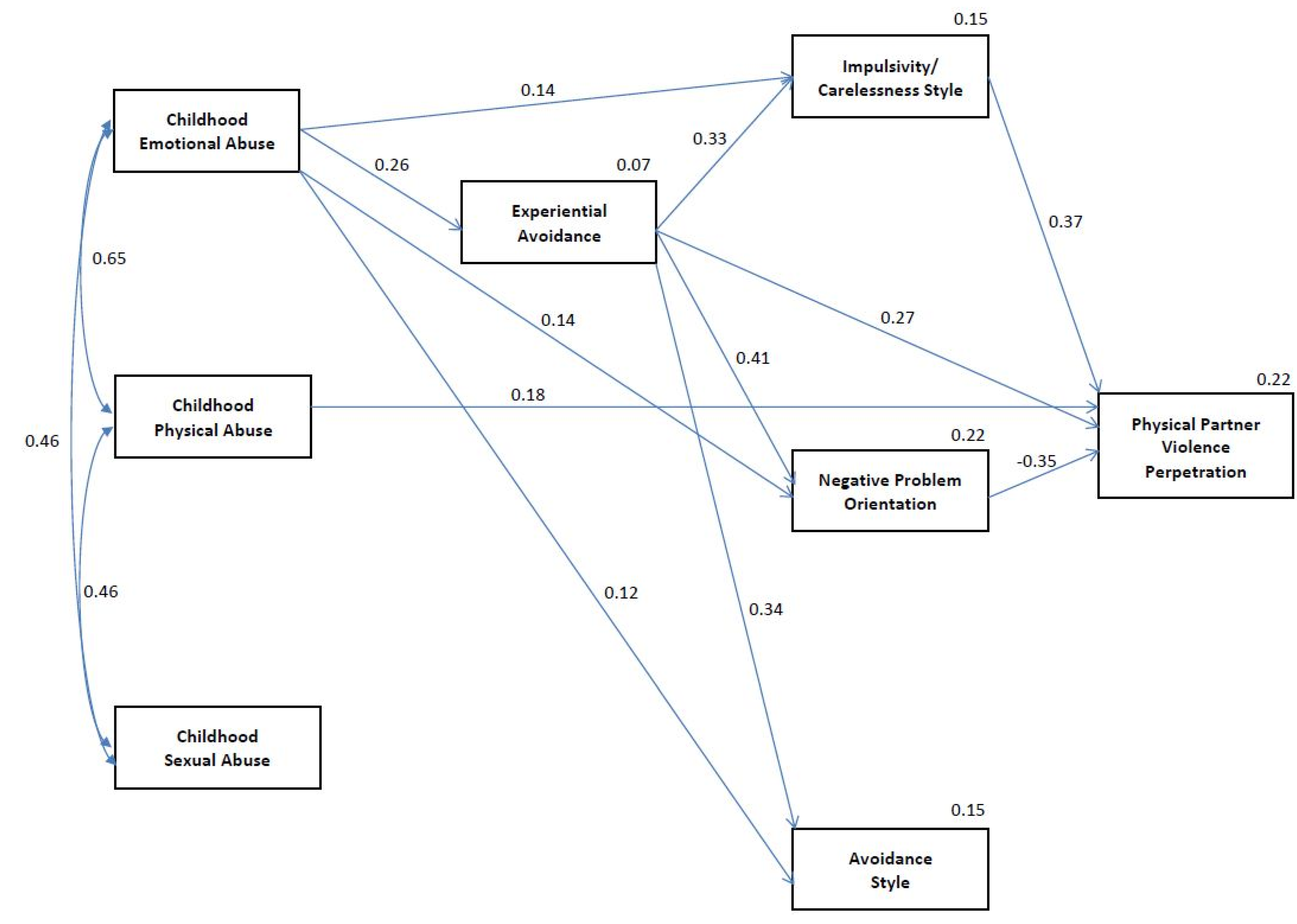
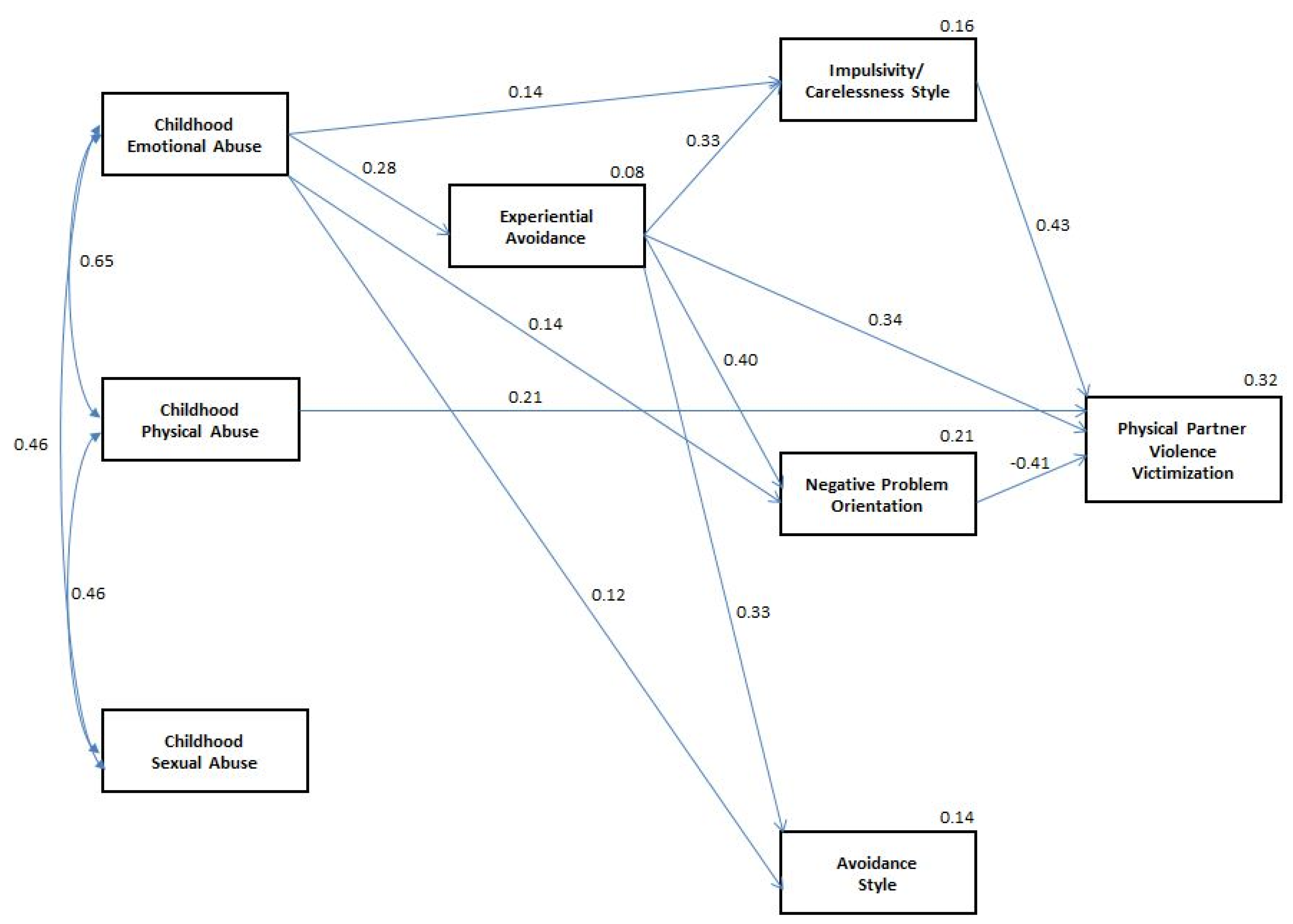
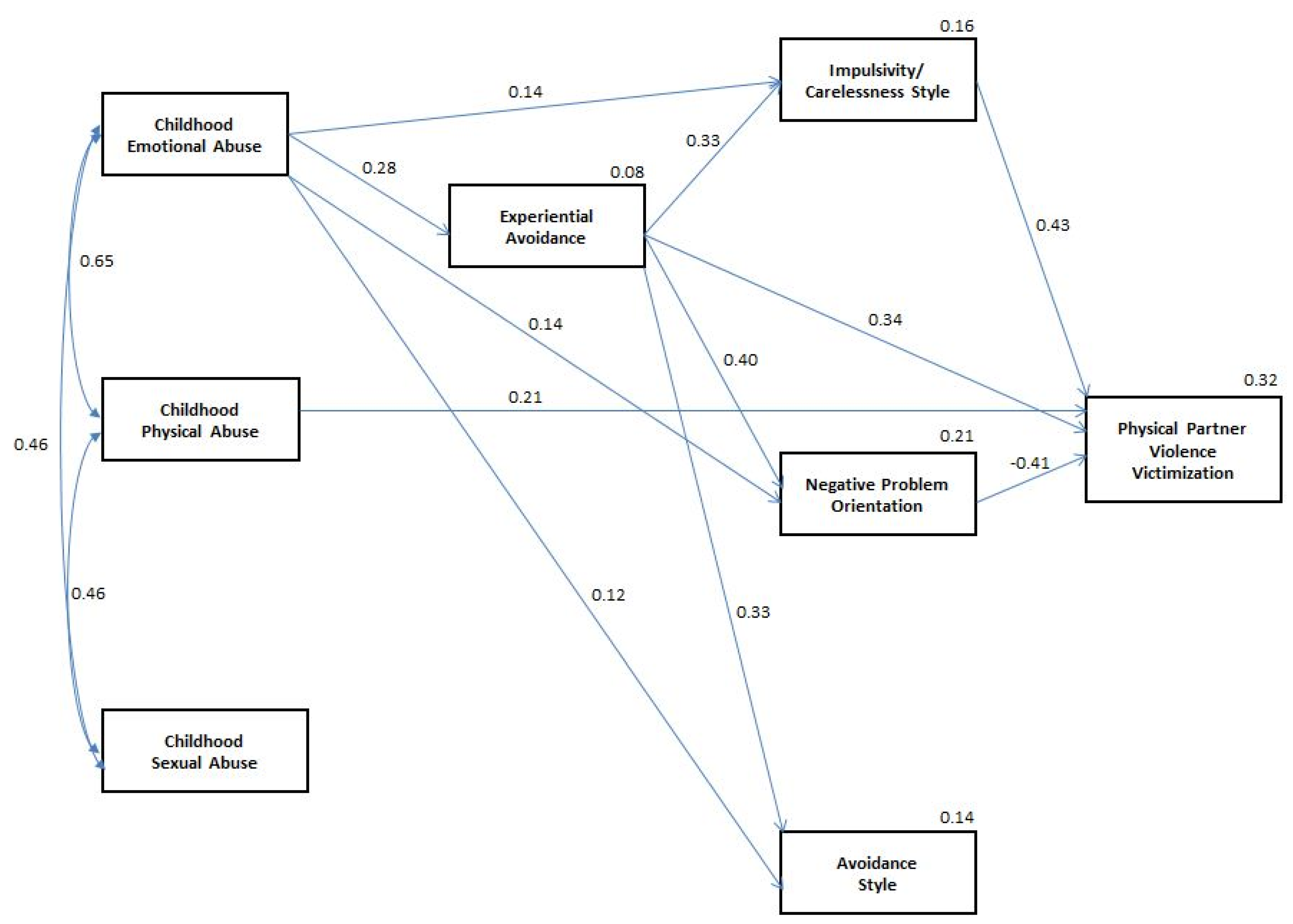
3.2. Path Analyses

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Finkelhor, D.; Ormrod, R.; Turner, H.; Hamby, S.L. The victimization of children and youth: A comprehensive, national survey. Child Maltreat. 2005, 10, 5–25. [Google Scholar] [CrossRef] [PubMed]
- Scher, C.D.; Stein, M.B.; Asmundson, G.J.G.; McCreary, D.R.; Forde, D.R. The Childhood Trauma Questionnaire in a community sample: Psychometric properties and normative data. J. Trauma. Stress 2001, 14, 843–857. [Google Scholar] [CrossRef] [PubMed]
- Dodge Reyome, N. Childhood emotional maltreatment and later intimate relationships: Themes from the empirical literature. J. Aggress. Maltreat. Trauma 2010, 19, 224–242. [Google Scholar]
- Glaser, D. Emotional abuse and neglect (psychological maltreatment): A conceptual framework. Child Abuse Negl. 2002, 26, 697–714. [Google Scholar] [CrossRef] [PubMed]
- Zurbriggen, E.L.; Gobin, R.L.; Freyd, J.J. Childhood emotional abuse predicts late adolescent sexual aggression perpetration and victimization. J. Aggress. Maltreat. Trauma 2010, 19, 204–223. [Google Scholar] [CrossRef]
- Bernstein, D.P.; Fink, L. Childhood Trauma Questionnaire: A Retrospective Self-Report Manual; Harcourt Brace & Company: San Antonio, TX, USA, 1998. [Google Scholar]
- U.S. Department of Health and Human Services; Administration for Children and Families; Administration on Children, Youth and Families; Children’s Bureau. Child Maltreatment 2013; Children’s Bureau: Washington, DC, USA, 2015. [Google Scholar]
- Stoltenborgh, M.; Bakermans-Kranenburg, M.; Alink, L.R.A.; van Ijzendoorn, M.H. The universality of childhood emotional abuse: A meta-analysis of worldwide prevalence. J. Aggress. Maltreat. Trauma 2012, 21, 870–890. [Google Scholar] [CrossRef]
- World Health Organization. Child abuse and neglect by parents and other caregivers. In World Report on Violence and Health; Krug, E.G., Dahlberg, L.L., Mercy, J.A., Zwi, A.B., Lozano, R., Eds.; World Health Organization: Geneva, Switzerland, 2002; pp. 57–86. [Google Scholar]
- Slep, A.M.S.; Heyman, R.E.; Snarr, J.D. Child emotional aggression and abuse: Definitions and prevalence. Child Abuse Negl. 2011, 35, 783–796. [Google Scholar] [PubMed]
