
Unveiling the Role of Emotion Regulation in the Relationship between Intimate Partner Violence Increases and Post-Traumatic Stress Disorder: A Mediation Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Participants
2.3. Measures
2.3.1. Revised Conflict Tactic Scale (CTS2)
2.3.2. The Perception of Increase of Occurrences of Intimate Partner Violence (PI-IPV)
2.3.3. Difficulties in Emotion Regulation Scale-Short Form (DERS-SF)
2.3.4. Impact of Event Scale Revised (IES-R)
2.4. Data Analysis
2.5. Sample Size Determination
3. Results
3.1. Preliminary Analysis

{kind=link}
{kind=link}
| Descriptive Statistics | Correlations | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | SK | K | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ||
| 1 | Psychological Aggression | 39.890 | 38.380 | 0.930 | 0.019 | - | |||||||
| 2 | Sexual Coercion | 5.316 | 11.337 | 2.744 | 7.366 | 0.422 ** | - | ||||||
| 3 | Physical Assault | 7.954 | 20.408 | 6.062 | 53.020 | 0.606 ** | 0.459 ** | - | |||||
| 4 | Injury | 3.288 | 8.408 | 4.531 | 27.111 | 0.504 ** | 0.355 ** | 0.668 ** | - | ||||
| 5 | Negotiation | 29.246 | 34.731 | 1.489 | 1.671 | 0.051 § | 0.088 § | 0.133 * | 0.091 § | - | |||
| 6 | PI–IPV | 6.581 | 3.926 | 0.621 | 0.449 | 0.418 ** | 0.295 ** | 0.410 ** | 0.342 ** | −0.211 ** | - | ||
| 7 | DERS Total | 45.419 | 14.228 | 0.522 | −0.318 | 0.198 ** | 0.154 ** | 0.134 * | 0.112 § | −0.021 § | 0.207 ** | - | |
| 8 | IES Total | 34.133 | 9.936 | −0.081 | −0.040 | 0.258 ** | 0.218 ** | 0.225 ** | 0.226 ** | −0.102 | 0.287 ** | 0.416 ** | - |
| External Variable | Dependent Variable | β* | β (SE) | 95%CI [L, U] | z-Value | p-Value |
|---|---|---|---|---|---|---|
| Psychological Aggression | DERS Total | 0.172 | 0.044 (0.027) | [−0.008; 0.098] | 1.719 | 0.101 |
| IES Total | 0.156 | 0.040 (0.018) | [0.004; 0.076] | 2.181 | 0.027 | |
| Sexual Coercion | DERS Total | 0.133 | 0.167 (0.085) | [−0.001; 0.335] | 1.674 | 0.052 |
| IES Total | 0.144 | 0.180 (0.057) | [0.067; 0.294] | 3.589 | 0.001 | |
| Physical Assault | DERS Total | 0.011 | 0.005 (0.060) | [−0.113; 0.124] | 0.096 | 0.927 |
| IES Total | −0.007 | −0.003 (0.040) | [−0.084; 0.077] | −0.074 | 0.931 | |
| Injury | DERS Total | 0.009 | 0.016 (0.141) | [−0.261; 0.294] | 0.109 | 0.907 |
| IES Total | 0.019 | 0.033 (0.095) | [−0.154; 0.221] | 0.362 | 0.723 | |
| Negotiation | DERS Total | 0.001 | 0.0003 (0.024) | [−0.047; 0.048] | 0.015 | 0.987 |
| IES Total | −0.090 | −0.025 (0.016) | [−0.058; 0.006] | −1.208 | 0.114 |
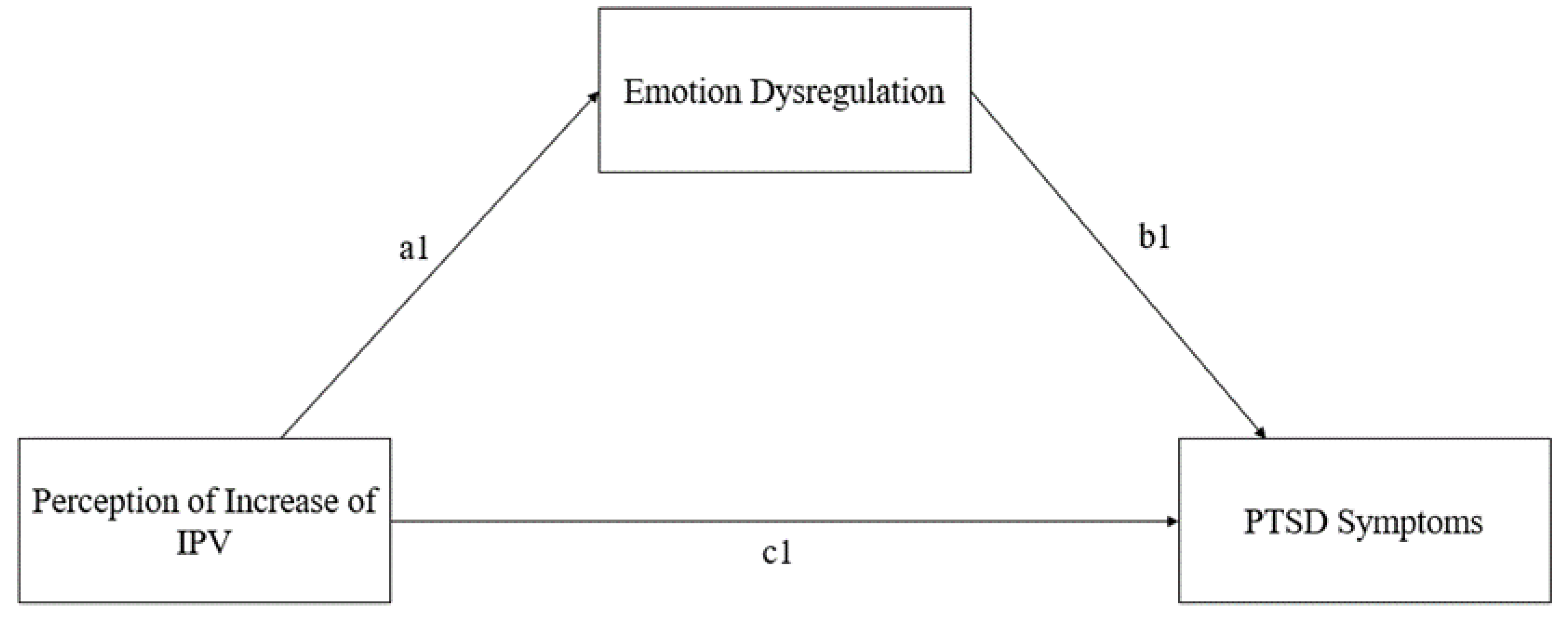
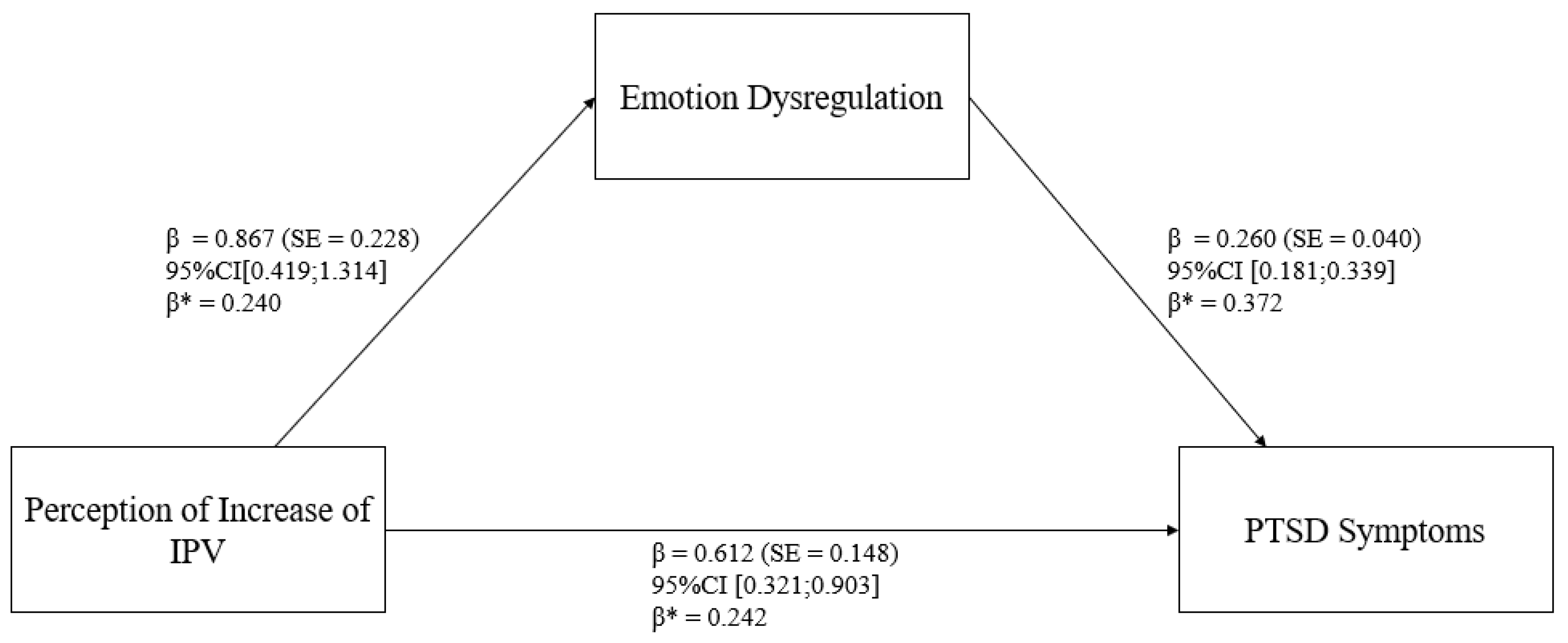
3.2. Mediation Model
4. Discussion
4.1. Clinical Implications
4.2. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krug, G.E.; Dahlberg, L.L.; Mercy, A.J.; Zwi, B.A.; Lozano, R. World Report on Violence and Health; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- WHO. Global, Regional and National Prevalence Estimates for Intimate Partner Violence against Women and Global and Regional Prevalence Estimates for Non-Partner Sexual Violence against Women; WHO: Geneva, Swizterland, 2021. [Google Scholar]
