1. Introduction
In recent years, several studies on psychology, behavior and health use rigorous techniques and measures of “space syntax” describing the network properties of spaces in terms of visibility and accessibility within hospitals and hospital nursing units of different geometry, size, and functions. As a result, the findings of these studies in dealing with the relationships between the network of spaces, on the one hand, and psychological responses and behavior, on the other, are less context-dependent and more generalizable [
1,
2,
3,
4,
5,
6,
7,
8,
9,
10,
11,
12]. Several space syntax studies to date, including the ones reported here, show strong relationships between spatial network measures and environmental behavior and psychology. Hillier and Hanson [
13] and Hillier [
14] are the two early publications that discuss the theoretical reasons why the relationships between network measures and behaviors are found.
In general, the space syntax studies of nursing units use two generic measures of network centrality-integration and control [
13] characterizing all the spaces in a unit, and one more specific measure of network centrality-targeted visibility [
8] characterizing only a few selected spaces/objects of interests based on the objective patterns of visibility and accessibility in the unit. Despite differences, however, all these space syntax measures are developed based on the same mathematical foundations described in [
13].
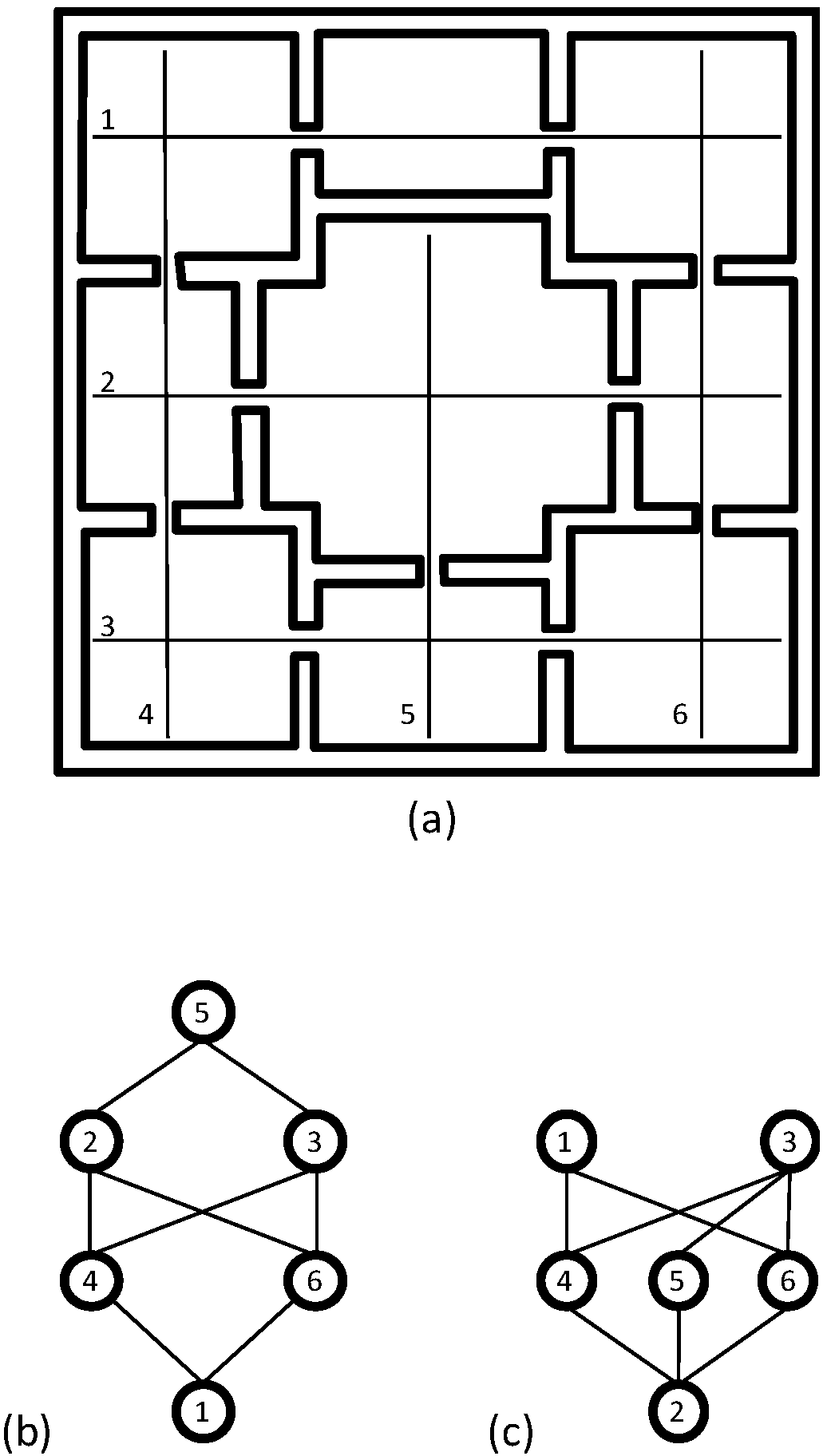
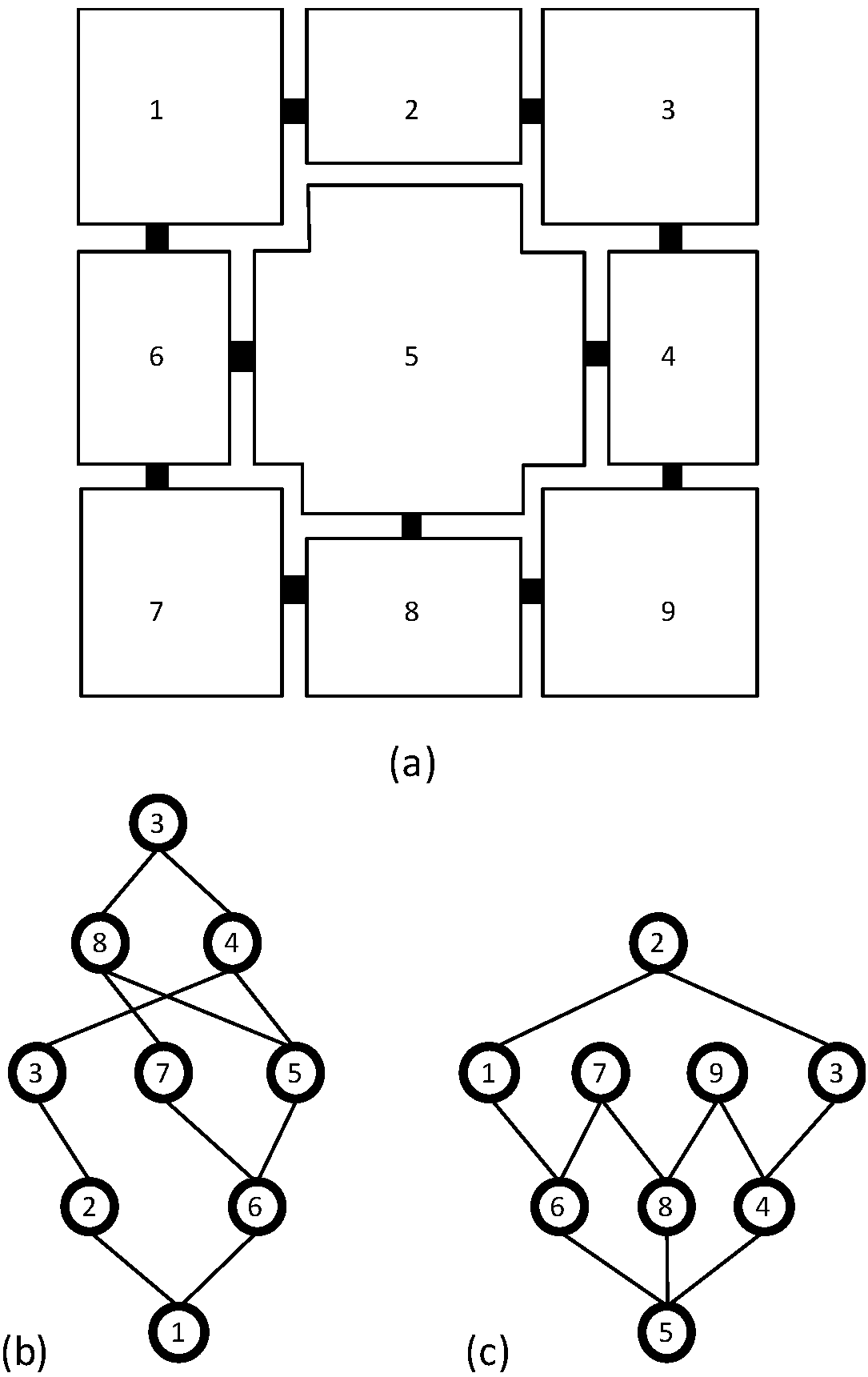
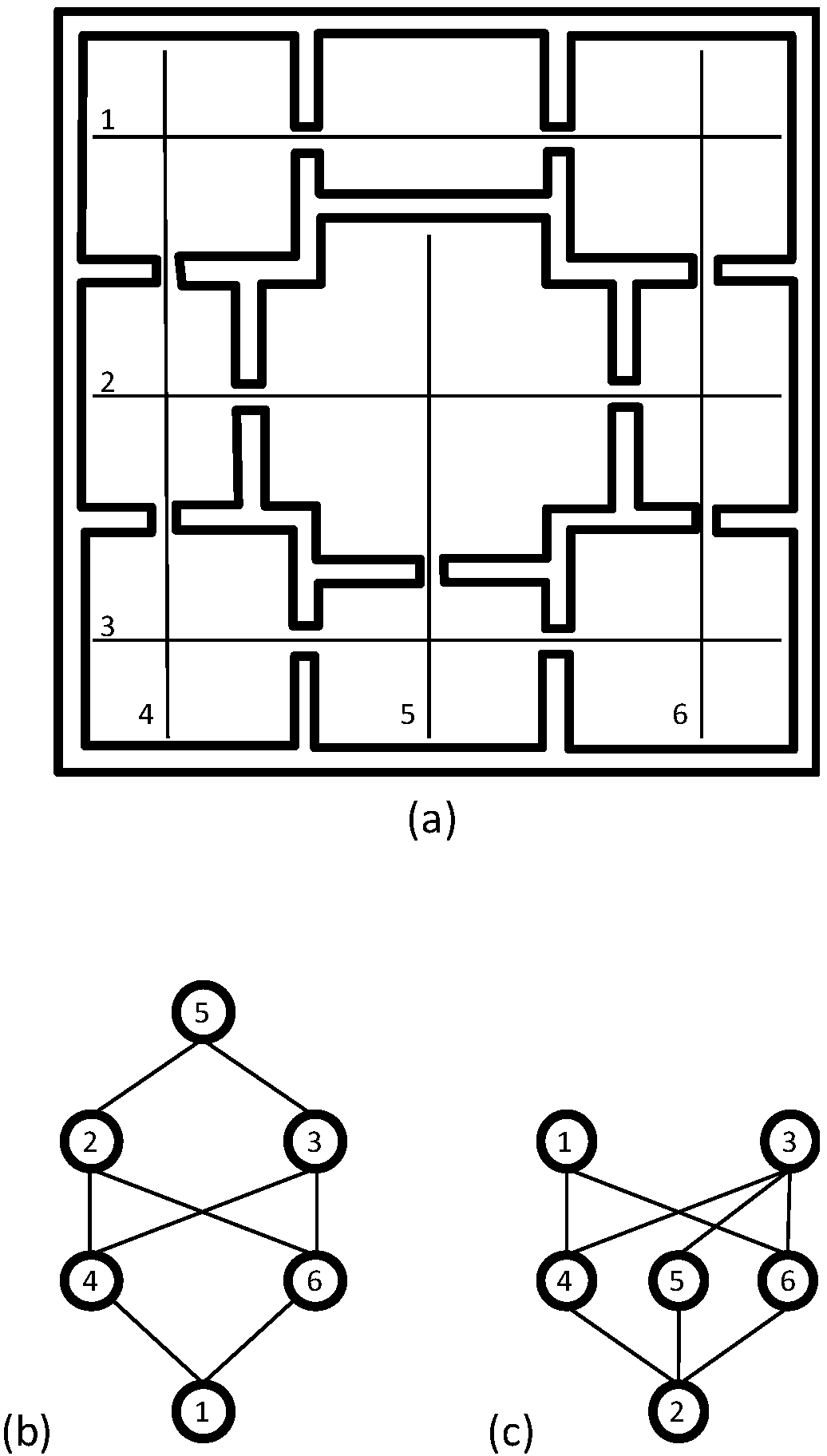
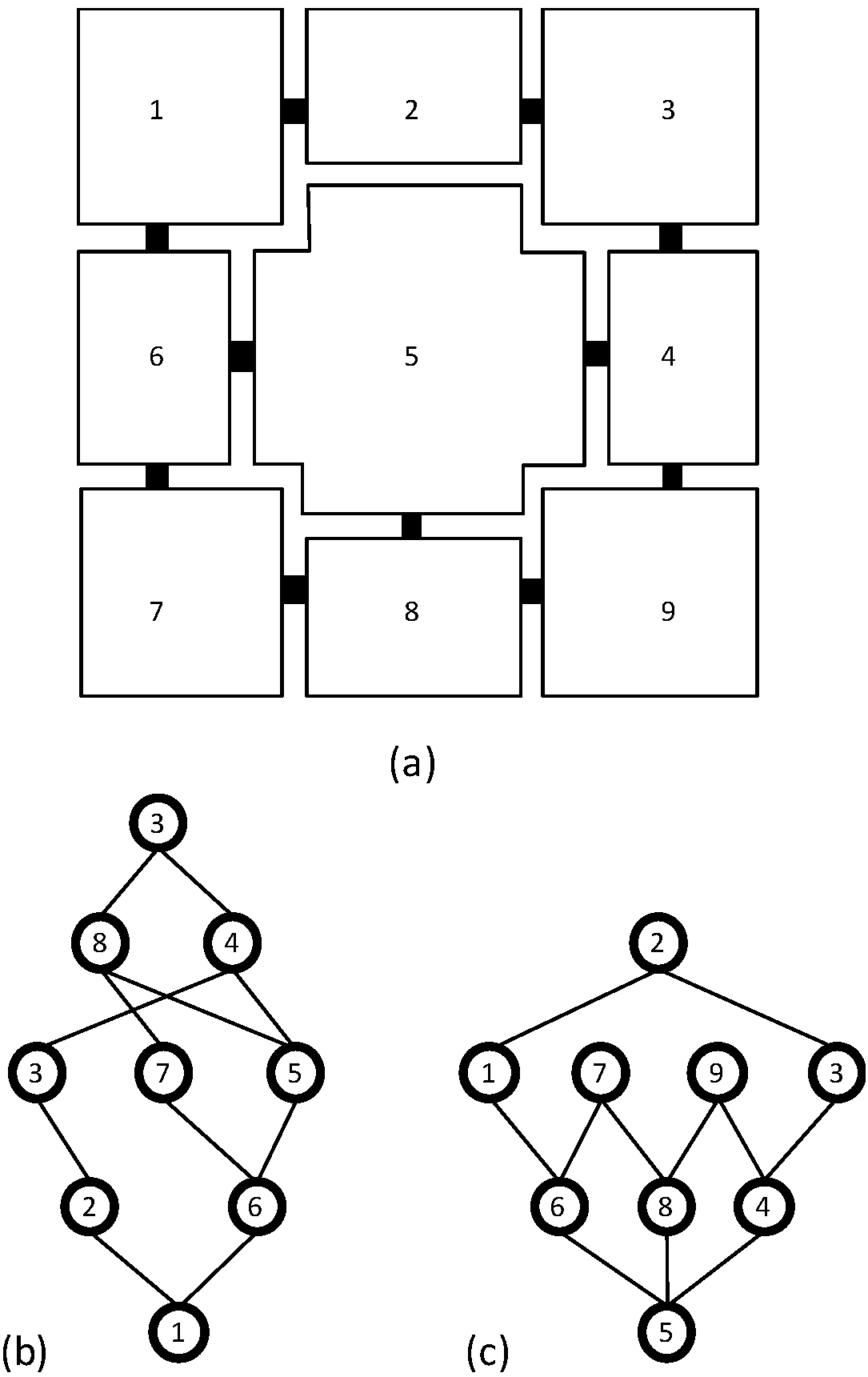
Simply defined, integration is a global network measure of centrality describing how a spatial element, which can be either 1- or 2-dimensional, is connected to all the other such elements in a layout. Spatial elements with higher integration are more easily visible and/or accessible from all the other similar elements in the layout; hence, they occupy more central positions in the system in terms of either visibility, accessibility, or both.
While integration is a global network measure, control is a local network measure of centrality that describes the degree to which a spatial element controls visual and/or physical access to its immediate neighboring spatial elements taking into account the number of alternative connections of each neighboring element. Hence, spatial elements with high control occupy more central positions within neighboring spaces in terms of how movement occurs among these neighboring elements.
In contrast to integration and control, the targeted visibility of a target, either a spatial element or an object, is computed based on the number of targets visible from a given target in relation to all the other similar targets in any given layout [
8]. (See the next section for additional information about these space syntax techniques and measures).
In their earlier study using integration and control, Alalouch and Aspinall [
