
Translating Formative Research into Intervention Content: Experiences with Face Washing for Trachoma Control in Rural Ethiopia

 , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Stage 1—Developing the Creative Brief: Synthesising Formative Research
2.2. Stage 2—Selecting Behaviour Change Techniques (BCTs)
2.3. Stage 3—Choosing an Overarching Intervention Concept
2.4. Stage 4—Developing Intervention Content
2.5. Stage 5—Finalising the Intervention’s Theory of Change
3. Results
3.1. Stage 1—Developing the Creative Brief: Synthesising Formative Research
3.2. Stage 2—Selecting Behaviour Change Techniques (BCTs)
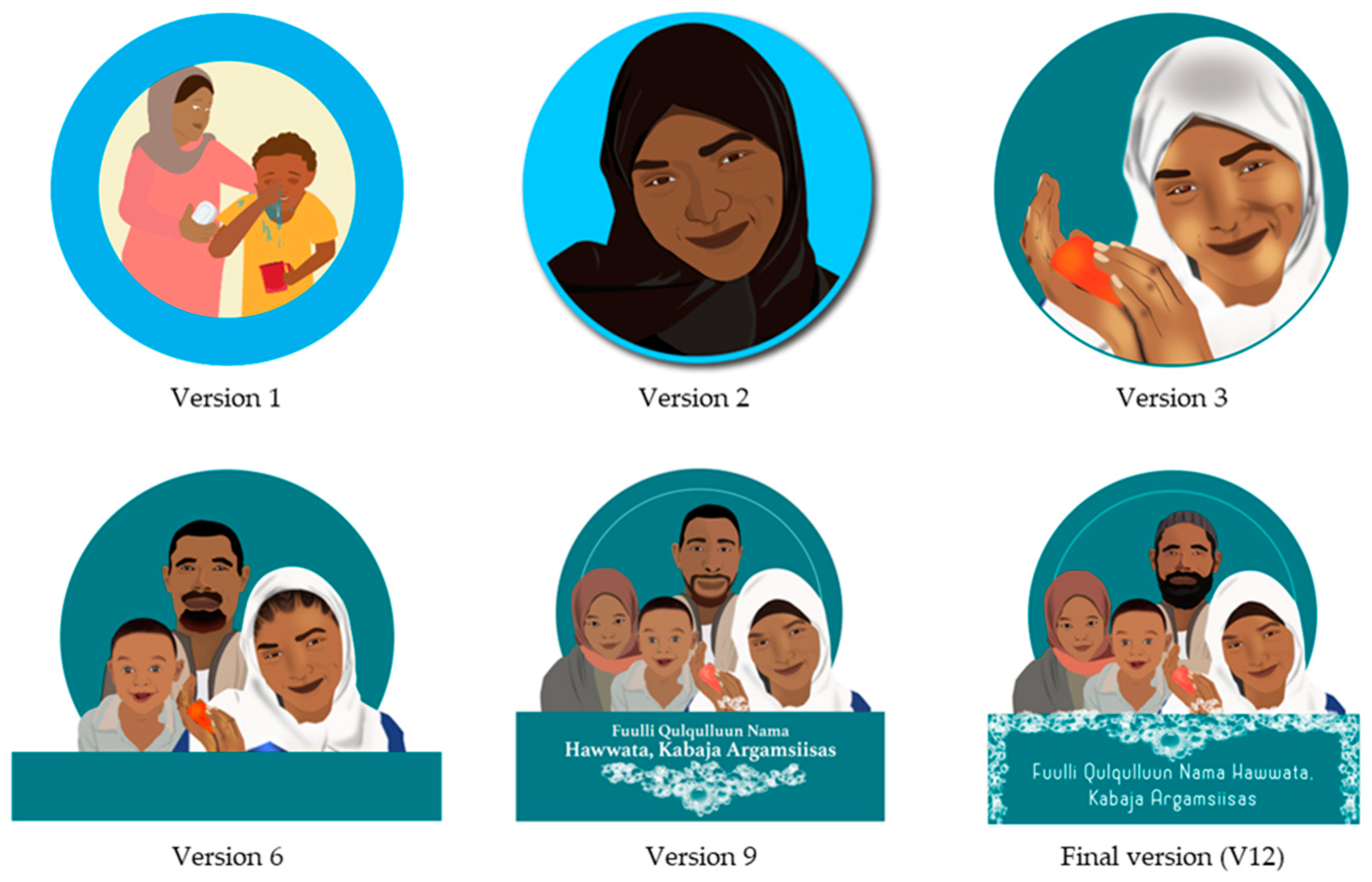
3.3. Stage 3—Choosing an Overarching Concept
“Children come from the family, so if the family is dignified the children will be dignified”.(Female caregiver, individual household interview on the concept of dignity, January 2020)