- Trickett, P.K.; Mennen, F.E.; Kim, K.; Sang, J. Emotional abuse in a sample of multiply maltreated, urban young adolescents: Issues of definition and identification. Child Abuse Negl. 2009, 33, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Claussen, A.H.; Crittenden, P.M. Physical and psychological maltreatment: Relations among types of maltreatment. Child Abuse Negl. 1991, 15, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Higgins, D.J.; McCabe, M.P. Multiple forms of child abuse and neglect: Adult retrospective reports. Aggress. Viol. Behav. 2001, 6, 547–578. [Google Scholar] [CrossRef]
- Trickett, P.K.; Kim, K.; Prindle, J. Variations in emotional abuse experiences among multiply maltreated young adolescents and relations with developmental outcomes. Child Abuse Negl. 2011, 35, 876–886. [Google Scholar] [PubMed]
- Berzenski, S.R.; Yates, T.M. Research on intimate partner violence: A developmental process analysis of the contribution of childhood emotional abuse to relationship violence. J. Aggress. Maltreat. Trauma 2010, 19, 180–203. [Google Scholar] [CrossRef]
- Perry, A.R.; DiLillo, D.; Peugh, J. Childhood psychological maltreatment and quality of marriage: The mediating role of psychological distress. J. Emot. Abuse 2007, 7, 117–142. [Google Scholar] [CrossRef]
- Briere, J.; Runtz, M. Differential adult symptomatology associated with three types of child abuse histories. Child Abuse Negl. 1990, 14, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Briere, J.; Runtz, M. Multivariate correlates of childhood psychological and physical maltreatment among university women. Child Abuse Negl. 1988, 12, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Teicher, M.H.; Samson, J.A.; Polcari, A.; McGreenery, C.E. Sticks, stones, and hurtful words: Relative effects of various forms of childhood maltreatment. Am. J. Psychiatry 2006, 163, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Harter, S. The effects of child abuse on the self-system. J. Aggress. Maltreat. Trauma 1998, 2, 147–169. [Google Scholar] [CrossRef]
- Hyman, S.M.; Garcia, M.; Sinha, R. Gender specific associations between types of childhood maltreatment and the onset, escalation and severity of substance use in cocaine dependent adults. Am. J. Drug Alcohol Abuse 2006, 32, 655–664. [Google Scholar] [CrossRef] [PubMed]