1] investigated locational effects on perceived privacy in six different types of multi-bed units in the UK. A group of 79 subjects were asked to complete a questionnaire on privacy and to select preferred and disliked locations on plans of hospital wards. In the study, participants’ chosen locations for privacy showed a systematic relationship with spatial network properties of the unit layouts. Their choices for both high and low privacy locations were best represented by integration and control. At a unit level participants’ preference for greater privacy was for units with low integration and high control values; and within any unit, at a bed location level participants’ preference for privacy was in lower integration and lower control locations.
Later, using the additional data collected during the study reported in Alalouch and Aspinall [
1], Alalouch
et al. [
2] investigated the effect of age, gender, previous experience of space and cultural background on people’s chosen spatial location for privacy. Spatial data for this more recent study were provided by Visibility Graph Analysis (VGA) of space syntax [
15]. Findings indicated a universal preference for spatial location of privacy across culture, age and gender, and a specific significant difference for spatial location of privacy as a result of previous spatial experience. However, more studies are needed on privacy and intervisibility involving people with direct hospital unit experience in different cultures before the findings of the study can be generalized.
In another study, using space syntax techniques, Hendrich
et al. [
5] looked at the correlations between the integration values of individual spaces of the units and the dataset of the radio-frequency identification (RFID) movement patterns of 53 nurses, covering 143 nursing shifts, from 5 medical-surgical units. The results of their study showed that as integration of patient rooms increased, so did the frequency of shorter visits to these rooms and the total amount of time spent in these rooms. Later, using the data of the study reported by Hendrich
et al. [
5], Choudhary
et al. [
4] developed Generalized Linear Modeling (GLM) techniques to interpret the relationships between integration of spaces and nurses’ movement. In their study, Cai and Zimring [
3] found strong correlations between the integration values of spaces and the frequency of nurses’ interaction and peer awareness in these spaces in two different wings of a neurological intensive care unit (ICU).
In a different kind of study, Trzpuc and Martin [
10] used data from semi-structured interviews with end users and the more generic measures of centrality of space syntax to test several hypotheses on the potential functional benefits of visibility and accessibility in three medical-surgical units. They found that nurses’ perception of the potential functional benefits of visibility and accessibility did not match the potential benefits of these units identified using their network centrality values. While the finding is interesting, several confounding factors existed in the study. Therefore, the authors pointed out the need for additional studies before any definite conclusion could be drawn.