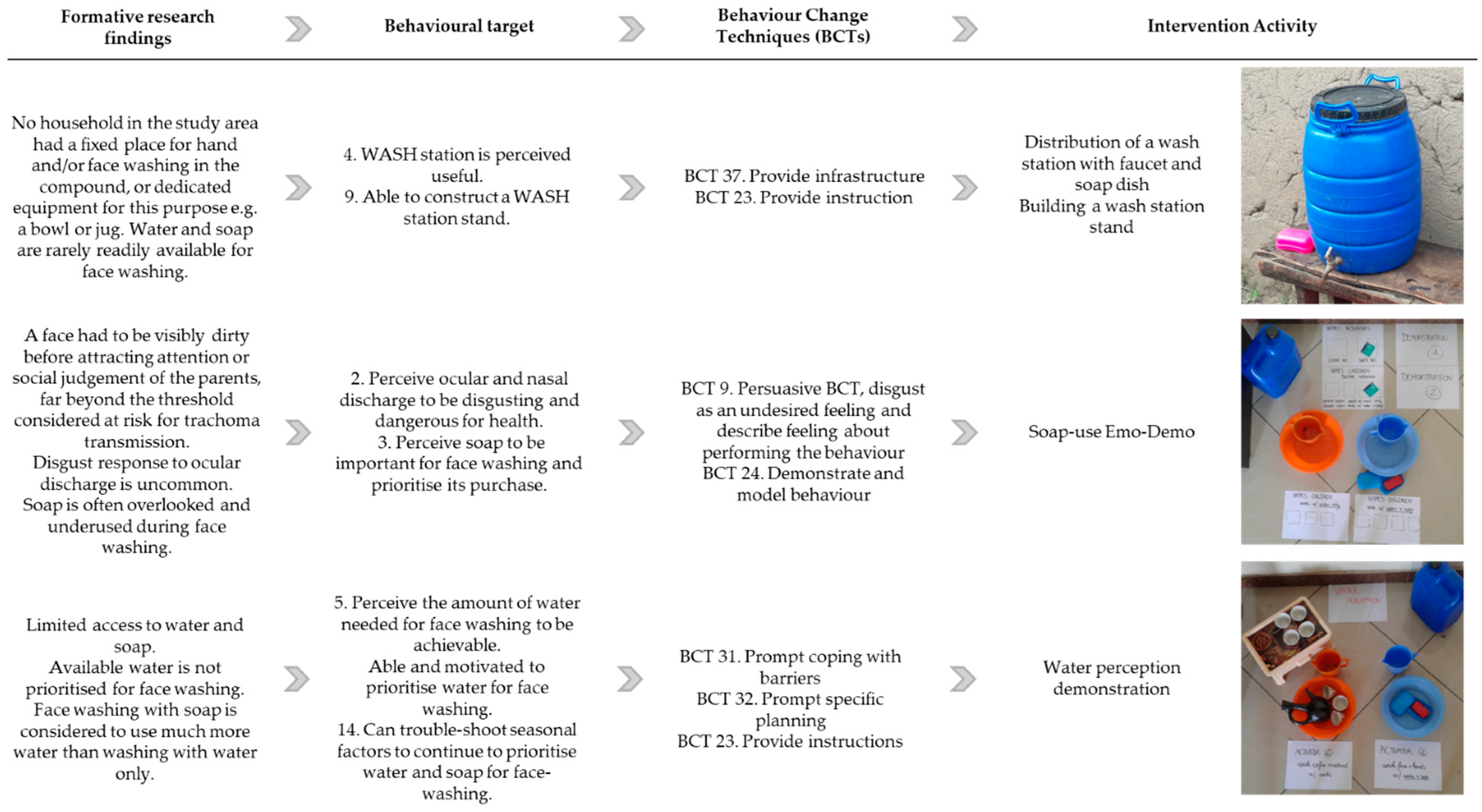
3.4. Stage 4—Developing Intervention Content
3.4.1. Intervention Activities
3.4.2. Intervention Package
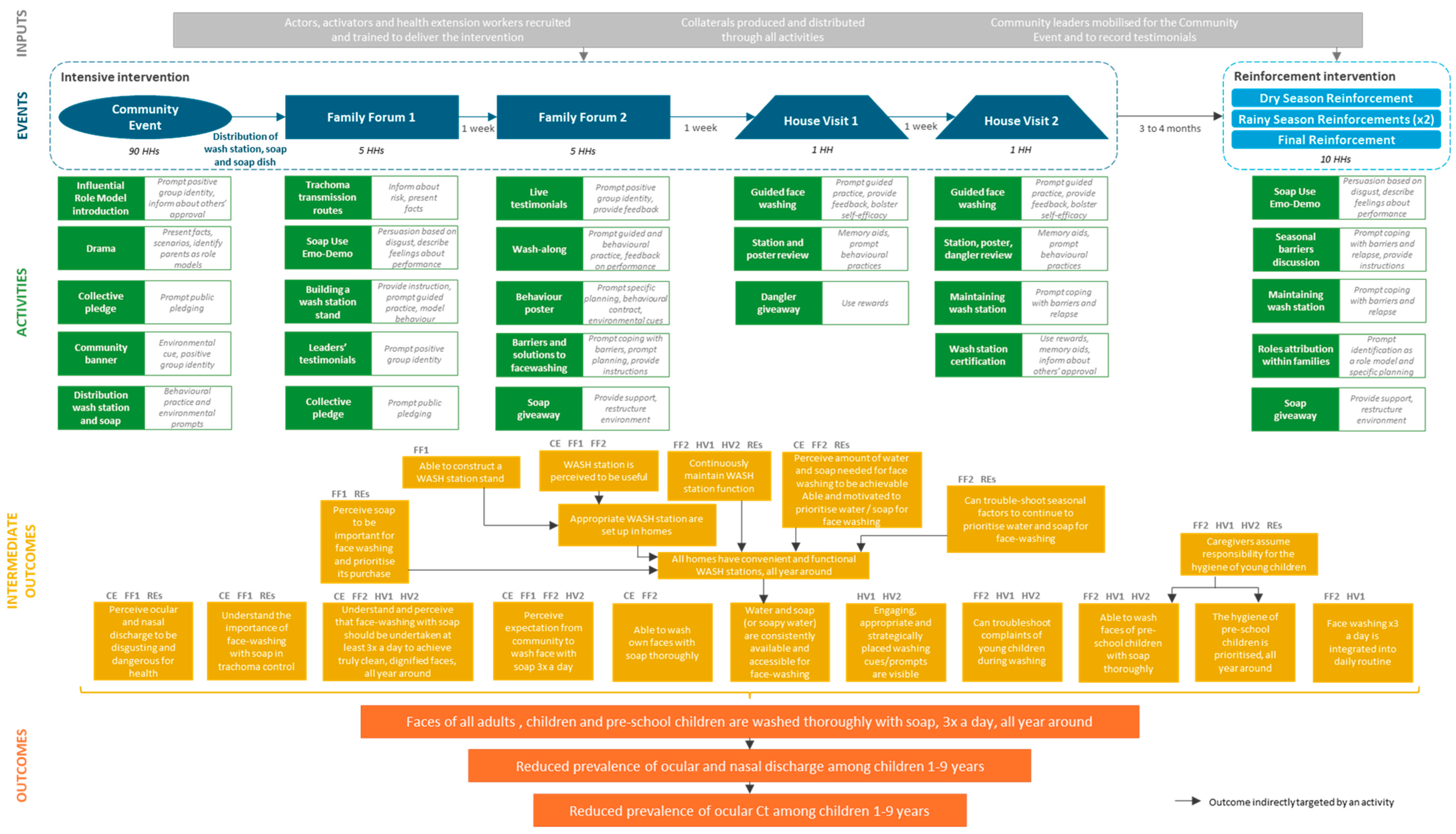
3.5. Stage 5—Finalising the Intervention’s Theory of Change
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abdou, A., Munoz, B. E., Nassirou, B., Kadri, B., Moussa, F., Baarè, I., Riverson, J., Opong, E., & West, S. K. (2010). How much is not enough? A community randomized trial of a Water and Health Education programme for Trachoma and Ocular C. trachomatis infection in Niger. Tropical Medicine & International Health, 15(1), 98–104. [Google Scholar] [CrossRef]
- Aragie, S., Wittberg, D. M., Tadesse, W., Dagnew, A., Hailu, D., Chernet, A., Melo, J. S., Aiemjoy, K., Haile, M., Zeru, T., Tadesse, Z., Gwyn, S., Martin, D. L., Arnold, B. F., Freeman, M. C., Nash, S. D., Callahan, E. K., Porco, T. C., Lietman, T. M., & Keenan, J. D. (2022). Water, sanitation, and hygiene for control of trachoma in Ethiopia (WUHA): A two-arm, parallel-group, cluster-randomised trial. The Lancet Global Health, 10(1), e87–e95. [Google Scholar] [CrossRef] [PubMed]
- Aunger, R., & Curtis, V. (2016). Behaviour centred design: Towards an applied science of behaviour change. Health Psychology Review, 10(4), 425–446. [Google Scholar] [CrossRef]
- Aunger, R., White, S., Greenland, K., & Curtis, V. (2017). Behaviour centred design. A practitioner’s manual. Available online: https://www.lshtm.ac.uk/sites/default/files/2017-03/BCD%20Manual.pdf (accessed on 17 September 2020).