- Schneider, R.; Baumrind, N.; Kimerling, R. Exposure to child abuse and risk for mental health problems in women. Violence Vict. 2007, 22, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Witkiewitz, K.; Dodge-Reyome, N. Recollections of childhood psychological maltreatment and self-reported eating disordered behaviors in undergraduate college females. J. Emot. Abuse 2001, 2, 15–29. [Google Scholar] [CrossRef]
- Dodge Reyome, N.; Ward, K.S.; Witkiewitz, K. Psychosocial variables as mediators of the relationship between childhood history of emotional maltreatment, codependency, and self-silencing. J. Aggress. Maltreat. Trauma 2010, 19, 159–179. [Google Scholar] [CrossRef]
- Drapeau, M.; Perry, J.C. Childhood trauma and adult interpersonal functioning: A study using the Core Conflictual Relationship Theme Method (CCRT). Child Abuse Negl. 2004, 28, 1049–1066. [Google Scholar] [CrossRef] [PubMed]
- Messman-Moore, T.; Coates, A.A. The impact of childhood psychological abuse on adult interpersonal conflict: The role of early maladaptive schemas and patterns of interpersonal behavior. J. Emot. Abuse 2007, 7, 75–92. [Google Scholar] [CrossRef]
- Loos, M.E.; Alexander, P.C. Differential effects associated with self-reported histories of abuse and neglect in a college sample. J. Interpers. Violence 1997, 12, 340–360. [Google Scholar] [CrossRef]
- Capaldi, D.M.; Knoble, N.B.; Shortt, J.W.; Kim, H.K. A systematic review of risk factors for intimate partner violence. Partner Abuse 2012, 3, 1–194. [Google Scholar] [CrossRef]
- Colman, R.A.; Widom, C.S. Childhood abuse and neglect and adult intimate relationships: A prospective study. Child Abuse Negl. 2004, 28, 1133–1151. [Google Scholar] [CrossRef] [PubMed]
- Cascardi, M.; O’Leary, K.D.; Lawrence, E.E.; Schlee, K.A. Characteristics of women physically abused by their spouses and who seek treatment regarding marital conflict. J. Consult. Clin. Psychol. 1995, 63, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Seedat, S.; Stein, M.B.; Forde, D.R. Association between physical partner violence, posttraumatic stress, childhood trauma, and suicide attempts in a community sample of women. Violence Vict. 2005, 20, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Wekerle, C.; Leung, E.; Wall, A.; MacMillan, H.; Boyle, M.; Trocme, N.; Waechter, R. The contribution of childhood emotional abuse to teen dating violence among child protective services-involved youth. Child Abuse Negl. 2009, 33, 45–58. [Google Scholar] [CrossRef] [PubMed]