- Gosangi, B.; Park, H.; Thomas, R.; Gujrathi, R.; Bay, C.P.; Raja, A.S.; Seltzer, S.E.; Balcom, M.C.; McDonald, M.L.; Orgill, D.P.; et al. Exacerbation of Physical Intimate Partner Violence during COVID-19 Pandemic. Radiology 2021, 298, E38–E45. [Google Scholar] [CrossRef] [PubMed]
- Mannarini, S.; Balottin, L.; Munari, C.; Gatta, M. Assessing conflict management in the couple: The definition of a latent dimension. Fam. J. 2017, 25, 13–22. [Google Scholar] [CrossRef]
- Cunha, O.; Caridade, S.; de Castro Rodrigues, A.; Cruz, A.R.; Peixoto, M.M. Perpetration of Intimate Partner Violence and COVID-19-Related Anxiety During the Second Lockdown in Portugal: The Mediating Role of Anxiety, Depression, and Stress. J. Fam. Violence 2023, 39, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Ambrosetti, J.; Macheret, L.; Folliet, A.; Wullschleger, A.; Amerio, A.; Aguglia, A.; Serafini, G.; Prada, P.; Kaiser, S.; Bondolfi, G.; et al. Psychiatric emergency admissions during and after COVID-19 lockdown: Short-term impact and long-term implications on mental health. BMC Psychiatry 2021, 21, 1–8. [Google Scholar] [CrossRef]
- Amerio, A.; Lugo, A.; Stival, C.; Fanucchi, T.; Gorini, G.; Pacifici, R.; Odone, A.; Serafini, G.; Gallus, S. COVID-19 lockdown impact on mental health in a large representative sample of Italian adults. J. Affect. Disord. 2021, 292, 398–404. [Google Scholar] [CrossRef]
- Kofman, Y.B.; Garfin, D.R. Home is not always a haven: The domestic violence crisis amid the COVID-19 pandemic. Psychol. Trauma: Theory Res. Pract. Policy 2020, 12, S199–S201. [Google Scholar] [CrossRef]
- Kourti, A.; Stavridou, A.; Panagouli, E.; Psaltopoulou, T.; Spiliopoulou, C.; Tsolia, M.; Sergentanis, T.N.; Tsitsika, A. Domestic Violence During the COVID-19 Pandemic: A Systematic Review. Trauma Violence Abus. 2023, 24, 719–745. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19: EU states report 60% rise in emergency calls about domestic violence. BMJ 2020, 369, m1872. [Google Scholar] [CrossRef]
- Anurudran, A.; Yared, L.; Comrie, C.; Harrison, K.; Burke, T. Domestic violence amid COVID-19. Int. J. Gynaecol. Obs. 2020, 150, 255–256. [Google Scholar] [CrossRef]
- Barbara, G.; Facchin, F.; Micci, L.; Rendiniello, M.; Giulini, P.; Cattaneo, C.; Vercellini, P.; Kustermann, A. COVID-19, Lockdown, and Intimate Partner Violence: Some Data from an Italian Service and Suggestions for Future Approaches. J. Womens Health 2020, 29, 1239–1242. [Google Scholar] [CrossRef]
- Trevillion, K.; Oram, S.; Feder, G.; Howard, L.M. Experiences of Domestic Violence and Mental Disorders: A Systematic Review and Meta-Analysis. PLoS ONE 2012, 7, e51740. [Google Scholar] [CrossRef] [PubMed]
- Bailey, K.; Trevillion, K.; Gilchrist, G. What works for whom and why: A narrative systematic review of interventions for reducing post-traumatic stress disorder and problematic substance use among women with experiences of interpersonal violence. J. Subst. Abus. Treat. 2019, 99, 88–103. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.G.; McNiff, J.; Clapp, J.D.; Olsen, S.A.; Avery, M.L.; Hagewood, J.H. Exploring negative emotion in women experiencing intimate partner violence: Shame, guilt, and PTSD. Behav. Ther. 2011, 42, 740–750. [Google Scholar] [CrossRef]