In addition, using the more generic measures of centrality of space syntax, Sagha Zadeh
et al. [
11] described the spatial relationships among clinical spaces in five medical-surgical units. The authors indicated that they measured movement distributions and identified possible conflicts with focus-demanding tasks, such as noise and interruptions in these units. However, they did not discuss how the data on movement distributions and possible conflicts were identified. Nevertheless, the authors identified several important areas in these units based on the study. Interestingly enough, some of these important areas such as report rooms, nourishment areas, and physician workspaces were not even included in the available healthcare design guidelines. The authors also identified that most caregivers move in patient corridors and nurses’ stations, posing the greatest possibility of interruptions by persons. They summarized the information in a visual diagram providing the “syntactic anatomy” of the units, and noted that the anatomy at this stage did not include many important design features including visibility, walking distance, scale, and number of beds and supply areas. They also noted that shadowing and observing of nurses would be necessary to customize the anatomy for individual cases in any future study.
Finally, using the more generic measures of centrality of space syntax, Kim and Lee [
6] investigated how the techniques of space syntax could be applied to assess the Whole-life Target Value Design (TVD) of healthcare facilities. While TVD can be defined as a management practice that strives to eliminate waste by setting a target cost and by spurring innovation within project constraints [
16], the Whole-life Target Value Design is a broad application of TVD toward facility operation and management, and user costs beyond initial costs of designing and building a facility. The authors used three hypothetical nursing units-shallow-plan, deep-plan and courtyard-plan-to determine which alternative is the most cost-efficient in terms of users. However, they do not define user costs in terms of financial value due to a lack of empirical evidence. Instead, they discuss user costs using such qualitative terms as high, medium and low. Based on the study, the authors found that the deep-plan has the lowest and the shallow-plan the highest user costs.
In contrast to the aforementioned studies using more general concepts of spatial centrality, Lu
et al. [
8] used the concept of targeted visibility in their study. The targeted visibility of such objects as patient beds in nursing units is important from a clinical perspective, because patient safety and medical outcomes often depend on how visible these beds are within a nursing unit [
7]. In their study on a Neurological ICU, Lu
et al. [
8] found that the distribution of staff density was more strongly correlated with the centrality measures computed based on targeted visibility than it was with the generic centrality measures. They also found that nurses, especially when interacting, prefer positions that provide high visual access to multiple patients; and that doctors prefer positions that maximize their awareness of the surrounding environment. Based on the study, Lu
et al. concluded that clinical staff members are tuned to different aspects of the visual structure of spaces based on their roles in hospital units.
In a later study, Lu and Zimring [
9] used the concept of targeted visibility to define the targeted visibility index (TVI) in order to compare different nursing units. TVI is expressed as the ratio of the average of the targeted visibility values of all locations and the total number of targets in the units. TVI, thus, describes the degree to which an observer can see all the targets in the units. Lu and Zimring used this measure to characterize the three units used in the study reported by Trites
et al. [
17], and found that the circulation spaces in the radial unit had the highest TVI, followed by the circulation spaces of the double-corridor units and then by that of the single-corridor unit. Thus, forty years after Trites
et al. [
17], these authors were able to define what Trites
et al. might have meant when they indicated that their radial unit had better visibility conditions than the double-corridor unit, which in turn had better visibility conditions than the single-corridor unit.
More recently, Lu
et al. [
7] reanalyzed Leaf
et al. [
18] data using TVI to describe the visibility of patient rooms in relation to ICU mortality. They found that among the sickest patients (those with Acute Physiology and Chronic Health Evaluation II > 30), visibility of patient rooms as measured by TVI accounted for 33.5% of the variance in ICU mortality (
p = 0.049), thus providing additional support for the importance of the visibility of patients in relation to ICU outcomes.
In summary, the studies using space syntax techniques have been able to show why and how the network properties of spaces are important for behaviors such as movement and interaction, psychological responses such as privacy, and medical and economic outcomes in nursing units. Together, they provide a way to develop theories linking behavior, psychological responses, and spatial network that bear some resemblance to Gibson’s concept of
affordance [
19,
20]. Gibson had offered this concept as an essential aspect of his theory of ecological perception, and argued that it is through the perception of affordances that animals perceive their environment, and that in any interaction between an animal and its environment, affordances allow the animal to perform certain actions with the environment. In general, positive affordances encourage human interactions, and negative affordances discourage them.
Later, Norman used the term “perceived affordability” describing the degree to which the affordance of an object maps onto its purpose [
21,
22]. If a chair does not allow the perceived affordance of “sit-ability”, then the natural mapping between its purpose and affordance does not exist. Since this absence of natural mapping breeds problems, one of the many goals of design research has been to understand how “perceived affordability” works in relation to design and its end users [
23,
24,
25,
26,
27].
In reality, however, the affordance of an object appears to be more easily defined than that of an environment. Space syntax theories and techniques are useful in this regard, because they use “perceptual primitives” (
i.e., objectively defined spatial elements which are perceptually meaningful) to define the objective structures of the environment, and then study how much of the variance in observed behavior and psychological responses can be explained by these structures [
28,
29,
30].
Yet, for the purposes of a theory explaining the effects of the network properties of spaces on behavior, psychological responses, and health in nursing units the number of space syntax studies reported in the literature remains insufficient. With the exception of Hendrich
et al. [
5] the reported studies are quite narrow in scope. Either they use only one or two case studies; or they use a very narrow set of predictor and dependent variables. In their study, using space syntax techniques, Hendrich
et al. used RFID movement data from as many as 5 medical-surgical units; but their datasets did not contain enough behavioral information. As a result, their findings were limited only to the frequency and the length of visits by nurses in patient rooms indicating a need for more studies on behaviors in nursing units.
Therefore, to further investigate the importance of the network properties of spaces in relation to behaviors in nursing units, the aim of this correlational research was to study the relationships between three network measures and four interaction-related behaviors in ICUs with different specialty types, size, and layout. The research focused on interaction-related behaviors because they promote effective communication and collaboration; and previous studies have indicated that effective communication and collaboration are key factors in patient and staff outcomes in hospitals and ICUs [
31]. In this regard, the research asked the following questions:
Are the ICUs included in the study similar or different in terms of spatial network properties describing visibility and accessibility? Our hypothesis concerning this is that the properties of spatial network in these ICUs would be similar because all ICUs require better environmental visibility and accessibility for efficient and effective patient care.
Are the observed patterns of interaction-related behaviors similar or different in the ICUs included in the study? Our hypothesis concerning this is that the observed behavioral patterns in the ICUs would be different from each other because of the differences in the clinical services they provide.
Are the interaction-related behaviors of ICU users (excluding patients) correlated with spatial network properties? Do the correlations vary based on the category of the participants engaged in these behaviors? Our hypothesis concerning this is that some interaction-related behaviors in these units would show consistent relations to spatial network measures describing accessibility and visibility. This might occur because all users generally would take advantages of spatial visibility and accessibility in ICUs to provide patient care.