- Biran, A., Schmidt, W. P., Varadharajan, K. S., Rajaraman, D., Kumar, R., Greenland, K., Gopalan, B., Aunger, R., & Curtis, V. (2014). Effect of a behaviour-change intervention on handwashing with soap in India (SuperAmma): A cluster-randomised trial. The Lancet Global Health, 2(3), e145–e154. [Google Scholar] [CrossRef]
- Biswas, S. K., Thomas, E. D., Masud, J., Zohura, F., Hasan, T., Parvin, T., Bhuyian, S. I., Minhaj, I., Johura, F., Sultana, M., Tahmina, S., Monira, S., Perin, J., Alam, M., & George, C. M. (2021). Formative research for the design of a baby water, sanitation, and hygiene mobile health program in Bangladesh (CHoBI7 Mobile Health Program). The American Journal of Tropical Medicine and Hygiene, 104(1), 357–371. [Google Scholar] [CrossRef] [PubMed]
- Czerniewska, A., Mwambuli, K., Curtis, V., & Aunger, R. (2023). Intervention design in public health: Adaptive messaging in the Tanzanian National Sanitation Campaign. Health Promotion International, 38(3), daad064. [Google Scholar] [CrossRef]
- Czerniewska, A., Versteeg, A., Shafi, O., Dumessa, G., Aga, M. A., Last, A., MacLeod, D., Sarah, V., Dodson, S., Negussu, N., Sori, B. K., Kirumba, M., Biran, A., Cairncross, S., Burton, M. J., & Greenland, K. (2020). Comparison of face washing and face wiping methods for trachoma control: A pilot study. The American Journal of Tropical Medicine and Hygiene, 102(4), 740–743. [Google Scholar] [CrossRef]
- De Buck, E., Van Remoortel, H., Hannes, K., Govender, T., Naidoo, S., Avau, B., Veegaete, A. V., Musekiwa, A., Lutje, V., Cargo, M., Mosler, H., Vandekerckhove, P., & Young, T. (2017). Approaches to promote handwashing and sanitation behaviour change in low- and middle-income countries: A mixed method systematic review. Campbell Systematic Reviews, 13(1), 1–447. [Google Scholar] [CrossRef]
- Delea, M. G., Solomon, H., Solomon, A. W., & Freeman, M. C. (2018). Interventions to maximize facial cleanliness and achieve environmental improvement for trachoma elimination: A review of the grey literature. PLoS Neglected Tropical Diseases, 12(1), e0006178. [Google Scholar] [CrossRef]
- De Silva, M. J., Breuer, E., Lee, L., Asher, L., Chowdhary, N., Lund, C., & Patel, V. (2014). Theory of Change: A theory-driven approach to enhance the Medical Research Council’s framework for complex interventions. Trials, 15(1), 267. [Google Scholar] [CrossRef]
- D’Mello-Guyett, L., Greenland, K., Bonneville, S., D’Hondt, R., Mashako, M., Gorski, A., Verheyen, D., Bergh, R. V. D., Maes, P., Checchi, F., & Cumming, O. (2020). Distribution of hygiene kits during a cholera outbreak in Kasaï-Oriental, Democratic Republic of Congo: A process evaluation. Conflict and Health, 14(1), 51. [Google Scholar] [CrossRef] [PubMed]
- Dreibelbis, R., Winch, P. J., Leontsini, E., Hulland, K. R. S., Ram, P. K., Unicomb, L., & Luby, S. P. (2013). The integrated behavioural model for water, sanitation, and hygiene: A systematic review of behavioural models and a framework for designing and evaluating behaviour change interventions in infrastructure-restricted settings. BMC Public Health, 13(1), 1015. [Google Scholar] [CrossRef] [PubMed]
- Ejere, H. O., Alhassan, M. B., & Rabiu, M. (2015). Face washing promotion for preventing active trachoma. Cochrane Database of Systematic Reviews, 2015(2), CD003659. [Google Scholar] [CrossRef]
- Freeman, M. C., Delea, M. G., Snyder, J. S., Garn, J. V., Belew, M., Caruso, B. A., Clasen, T. F., Sclar, G. D., Tesfaye, Y., Woreta, M., Zewudie, K., & Gobezayehu, A. G. (2022). The impact of a demand-side sanitation and hygiene promotion intervention on sustained behavior change and health in Amhara, Ethiopia: A cluster-randomized trial. PLoS Global Public Health, 2(1), e0000056. [Google Scholar] [CrossRef] [PubMed]
- French, S. D., Green, S. E., O’Connor, D. A., McKenzie, J. E., Francis, J. J., Michie, S., Buchbinder, R., Schattner, P., Spike, N., & Grimshaw, J. M. (2012). Developing theory-informed behaviour change interventions to implement evidence into practice: A systematic approach using the Theoretical Domains Framework. Implementation Science, 7(1), 38. [Google Scholar] [CrossRef]
- Friedrich, M., Balasundaram, T., Muralidharan, A., Raman, V. R., & Mosler, H.-J. (2020). Increasing latrine use in rural Karnataka, India using the risks, attitudes, norms, abilities, and self-regulation approach: A cluster-randomized controlled trial. Science of the Total Environment, 707, 135366. [Google Scholar] [CrossRef]