- Gay, L.E.; Harding, H.G.; Jackson, J.L.; Burns, E.E.; Baker, B.D. Attachment style and early maladaptive schemas as mediators of the relationship between childhood emotional abuse and intimate partner violence. J. Aggress. Maltreat. Trauma 2013, 22, 408–424. [Google Scholar] [CrossRef]
- Crawford, E.; Wright, M.O. The impact of childhood psychological maltreatment on interpersonal schemas and subsequent experiences of relationship aggression. J. Emot. Abuse 2007, 7, 93–116. [Google Scholar] [CrossRef]
- D’Zurilla, T.J.; Maydeu-Olivares, A. Conceptual and methodological issues in social problem-solving assessment. Behav. Ther. 1995, 26, 409–432. [Google Scholar] [CrossRef]
- Lemerise, E.A.; Arsenio, W.F. An integrated model of emotion processes and cognition in social information processing. Child Dev. 2000, 71, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Saarni, C.; Campos, J.J.; Camras, L.A.; Witherington, D. Emotional Development: Action, Communication, and Understanding; Eisenberg, N., Damon, W., Lerner, R.M., Eds.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2006; pp. 226–299. [Google Scholar]
- Hayes, S.C.; Wilson, K.G.; Gifford, E.V.; Follette, V.M.; Strosahl, K. Experiential avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. J. Consult. Clin. Psychol. 1996, 64, 1152–1168. [Google Scholar] [CrossRef] [PubMed]
- Chapman, A.L.; Gratz, K.L.; Brown, M.Z. Solving the puzzle of deliberate self-harm: The experiential avoidance model. Behav. Res. Ther. 2006, 44, 371–394. [Google Scholar] [CrossRef] [PubMed]
- Tull, M.T.; Gratz, K.L.; Salters, K.; Roemer, L. The role of experiential avoidance in posttraumatic stress symptoms and symptoms of depression, anxiety, and somatization. J. Nerv. Ment. Dis. 2004, 192, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Polusny, M.A.; Rosenthal, M.Z.; Aban, I.; Follette, V.M. Experiential avoidance as a mediator of the effects of adolescent sexual victimization on negative adult outcomes. Violence Vict. 2004, 19, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Tull, M.T.; Jakupcak, M.; Paulson, A.; Gratz, K.L. The role of emotional inexpressivity and experiential avoidance in the relationship between posttraumatic stress disorder symptom severity and aggressive behavior among men exposed to interpersonal violence. Anxiety Stress Coping 2007, 20, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Reddy, M.K.; Meis, L.A.; Erbes, C.R.; Polusny, M.A.; Compton, J.S. Associations among experiential avoidance, couple adjustment, and interpersonal aggression in returning Iraqi war veterans and their partners. J. Consult. Clin. Psychol. 