- Beeble, M.L.; Bybee, D.; Sullivan, C.M.; Adams, A.E. Main, mediating, and moderating effects of social support on the well-being of survivors of intimate partner violence across 2 years. J. Consult. Clin. Psychol. 2009, 77, 718–729. [Google Scholar] [CrossRef]
- Nathanson, A.M.; Shorey, R.C.; Tirone, V.; Rhatigan, D.L. The Prevalence of Mental Health Disorders in a Community Sample of Female Victims of Intimate Partner Violence. Partn. Abus. 2012, 3, 59–75. [Google Scholar] [CrossRef]
- Taccini, F.; Mannarini, S. How Are Survivors of Intimate Partner Violence and Sexual Violence Portrayed on Social Media? J. Media Psychol. 2024. [Google Scholar] [CrossRef]
- APA. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; Raffaello Cortina Editore: Milano, Italy, 2013. [Google Scholar]
- Weiss, N.H.; Darosh, A.G.; Contractor, A.A.; Forkus, S.R.; Dixon-Gordon, K.L.; Sullivan, T.P. Heterogeneity in emotion regulation difficulties among women victims of domestic violence: A latent profile analysis. J. Affect. Disord. 2018, 239, 192–200. [Google Scholar] [CrossRef]
- Rossi, A.A.; Panzeri, A.; Taccini, F.; Parola, A.; Mannarini, S. The Rising of the Shield hero. Development of the Post-Traumatic Symptom Questionnaire (PTSQ) and Assessment of the Protective Effect of self-esteem from trauma-related Anxiety and Depression. J. Child Adolesc. Trauma 2022, 17, 83–101. [Google Scholar] [CrossRef] [PubMed]
- Guglielmetti, M.; Serafini, G.; Amore, M.; Martelletti, P. The relation between persistent post-traumatic headache and ptsd: Similarities and possible differences. Int. J. Environ. Res. Public Health 2020, 17, 4024. [Google Scholar] [CrossRef]
- Bogat, G.A.; Levendosky, A.A.; Theran, S.; von Eye, A.; Davidson, W.S. Predicting the psychosocial effects of interpersonal partner violence (IPV). How much does a woman’s history of IPV matter? J. Interpers. Violence 2003, 18, 1271–1291. [Google Scholar] [CrossRef]
- Tran, H.N.; Beck, J.G. Are Peritraumatic Perceptions of Fear/Life Threat and Posttraumatic Negative Self-Conscious Appraisals/Emotions Differentially Associated with PTSD Symptoms? Cogn. Ther. Res. 2019, 43, 272–283. [Google Scholar] [CrossRef]
- Ruork, A.K.; McLean, C.L.; Fruzzetti, A.E. It Happened Matters More Than What Happened: Associations Between Intimate Partner Violence Abuse Type, Emotion Regulation, and Post-Traumatic Stress Symptoms. Violence Against Women 2021, 28, 1158–1170. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Hughes, M.; Unterstaller, U. Post-traumatic stress disorder (PTSD) in victims of domestic violence: A review of the research. Trauma Violence Abus. 2001, 2, 99–119. [Google Scholar] [CrossRef]
- Becker, K.D.; Stuewig, J.; McCloskey, L.A. Traumatic stress symptoms of women exposed to different forms of childhood victimization and intimate partner violence. J. Interpers. Violence 2010, 25, 1699–1715. [Google Scholar] [CrossRef]
