
Brain Network Abnormalities in Obsessive–Compulsive Disorder: Insights from Edge Functional Connectivity Analysis
 ,
, 
Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Data Acquisition
2.3. Functional Imaging Data Preprocessing
2.4. Clinical Assessments
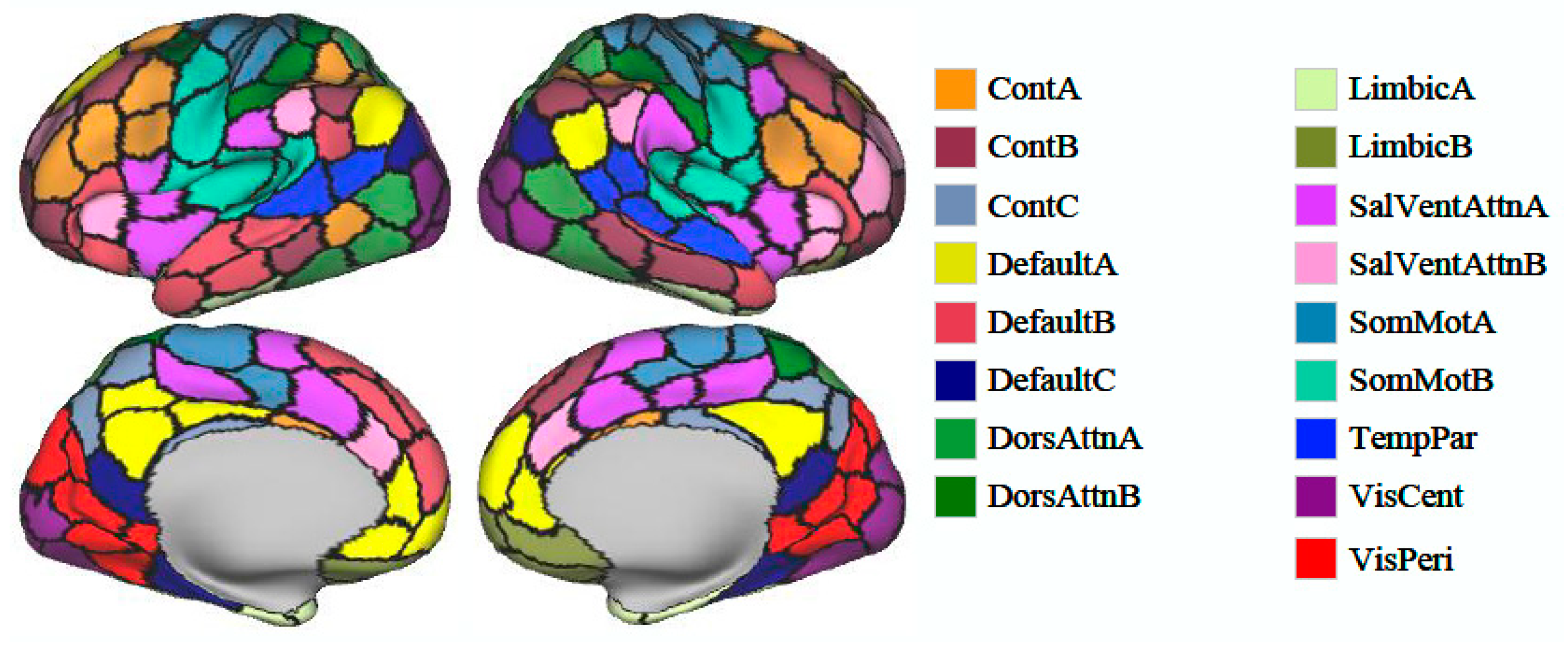
2.5. Brain Parcellation and Intrinsic Connectivity Network Analysis
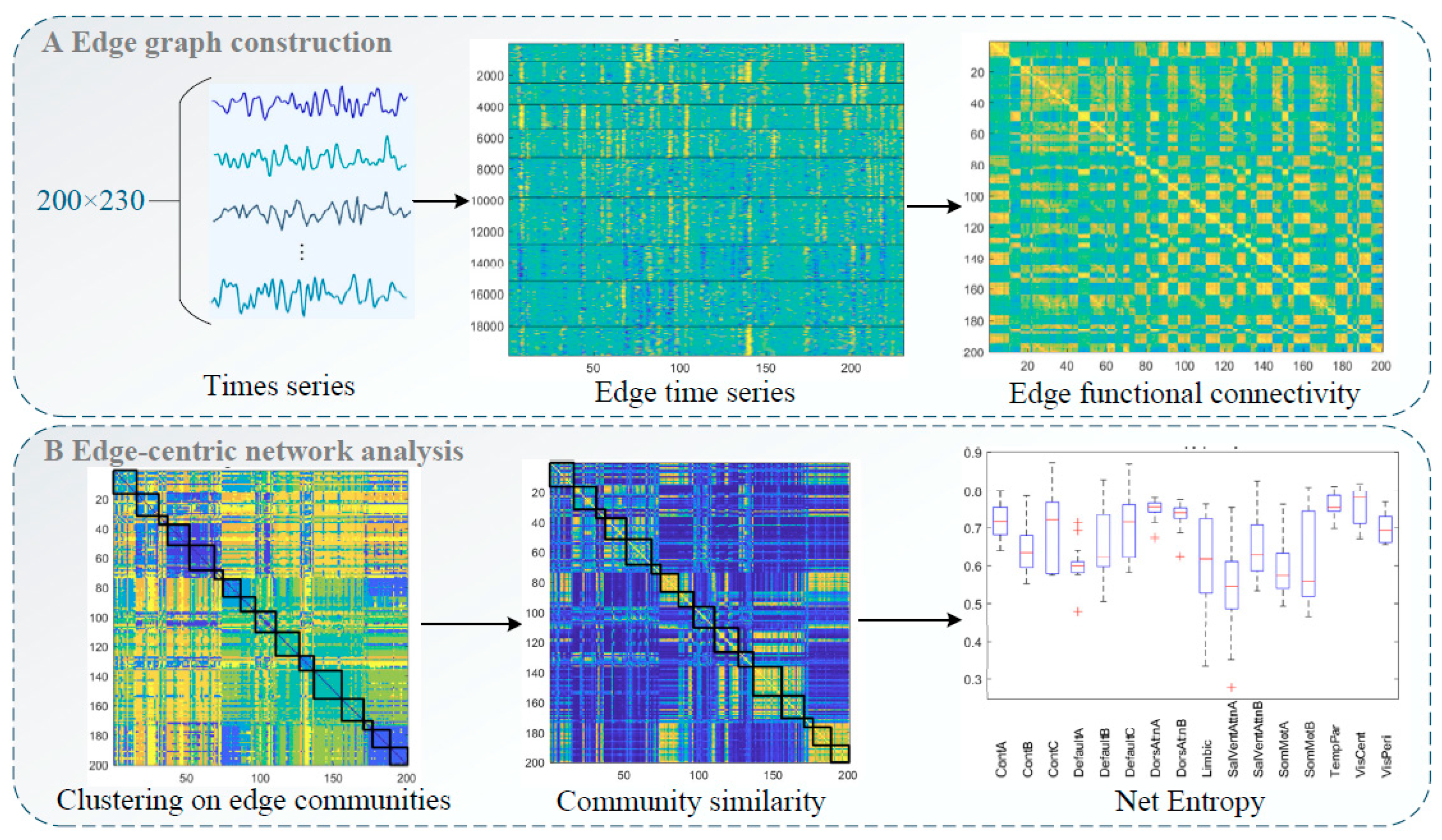
2.5.1. Edge Graph Construction
2.5.2. Entropy Calculation
2.5.3. Community Similarity Calculation
2.6. Statistical Analysis
3. Results
3.1. Participants’ Demographic and Clinical Characteristics
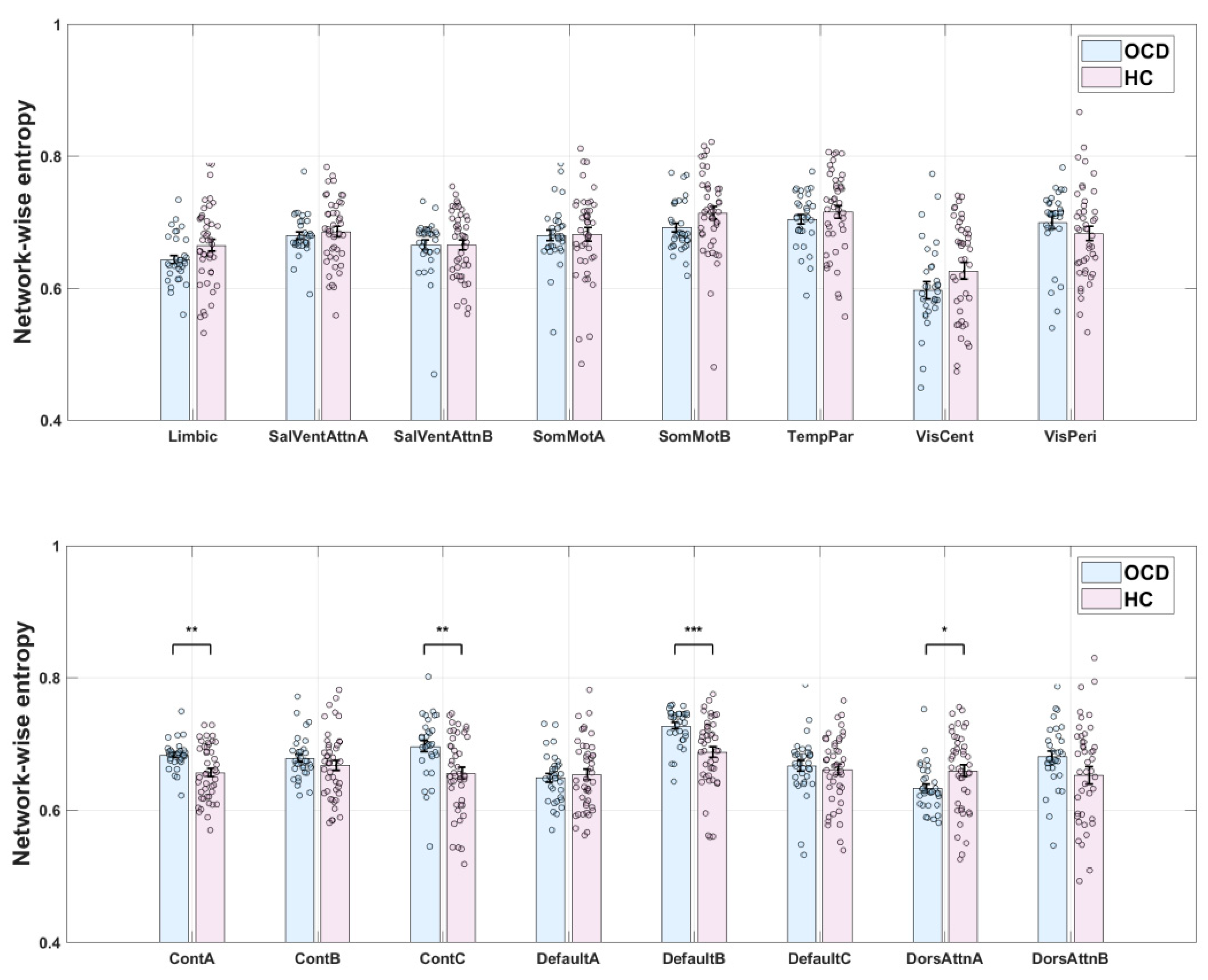
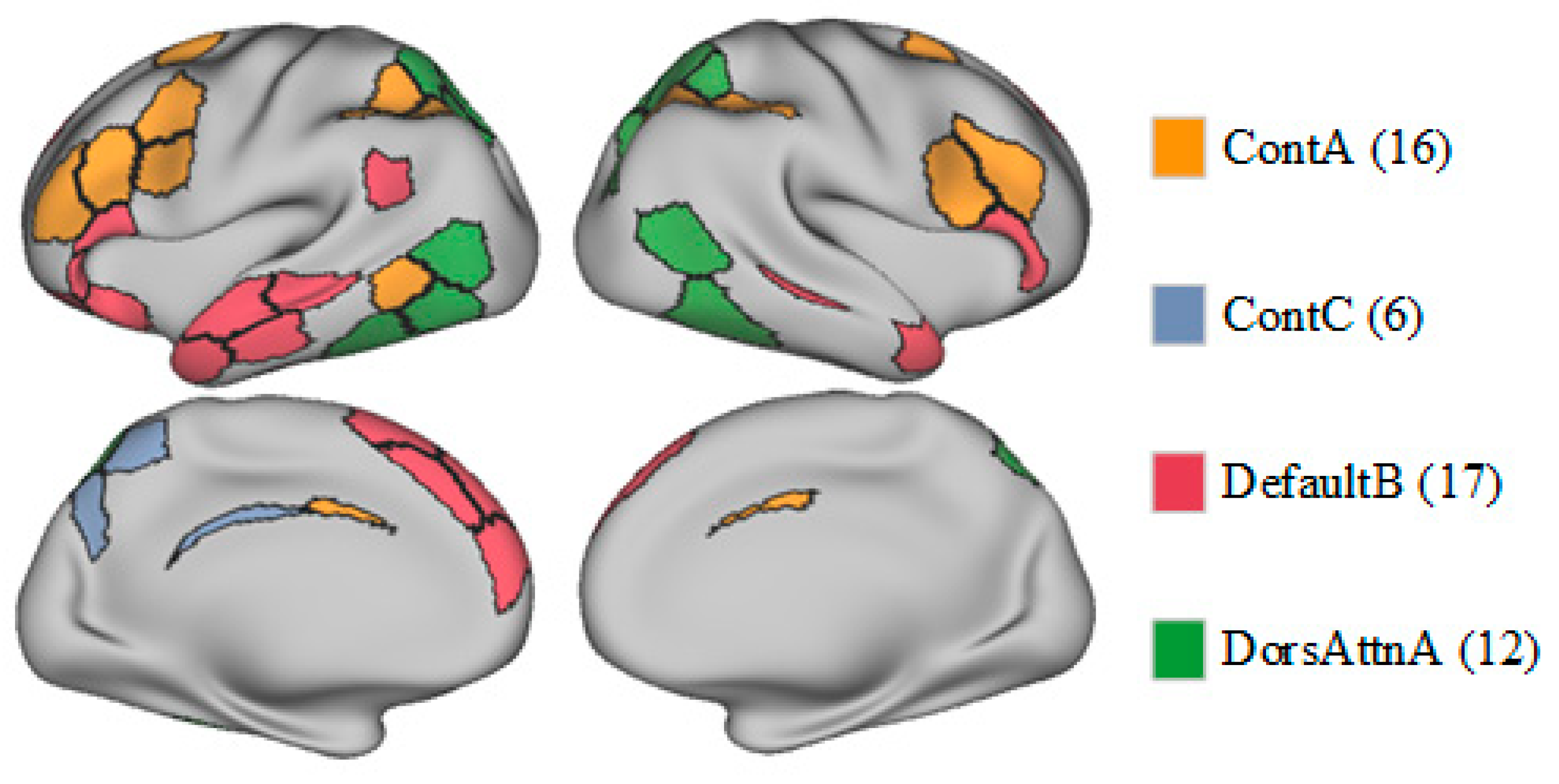
3.2. Group Differences in eFC and Entropy
4. Discussion
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aron, A. R., Durston, S., Eagle, D. M., Logan, G. D., Stinear, C. M., & Stuphorn, V. (2007). Converging evidence for a fronto-basal-ganglia network for inhibitory control of action and cognition. Journal of Neuroscience, 27(44), 11860–11864. [Google Scholar] [CrossRef]
- Bakay, H., Ulasoglu-Yildiz, C., Kurt, E., Demiralp, T., & Tükel, R. (2024). Hyperconnecitivity between dorsal attention and frontoparietal networks predicts treatment response in obsessive-compulsive disorder. Psychiatry Research: Neuroimaging, 337, 111763. [Google Scholar] [CrossRef] [PubMed]
- Baldermann, J. C., Schüller, T., Kohl, S., Voon, V., Li, N., Hollunder, B., Figee, M., Haber, S. N., Sheth, S. A., Mosley, P. E., Huys, D., Johnson, K. A., Butson, C., Ackermans, L., van der Vlis, T. B., Leentjens, A. F., Barbe, M., Visser-Vandewalle, V., Kuhn, J., … Horn, A. (2021). Connectomic deep brain stimulation for obsessive-compulsive disorder. Biological Psychiatry, 90(10), 678–688. [Google Scholar] [CrossRef] [PubMed]
- Bardella, G., Giuffrida, V., Giarrocco, F., Brunamonti, E., Pani, P., & Ferraina, S. (2024). Response inhibition in pre-motor cortex corresponds to a complex reshuffle of the mesoscopic information network. Network Neuroscience, 8(2), 597–622. [Google Scholar] [CrossRef] [PubMed]
- Becker, H. C., Beltz, A. M., Himle, J. A., Abelson, J. L., Block, S. R., Taylor, S. F., & Fitzgerald, K. D. (2024). Changes in brain network connections after exposure and response prevention therapy for obsessive-compulsive disorder in adolescents and adults. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 9(1), 70–79. [Google Scholar] [CrossRef]
- Becker, H. C., Norman, L. J., Yang, H., Monk, C. S., Phan, K. L., Taylor, S. F., Liu, Y., Mannella, K., & Fitzgerald, K. D. (2023). Disorder-specific cingulo-opercular network hyperconnectivity in pediatric OCD relative to pediatric anxiety. Psychological Medicine, 53(4), 1468–1478. [Google Scholar] [CrossRef]