2011, 79, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Gratz, K.L.; Bornovalova, M.A.; Delany-Brumsey, A.; Nick, B.; Lejuez, C.W. A laboratory-based study of the relationship between childhood abuse and experiential avoidance among inner-city substance users: The role of emotional nonacceptance. Behav. Ther. 2007, 38, 256–268. [Google Scholar] [CrossRef] [PubMed]
- Shenk, C.E.; Putnam, F.W.; Noll, J.G. Experiential avoidance and the relationship between child maltreatment and PTSD symptoms: Preliminary evidence. Child Abuse Negl. 2012, 36, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Krause, E.D.; Mendelson, T.; Lynch, T.R. Childhood emotional invalidation and adult psychological distress: The mediating role of emotional inhibition. Child Abuse Negl. 2003, 27, 199–213. [Google Scholar] [CrossRef] [PubMed]
- Gratz, K.L.; Paulson, A.; Jakupcak, M.; Tull, M.T. Exploring the relationship between childhood maltreatment and intimate partner abuse: Gender differences in the mediating role of emotion dysregulation. Violence Vict. 2009, 24, 68–82. [Google Scholar] [CrossRef] [PubMed]
- D’Zurilla, T.J.; Nezu, A.M.; Maydeu-Olivares, A. Social Problem-Solving Inventory-Revised (SPSI-R): Technical Manual; Multi-Health Systems, Inc.: North Tonawanda, NY, USA, 2002. [Google Scholar]
- Maydeu-Olivares, A.; D’Zurilla, T.J. A factor analysis of the Social Problem-Solving Inventory using polychoric correlations. Eur. J. Psychol. Assess. 1995, 11, 98–107. [Google Scholar] [CrossRef]
- Maydeu-Olivares, A.; D’Zurilla, T.J. A factor-analytic study of the social problem-solving inventory: An integration of theory and data. Cognit. Ther. Res. 1996, 20, 115–133. [Google Scholar] [CrossRef]
- D’Zurilla, T.J.; Nezu, A.M.; Maydeu-Olivares, A. Social Problem Solving: Theory and Assessment; Chang, E.C., D’Zurilla, T.J., Sanna, L.J., Eds.; American Psychological Association: Washington, DC, USA, 2004; pp. 11–27. [Google Scholar]
- Nezu, A.M.; Ronan, G.F. Life stress, current problems, problem solving, and depressive symptoms: An integrative model. J. Consult. Clin. Psychol. 1985, 53, 693–697. [Google Scholar] [CrossRef] [PubMed]
- Nezu, A.M. Negative life stress and anxiety: Problem solving as a moderator variable. Psychol. Rep. 1986, 58, 279–283. [Google Scholar] [CrossRef] [PubMed]