4. Discussion
4.1. Rank Order of Different Categories of Spaces in the Units
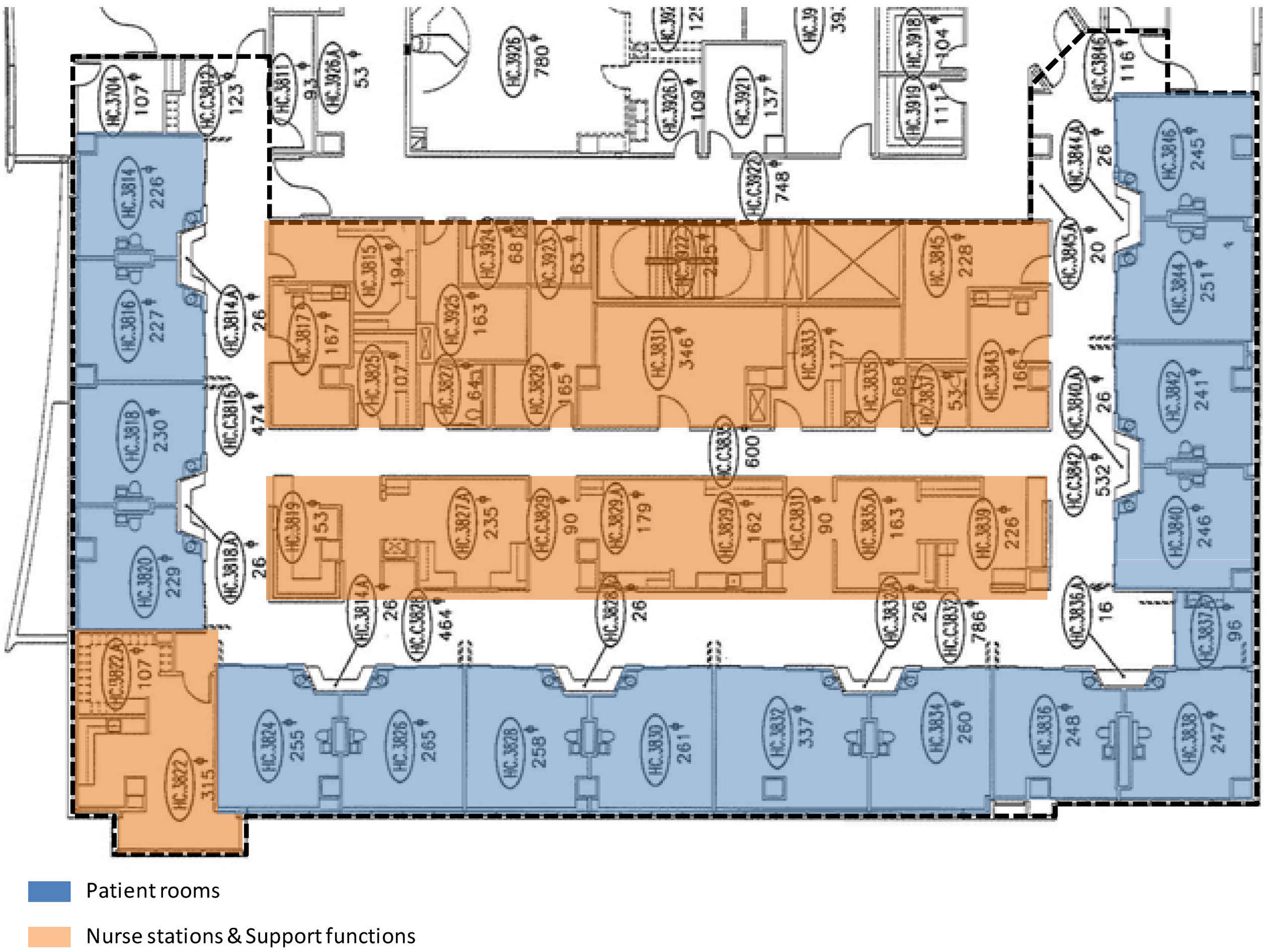
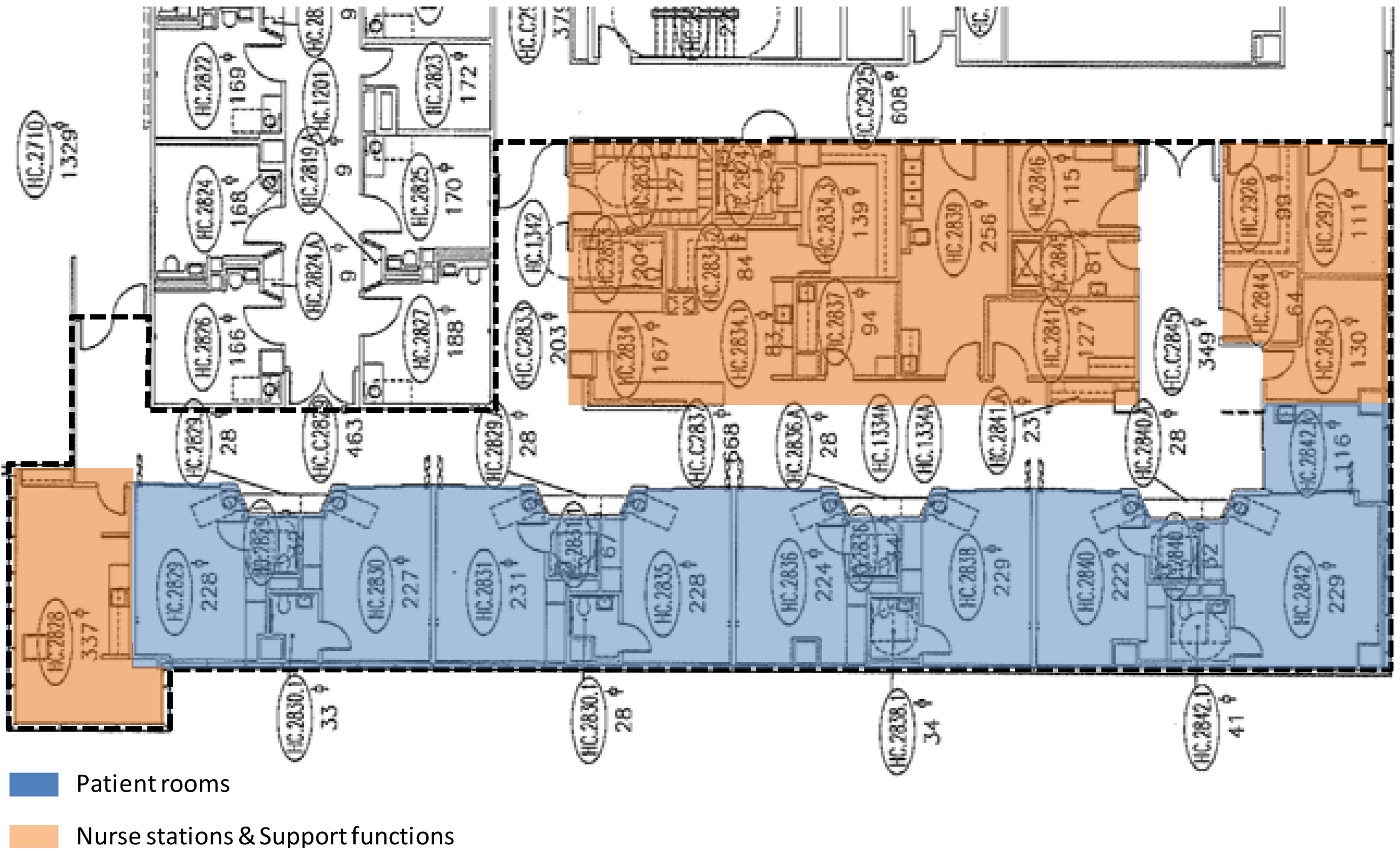
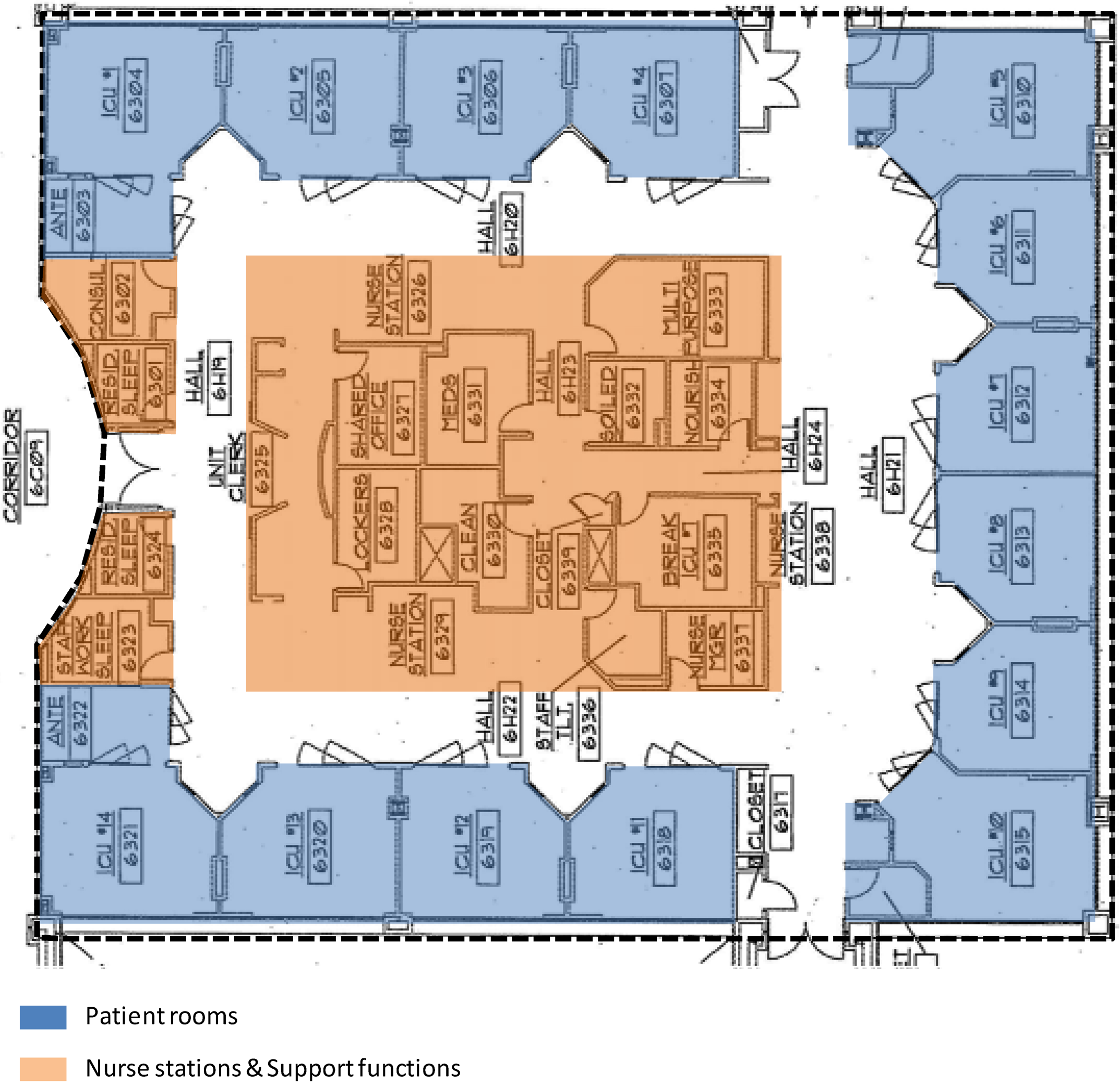
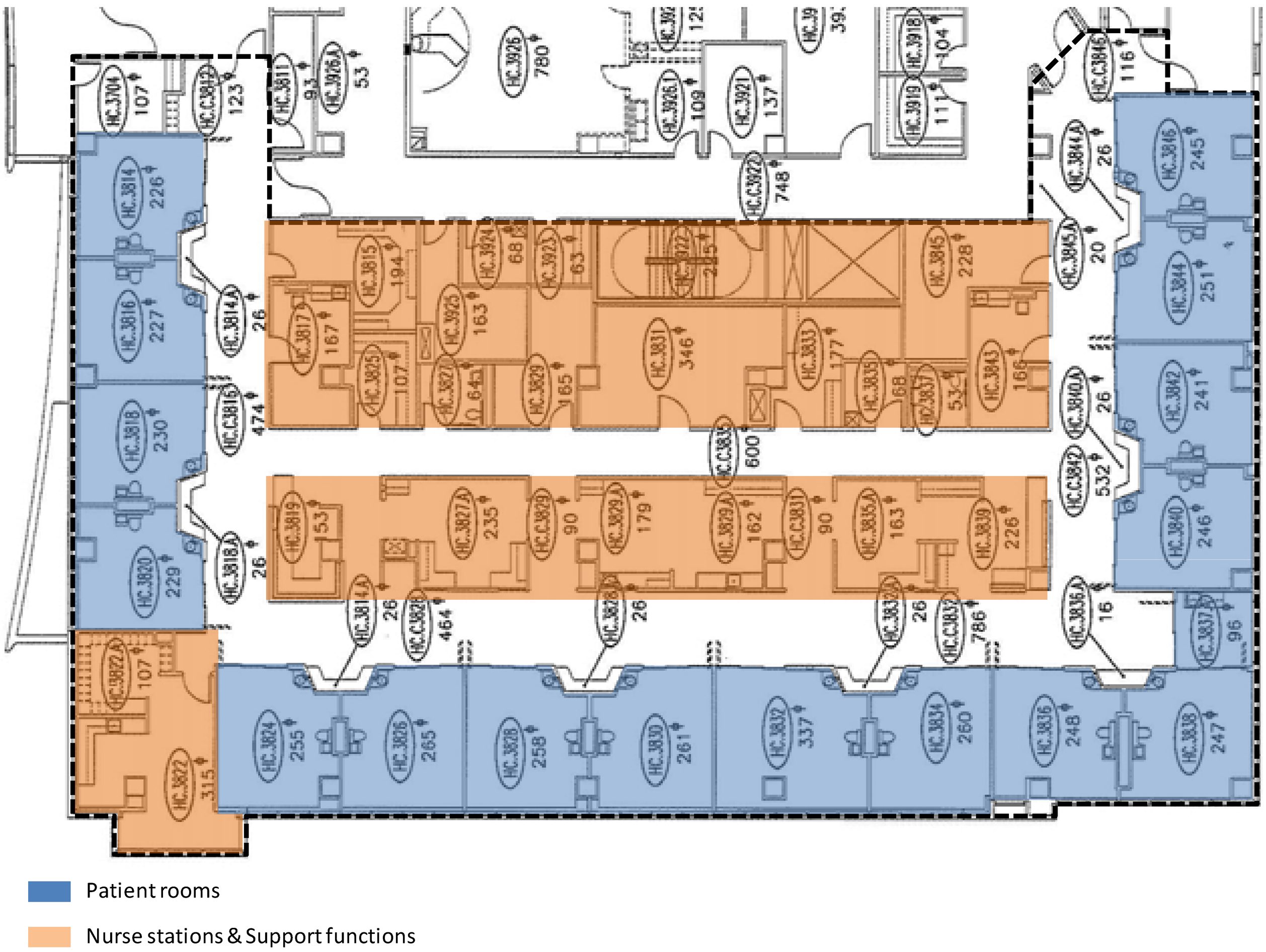
All ICUs require sufficient environmental visibility and accessibility for efficient and effective patient care. Therefore, it was hypothesized that the four ICUs included in this study would show similarities in spatial network properties describing environmental visibility and accessibility. The spatial layout analysis of the ICUs using the network measures of space syntax confirmed the hypothesis. Despite differences in specialty type, unit size, unit layout, and the distribution patterns of interaction-related behaviors, the ICUs included in the study showed underlying structural similarities defined by spatial networks.
The underlying structural similarities found here in the ICUs are also found in other designed environments of different size, shape and geometry [
13,
14,
35]. The literature has termed these similarities as “spatial genotypes”, and has argued that they are fundamental in the way designed environments representing a “type” reproduce social and cultural knowledge [
14,
35]. In this sense, the findings of this study are not surprising. They only reinforce the fact that all ICUs must embody a shared body of commonly-held programmatic knowledge in their spatial structures regardless of specialty type, unit size, unit geometry, and behaviors to represent a particular “type” of environmental setting. Without such a shared body of spatial knowledge, designers may not be able to design ICUs and users may not be able to use them.
The importance of the spatial similarities among the four ICUs is further emphasized by the fact that many significant correlations between spatial network measures and interaction-related behaviors among nurses, physicians, and others were found in these units. It is quite possible that these correlations were an artifact of the spatial genotypes of these ICUs over and above the similar functional needs of different groups of users. If our interpretations of the environment-behavior relationships found in this study are correct, then it can be argued that “spatial genotypes” are an essential component of Gibson’s concept of affordance [
20]. That is because they help define the inherent conditions or qualities of the environment (
i.e., affordances) that provide users with opportunities for taking certain actions in and with the environment.
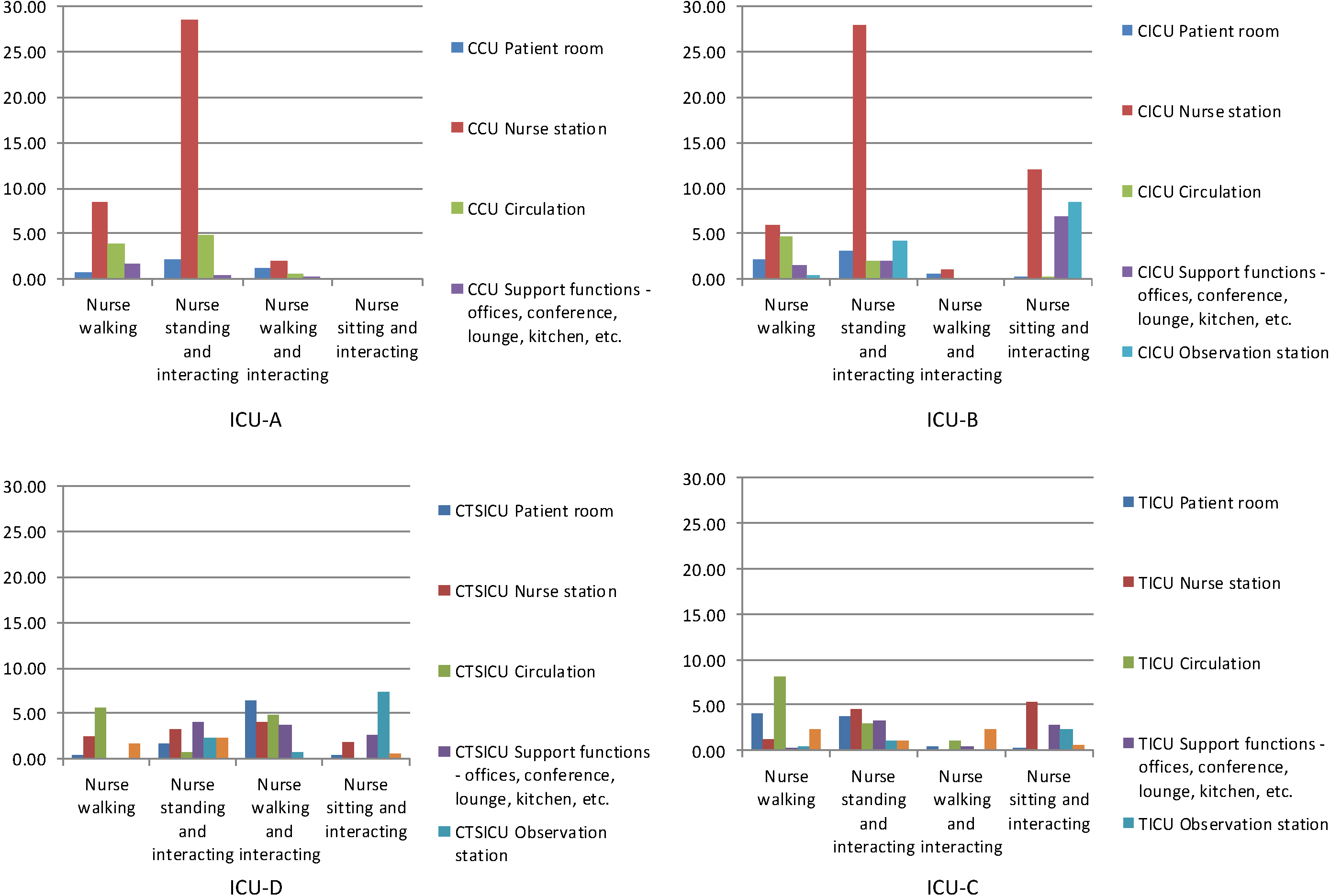
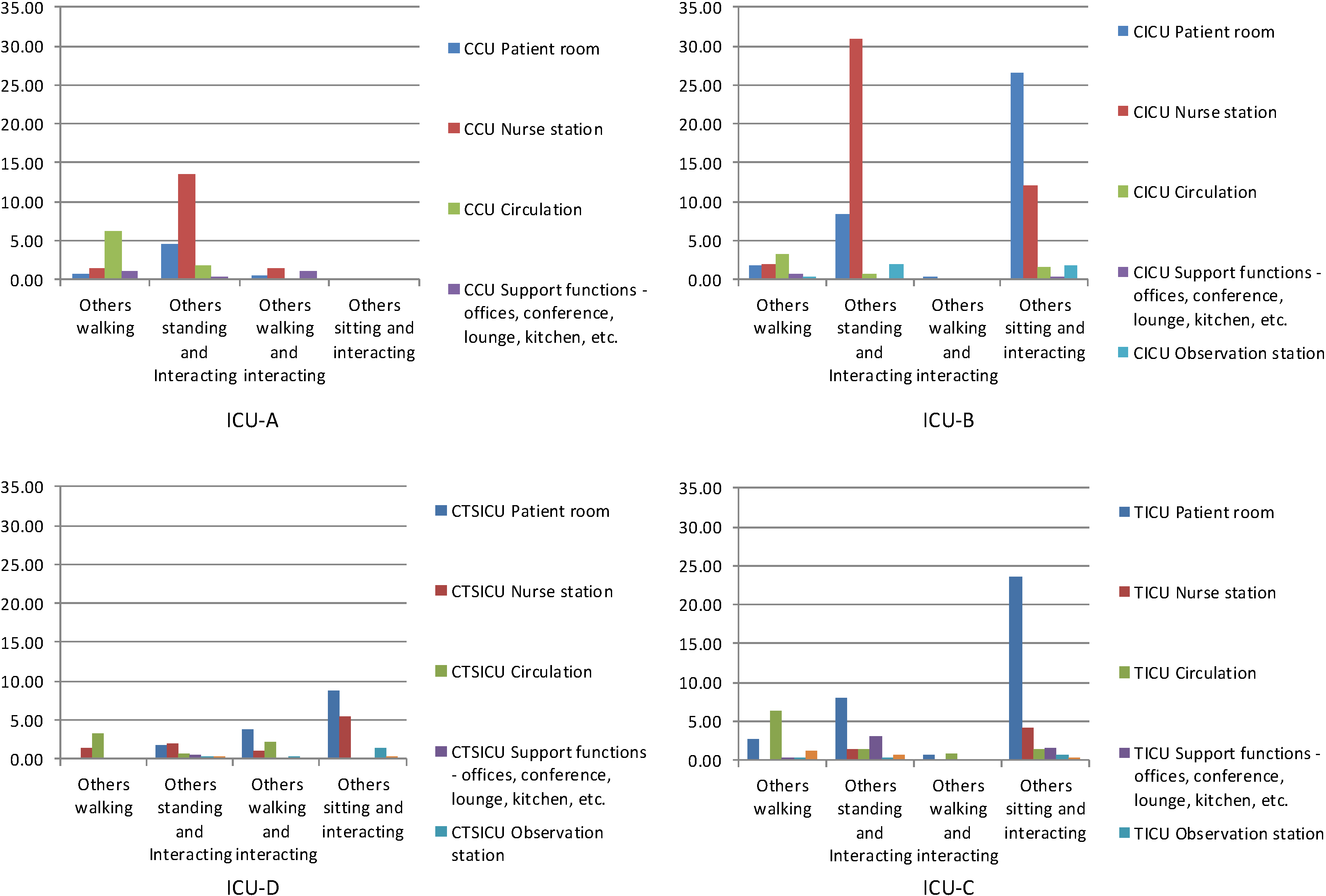
4.2. Behavioral Observations
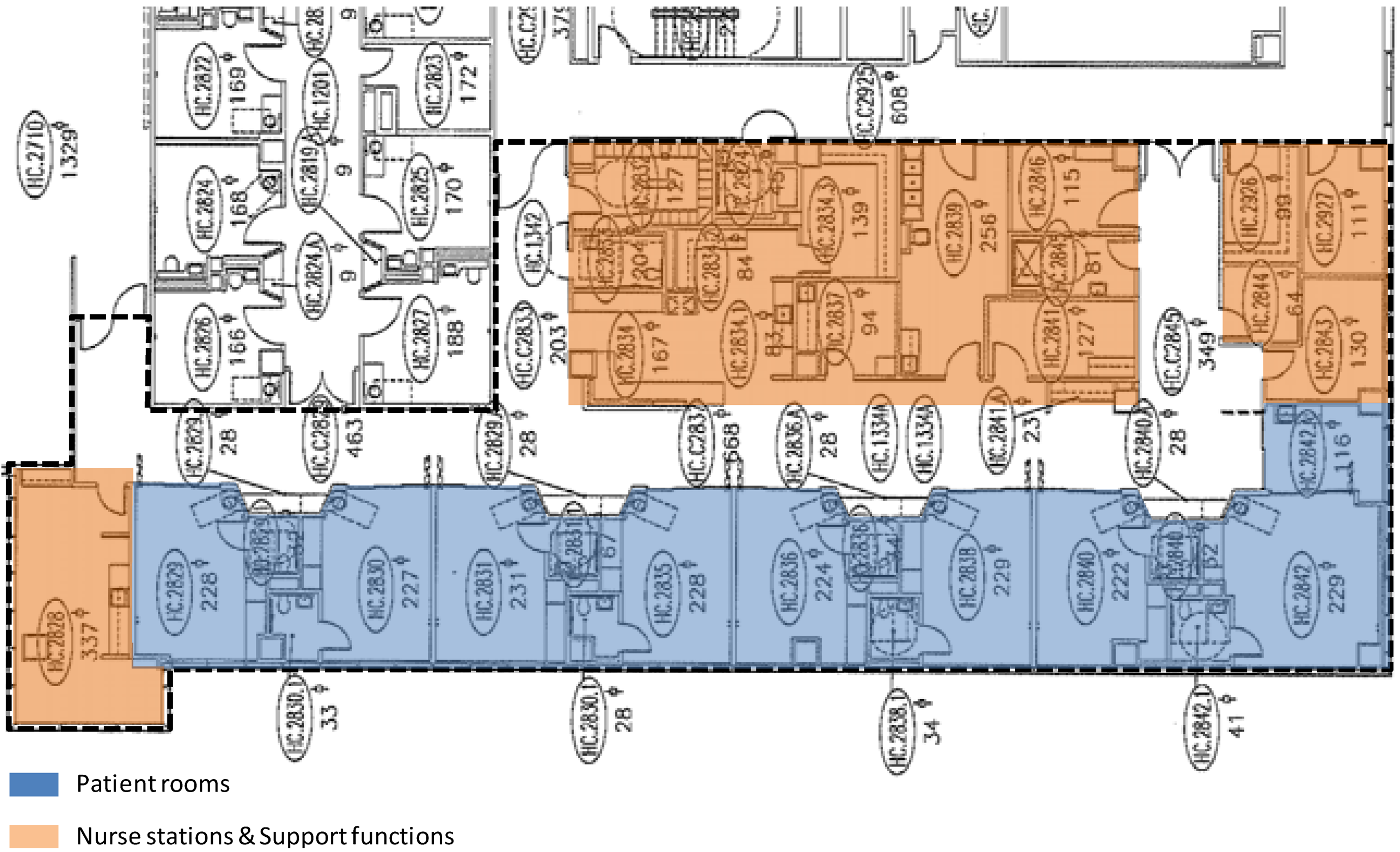
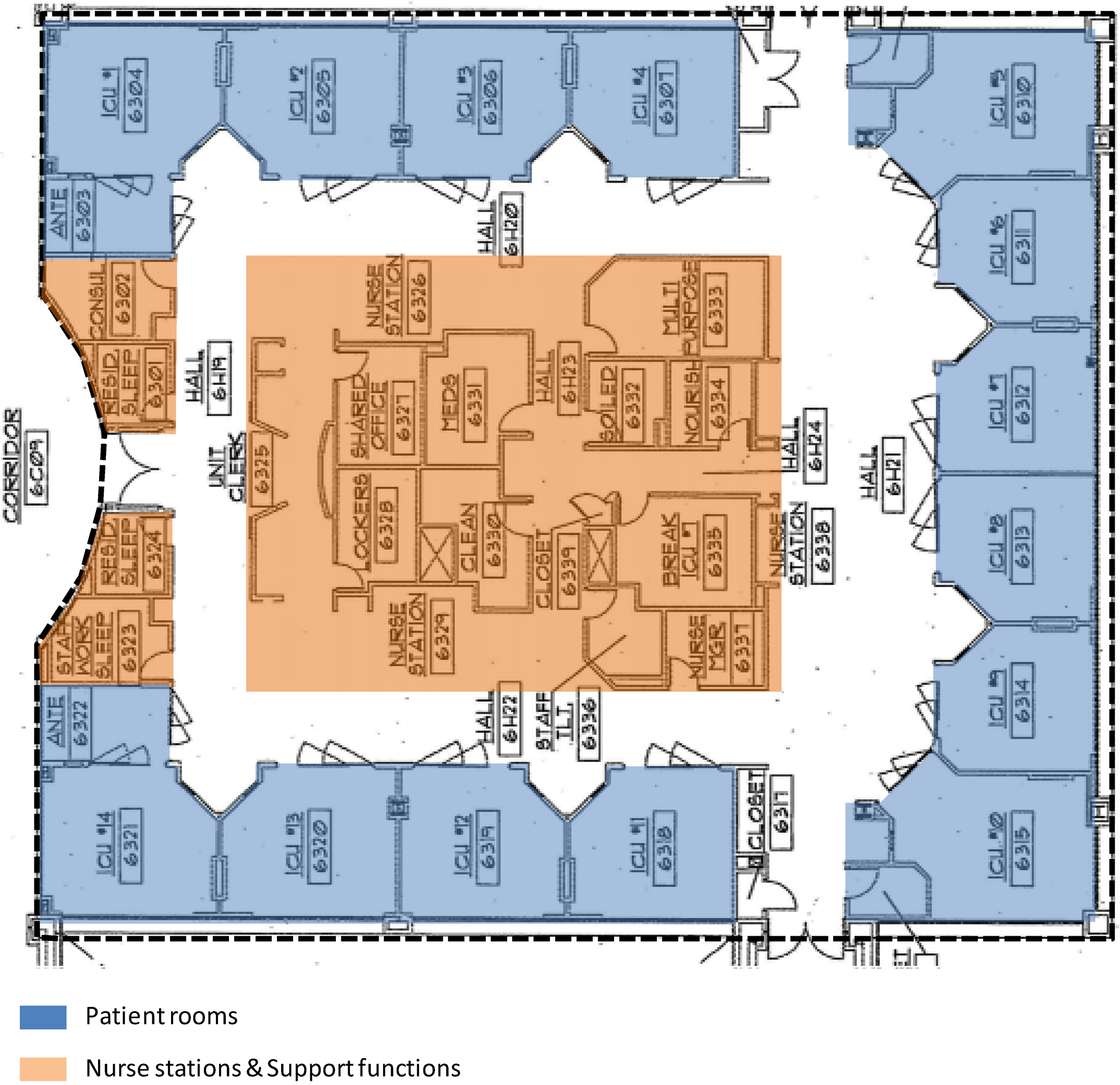
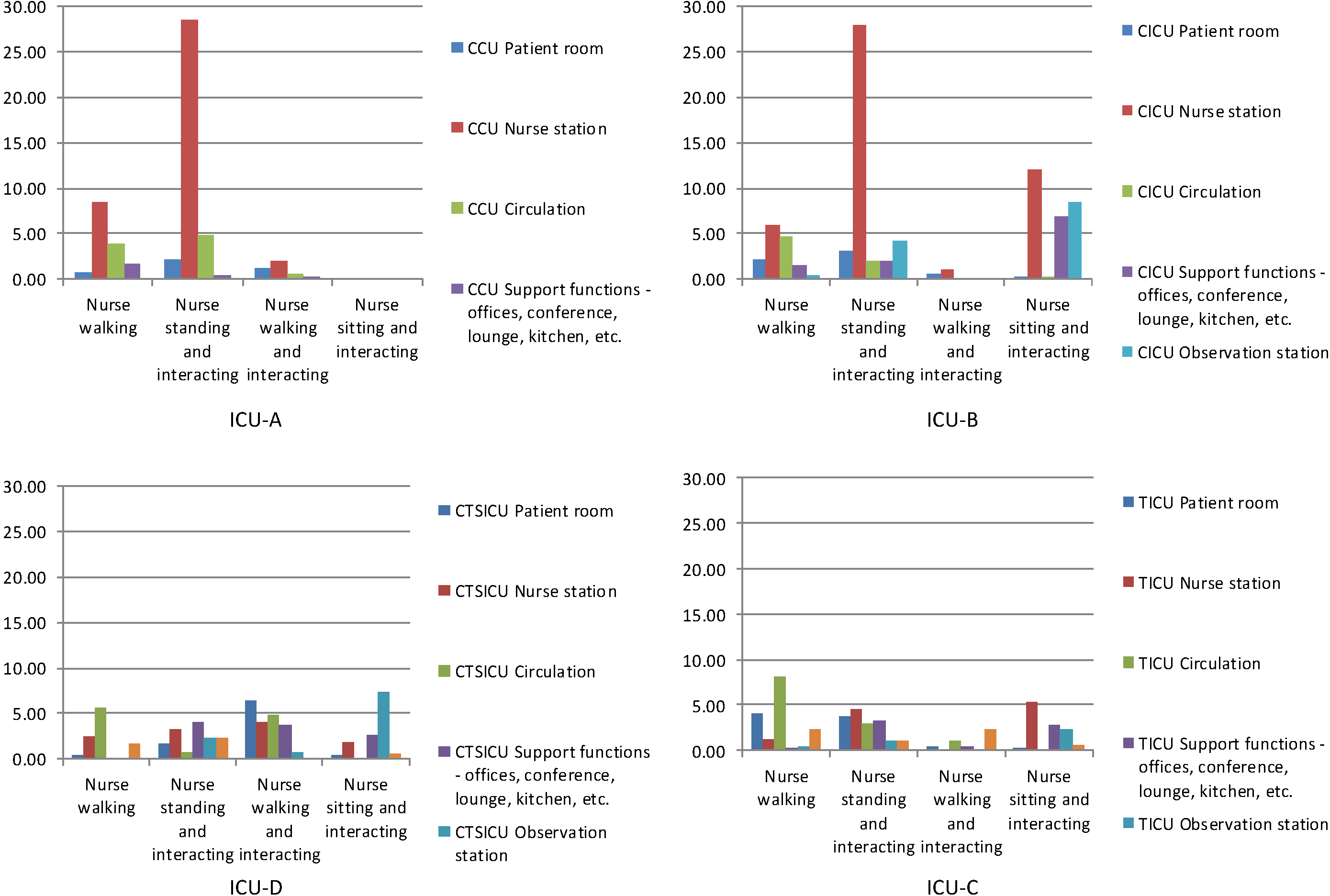
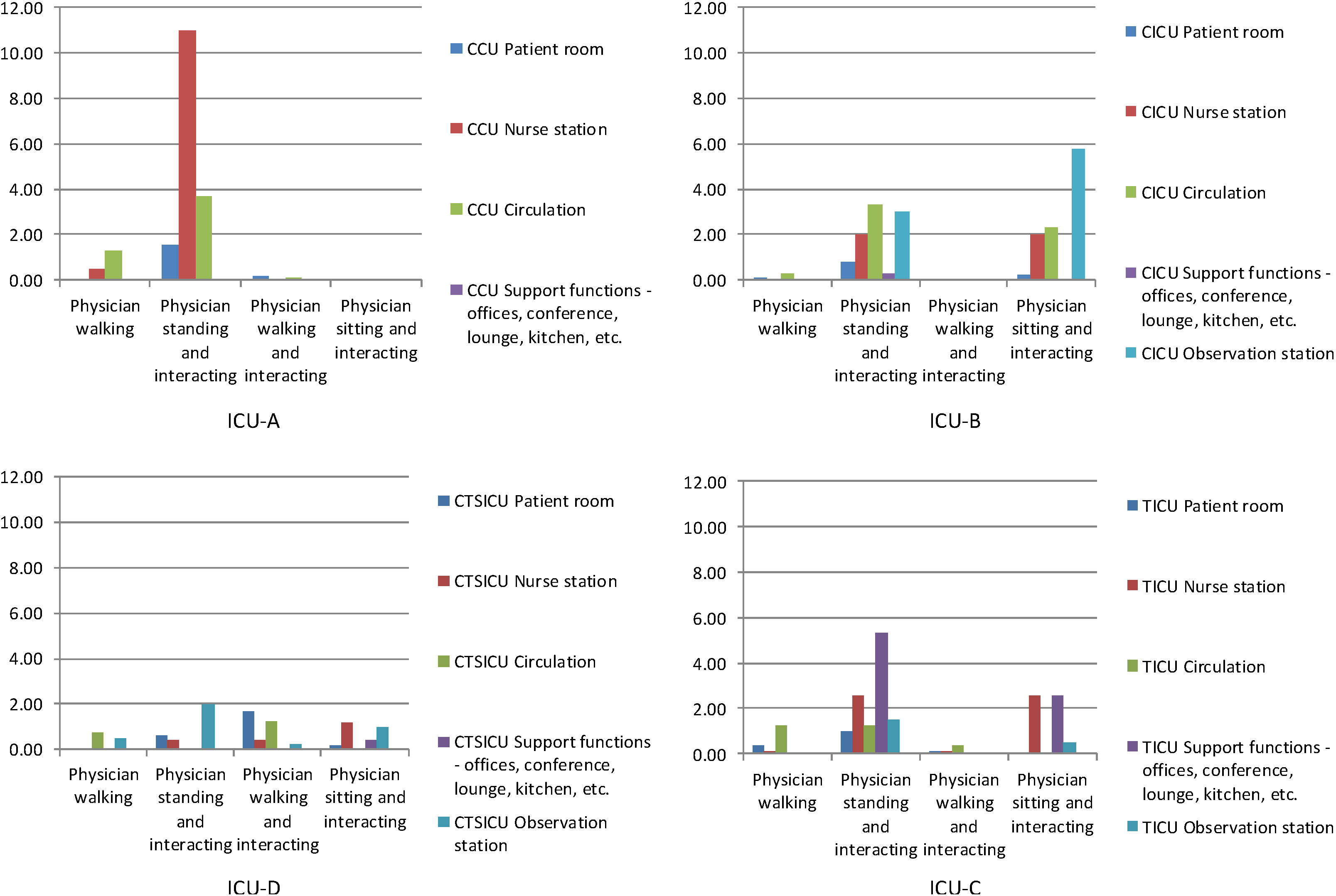