- Beucke, J. C., Sepulcre, J., Eldaief, M. C., Sebold, M., Kathmann, N., & Kaufmann, C. (2014). Default mode network subsystem alterations in obsessive–compulsive disorder. The British Journal of Psychiatry, 205(5), 376–382. [Google Scholar] [CrossRef]
- Bosc, M., Bioulac, B., Langbour, N., Nguyen, T. H., Goillandeau, M., Dehay, B., Burbaud, P., & Michelet, T. (2017). Checking behavior in rhesus monkeys is related to anxiety and frontal activity. Scientific Reports, 7(1), 45267. [Google Scholar] [CrossRef]
- Brown, M. R., Benoit, J. R., Juhás, M., Dametto, E., Tse, T. T., MacKay, M., Sen, B., Carroll, A. M., Hodlevskyy, O., Silverstone, P. H., Dolcos, F., Dursun, S. M., & Greenshaw, A. J. (2015). fMRI investigation of response inhibition, emotion, impulsivity, and clinical high-risk behavior in adolescents. Frontiers in Systems Neuroscience, 9, 124. [Google Scholar] [CrossRef]
- Bruin, W. B., Denys, D., & van Wingen, G. (2019). Diagnostic neuroimaging markers of obsessive-compulsive disorder: Initial evidence from structural and functional MRI studies. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 91, 49–59. [Google Scholar] [CrossRef]
- Bruin, W. B., Taylor, L., Thomas, R. M., Shock, J. P., Zhutovsky, P., Abe, Y., Alonso, P., Ameis, S. H., Anticevic, A., Arnold, P. D., Assogna, F., Benedetti, F., Beucke, J. C., Boedhoe, P. S. W., Bollettini, I., Bose, A., Brem, S., Brennan, B. P., Buitelaar, J. K., … van Wingen, G. A. (2020). Structural neuroimaging biomarkers for obsessive-compulsive disorder in the ENIGMA-OCD consortium: Medication matters. Translational Psychiatry, 10(1), 342. [Google Scholar] [CrossRef] [PubMed]
- Buschman, T. J., & Miller, E. K. (2007). Top-down versus bottom-up control of attention in the prefrontal and posterior parietal cortices. Science, 315(5820), 1860–1862. [Google Scholar] [CrossRef] [PubMed]
- Chumin, E. J., Faskowitz, J., Esfahlani, F. Z., Jo, Y., Merritt, H., Tanner, J., Cutts, S. A., Pope, M., Betzel, R., & Sporns, O. (2022). Cortico-subcortical interactions in overlapping communities of edge functional connectivity. NeuroImage, 250, 118971. [Google Scholar] [CrossRef] [PubMed]
- Criaud, M., Wardak, C., Ben Hamed, S., Ballanger, B., & Boulinguez, P. (2012). Proactive inhibitory control of response as the default state of executive control. Frontiers in Psychology, 3, 59. [Google Scholar] [CrossRef]
- Cui, G., Ou, Y., Chen, Y., Lv, D., Jia, C., Zhong, Z., Yang, R., Wang, Y., Meng, X., Cui, H., Li, C., Sun, Z., Wang, X., Guo, W., & Li, P. (2020). Altered global brain functional connectivity in drug-naive patients with obsessive-compulsive disorder. Frontiers in Psychiatry, 11, 98. [Google Scholar] [CrossRef]
- De Wit, S. J., Van Der Werf, Y. D., Mataix-Cols, D., Trujillo, J. P., Van Oppen, P., Veltman, D. J., & Van Den Heuvel, O. A. (2015). Emotion regulation before and after transcranial magnetic stimulation in obsessive compulsive disorder. Psychological Medicine, 45(14), 3059–3073. [Google Scholar] [CrossRef]