- D’Zurilla, T.J.; Sheedy, C.F. Relation between social problem-solving ability and subsequent level of psychological stress in college students. J. Pers. Soc. Psychol. 1991, 61, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Nezu, A.M.; Ronan, G.F. Social problem solving and depression: Deficits in generating alternatives and decision making. South. Psychol. 1987, 3, 29–34. [Google Scholar]
- Nezu, A.M.; Ronan, G.F. Social problem solving as a moderator of stress-related depressive symptoms: A prospective analysis. J. Couns. Psychol. 1988, 35, 134–138. [Google Scholar] [CrossRef]
- Kant, G.L.; D’Zurilla, T.J.; Maydeu-Olivares, A. Social problem solving as a mediator of stress-related depression and anxiety in middle-aged and elderly community residents. Cognit. Ther. Res. 1997, 21, 73–96. [Google Scholar] [CrossRef]
- Chang, E.C.; D’Zurilla, T.J. Relations between problem orientation and optimism, pessimism, and trait affectivity: A construct validation study. Behav. Res. Ther. 1996, 34, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Christensen, A.; Shenk, J.L. Communication, conflict, and psychological distance in nondistressed, clinic, and divorcing couples. J. Consult. Clin. Psychol. 1991, 59, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Sabourin, S.; Laporte, L.; Wright, J. Problem solving self-appraisal and coping efforts in distressed and nondistressed couples. J. Marital Fam. Ther. 1990, 16, 89–97. [Google Scholar] [CrossRef]
- Nezu, A.M. Problem solving and behavior therapy revisited. Behav. Ther. 2004, 35, 1–33. [Google Scholar] [CrossRef]
- D’Zurilla, T.; Chang, E.C.; Sanna, L.J. Self-esteem and social problem solving as predictors of aggression in college students. J. Soc. Clin. Psychol. 2003, 22, 424–440. [Google Scholar] [CrossRef]
- Lochman, J.E.; Lampron, L.B. Situational social problem-solving skills and self-esteem of aggressive and nonaggressive boys. J. Abnorm. Child Psychol. 1986, 14, 605–617. [Google Scholar] [CrossRef] [PubMed]
- Lochman, J.E.; Wayland, K.K.; White, K.J. Social goals: Relationship to adolescent adjustment and to social problem solving. J. Abnorm. Child Psychol. 1993, 21, 135–151. [Google Scholar] [CrossRef] [PubMed]
