
The Challenge Coping and Resilience of the Families of School-Aged Children with Autism Spectrum Disorder in China: A Qualitative Study


Abstract
1. Introduction
1.1. Autism Spectrum Disorder (ASD)
1.2. Families of Children with ASD
1.3. Resilience in Families of Individuals with ASD
1.4. Current Research
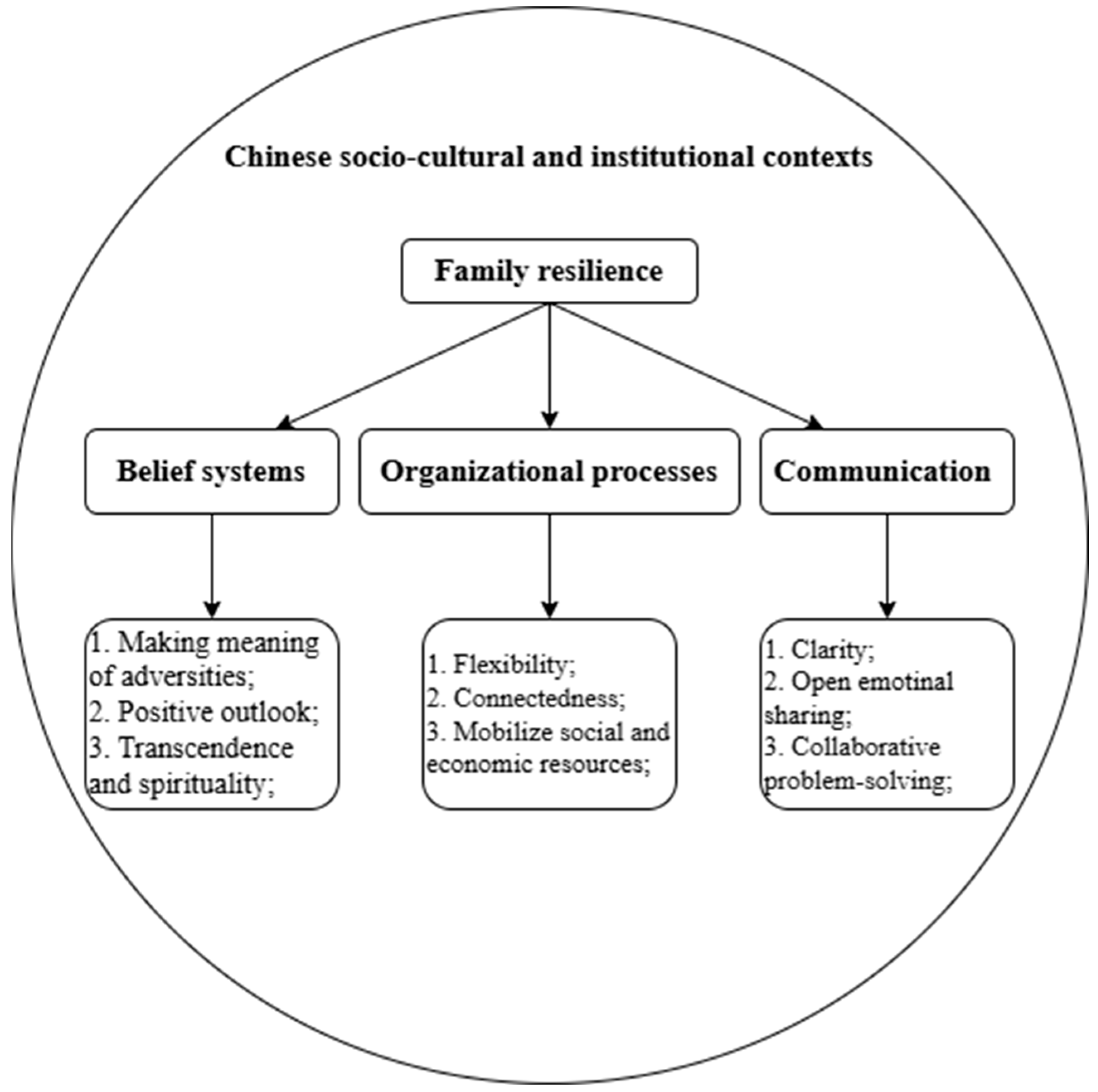
1.5. Theoretical Framework and Research Questions
2. Method
2.1. Research Design
2.2. Research Participants
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Main Challenges
3.1.1. Difficulties in Family Care
“I don’t know how much of each meal will fill him up, and several times he’s eaten until he vomits. Also, he’s growing taller and taller, and there’s no way I can control him effectively by myself anymore when he’s angry”.(1-1)
3.1.2. Parenting Burnout
“I sometimes just have a deep sense of powerlessness, feeling abandoned and isolated. The whole person is drained. When I come home from work, I don’t want to take care of the child or talk to anyone else in the family”.(3-1)
“Passing on the family line is of course important! I’ve told them many times to have another child while I’m still healthy and I’ll take care of him or her”.(8-2)
3.1.3. Educational Plights
“There is no special education school in my county, and I have contacted several ordinary schools and they all refused to enroll my child. So, I had to ask relatives and friends about schools in other places, and it took me months to settle on coming to the current school. In response, my wife and I have moved and looked for new jobs”.(7-2)
3.1.4. Inadequate Community Support Systems
“The community service center provides my child with an annual allowance of 500 RMB, and other than that, there is no other coverage. That’s not even enough money to cover half a month’s expenses for my child. My child sometimes has diarrhea and fever, and the community health center doesn’t dare to diagnose my child and tells us to go to a big hospital. The help they give us is very limited and not enough to relieve the pressure of us parents”.(8-1)
3.2. The Challenge Coping Process
3.2.1. Belief Systems
Emotional Adjustment: Accepting and Facing Reality
“The older the child gets, the more obvious some of the behavioral problems become. It doesn’t do us any good to keep fluke mind, it only deepens the pain. Instead, I have a sense of relief after truly recognizing and accepting that my child is different”.(6-1)
Cognitive Adjustment: Redefining Expectation
“It is not fair to the child or to us to continue to have great ambitions for our child. Holding on to such ideas will only lead to tragedy. We are content as long as our child is healthy and suffers no other pain. We’ll be there for him”.(4-1)
Behavior Adjustment: Self-Empowerment
“My child has ASD and there is no way for him to go through life like a normal child. But I won’t give up, I will do my best to support his rehabilitation, even if the progress is not obvious, I accept it. I learned some family intervention methods online and, by now, have been sticking to family intervention for 5 years. As a parent of a child with ASD, I think it’s the right thing to do. As long as he can stay healthy, I will be satisfied”.(2-1)