- Diesburg, D. A., & Wessel, J. R. (2021). The Pause-then-Cancel model of human action-stopping: Theoretical considerations and empirical evidence. Neuroscience & Biobehavioral Reviews, 129, 17–34. [Google Scholar] [CrossRef]
- Faskowitz, J., Esfahlani, F. Z., Jo, Y., Sporns, O., & Betzel, R. F. (2020). Edge-centric functional network representations of human cerebral cortex reveal overlapping system-level architecture. Nature Neuroscience, 23(12), 1644–1654. [Google Scholar] [CrossRef]
- Fitzgerald, K. D., Schroder, H. S., & Marsh, R. (2021). Cognitive control in pediatric obsessive-compulsive and anxiety disorders: Brain-behavioral targets for early intervention. Biological Psychiatry, 89(7), 697–706. [Google Scholar] [CrossRef]
- Foa, E. B., Huppert, J. D., Leiberg, S., Langner, R., Kichic, R., Hajcak, G., & Salkovskis, P. M. (2002). The Obsessive-Compulsive Inventory: Development and validation of a short version. Psychological Assessment, 14(4), 485. [Google Scholar] [CrossRef]
- Fornaro, S., & Vallesi, A. (2024). Functional connectivity abnormalities of brain networks in obsessive–compulsive disorder: A systematic review. Current Psychology, 43(1), 900–930. [Google Scholar] [CrossRef]
- Geffen, T., Smallwood, J., Finke, C., Olbrich, S., Sjoerds, Z., & Schlagenhauf, F. (2022). Functional connectivity alterations between default mode network and occipital cortex in patients with obsessive-compulsive disorder (OCD). NeuroImage: Clinical, 33, 102915. [Google Scholar] [CrossRef] [PubMed]
- Ghani, U., Signal, N., Niazi, I. K., & Taylor, D. (2020). ERP based measures of cognitive workload: A review. Neuroscience & Biobehavioral Reviews, 118, 18–26. [Google Scholar] [CrossRef]
- Giuffrida, V., Marc, I. B., Ramawat, S., Fontana, R., Fiori, L., Bardella, G., Fagioli, S., Ferraina, S., Brunamonti, E., & Pani, P. (2023). Reward prospect affects strategic adjustments in stop signal task. Frontiers in Psychology, 14, 1125066. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, Ó. F., Carvalho, S., Leite, J., Fernandes-Goncalves, A., Carracedo, A., & Sampaio, A. (2016). Cognitive and emotional impairments in obsessive–compulsive disorder: Evidence from functional brain alterations. Porto Biomedical Journal, 1(3), 92–105. [Google Scholar] [CrossRef]
- Gonçalves, Ó. F., Soares, J. M., Carvalho, S., Leite, J., Ganho-Ávila, A., Fernandes-Gonçalves, A., Pocinho, F., Carracedo, A., & Sampaio, A. (2017). Patterns of default mode network deactivation in obsessive compulsive disorder. Scientific Reports, 7(1), 44468. [Google Scholar] [CrossRef]
- Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Fleischmann, R. L., Hill, C. L., Heninger, G. R., & Charney, D. S. (1989). The Yale-Brown obsessive compulsive scale: I. Development, use, and reliability. Archives of General Psychiatry, 46(11), 1006–1011. [Google Scholar] [CrossRef]