- Chandra, P.S.; Satyanarayana, V.A.; Carey, M.P. Women reporting intimate partner violence in India: Associations with PTSD and depressive symptoms. Arch. Women’s Ment. Health 2009, 12, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Tomkins, J.; Jolliffe Simpson, A.D.; Polaschek, D.L.L. High-risk Victims of Intimate Partner Violence: An Examination of Abuse Characteristics, Psychosocial Vulnerabilities and Reported Revictimization. J. Fam. Violence 2023. [Google Scholar] [CrossRef]
- Krause, E.D.; Kaltman, S.; Goodman, L.; Dutton, M.A. Role of distinct PTSD symptoms in intimate partner reabuse: A prospective study. J. Trauma Stress 2006, 19, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Kuijpers, K.F.; van der Knaap, L.M.; Winkel, F.W. Risk of Revictimization of Intimate Partner Violence: The Role of Attachment, Anger and Violent Behavior of the Victim. J. Fam. Violence 2012, 27, 33–44. [Google Scholar] [CrossRef]
- Iverson, K.M.; Litwack, S.D.; Pineles, S.L.; Suvak, M.K.; Vaughn, R.A.; Resick, P.A. Predictors of intimate partner violence revictimization: The relative impact of distinct PTSD symptoms, dissociation, and coping strategies. J. Trauma Stress 2013, 26, 102–110. [Google Scholar] [CrossRef]
- Lilly, M.M.; London, M.J.; Bridgett, D.J. Using SEM to examine emotion regulation and revictimization in predicting PTSD symptoms among childhood abuse survivors. Psychol. Trauma Theory Res. Pract. Policy 2014, 6, 644. [Google Scholar] [CrossRef]
- Costa, E.C.V.; Botelheiro, A.A.L.P. The impact of intimate partner violence on psychological well-being: Predictors of posttraumatic stress disorder and the mediating role of insecure attachment styles. Eur. J. Trauma Dissociation 2021, 5, 100151. [Google Scholar] [CrossRef]
- Babcock, J.C.; Roseman, A.; Green, C.E.; Ross, J.M. Intimate partner abuse and PTSD symptomatology: Examining mediators and moderators of the abuse-trauma link. J. Fam. Psychol. JFP J. Div. Fam. Psychol. Am. Psychol. Assoc. (Div. 43) 2008, 22, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Ehring, T.; Quack, D. Emotion regulation difficulties in trauma survivors: The role of trauma type and PTSD symptom severity. Behav. Ther. 2010, 41, 587–598. [Google Scholar] [CrossRef]
- Gratz, K.L.; Roemer, L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Kraiss, J.T.; ten Klooster, P.M.; Moskowitz, J.T.; Bohlmeijer, E.T. The relationship between emotion regulation and well-being in patients with mental disorders: A meta-analysis. Compr. Psychiatry 2020, 102, 152189. [Google Scholar] [CrossRef] [PubMed]
- Sloan, E.; Hall, K.; Moulding, R.; Bryce, S.; Mildred, H.; Staiger, P.K. Emotion regulation as a transdiagnostic treatment construct across anxiety, depression, substance, eating and borderline personality disorders: A systematic review. Clin. Psychol. Rev. 2017, 57, 141–163. [Google Scholar] [CrossRef]