- Gittelsohn, J., Steckler, A., Johnson, C. C., Pratt, C., Grieser, M., Pickrel, J., Stone, E. J., Conway, T., Coombs, D., & Staten, L. K. (2006). Formative research in school and community-based health programs and studies: “State of the Art” and the TAAG approach. Health Education & Behavior, 33(1), 25–39. [Google Scholar] [CrossRef]
- Glasgow, R. E., & Linnan, L. (2008). Evaluation of theory-based interventions. In K. Glanz, B. K. Rimer, & K. Viswanath (Eds.), Health behaviour and health education. Theory, Research and Practice. Jossey-Bass. [Google Scholar]
- Greenland, K., Chipungu, J., Chilekwa, J., Chilengi, R., & Curtis, V. (2017). Disentangling the effects of a multiple behaviour change intervention for diarrhoea control in Zambia: A theory-based process evaluation. Globalization and Health, 13(1), 78. [Google Scholar] [CrossRef]
- Greenland, K., Czerniewska, A., Guye, M., Legesse, D., Ahmed Mume, A., Abdurahman, O. S., Aga, M. A., Miecha, H., Bejiga, G. S., Sarah, V., Burton, M., & Last, A. (2022). Seasonal variation in water use for hygiene in Oromia, Ethiopia, and its implications for trachoma control: An intensive observational study. PLoS Neglected Tropical Diseases, 16(5), e0010424. [Google Scholar] [CrossRef]
- Greenland, K., White, S., Sommers, K., Biran, A., Burton, M. J., Sarah, V., & Alemayehu, W. (2019). Selecting behaviour change priorities for trachoma ‘F’ and ‘E’ interventions: A formative research study in Oromia, Ethiopia. PLoS Neglected Tropical Diseases, 13(10), e0007784. [Google Scholar] [CrossRef]
- Inauen, J., & Mosler, H.-J. (2014). Developing and testing theory-based and evidence-based interventions to promote switching to arsenic-safe wells in Bangladesh. Journal of Health Psychology, 19(12), 1483–1498. [Google Scholar] [CrossRef]
- Jacob Arriola, K. R., Ellis, A., Webb-Girard, A., Ogutu, E. A., McClintic, E., Caruso, B., & Freeman, M. C. (2020). Designing integrated interventions to improve nutrition and WASH behaviors in Kenya. Pilot and Feasibility Studies, 6(1), 10. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, J., Bisimwa, L., Thomas, E. D., Williams, C., Ntakirutimana, J., Coglianese, N., Bauler, S., François, R., Sanvura, P., Bisimwa, J. C., Mirindi, P., & George, C. M. (2021). Formative research for the development of baby water, sanitation, and hygiene interventions for young children in the Democratic Republic of the Congo (REDUCE program). BMC Public Health, 21(1), 427. [Google Scholar] [CrossRef] [PubMed]
- Last, A., Versteeg, B., Shafi Abdurahman, O., Robinson, A., Dumessa, G., Abraham Aga, M., Bejiga, G. S., Negussu, N., Greenland, K., Czerniewska, A., Thomson, N., Cairncross, S., Sarah, V., Macleod, D., Solomon, A. W., Logan, J., & Burton, M. J. (2020). Detecting extra-ocular Chlamydia trachomatis in a trachoma-endemic community in Ethiopia: Identifying potential routes of transmission. PLoS Neglected Tropical Diseases, 14(3), e0008120. [Google Scholar] [CrossRef] [PubMed]
- Michie, S. (2008). Designing and implementing behaviour change interventions to improve population health. Journal of Health Services Research & Policy, 13(3_suppl), 64–69. [Google Scholar] [CrossRef]
- Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., Eccles, M. P., Cane, J., & Wood, C. E. (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Annals of Behavioral Medicine, 46(1), 81–95. [Google Scholar] [CrossRef]
- Michie, S., van Stralen, M. M., & West, R. (2011). The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implementation Science, 6(1), 42. [Google Scholar] [CrossRef]
- Mosler, H. J. (2012). A systematic approach to behavior change interventions for the water and sanitation sector in developing countries: A conceptual model, a review, and a guideline. International Journal of Environmental Health Research, 22(5), 431–449. [Google Scholar] [CrossRef]
- Mosler, H. J. (2016). Catalog of behavior change techniques (BCTs). ESI 3.1 to a practical guide using the RANAS approach version 1.0, August 2016. Available online: https://76ddba31-385f-4f1b-a8fc-00db654c6cbf.filesusr.com/ugd/accbe3_2540cf86e0e84a779156dd4a58aaab14.pdf (accessed on 17 September 2020).