- Graat, I., Balke, S., Prinssen, J., de Koning, P., Vulink, N., Mocking, R., & Denys, D. (2022). Effectiveness and safety of deep brain stimulation for patients with refractory obsessive compulsive disorder and comorbid autism spectrum disorder; a case series. Journal of Affective Disorders, 299, 492–497. [Google Scholar] [CrossRef]
- Grant, K. A., Newman, N., Lynn, C., Davenport, C., Gonzales, S., Carlson, V. C. C., & Kroenke, C. D. (2022). Brain functional connectivity mapping of behavioral flexibility in rhesus monkeys. Journal of Neuroscience, 42(24), 4867–4878. [Google Scholar] [CrossRef]
- Halvorsen, M., Samuels, J., Wang, Y., Greenberg, B. D., Fyer, A. J., McCracken, J. T., Geller, D. A., Knowles, J. A., Zoghbi, A. W., Pottinger, T. D., Grados, M. A., Riddle, M. A., Bienvenu, O. J., Nestadt, P. S., Krasnow, J., Goes, F. S., Maher, B., Nestadt, G., & Goldstein, D. B. (2021). Exome sequencing in obsessive–compulsive disorder reveals a burden of rare damaging coding variants. Nature Neuroscience, 24(8), 1071–1076. [Google Scholar] [CrossRef]
- Harrison, B. J., Soriano-Mas, C., Pujol, J., Ortiz, H., López-Solà, M., Hernández-Ribas, R., Deus, J., Alonso, P., Yücel, M., Pantelis, C., Menchon, J. M., & Cardoner, N. (2009). Altered corticostriatal functional connectivity in obsessive-compulsive disorder. Archives of General Psychiatry, 66(11), 1189–1200. [Google Scholar] [CrossRef] [PubMed]
- Herzog, S. A., & Brakoulias, V. (2022). The role of neurophysiological biomarkers in obsessive-compulsive disorder. Current Medicinal Chemistry, 29(35), 5584–5594. [Google Scholar] [CrossRef]
- Inventory-Ii, B. D. (2010). Beck depression inventory-II. Corsini Encyclopedia of Psychology, 1(1), 210. [Google Scholar]
- Jacoby, N., Bruneau, E., Koster-Hale, J., & Saxe, R. (2016). Localizing pain matrix and theory of mind networks with both verbal and non-verbal stimuli. NeuroImage, 126, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Jana, S., Gopal, A., & Murthy, A. (2021). Computational mechanisms mediating inhibitory control of coordinated eye-hand movements. Brain Sciences, 11(5), 607. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X., Li, X., Xing, H., Huang, X., Xu, X., & Li, J. (2021). Brain entropy study on obsessive-compulsive disorder using resting-state fMRI. Frontiers in Psychiatry, 12, 764328. [Google Scholar] [CrossRef]
- Keshmiri, S. (2020). Entropy and the brain: An overview. Entropy, 22(9), 917. [Google Scholar] [CrossRef]
- Kong, R., Yang, Q., Gordon, E., Xue, A., Yan, X., Orban, C., Zuo, X., Spreng, N., Ge, T., Holmes, A., Eickhoff, S., & Yeo, B. T. (2021). Individual-specific areal-level parcellations improve functional connectivity prediction of behavior. Cerebral Cortex, 31(10), 4477–4500. [Google Scholar] [CrossRef]