- Verzeletti, C.; Zammuner, V.L.; Galli, C.; Agnoli, S. Emotion regulation strategies and psychosocial well-being in adolescence. Cogent Psychol. 2016, 3, 1199294. [Google Scholar] [CrossRef]
- Taccini, F.; Rossi, A.A.; Mannarini, S. Women’s EmotionS, Trauma and EmpowErMent (W-ES.T.EEM) study protocol: A psychoeducational support intervention for victims of domestic violence—A randomised controlled trial. BMJ Open 2022, 12, e060672. [Google Scholar] [CrossRef]
- Taccini, F.; Domoney, J.; Ocloo, J.; Heslin, M.; Byford, S.; Bick, D.; Howard, L.M.; MacMillan, H.; Mannarini, S.; Ramchandani, P.; et al. ‘It’s so Beneficial to be Able to Stop the Cycle’: Perceptions of Intergenerational Transmission of Violence and Parenting Practices Among Pregnant Women and their Abusive Partners. J. Fam. Violence 2024. [Google Scholar] [CrossRef]
- Puente-Martínez, A.; Ubillos-Landa, S.; Rovira, D.P. The mediating role of response-focused emotion regulation strategies in intimate partner violence across the stages of change. Curr. Psychol. 2024, 43, 14604–14618. [Google Scholar] [CrossRef]
- Simpson, L.E.; Raudales, A.M.; Reyes, M.E.; Sullivan, T.P.; Weiss, N.H. Intimate Partner Violence and Posttraumatic Stress Symptoms: Indirect Effects Through Negative and Positive Emotion Dysregulation. J. Interpers. Violence 2022, 37, NP14008–NP14035. [Google Scholar] [CrossRef] [PubMed]
- Katz, L.F.; Gurtovenko, K. Posttraumatic stress and emotion regulation in survivors of intimate partner violence. J. Fam. Psychol. JFP J. Div. Fam. Psychol. Am. Psychol. Assoc. (Div. 43) 2015, 29, 528–536. [Google Scholar] [CrossRef]
- Goldsmith, R.E.; Chesney, S.A.; Heath, N.M.; Barlow, M.R. Emotion Regulation Difficulties Mediate Associations Between Betrayal Trauma and Symptoms of Posttraumatic Stress, Depression, and Anxiety. J. Trauma Stress 2013, 26, 376–384. [Google Scholar] [CrossRef]
- Mannarini, S.; Balottin, L.; Palmieri, A.; Carotenuto, F. Emotion regulation and parental bonding in families of adolescents with internalizing and externalizing symptoms. Front. Psychol. 2018, 9, 1493. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.W.; Kaloupek, D.G.; Dillon, A.L.; Keane, T.M. Externalizing and internalizing subtypes of combat-related PTSD: A replication and extension using the PSY-5 scales. J. Abnorm. Psychol. 2004, 113, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Weiss, N.H.; Nelson, R.J.; Contractor, A.A.; Sullivan, T.P. Emotion dysregulation and posttraumatic stress disorder: A test of the incremental role of difficulties regulating positive emotions. Anxiety Stress Coping 2019, 32, 443–456. [Google Scholar] [CrossRef]
- Taylor, S.; Koch, W.J.; McNally, R.J. How does anxiety sensitivity vary across the anxiety disorders? J. Anxiety Disord. 1992, 6, 249–259. [Google Scholar] [CrossRef]
- Iverson, K.; Shenk, C.; Fruzzetti, A. Dialectical Behavior Therapy for Women Victims of Domestic Abuse: A Pilot Study. Prof. Psychol. Res. Pract. 2009, 40, 242–248. [Google Scholar] [CrossRef]
- Katz, L.F.; Gurtovenko, K.; Maliken, A.; Stettler, N.; Kawamura, J.; Fladeboe, K. An emotion coaching parenting intervention for families exposed to intimate partner violence. Dev. Psychol. 2020, 56, 638–651. [Google Scholar] [CrossRef]