- O’Cathain, A., Croot, L., Duncan, E., Rousseau, N., Sworn, K., Turner, K. M., Yardley, L., & Hoddinott, P. (2019). Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open, 9(8), e029954. [Google Scholar] [CrossRef]
- Ogutu, E. A., Ellis, A., Rodriguez, K. C., Caruso, B. A., McClintic, E. E., Ventura, S. G., Arriola, K. R. J., Kowalski, A. J., Linabarger, M., Wodnik, B. K., Webb-Girard, A., Muga, R., & Freeman, M. C. (2022). Determinants of food preparation and hygiene practices among caregivers of children under two in Western Kenya: A formative research study. BMC Public Health, 22(1), 1865. [Google Scholar] [CrossRef]
- Panulo, M., Chidziwisano, K., Beattie, T. K., Tilley, E., Kambala, C., & Morse, T. (2022). Process evaluation of “The Hygienic Family” intervention: A community-based water, sanitation, and hygiene project in rural Malawi. International Journal of Environmental Research and Public Health, 19(11), 6771. [Google Scholar] [CrossRef] [PubMed]
- Shafi Abdurahman, O., Last, A., Macleod, D., Habtamu, E., Versteeg, B., Dumessa, G., Guye, M., Nure, R., Adugna, D., Miecha, H., Greenland, K., & Burton, M. J. (2023). Trachoma risk factors in Oromia region, Ethiopia. PLoS Neglected Tropical Diseases, 17(11), e0011679. [Google Scholar] [CrossRef]
- Singh, D. R., Sah, R. K., Simkhada, B., & Darwin, Z. (2023). Potentials and challenges of using co-design in health services research in low- and middle-income countries. Global Health Research and Policy, 8(1), 5. [Google Scholar] [CrossRef]
- Sule, M. N., Mosha, J., Soboka, T. E., Kinung’hi, S. M., Sfynia, C., Rafiq, K., Dower, A., Comparet, M., Bewley, E., Angelo, T., Beshah, F. Z., & Templeton, M. R. (2022). A novel theatre-based behaviour change approach for influencing community uptake of schistosomiasis control measures. Parasites & Vectors, 15(1), 301. [Google Scholar] [CrossRef]
- Taylor, H. R., Burton, M. J., Haddad, D., West, S., & Wright, H. (2014). Trachoma. Lancet, 384(9960), 2142–2152. [Google Scholar] [CrossRef] [PubMed]
- Tidwell, J. B., Chipungu, J., Chilengi, R., Curtis, V., & Aunger, R. (2019). Using a theory-driven creative process to design a peri-urban on-site sanitation quality improvement intervention. BMC Public Health, 19(1), 565. [Google Scholar] [CrossRef] [PubMed]
- Vargas, C., Whelan, J., Brimblecombe, J., & Allendera, S. (2022). Co-creation, co-design and co-production for public health: A perspective on definitions and distinctions. Public Health Research & Practice, 32(2), e3222211. [Google Scholar]
- Weiss, C. (1995). Nothing as practical as a good theory: Exploring theory-based evaluation in complex community initiatives for children and families. In J. Connell, A. Kubisch, L. Schorr, & C. Weiss (Eds.), New approaches to evaluating community initiatives: Volume 1, concepts, methods, and contexts. The Aspen Institute. [Google Scholar]
- World Health Organization. (2020). Ending the neglect to attain the sustainable development goals: A road map for neglected tropical diseases 2021–2030. World Health Organization. [Google Scholar]
- World Health Organization. (2024). WHO alliance for the global elimination of trachoma: Progress report on elimination of trachoma, 2023. Weekly Epidemiological Record, 28(99), 363–380. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| RANAS Behavioural Factor | Formative Research Findings on Face Washing Behaviour and Its Potential Determinants |
|---|---|
| Risk | Awareness of trachoma: common; awareness of link between hygiene and trachoma prevention: moderate; little fear of blindness from trachoma |
| Attitude | Disgust response to ocular discharge: uncommon; soap use for body washing: uncommon; reward/recognition for children who wash: none; pleasure experienced from washing: refreshment when dusty; water needed: more water needed if soap is used (1 L vs. 0.5 L per person per wash) Emotional drivers: Social judgement/affiliation motive: cannot publicly judge others, but mothers fear being judged; celebrity/role model/status motive: unimportant; nurture motive: weak, fathers interested in engaging with health activities and issues |
| Norm | Face washing with soap practises in the morning only; use of soap: not expected; being clean: expected at school but not at home; handwashing before meals: expected, low emphasis on face washing; gossiping or visibly judging neighbours: unacceptable; role models do not use soap; responsibility for hygiene of adults and children: self; responsibility for hygiene of very young children: mothers and occasionally fathers, limited involvement of fathers in childcare; responsibility for water collection: mothers or older children |
| Ability | Socioeconomic status: poor and very poor; water taps at home: uncommon, water storage in jerry cans; washing stations: uncommon; capability of small children to perform effective washing with minimal water: very limited; children resist washing which makes it difficult for mothers; discomfort/pain associated with soap in eyes, soap use dries the skin |
| Self-regulation | Responsibility for financial decisions about household purchases: fathers; responsibility for digging holes/building infrastructure: fathers; fathers oversee the activities of mothers; limited access to water and soap; high water scarcity (especially in dry season); soap availability: can be purchased at local market affordably; washing prompts: waking, evening meal; physical washing prompts: uncommon; washing equipment: plastic bowls/buckets/teapots/cups/cans, fabric use for face drying: uncommon |