- Kopřivová, J., Congedo, M., Horáček, J., Praško, J., Raszka, M., Brunovský, M., Kohútová, B., & Höschl, C. (2011). EEG source analysis in obsessive–compulsive disorder. Clinical Neurophysiology, 122(9), 1735–1743. [Google Scholar] [CrossRef]
- Liu, Q., Gao, F., Wang, X., Xia, J., Yuan, G., Zheng, S., Zhong, M., & Zhu, X. (2023). Cognitive inflexibility is linked to abnormal frontoparietal-related activation and connectivity in obsessive-compulsive disorder. Human Brain Mapping, 44(16), 5460–5470. [Google Scholar] [CrossRef]
- Maatoug, R., Goff, B. L., Rotge, J. Y., Jaafari, N., Guillin, O., & Millet, B. (2019). Performance in delayed non-matching to sample task predicts the diagnosis of obsessive–compulsive disorder. Translational Psychiatry, 9(1), 338. [Google Scholar] [CrossRef]
- Masharipov, R., Korotkov, A., Knyazeva, I., Cherednichenko, D., & Kireev, M. (2023). Impaired non-selective response inhibition in obsessive-compulsive disorder. International Journal of Environmental Research and Public Health, 20(2), 1171. [Google Scholar] [CrossRef]
- McLaughlin, N. C., Kirschner, J., Foster, H., O’Connell, C., Rasmussen, S. A., & Greenberg, B. D. (2016). Stop signal reaction time deficits in a lifetime obsessive-compulsive disorder sample. Journal of the International Neuropsychological Society, 22(7), 785–789. [Google Scholar] [CrossRef]
- Norman, L. J., Carlisi, C., Lukito, S., Hart, H., Mataix-Cols, D., Radua, J., & Rubia, K. (2016). Structural and functional brain abnormalities in attention-deficit/hyperactivity disorder and obsessive-compulsive disorder: A comparative meta-analysis. JAMA Psychiatry, 73(8), 815–825. [Google Scholar] [CrossRef] [PubMed]
- Pani, P., Menghini, D., Napolitano, C., Calcagni, M., Armando, M., Sergeant, J. A., & Vicari, S. (2013). Proactive and reactive control of movement are differently affected in attention deficit hyperactivity disorder children. Research in Developmental Disabilities, 34(10), 3104–3111. [Google Scholar] [CrossRef]
- Peng, Z. W., Xu, T., He, Q. H., Shi, C. Z., Wei, Z., Miao, G. D., Jing, J., Lim, K. O., Zuo, X. N., & Chan, R. C. K. (2014). Default network connectivity as a vulnerability marker for obsessive compulsive disorder. Psychological Medicine, 44(7), 1475–1484. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z. W., Yang, W. H., Miao, G. D., Jing, J., & Chan, R. C. (2011). The Chinese version of the Obsessive-Compulsive Inventory-Revised scale: Replication and extension to non-clinical and clinical individuals with OCD symptoms. BMC Psychiatry, 11, 129. [Google Scholar] [CrossRef]
- Perera, M. P. N., Mallawaarachchi, S., Bailey, N. W., Murphy, O. W., & Fitzgerald, P. B. (2023). Obsessive–compulsive disorder (OCD) is associated with increased engagement of frontal brain regions across multiple event-related potentials. Psychological Medicine, 53(15), 7287–7299. [Google Scholar] [CrossRef]