- Muñoz-Rivas, M.; Bellot, A.; Montorio, I.; Ronzón-Tirado, R.; Redondo, N. Profiles of Emotion Regulation and Post-Traumatic Stress Severity among Female Victims of Intimate Partner Violence. Int. J. Environ. Res. Public Health 2021, 18, 6865. [Google Scholar] [CrossRef]
- Straus, M.; Hamby, S.; Boney-McCoy, S.; Sugarman, D. The Revised Conflict Tactics Scales (CTS2): Development and Preliminary Psychometric Data. J. Fam. Issues 1996, 17, 283–316. [Google Scholar] [CrossRef]
- Signorelli, M.; Arcidiacono, E.; Musumeci, G.; Di Nuovo, S.; Aguglia, E. Detecting Domestic Violence: Italian Validation of Revised Conflict Tactics Scale (CTS-2). J. Fam. Violence 2014, 29, 361–369. [Google Scholar] [CrossRef]
- Taccini, F.; Rossi, A.A.; Mannarini, S. Understanding the role of self-esteem and emotion dysregulation in victims of intimate partner violence. Fam. Process 2024. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, E.A.; Xia, M.; Fosco, G.; Yaptangco, M.; Skidmore, C.R.; Crowell, S.E. The Difficulties in Emotion Regulation Scale Short Form (DERS-SF): Validation and Replication in Adolescent and Adult Samples. J. Psychopathol. Behav. Assess. 2016, 38, 443–455. [Google Scholar] [CrossRef]
- Rossi, A.A.; Panzeri, A.; Mannarini, S. The Italian Version of the Difficulties in Emotion Regulation Scale—Short Form (IT-DERS-SF): A Two-step Validation Study. J. Psychopathol. Behav. Assess. 2023, 45, 572–590. [Google Scholar] [CrossRef]
- Weiss, D.S.; Marmar, C. The Impact of Events Scale—Revised. In Assessing Psychological Trauma and PTSD; Wilson, J.P., Keane, T., Eds.; Guilford Press: New York, NY, USA, 1997; Volume 19, pp. 399–411. [Google Scholar]
- Craparo, G.; Faraci, P.; Rotondo, G.; Gori, A. The Impact of Event Scale—Revised: Psychometric properties of the Italian version in a sample of flood victims. Neuropsychiatr. Dis. Treat. 2013, 9, 1427–1432. [Google Scholar] [CrossRef] [PubMed]
- Creamer, M.; Bell, R.; Failla, S. Psychometric properties of the Impact of Event Scale—Revised. Behav. Res. Ther. 2003, 41, 1489–1496. [Google Scholar] [CrossRef]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Ahmed Khan, F.; Napolean Shanmugam, G.; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef]
- Rodríguez-Rey, R.; Garrido-Hernansaiz, H.; Collado, S. Psychological Impact and Associated Factors During the Initial Stage of the Coronavirus (COVID-19) Pandemic Among the General Population in Spain. Front. Psychol. 2020, 11, 1540. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- R Core Team. The R Project for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- Rosseel, Y. lavaan: An R package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Rosseel, Y.; Oberski, D.; Byrnes, J.; Vanbrabant, L.; Savalei, V.; Merkle, E.; Hallquist, M.; Rhemtulla, M.; Katsikatsou, M.; Barendse, M. Package ‘lavaan’. 2015. Available online: https://cran.r-project.org/web/packages/lavaan/index.html (accessed on 1 September 2024).