- Lochman, J.E.; Dodge, K.A. Social-cognitive processes of severly violent, moderately aggressive, and nonaggressive boys. J. Consult. Clin. Psychol. 1994, 62, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Buss, A.H.; Perry, M. The aggression questionnaire. J. Pers. Soc. Psychol. 1992, 63, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Londahl, E.A.; Tverskoy, A.; D’Zurilla, T.J. The relations of internalizing symptoms to conflict and interpersonal problem solving in close relationships. Cognit. Ther. Res. 2005, 29, 445–462. [Google Scholar] [CrossRef]
- Burns, E.E.; Jackson, J.L.; Harding, H.G. Child maltreatment, emotion regulation, and posttraumatic stress: The impact of emotional abuse. J. Aggress. Maltreat. Trauma 2010, 19, 801–819. [Google Scholar] [CrossRef]
- Shipman, K.L.; Schneider, R.; Fitzgerald, M.M.; Sims, C.; Swisher, L.; Edwards, A. Maternal emotion socialization in maltreating and non-maltreating families: Implications for children’s emotion regulation. Soc. Dev. 2007, 16, 268–285. [Google Scholar] [CrossRef]
- Straus, M.A.; Hamby, S.L.; Boney-McCoy, S.; Sugarman, D.B. The revised Conflict Tactics Scales (CTS2): Development and preliminary psychometric data. J. Fam. Issues 1996, 17, 283–316. [Google Scholar] [CrossRef]
- Regan, K.V.; Bartholomew, K.; Kwong, M.J.; Trinke, S.J.; Henderson, A.J.Z. The relative severity of acts of physical violence in heterosexual relationships: An item response theory analysis. Pers. Relatsh. 2006, 13, 37–52. [Google Scholar] [CrossRef]
- Bernstein, D.P.; Fink, L.; Handelsman, L.; Foote, J.; Lovejoy, M.; Wenzel, K.; Sapareto, E.; Ruggiero, J. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am. J. Psychiatry 1994, 151, 1132–1136. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Strosahl, K.; Wilson, K.G.; Bissett, R.T.; Pistorello, J.; Toarmino, D.; Polusny, M.A.; Dykstra, T.A.; Batten, S.V.; Bergan, J.; et al. Measuring experiential avoidance: A preliminary test of a working model. Psychol. Rec. 2004, 54, 553–578. [Google Scholar]
- Catania, J.A.; Binson, D.; Canchola, J.; Pollack, L.M.; Hauck, W. Effects of interviewer gender, interviewer choice, and item wording on responses to questions concerning sexual behavior. Public Opin. Q. 1996, 60, 345–375. [Google Scholar] [CrossRef]
- Arbuckle, J.L. AMOS, Version 7; SPSS Inc.: Chicago, IL, USA, 2006. [Google Scholar]
- Daigneault, I.; Hébert, M.; McDuff, P. Men’s and women’s childhood sexual abuse and victimization in adult partner relationships: A study of risk factors. Child Abuse Negl. 2009, 33, 638–647. [Google Scholar] [CrossRef] [PubMed]