3.2.2. Organizational Processes
Adjustment of Intra-Household Labor Division
“It used to be that both kids were working and I was taking care of my grandson all by myself. Now, my grandson has grown up and I was unable to take care of him on my own. So, my daughter-in-law has taken the initiative to adjust her job, earning less each month but spending more time at home. She has given a lot to this family”.(3-2)
Adjustment of Family Decision-Making Patterns
“In the past, the children’s father and grandfather used to make all the decisions in the family. Now, when there is something important in the family, we discuss it together and then make decisions”.(5-2)
Mobilization of External Resources
“I’m too weak on my own. I joined an organization full of parents or grandparents etc. of children with ASD. We joined together to give advice to the Education Bureau, and they accepted it very quickly. Moreover, there are some government subsidies that many families wouldn’t know about if it wasn’t for the sharing of organization members”.(7-1)
3.2.3. Communication
Internal Communication: Reflection and Sharing
“I do self-reflection if I do something wrong. We have a hard enough time as a family. I communicate with my family if I am unhappy or happy about something, all to protect our family”.(7-2)
External Communication: Compromise and Patience
“Staying tough is not an option. We must remain patient enough and make appropriate compromises. We cannot expect all these security and welfare benefits to be provided in one step, and we have to take our time”.(2-1)
4. Discussion
5. Conclusions
6. Theoretical Contributions
7. Research Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Altiere, M. J., & von Kluge, S. (2009). Family functioning and coping behaviors in parents of children with autism. Journal of Child and Family Studies, 18(1), 83–92. [Google Scholar] [CrossRef]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders. American Psychiatric Association. [Google Scholar] [CrossRef]
- Bayat, M., & Schuntermann, P. (2013). Enhancing resilience in families of children with autism spectrum disorder. In Handbook of family resilience (pp. 409–424). Springer New York. [Google Scholar] [CrossRef]
- Bonis, S. (2016). Stress and parents of children with autism: A review of literature. Issues in Mental Health Nursing, 37(3), 153–163. [Google Scholar] [CrossRef] [PubMed]
- Central People’s Government of the People’s Republic of China. (2020, October 18). Law of the People’s Republic of China on the protection of minors. Available online: https://www.gov.cn/xinwen/2020-10/18/content_5552113.htm (accessed on 1 December 2024).
- Central People’s Government of the People’s Republic of China. (2021, October 29). Law of the People’s Republic of China on compulsory education. Available online: https://www.gov.cn/guoqing/2021-10/29/content_5647617.htm (accessed on 1 December 2024).