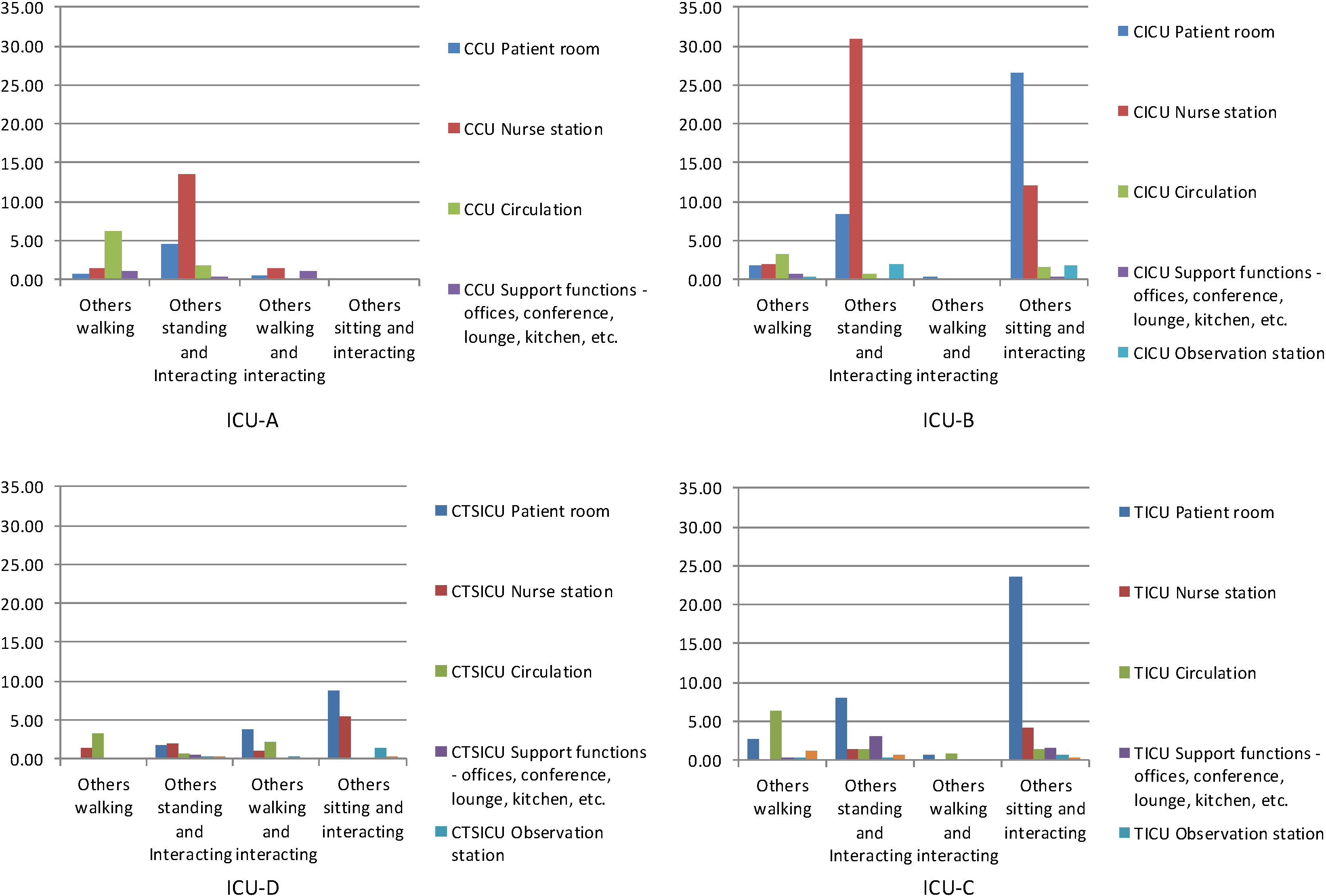
The four ICUs included in the study were different in terms specialty type, layout, shape, size, and composition. Therefore, it was hypothesized that the patterns of distribution of interaction-related behaviors in these units would be different. The findings of the observational study confirmed the hypothesis. In general, “standing and interacting” behaviors among different population groups—nurses, physicians, and others—were concentrated in one or two areas such as the nurse stations in ICU-A and ICU-B. In contrast, these behaviors were distributed over several areas in ICU-D and ICU-C. These differences in the distribution patterns of “standing and interacting” behaviors might have been due to the nature of clinical care given to patients in these units. In ICU-A and ICU-B, care regimens are relatively routinized and predictable. As result, “standing and interacting” occurred more predictably in some areas of ICU-A and ICU-B. In contrast, “standing and interacting” occurred more randomly in ICU-D and ICU-C patients in relation to more unpredictable and less routinized care regimens. However, it is also possible that ICU-D (16-bed) and ICU-C (14-bed) provided more opportunities for interaction than ICU-A (12-bed) and ICU-B (8-bed), simply because they were larger. This would then raise many interesting questions, such as: How much of the observed variations in behavioral patterns were due to the specialty type of these ICUs and how much due to their differences in size? Is it possible that at a certain threshold defined by unit size we would always expect a significant change in the distribution of interaction-related behaviors regardless of unit specialty? If so, where is this threshold? Is it always found between 12 and 14 as was observed in this study, or can this change in distribution also be found for other sizes? Is it possible that the differences in interaction-related behavior occur only due to the differences in specialty types, and that such differences have nothing to do with the size of a unit? Again, more studies on more ICUs of different specialty types and sizes are needed to answer these questions.
4.3. Correlational Analysis
The findings of the correlational analysis indicated many consistent relationships between network measures and interaction-related behaviors in these ICUs despite unit differences and differences in the distribution patterns of the behaviors.
Among other things, the findings showed that when nurses and physicians spent time “sitting and interacting” in these units they chose locations with higher axial integration (i.e., axial lines with better global environmental visibility and accessibility), probably to help maintain a level of environmental awareness that was required in the intense environment of ICUs.