| RANAS Behavioural Factors | Intervention Target | RANAS Behaviour Change Techniques |
|---|---|---|
| Risk factors | ||
| Factual knowledge | 1. Understand the importance of face washing with soap in trachoma control. | BCT 1. Present facts BCT 2. Present scenarios |
| Vulnerability | 2. Perceive ocular and nasal discharge to be disgusting and dangerous for health. | BCT 3. Inform about and assess personal risk |
| Attitudinal factors | ||
| Beliefs about costs and benefits | 2. Perceive ocular and nasal discharge to be disgusting and dangerous for health. 3. Perceive soap to be important for face washing and prioritise its purchase. 4. WASH station is perceived to be useful. 5. Perceive amount of water and soap needed for face washing to be achievable. Able and motivated to prioritise water/soap for face washing. | BCT 5. Inform about and assess costs and benefits BCT 6. Use subsequent reward BCT 7. Self-incentive BCT 8. Inform about and assess social and environmental consequences BCT 9. Describe feelings about performing and about consequences of the behaviour |
| Normative factors | ||
| Others’ behaviour | 6. Perceive expectation from community to wash face with soap 3× a day. 7. Understand and perceive that face washing with soap should be undertaken at least 3× a day to achieve truly clean, dignified faces, all year around. | BCT 11. Inform about others’ behaviour BCT 13. Prompt public pledging |
| Others’ (dis)approval | 6. Perceive expectation from community to wash face with soap 3× a day. 7. Understand and perceive that face washing with soap should be undertaken at least 3× a day to achieve truly clean, dignified faces, all year around. | BCT 15. Inform about others’ approval/disapproval |
| Personal norms | 7. Understand and perceive that face washing with soap should be undertaken at least 3× a day to achieve truly clean, dignified faces, all year around. 8. Caregiver assume responsibility for the hygiene of young children. | BCT 17. Provide a positive group identity and use in-group terms BCT 18. Prompt identification as role model |
| Ability factors | ||
| Action knowledge | 9. Able to construct a WASH station stand. | BCT 23. Provide instruction |
| Confidence in ability | 10. Able to wash faces of pre-school children with soap thoroughly. 11. Can troubleshoot complaints of young children during washing. 12. Able to wash own faces with soap thoroughly. | BCT 24. Demonstrate and model behaviour BCT 25. Prompt guided practice BCT 26. Prompt behavioural practice BCT 27. Organise social support BCT 28. Set graded tasks/goals |
| Confidence in continuation | 13. Continuously maintain WASH station function. | BCT 29. Reattribute past successes and failures |
| Confidence in recovering | 14. Can trouble-shoot seasonal factors to continue to prioritise water and soap for face washing. | BCT 31. Prompt coping with relapse |
| Self-regulation factors | ||
| Action planning | 15. Face washing 3× a day is integrated into daily routine. | BCT 32. Prompt specific planning |
| Action control | 16. Appropriate WASH station are set up in homes. 17. All homes have convenient and functional WASH stations, all year around. 18. Water and soap (or soapy water) are consistently available and accessible for face washing. | BCT 33. Prompt (self) monitoring of behaviour BCT 34. Provide feedback on performance BCT 35. Highlight discrepancy between set goal and actual behaviour |
| Barrier planning | 14. Can trouble-shoot seasonal factors to continue to prioritise water and soap for face washing. 19. The hygiene of pre-school children is prioritised, all year around. | BCT 36. Prompt coping with barriers BCT 37. Restructure the social and physical environment |
| Remembering | 20. Engaging, appropriate and strategically placed washing cues/prompts are visible. | BCT 38. Use memory aids and environmental prompts |
| Commitment | 15. Face washing 3× a day is integrated into daily routine. 19. The hygiene of pre-school children is prioritised, all year around. | BCT 39. Prompt goal setting BCT 40. Prompt to agree on a behavioural contract |
| Emotional Driver | Comprehension | Acceptability | Relatability | Perceived Link to Face Washing |
|---|---|---|---|---|
| Pair-bond love | High | High | High | High |
| Nurture | Low | Moderate | Moderate | Moderate |
| Status | High | Low | Moderate | High |
| Dignity | High | High | High | High |
| Event | Audience | Implementers | Purpose | Content | Timing | Duration |
|---|---|---|---|---|---|---|
| Community Event | 90 households from three garees * | 2 Actors 2 Health Volunteers 2 Community leaders | Raise awareness and credibility of the Faces of Dignity intervention, increase buy-in, and initiate face washing | A 20 min drama presenting scenarios of face washing behaviours, highlighting parents as role models and soap use as essential for family dignity. A collective pledge, led by community leaders, prompting public commitment and creating normative expectations to adopt the target behaviour. Distribution of wash stations with a faucet and soap to facilitate ability to perform the behaviour. | First event | 1 h |