- Cheng, J., Dai, Y., Lin, S., & Ye, H. (2021). Clan culture and family ownership concentration: Evidence from China. China Economic Review, 70, 101692. [Google Scholar] [CrossRef]
- China Disabled Persons’ Federation. (2024, April 18). Disabled persons’ federation data. Available online: https://www.cdpf.org.cn//zwgk/zccx/index.htm (accessed on 1 December 2024).
- Chow, T. S., Tang, C. S. K., Siu, T. S. U., & Kwok, H. S. H. (2022). Family resilience scale short form (FRS16): Validation in the US and Chinese samples. Frontiers in Psychiatry, 13, 845803. [Google Scholar] [CrossRef]
- Clarke, V., & Braun, V. (2018). Using thematic analysis in counselling and psychotherapy research: A critical reflection. Counselling and Psychotherapy Research, 18(2), 107–110. [Google Scholar] [CrossRef]
- Cole, L., Kharwa, Y., Khumalo, N., Reinke, J. S., & Karrim, S. B. S. (2017). Caregivers of school-aged children with autism: Social media as a source of support. Journal of Child and Family Studies, 26(12), 3464–3475. [Google Scholar] [CrossRef]
- Dawson, G., Rieder, A. D., & Johnson, M. H. (2023). Prediction of autism in infants: Progress and challenges. The Lancet Neurology, 22(3), 244–254. [Google Scholar] [CrossRef]
- Dearnley, C. (2005). A reflection on the use of semi-structured interviews. Nurse Researcher, 13(1), 19–28. [Google Scholar] [CrossRef]
- De Haan, L., Hawley, D. R., & Deal, J. E. (2002). Operationalizing family resilience: A methodological strategy. The American Journal of Family Therapy, 30(4), 275–291. [Google Scholar] [CrossRef]
- Faulkner, S. L., & Trotter, S. P. (2017). Data saturation. In The International encyclopedia of communication research methods (pp. 1–2). Wiley. [Google Scholar] [CrossRef]
- Feng, Y., Zhou, X., Qin, X., Cai, G., Lin, Y., Pang, Y., Chen, B., Deng, T., & Zhang, L. (2022). Parental self-efficacy and family quality of life in parents of children with autism spectrum disorder in China: The possible mediating role of social support. Journal of Pediatric Nursing, 63, 159–167. [Google Scholar] [CrossRef]
- Gao, X., & Drani, S. (2024). Parent-implemented interventions in Chinese families of children with autism spectrum disorder. Humanities and Social Sciences Communications, 11(1), 196. [Google Scholar] [CrossRef]
- Gao, X., Lu, X., & Drani, S. (2023). Growing in adversity: A narrative study of resilience generation in Chinese families of children with ASD. Behavioral Sciences, 13(2), 136. [Google Scholar] [CrossRef]
- Gülbetekin, E., Kardaş Özdemir, F., & Aşut, G. (2024). The mediator role of parenting stress in the effect of stigmatization on burnout in parents of children with autism: A structural equality model. Journal of Pediatric Nursing, 78, e323–e329. [Google Scholar] [CrossRef] [PubMed]
- Ha, V. S., Whittaker, A., Whittaker, M., & Rodger, S. (2014). Living with autism spectrum disorder in Hanoi, Vietnam. Social Science & Medicine, 120, 278–285. [Google Scholar] [CrossRef]
- Hashimoto, N. K. (2020). Reclaiming joy: Finding resilience in families with children with autism. Available online: https://via.library.depaul.edu/soe_etd (accessed on 3 December 2024).