- Pickenhan, L., & Milton, A. L. (2024). Preclinical animal models and assays of neuropsychiatric disorders: Old problems and new vistas. Cognitive, Affective & Behavioral Neuroscience, 24(2), 187–190. [Google Scholar] [CrossRef]
- Posner, J., Song, I., Lee, S., Rodriguez, C. I., Moore, H., Marsh, R., & Blair Simpson, H. (2017). Increased functional connectivity between the default mode and salience networks in unmedicated adults with obsessive-compulsive disorder. Human Brain Mapping, 38(2), 678–687. [Google Scholar] [CrossRef]
- Renzi, D. A. (1985). State-trait anxiety inventory. Measurement and Evaluation in Counseling and Development, 18(2), 86–89. [Google Scholar] [CrossRef]
- Ruchsow, M., Reuter, K., Hermle, L., Ebert, D., Kiefer, M., & Falkenstein, M. (2007). Executive control in obsessive-compulsive disorder: Event-related potentials in a Go/Nogo task. Journal of Neural Transmission, 114, 1595–1601. [Google Scholar] [CrossRef]
- Saad, Z. S., Gotts, S. J., Murphy, K., Chen, G., & Cox, R. W. (2012). Trouble at rest: How correlation patterns and group differences become distorted after global signal regression. Brain Connectivity, 2(1), 25–32. [Google Scholar] [CrossRef]
- Siddeswara, L. B., Sravanti, L., Sachin, N., & Girimaji, S. C. (2021). Very early-onset Obsessive-Compulsive Disorder in pre-schoolers: A prospective case series. Asian Journal of Psychiatry, 65, 102857. [Google Scholar] [CrossRef]
- Stern, E. R., Muratore, A. F., Taylor, S. F., Abelson, J. L., Hof, P. R., & Goodman, W. K. (2017). Switching between internally and externally focused attention in obsessive-compulsive disorder: Abnormal visual cortex activation and connectivity. Psychiatry Research: Neuroimaging, 265, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, H., Murayama, K., Nemoto, K., Tomita, M., Hasuzawa, S., Mizobe, T., Kato, K., Ohno, A., Tsuruta, S., Togao, O., Hiwatashi, A., & Nakao, T. (2022). Increased functional connectivity between presupplementary motor area and inferior frontal gyrus associated with the ability of motor response inhibition in obsessive–compulsive disorder. Human Brain Mapping, 43(3), 974–984. [Google Scholar] [CrossRef]
- Towey, J. P., Tenke, C. E., Bruder, G. E., Leite, P., Friedman, D., Liebowitz, M., & Hollander, E. (1994). Brain event-related potential correlates of overfocused attention in obsessive-compulsive disorder. Psychophysiology, 31(6), 535–543. [Google Scholar] [CrossRef] [PubMed]
- Uhre, V. F., Larsen, K. M., Herz, D. M., Baaré, W., Pagsberg, A. K., & Siebner, H. R. (2022). Inhibitory control in obsessive compulsive disorder: A systematic review and activation likelihood estimation meta-analysis of functional magnetic resonance imaging studies. NeuroImage: Clinical, 36, 103268. [Google Scholar] [CrossRef]