- Backhaus, K.; Erichson, B.; Plinke, W.; Weiber, R. Multivariate Analysemethoden. Eine Anwendungsorientierte Einführung. 11. Auflage; Springer: Amsterdam, The Netherlands, 2010; p. 583. [Google Scholar]
- Revelle, W. Psych: Procedures for Personality and Psychological Research. 2018. Available online: https://cran.r-project.org/web/packages/psych/index.html (accessed on 1 September 2024).
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Bache, S.; Wickham, H. magrittr: A Forward-Pipe Operator for R. Available online: https://cran.r-project.org/web/packages/magrittr/magrittr.pdf (accessed on 1 September 2024).
- Wickham, H.; François, R.; Henry, L.; Müller, K.; Vaughan, D. dplyr: A Grammar of Data Manipulation. Available online: https://dplyr.tidyverse.org (accessed on 1 September 2024).
- Bernaards, C.; Jennrich, R. Gradient Projection Algorithms and Software for Arbitrary Rotation Criteria in Factor Analysis. Educ. Psychol. Meas. 2005, 65, 676–696. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 3rd ed.; Guilford Publications: New York, NY, USA, 2022. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Pearson: Harlow, UK, 2014. [Google Scholar]
- Satorra, A.; Bentler, P.M. A scaled difference chi-square test statistic for moment structure analysis. Psychometrika 2001, 66, 507–514. [Google Scholar] [CrossRef]
- Peitzmeier, S.M.; Fedina, L.; Ashwell, L.; Herrenkohl, T.I.; Tolman, R. Increases in Intimate Partner Violence During COVID-19: Prevalence and Correlates. J. Interpers. Violence 2022, 37, Np20482–Np20512. [Google Scholar] [CrossRef]
- Moreira, D.N.; Pinto da Costa, M. The impact of the Covid-19 pandemic in the precipitation of intimate partner violence. Int. J. Law Psychiatry 2020, 71, 101606. [Google Scholar] [CrossRef]
- Villalta, L.; Khadr, S.; Chua, K.C.; Kramer, T.; Clarke, V.; Viner, R.M.; Stringaris, A.; Smith, P. Complex post-traumatic stress symptoms in female adolescents: The role of emotion dysregulation in impairment and trauma exposure after an acute sexual assault. Eur. J. Psychotraumatol. 2020, 11, 1710400. [Google Scholar] [CrossRef]
- Hechtman, L.A.; Raila, H.; Chiao, J.Y.; Gruber, J. Positive Emotion Regulation and Psychopathology: A Transdiagnostic Cultural Neuroscience Approach. J. Exp. Psychopathol. 2013, 4, 502–528. [Google Scholar] [CrossRef] [PubMed]
- Quoidbach, J.; Mikolajczak, M.; Gross, J.J. Positive interventions: An emotion regulation perspective. Psychol. Bull. 2015, 141, 655–693. [Google Scholar] [CrossRef]
- Abravanel, B.T.; Sinha, R. Emotion dysregulation mediates the relationship between lifetime cumulative adversity and depressive symptomatology. J. Psychiatr. Res. 2015, 61, 89–96. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Sawyer, A.T.; Fang, A.; Asnaani, A. Emotion dysregulation model of mood and anxiety disorders. Depress. Anxiety 2012, 29, 409–416. [Google Scholar] [CrossRef]
- Orgeta, V. Emotion dysregulation and anxiety in late adulthood. J. Anxiety Disord. 2011, 25, 1019–1023. [Google Scholar] [CrossRef] [PubMed]
- Weiss, N.H.; Tull, M.T.; Lavender, J.; Gratz, K.L. Role of emotion dysregulation in the relationship between childhood abuse and probable PTSD in a sample of substance abusers. Child Abus. Negl. 2013, 37, 944–954. [Google Scholar] [CrossRef]
- Siegel, J.P. Breaking the Links in Intergenerational Violence: An Emotional Regulation Perspective. Fam. Process 2013, 52, 163–178. [Google Scholar] [CrossRef]
- Cloitre, M.; Scarvalone, P.; Difede, J. Posttraumatic Stress Disorder, Self- and Interpersonal Dysfunction Among Sexually Retraumatized Women. J. Trauma. Stress 1997, 10, 437–452. [Google Scholar] [CrossRef]