The findings also showed that correlations between “sitting and interacting” and axial integration were stronger in circulation spaces and nurse stations than they were at the unit level suggesting an interaction effect of these of spaces on the relationship. The interaction effect might have been due to any additional “sitting and interacting” behaviors generated by the observation stations that were located along circulation spaces, and by the technology and furniture that were available in the nurse stations of these ICUs.
In addition, the findings also showed that axial integration was negatively correlated with “walking and interacting” among nurses, and node integration was negatively correlated with “walking” among nurses. These findings contradicted our expectations that dynamic behaviors would be positively correlated with axial integration, and static behaviors would be positively correlated with node integration. Instead, they support a more general idea that “walking” or “walking and interacting” among nurses occurred less in more globally connected spaces regardless of whether the network was defined by functionally distinct spaces or by a set of axial lines.
Interesting, however, was the fact that “walking” among nurses, physicians and others was negatively correlated with node integration, but was positively correlated with node control. In other words, everyone in ICUs walked more in those spaces that provided better control over neighboring spaces, and less in those that provided better global visibility and accessibility. Though the findings were unexpected, the reason for this could have been that everyone in ICUs was generally more interested in taking opportunities that became available in neighboring spaces and therefore walked more in spaces with higher node control. Examples of such opportunities may include asking the physician or the nurse a question who is attending a patient next door, or seeking help of a nurse who is working on a computer in a nearby space. Taking advantages of such opportunities generally are easier from spaces with higher node control, simply because these spaces have better control over the neighboring spaces.
Finally, network measures had different relationships with interaction-related behaviors in different categories of spaces. For example, axial integration had no relationship with interaction-related behaviors in patient rooms; node control had no relationship with the behaviors in nurse stations; and node integration and control had very weak relationships with the behaviors in circulation spaces. Except for the fact that axial integration had positive correlations with “sitting and interacting” among nurses and physicians, network measures also had different correlations with interaction-related behaviors among different population categories. In simple words, the relationships of network measures with interaction-related behaviors depended on both spatial characteristics and population category.