- Vaghi, M. M., Vértes, P. E., Kitzbichler, M. G., Apergis-Schoute, A. M., van der Flier, F. E., Fineberg, N. A., Sule, A., Zaman, R., Voon, V., Kundu, P., Bullmore, E. T., & Robbins, T. W. (2017). Specific frontostriatal circuits for impaired cognitive flexibility and goal-directed planning in obsessive-compulsive disorder: Evidence from resting-state functional connectivity. Biological Psychiatry, 81(8), 708–717. [Google Scholar] [CrossRef]
- Varley, T. F., Sporns, O., Schaffelhofer, S., Scherberger, H., & Dann, B. (2023). Information-processing dynamics in neural networks of macaque cerebral cortex reflect cognitive state and behavior. Proceedings of the National Academy of Sciences, 120(2), e2207677120. [Google Scholar] [CrossRef]
- Viol, K., Aas, B., Kastinger, A., Kronbichler, M., Schöller, H., Reiter, E.-M., & Schiepek, G. (2019). Individual OCD-provoking stimuli activate disorder-related and self-related neuronal networks in fMRI. Psychiatry Research: Neuroimaging, 283, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Wang, J., Wei, Z., Wang, H., Jiang, Z., & Peng, Z. (2015). Psychometric properties of the Chinese version of the Obsessive Beliefs Questionnaire-44 (OBQ-44). BMC Psychiatry, 15, 188. [Google Scholar] [CrossRef]
- Wheaton, M. G., Kalanthroff, E., Mandel, M., Marsh, R., & Simpson, H. B. (2025). Neurocognitive performance in obsessive-compulsive disorder before and after treatment with cognitive behavioral therapy. Journal of Behavior Therapy and Experimental Psychiatry, 87, 102019. [Google Scholar] [CrossRef] [PubMed]
- Yang, G. J., Murray, J. D., Glasser, M., Pearlson, G. D., Krystal, J. H., Schleifer, C., Repovs, G., & Anticevic, A. (2017). Altered global signal topography in schizophrenia. Cerebral Cortex, 27(11), 5156–5169. [Google Scholar] [CrossRef]
- Yu, J., Xu, Q., Ma, L., Huang, Y., Zhu, W., Liang, Y., Wang, Y., Tang, W., Zhu, C., & Jiang, X. (2024). Functional MRI-Specific Alternations in default mode network in obsessive–compulsive disorder: A voxel-based meta-analysis. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging. in press. [Google Scholar] [CrossRef]
- Zhai, R., Tong, G., Li, Z., Song, W., Hu, Y., Xu, S., Wei, Q., Zhang, X., Li, Y., Liao, B., Yuan, C., Fan, Y., Song, G., Ouyang, Y., Zhang, W., Tang, Y., Jin, M., Zhang, Y., Li, H., … Wang, Z. (2023). Rhesus monkeys exhibiting spontaneous ritualistic behaviors resembling obsessive-compulsive disorder. National Science Review, 10(11), nwad312. [Google Scholar] [CrossRef]
- Zhang, T., Wang, J., Yang, Y., Wu, Q., Li, B., Chen, L., Yue, Q., Tang, H., Yan, C., Lui, S., Huang, X., Chan, R. C. K., Zang, Y., He, Y., & Gong, Q. (2011). Abnormal small-world architecture of top–down control networks in obsessive–compulsive disorder. Journal of Psychiatry and Neuroscience, 36(1), 23–31. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Network | Function |
|---|---|
| Visual central network | Primarily the processing of central visual information |