| Family Forum 1 | 5 neighbouring households | 1 Activator 1 Health Volunteer | Build knowledge, skills, and motivation for face washing. Empower households to construct wash stations to aid habit formation. | Description of trachoma transmission routes to increase knowledge. Soap Use Emo Demo to elicit disgust as a driver for behaviour change. Distribution of an instruction flyer to guide households in building an accessible washstand for their wash station. Pre-recorded testimonials from role models informing about expected behavioural practise. Collective pledge with participants committing to building the station and ensuring three daily washes. | 1 week post Community Event | 1 h and 30 min |
| Family Forum 2 | 5 neighbouring households | 1 Activator 1 Health Volunteer | Overcome early barriers related to wash station construction and use. Emphasise the need and build capacity to practise the target behaviour. | Live testimonials for participants to share experiences and provide feedback to develop tailored solutions. Wash-along activity to reinforce self-efficacy. Water prioritisation activities, soapy water demonstration, and distribution of a bar of soap to address barriers to sustained behaviour change, such as water and soap availability. Distribution of the “Dignified Day” poster as a behavioural reminder. | 1 week post Family Forum 1 | 1 h and 30 min |
| Household Visit 1 | 1 household | 1 Health Volunteer | Provide personalised support to practise the target behaviour. | Wash station assessment with tailored feedback. Review of the “Dignified Day” poster. Distribution of a dangler serving as a reminder for face washing. | 1 week post Family Forum 2 | 20 to 30 min |
| Household Visit 2 | 1 household | 1 Activator | Provide ongoing and personalised support to practise the target behaviour and to maintain the wash station. | Face washing with soap demonstration to reinforce behavioural practise and self-efficacy. A short video on wash station maintenance to prompt coping with barriers and behavioural relapse. Distribution of a certification sticker for the wash station to reward households for their efforts to maintain behavioural practice. | 1 week post Household Visit 1 | 30 to 45 min |
| First Rainy Season Reinforcement Event | 10 neighbouring households | 2 Activators 1 Health Volunteer | Overcome seasonal barriers to behaviour practise. Reinforce the intervention’s messages. | Reminder of trachoma transmission routes. Soap use Emo Demo to elicit disgust as a driver. Problem-solving testimonials and discussion, i.e., lack of time and soap. Maintaining wash station functional. Attributing roles in the family (e.g., washing, repairing). Soap giveaway. | Prior to start of the rainy season | 45 min to 1 h |
| Dry Season Reinforcement Event | 10 neighbouring households | 2 Activators 1 Health Volunteer | Overcome seasonal barriers to behaviour practise. Reinforce the intervention’s messages. | Reminder of trachoma transmission routes. Demonstration of the benefits of washing with soap. Problem-solving testimonials and discussion, i.e., wash station maintenance and lack of water. Water prioritisation activities. Short drama on avoiding procrastination. Attributing roles in the family. Soap giveaway. | Prior to start of the dry season | 45 min to 1 h |
| Second Rainy Season Reinforcement Event | 10 neighbouring households | 1 Health Volunteer | Check wash station use and maintenance. Reinforce the intervention’s message. | Demonstration of wash station maintenance. Reminder of the importance of soap for face washing and troubleshooting issues with soap availability (i.e., making soapy water). Attributing roles in the family (i.e., a child cannot wash their face as thoroughly as a caregiver can). | Prior to start of the rainy season | 30 to 45 min |
| Final Reinforcement Event | 10 neighbouring households | 2 Activators 1 Health Volunteer | Overcome seasonal barriers to behaviour practise. Reinforce the intervention’s messages. | Small gender-separated group events: roles and responsibilities regarding hygiene behaviours (role-modelling) and wash station maintenance. Whole-group event: problem-solving through testimonials and discussion (i.e., lack of soap). Short drama on benefits of washing faces with soap. Soap giveaway. | Last event | 1 h to 1 h and 30 min |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Collin, C.; Biran, A.; Czerniewska, A.; Legesse, D.; Guye, M.; Mume, A.A.; Etu, E.S.; Abashawl, A.; Alemayehu, W.; Dodson, S.; et al. Translating Formative Research into Intervention Content: Experiences with Face Washing for Trachoma Control in Rural Ethiopia. Behav. Sci. 2025, 15, 355. https://doi.org/10.3390/bs15030355
Collin C, Biran A, Czerniewska A, Legesse D, Guye M, Mume AA, Etu ES, Abashawl A, Alemayehu W, Dodson S, et al. Translating Formative Research into Intervention Content: Experiences with Face Washing for Trachoma Control in Rural Ethiopia. Behavioral Sciences. 2025; 15(3):355. https://doi.org/10.3390/bs15030355
Chicago/Turabian StyleCollin, Claire, Adam Biran, Alexandra Czerniewska, Demitu Legesse, Meseret Guye, Asanti Ahmed Mume, Edao Sinba Etu, Aida Abashawl, Wondu Alemayehu, Sarity Dodson, and et al. 2025. "Translating Formative Research into Intervention Content: Experiences with Face Washing for Trachoma Control in Rural Ethiopia" Behavioral Sciences 15, no. 3: 355. https://doi.org/10.3390/bs15030355
APA StyleCollin, C., Biran, A., Czerniewska, A., Legesse, D., Guye, M., Mume, A. A., Etu, E. S., Abashawl, A., Alemayehu, W., Dodson, S., Abdurahman, O. S., Habtamu, E., Adugna, D., Burton, M. J., Last, A., & Greenland, K. (2025). Translating Formative Research into Intervention Content: Experiences with Face Washing for Trachoma Control in Rural Ethiopia. Behavioral Sciences, 15(3), 355. https://doi.org/10.3390/bs15030355