5. Conclusions
This study looked at the effects of the network properties of spaces on the interaction-related behaviors among different user groups in four ICUs of different size, shape, layout, and specialty type. Systematic field observations showed significant differences in the spatial distribution of interaction-related behaviors in the ICUs. Yet, several consistent relationships between interaction-related behaviors and environmental accessibility and visibility defined using different local and global network measures were found. A remarkable degree of similarity in environmental visibility and accessibility among different categories of spaces in these units, as was shown in the rank order of the network measures of these spaces, could have been one of the reasons why interaction-related behaviors showed consistent relationships with network measures in these units. This is important in light of the fact that the need for better environmental visibility and accessibility for efficient and effective patient care may not diminish in ICUs in the near future, even though shifts in patient profiles, care delivery models, technology, labor force, etc. will continue to change how critical care is provided in ICUs.
It is also important to note here that despite any structural similarities and any consistent relationships between network measures and interaction-related behaviors in the ICUs, spatial distribution patterns of interaction-related behaviors of different user groups were different in different ICUs. In other words, different categories of users used spaces differently for their interactions in these units with somewhat similar structures of spatial networks. The findings, therefore, suggest that even though some commonly held programmatic knowledge is embedded in spatial networks in a similar way in different ICUs, such embedding is flexible enough to accommodate functional variations among different user groups. They also suggest that design interventions that require no changes in spatial network can be used to encourage or discourage interaction-related behaviors in ICU spaces.
To conclude, this study linking network properties of spaces to interaction-related behaviors in ICUs provides support for the importance network properties for behavior and psychological responses in nursing units. It also provides support for the concept of environmental affordance, for it shows many consistent relationships between objectively defined spatial network measures and interaction-related behaviors in ICUs despite unit differences and differences in the distribution patterns of the behaviors. Among them are the fact that spatial networks were used different user groups to maintain environmental awareness in ICUs; that certain network measures remained unchanged for certain categories of spaces in every ICU; and that the affordance of spaces with same network properties were often enhanced using additional furniture and fixtures to improve interaction-related behaviors.