- Iverson, K.M.; Mercado, R.; Carpenter, S.L.; Street, A.E. Intimate partner violence among women veterans: Previous interpersonal violence as a risk factor. J. Trauma. Stress 2013, 26, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Renner, L.M.; Whitney, S.D. Risk factors for unidirectional and bidirectional intimate partner violence among young adults. Child Abuse Negl. 2012, 36, 40–52. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Corso, P.S. Gender differences in the connections between violence experienced as a child and perpetration of intimate partner violence in young adulthood. J. Fam. Violence 2008, 23, 303–313. [Google Scholar] [CrossRef]
- Shorey, R.C.; Brasfield, H.; Febres, J.; Stuart, G.L. The association between impulsivity, trait anger, and the perpetration of intimate partner and general violence among women arrested for domestic violence. J. Interpers. Violence 2011, 26, 2681–2697. [Google Scholar] [CrossRef] [PubMed]
- Schafer, J.; Caetano, R.; Cunradi, C.B. A path model of risk factors for intimate partner violence among couples in the United States. J. Interpers. Violence 2004, 19, 127–142. [Google Scholar] [CrossRef] [PubMed]
- Whitfield, C.L.; Anda, R.F.; Dube, S.R.; Felitti, V.J. Violent childhood experiences and the risk of intimate partner violence in adults: Assessment in a large health maintenance organization. J. Interpers. Violence 2003, 18, 166–185. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Press: New York, NY, USA, 1998. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bell, K.M.; Higgins, L. The Impact of Childhood Emotional Abuse and Experiential Avoidance on Maladaptive Problem Solving and Intimate Partner Violence. Behav. Sci. 2015, 5, 154-175. https://doi.org/10.3390/bs5020154
Bell KM, Higgins L. The Impact of Childhood Emotional Abuse and Experiential Avoidance on Maladaptive Problem Solving and Intimate Partner Violence. Behavioral Sciences. 2015; 5(2):154-175. https://doi.org/10.3390/bs5020154
Chicago/Turabian StyleBell, Kathryn M., and Lorrin Higgins. 2015. "The Impact of Childhood Emotional Abuse and Experiential Avoidance on Maladaptive Problem Solving and Intimate Partner Violence" Behavioral Sciences 5, no. 2: 154-175. https://doi.org/10.3390/bs5020154
APA StyleBell, K. M., & Higgins, L. (2015). The Impact of Childhood Emotional Abuse and Experiential Avoidance on Maladaptive Problem Solving and Intimate Partner Violence. Behavioral Sciences, 5(2), 154-175. https://doi.org/10.3390/bs5020154