| Visual peripheral network | Processing of peripheral visual information |
| Somatomotor network A | Involved in bodily sensation and motor control |
| Somatomotor network B | Related to bodily sensation and movement, potentially involving more specific motor or sensory regions |
| Dorsal Attention network A | Involved in the allocation and control of spatial attention |
| Dorsal Attention network B | Similar to network A, responsible for various attention tasks |
| Salience/ventral attention network A | Processng of the salience of external stimuli |
| Salience/ventral attention network B | May be involved in emotional and stimulus response processing |
| Limbic network | Associated with emotional processing and memory functions, handling of emotions and autonomic functions |
| Control network A | Cognitive control, decision making, and executive functions |
| Control network B | Similar to control network A, involved in various cognitive control tasks |
| Control network C | Associated with complex cognitive tasks and executive functions |
| Default mode network A | Involved in introspection, memory recall, and social cognition |
| Default mode network B | Involved in self-referential cognitive processes |
| Default mode network C | Involved in broader internal thought processes and memory |
| Temporoparietal network | Involved in social cognition, language processing, and multisensory integration |
| Characteristic | OCD | HC | p |
|---|---|---|---|
| n | 33 | 44 | - |
| Age (years) | 21.77 ± 7.79 | 21.11 ± 5.09 | 0.789 |
| Sex (female) | 9 | 20 | 0.103 |
| Onset age | 16.52 ± 5.66 | NA | - |
| Education (years) | 11.17 ± 1.41 | 13.95 ± 4.24 | <0.001 |
| Y-BOCS score | 12.26 ± 6.54 | 11.25 ± 5.35 | <0.001 |
| BDI score | 11.47 ± 11.41 | 10.99 ± 4.89 | <0.001 |
| STAI score | 86.43 ± 23.86 | 84.50 ± 14.44 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, Y.; Liu, H.; Liu, H.; Lin, D.; Wu, S.; Peng, Z. Brain Network Abnormalities in Obsessive–Compulsive Disorder: Insights from Edge Functional Connectivity Analysis. Behav. Sci. 2025, 15, 488. https://doi.org/10.3390/bs15040488
Xu Y, Liu H, Liu H, Lin D, Wu S, Peng Z. Brain Network Abnormalities in Obsessive–Compulsive Disorder: Insights from Edge Functional Connectivity Analysis. Behavioral Sciences. 2025; 15(4):488. https://doi.org/10.3390/bs15040488
Chicago/Turabian StyleXu, Yongwang, Hongfei Liu, Haiyan Liu, Defeng Lin, Sipeng Wu, and Ziwen Peng. 2025. "Brain Network Abnormalities in Obsessive–Compulsive Disorder: Insights from Edge Functional Connectivity Analysis" Behavioral Sciences 15, no. 4: 488. https://doi.org/10.3390/bs15040488
APA StyleXu, Y., Liu, H., Liu, H., Lin, D., Wu, S., & Peng, Z. (2025). Brain Network Abnormalities in Obsessive–Compulsive Disorder: Insights from Edge Functional Connectivity Analysis. Behavioral Sciences, 15(4), 488. https://doi.org/10.3390/bs15040488