- Hassanein, E. E. A., Adawi, T. R., & Johnson, E. S. (2021). Social support, resilience, and quality of life for families with children with intellectual disabilities. Research in Developmental Disabilities, 112, 103910. [Google Scholar] [CrossRef]
- Henry, C. S., Sheffield Morris, A., & Harrist, A. W. (2015). Family resilience: Moving into the third wave. Family Relations, 64(1), 22–43. [Google Scholar] [CrossRef]
- Hosseinpour, A., Younesi, S. J., Azkhosh, M., Safi, M. H., & Biglarian, A. (2022). Exploring challenges and needs of parents providing care to children with autism spectrum disorders: A qualitative study. Iranian Journal of Psychiatry and Behavioral Sciences, 16(3), e127300. [Google Scholar] [CrossRef]
- Ilias, K., Cornish, K., Park, M. S.-A., Toran, H., & Golden, K. J. (2019). Risk and resilience among mothers and fathers of primary school age children with ASD in Malaysia: A qualitative constructive grounded theory approach. Frontiers in Psychology, 9, 2275. [Google Scholar] [CrossRef]
- In, J. (2017). Introduction of a pilot study. Korean Journal of Anesthesiology, 70(6), 601. [Google Scholar] [CrossRef]
- Kallio, H., Pietilä, A. M., Johnson, M., & Kangasniemi, M. (2016). Systematic methodological review: Developing a framework for a qualitative semi-structured interview guide. Journal of Advanced Nursing, 72(12), 2954–2965. [Google Scholar] [CrossRef]
- Kuhlthau, K., Payakachat, N., Delahaye, J., Hurson, J., Pyne, J. M., Kovacs, E., & Tilford, J. M. (2014). Quality of life for parents of children with autism spectrum disorders. Research in Autism Spectrum Disorders, 8(10), 1339–1350. [Google Scholar] [CrossRef]
- Kunselman, A. R. (2024). A brief overview of pilot studies and their sample size justification. Fertility and Sterility, 121(6), 899–901. [Google Scholar] [CrossRef] [PubMed]
- Maltby, J., Day, L., Flowe, H. D., Vostanis, P., & Chivers, S. (2019). Psychological trait resilience within ecological systems theory: The resilient systems scales. Journal of Personality Assessment, 101(1), 44–53. [Google Scholar] [CrossRef] [PubMed]
- Manning, M. M., Wainwright, L., & Bennett, J. (2011). The double ABCX model of adaptation in racially diverse families with a school-age child with autism. Journal of Autism and Developmental Disorders, 41(3), 320–331. [Google Scholar] [CrossRef]
- Mihas, P. (2023). Qualitative research methods: Approaches to qualitative data analysis. In International encyclopedia of education (4th ed., pp. 302–313). Elsevier. [Google Scholar] [CrossRef]
- Ng, C. S. M., & Ng, S. S. L. (2022). A qualitative study on the experience of stigma for Chinese parents of children with autism spectrum disorder. Scientific Reports, 12(1), 19550. [Google Scholar] [CrossRef]
- Peat, G., Rodriguez, A., & Smith, J. (2019). Interpretive phenomenological analysis applied to healthcare research. Evidence Based Nursing, 22(1), 7–9. [Google Scholar] [CrossRef]
- Rivard, M., Terroux, A., Parent-Boursier, C., & Mercier, C. (2014). Determinants of stress in parents of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 44(7), 1609–1620. [Google Scholar] [CrossRef]
- Sardohan Yildirim, A. E., Altindağ Kumaş, Ö., & Yazicioğlu, T. (2025). Social support, resilience and life satisfaction in families with special needs children. Journal of Pediatric Nursing, 80, 16–23. [Google Scholar] [CrossRef]
- Shattnawi, K. K., Bani, S. W. M., Al-Natour, A., Al-Hammouri, M. M., Al-Azzam, M., & Joseph, R. A. (2021). Parenting a child with autism spectrum disorder: Perspective of jordanian mothers. Journal of Transcultural Nursing, 32(5), 474–483. [Google Scholar] [CrossRef]
- Shorey, S., Ng, E. D., Haugan, G., & Law, E. (2020). The parenting experiences and needs of Asian primary caregivers of children with autism: A meta-synthesis. Autism, 24(3), 591–604. [Google Scholar] [CrossRef]
- Smith, J. A., & Osborn, M. (2015). Interpretative phenomenological analysis as a useful methodology for research on the lived experience of pain. British Journal of Pain, 9(1), 41–42. [Google Scholar] [CrossRef] [PubMed]
- Summers, J. A., Marquis, J., Mannan, H., Turnbull, A. P., Fleming, K., Poston, D. J., Wang, M., & Kupzyk, K. (2007). Relationship of perceived adequacy of services, family–professional partnerships, and family quality of life in early childhood service programmes. International Journal of Disability, Development and Education, 54(3), 319–338. [Google Scholar] [CrossRef]
- Tait, K., Fung, F., Hu, A., Sweller, N., & Wang, W. (2016). Understanding Hong Kong Chinese families’ experiences of an autism/ASD diagnosis. Journal of Autism and Developmental Disorders, 46(4), 1164–1183. [Google Scholar] [CrossRef] [PubMed]
- Thabane, L., Ma, J., Chu, R., Cheng, J., Ismaila, A., Rios, L. P., Robson, R., Thabane, M., Giangregorio, L., & Goldsmith, C. H. (2010). A tutorial on pilot studies: The what, why and how. BMC Medical Research Methodology, 10, 1. [Google Scholar] [CrossRef]
- Tong, A., Sainsbury, P., & Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care, 19(6), 349–357. [Google Scholar] [CrossRef]
- Turns, B., Ramisch, J., & Whiting, J. (Eds.). (2019). Systemically treating autism. Routledge. [Google Scholar] [CrossRef]
- Walsh, F. (2015). Strengthening family resilience. Guilford publications. [Google Scholar]
- Walsh, F. (2021). Family resilience. In Multisystemic resilience (pp. 255–270). Oxford University Press. [Google Scholar] [CrossRef]
- Wang, P., Michaels, C. A., & Day, M. S. (2011). Stresses and coping strategies of chinese families with children with autism and other developmental disabilities. Journal of Autism and Developmental Disorders, 41(6), 783–795. [Google Scholar] [CrossRef]
- West, C., Usher, K., & Foster, K. (2011). Family resilience: Towards a new model of chronic pain management. Collegian, 18(1), 3–10. [Google Scholar] [CrossRef]
- WHO. (2023, November 15). Autism. Available online: https://www.who.int/news-room/fact-sheets/detail/autism-spectrum-disorders?gad_source=1&gclid=Cj0KCQjwmOm3BhC8ARIsAOSbapVIGbP5Qh-UU8YTDaDHBkd7hfb9W2jTeKFoXRWNN-YlAEk9GyjronYaAoxkEALw_wcB (accessed on 1 December 2024).