Despite its contributions, the limitations of the study are clear. Even though the study included more interaction-related behaviors than any previous studies in nursing units using space syntax techniques, the data were limited to who participated in these interactions, where they participated, how frequently they participated, and what they did (moving, sitting, or standing) as they interacted. In future studies, it would be necessary to learn when, why, and for how long they participated in these interactions related behaviors. Observing when interactions occur should help us learn if some interaction-related behaviors are dependent on the time of the day. Knowing why interactions occur may help us learn their purpose and type. Some interactions are social in nature, while others are task-related. Some interactions are interruptions, while others are not. Knowing the durations of interactions may help us determine their spatial and technological needs. While shorter interactions can easily occur in corridors, longer interactions may require dedicated spaces.
With regard to space syntax techniques and measures, this study used only a few of many that are available. Each of these techniques and measures describes different aspects of spatial networks. Already in previous studies, visibility graph analysis (VGA) and targeted visibility analysis have shown usefulness for behavioral and psychological studies in nursing units. In future studies, it would be necessary to study the usefulness of these other techniques and measures for interaction-related behaviors in nursing units.
Finally, a few words need to be said on the bivariate correlation analysis used here to detect the relationship between a network variable and the frequency of an interaction-related behavior in ICUs. Though the analysis helped quantify the strength of the linear relationship between any two variables, in the future one should consider regression models to see if the frequency of an interaction-related behavior can be predicted by one or more spatial network variables. In addition, though the data were analyzed based on space and population categories to eliminate possible inflation in correlation due to subgroup effects, future studies should also consider gender, education, experience, and/or age to eliminate additional grouping effects within space and population categories.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}