- Bouthillier, D.; Julien, D.; Dubé, M.; Bélanger, I.; Hamelin, M. Predictive Validity of Adult Attachment Measures in Relation to Emotion Regulation Behaviors in Marital Interactions. J. Adult Dev. 2002, 9, 291–305. [Google Scholar] [CrossRef]
- Colombo, D.; Fernández-Álvarez, J.; García Palacios, A.; Cipresso, P.; Botella, C.; Riva, G. New Technologies for the Understanding, Assessment, and Intervention of Emotion Regulation. Front. Psychol. 2019, 10, 1261. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.A.; Marconi, M.; Taccini, F.; Verusio, C.; Mannarini, S. Screening for Distress in Oncological Patients: The Revised Version of the Psychological Distress Inventory (PDI-R). Front. Psychol. 2022, 13, 859478. [Google Scholar] [CrossRef] [PubMed]
- Cloitre, M.; Koenen, K.C.; Cohen, L.R.; Han, H. Skills training in affective and interpersonal regulation followed by exposure: A phase-based treatment for PTSD related to childhood abuse. J. Consult. Clin. Psychol. 2002, 70, 1067–1074. [Google Scholar] [CrossRef]
- Trombetta, T.; Rollè, L. Intimate Partner Violence Perpetration Among Sexual Minority People and Associated Factors: A Systematic Review of Quantitative Studies. Sex. Res. Soc. Policy 2022, 20, 886–935. [Google Scholar] [CrossRef]
- Trombetta, T.; Balocco, V.; Santoniccolo, F.; Paradiso, M.N.; Rollè, L. Internalized Homonegativity, Emotion Dysregulation, and Isolating Behaviors Perpetration among Gay and Lesbian Couples. Int. J. Environ. Res. Public Health 2023, 20, 1593. [Google Scholar] [CrossRef]
- Mannarini, S.; Taccini, F.; Rossi, A.A. The Role of Alexithymia and Impulsivity in Male Victims and Perpetrators of Intimate Partner Violence. Behav. Sci. 2023, 13, 402. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cheng, Z. Cross-sectional studies: Strengths, weaknesses, and recommendations. Chest 2020, 158, S65–S71. [Google Scholar] [CrossRef] [PubMed]
| Path | β* | β (SE) | 95% CI [L-U] | z-Value | R2 | |
|---|---|---|---|---|---|---|
| Outcome: DERS Total (M) Perception of Increase of IPV (X) → DERS Total (M) | (a1) | 0.240 | 0.867 (0.228) | [0.419; 1.314] | 3.796 *** | 0.057 |
| Outcome: PTSD Symptoms (Y) DERS Total (M) → PTSD Symptoms (Y) Perception of Increase of IPV (X) → PTSD Symptoms (Y) | (b1) (c1) | 0.372 0.242 | 0.260 (0.040) 0.612 (0.148) | [0.181; 0.339] [0.321; 0.903] | 6.455 *** 0.413 *** | 0.242 |
| Effect of X on Y via M | (a1*b1) | 0.089 | 0.225 (0.069) | [0.090; 0.361] | 3.269 *** | |
| Total Effect of the Model | 0.022 | 0.138 (0.043) | [0.054; 0.222] | 3.211 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taccini, F.; Rossi, A.A.; Mannarini, S. Unveiling the Role of Emotion Regulation in the Relationship between Intimate Partner Violence Increases and Post-Traumatic Stress Disorder: A Mediation Analysis. Behav. Sci. 2024, 14, 799. https://doi.org/10.3390/bs14090799
Taccini F, Rossi AA, Mannarini S. Unveiling the Role of Emotion Regulation in the Relationship between Intimate Partner Violence Increases and Post-Traumatic Stress Disorder: A Mediation Analysis. Behavioral Sciences. 2024; 14(9):799. https://doi.org/10.3390/bs14090799
Chicago/Turabian StyleTaccini, Federica, Alessandro Alberto Rossi, and Stefania Mannarini. 2024. "Unveiling the Role of Emotion Regulation in the Relationship between Intimate Partner Violence Increases and Post-Traumatic Stress Disorder: A Mediation Analysis" Behavioral Sciences 14, no. 9: 799. https://doi.org/10.3390/bs14090799
APA StyleTaccini, F., Rossi, A. A., & Mannarini, S. (2024). Unveiling the Role of Emotion Regulation in the Relationship between Intimate Partner Violence Increases and Post-Traumatic Stress Disorder: A Mediation Analysis. Behavioral Sciences, 14(9), 799. https://doi.org/10.3390/bs14090799