- Xiong, A., & Li, Y. (2024). The role of social capital in building community disaster resilience–empirical evidences from rural China. International Journal of Disaster Risk Reduction, 110, 104623. [Google Scholar] [CrossRef]
- Yang, M., Zhang, Y., Yu, Z., Zhang, M., Yao, Y., Wang, Z., & Qiu, G. (2018). Analysis of the correlation between psychological resilience and social support among parents of children with autism in a hospital in Guangzhou. Medicine and Society, 11, 71–73. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Family No. | Family Structure | Age of Individual with ASD | Participant No. | Age | Gender | Kinship | Educational Level | Scale Score | M (SD) | t-Value |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Core family | 10 | 1-1 | 35 | Female | Mother | Secondary school | 46 | 49.25 (2.86) | −0.223 |
| 1-2 | 37 | Male | Father | Secondary school | 49 | |||||
| 2 | Extended family | 16 | 2-1 | 42 | Male | Father | Bachelor’s degree | 48 | ||
| 2-2 | 46 | Female | Mother | Secondary school | 50 | |||||
| 3 | Extended family | 14 | 3-1 | 39 | Male | Father | Bachelor’s degree | 45 | ||
| 3-2 | 59 | Female | Grandma | Primary school | 49 | |||||
| 4 | Extended family | 12 | 4-1 | 35 | Female | Mother | Secondary school | 51 | ||
| 4-2 | 57 | Male | Grandpa | Primary school | 49 | |||||
| 5 | Core family | 9 | 5-1 | 34 | Male | Father | Primary school | 53 | ||
| 5-2 | 38 | Female | Mother | Secondary school | 51 | |||||
| 6 | Extended family | 9 | 6-1 | 32 | Female | Mother | Bachelor’s degree | 45 | ||
| 6-2 | 51 | Female | Grandma | Primary school | 47 | |||||
| 7 | Extended family | 13 | 7-1 | 39 | Female | Mother | Secondary school | 55 | ||
| 7-2 | 39 | Male | Father | Bachelor’s degree | 51 | |||||
| 8 | Extended family | 11 | 8-1 | 34 | Male | Father | Bachelor’s degree | 52 | ||
| 8-2 | 55 | Female | Grandma | Secondary school | 47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, F.; Gao, X. The Challenge Coping and Resilience of the Families of School-Aged Children with Autism Spectrum Disorder in China: A Qualitative Study. Behav. Sci. 2025, 15, 409. https://doi.org/10.3390/bs15040409
Han F, Gao X. The Challenge Coping and Resilience of the Families of School-Aged Children with Autism Spectrum Disorder in China: A Qualitative Study. Behavioral Sciences. 2025; 15(4):409. https://doi.org/10.3390/bs15040409
Chicago/Turabian StyleHan, Fengying, and Xin Gao. 2025. "The Challenge Coping and Resilience of the Families of School-Aged Children with Autism Spectrum Disorder in China: A Qualitative Study" Behavioral Sciences 15, no. 4: 409. https://doi.org/10.3390/bs15040409
APA StyleHan, F., & Gao, X. (2025). The Challenge Coping and Resilience of the Families of School-Aged Children with Autism Spectrum Disorder in China: A Qualitative Study. Behavioral Sciences, 15(4), 409. https://doi.org/10.3390/bs15040409