
Digital Platform for the Prevention of Suicidal Behaviour and Non-Suicidal Self-Injuries in Adolescents: The SmartCrisis-Teen Study Protocol

 , , , , , , and
, , , , , , and 
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
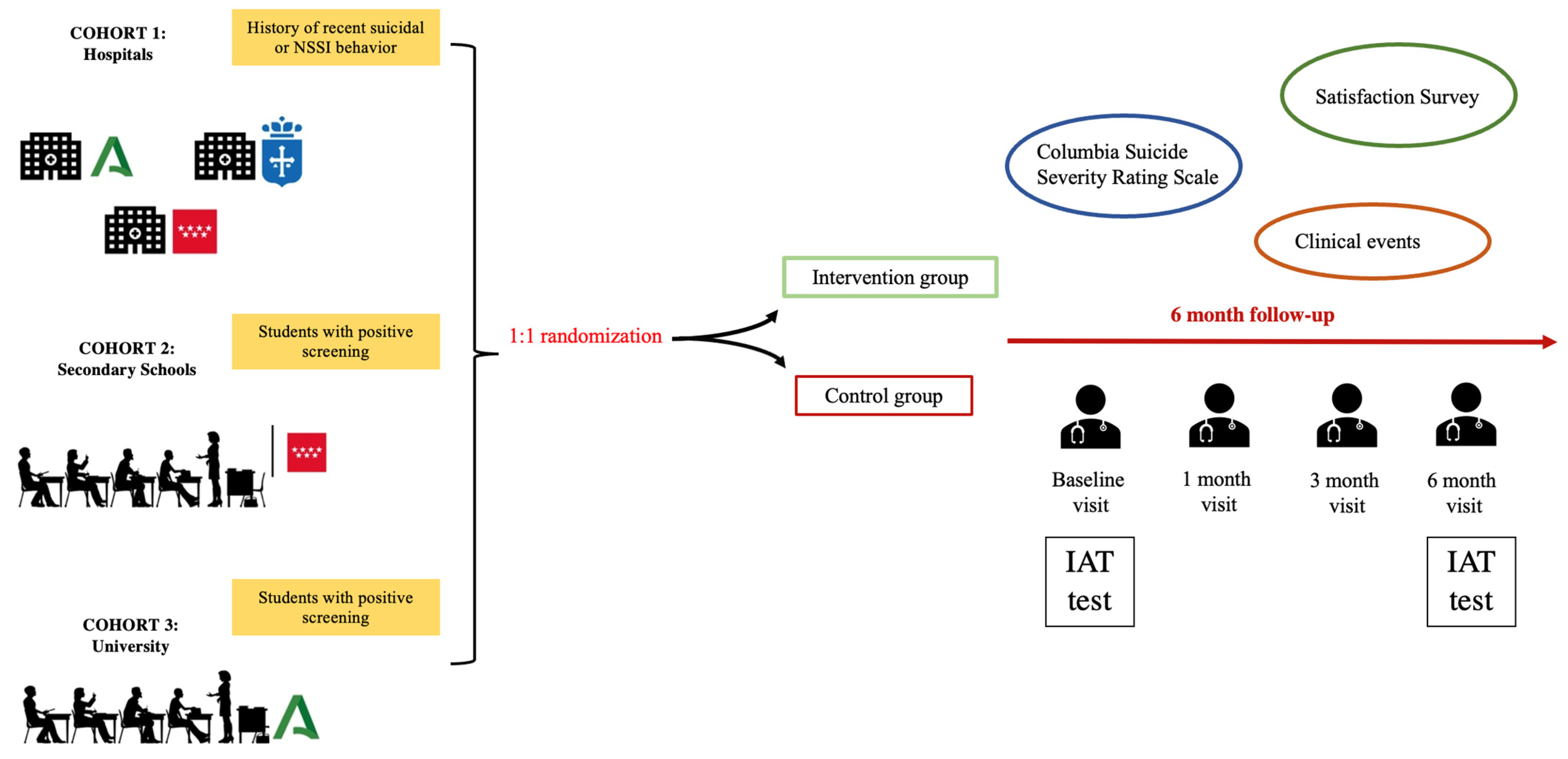
2.1. Setting and Design
2.2. Sample
2.2.1. Cohort 1: Clinical Setting
- Being between 13 and 17 years old.
- Presenting a suicide attempt or an NSSI in the month previous to recruitment.
- Being able to understand the project and being interested in participating.
- Having parents or legal guardians capable of signing the informed consent.
- Being fluent in Spanish.
- Owning a smartphone with internet access and iOS or Android operating system.
- Refusal to install the mobile application.
- Any circumstance or indication that discourages the regular use of a mobile phone (e.g., addiction to new technologies).
2.2.2. Cohort 2: High School
- Being between 13 and 17 years old.
- Testing positive in the screening that will be carried out at the centers (explained below).
- Being able to understand the project and being interested in participating
- Having parents or legal guardians capable of signing the informed consent.
- Being fluent in Spanish
- Owning a smartphone with internet access and iOS or Android operating system.
- Refusal to install the mobile application.
- Any circumstance or indication that discourages the regular use of a mobile phone (e.g., addiction to new technologies).
2.2.3. Cohort 3: University Setting
- Testing positive in the screening that will be carried out at the center (explained below).
- Being able to understand the project and being interested in participating.
- Being capable of signing the informed consent.
- Being fluent in Spanish.
- Owning a smartphone with internet access and iOS or Android operating system.
- Refusal to install the mobile application.
- Any circumstance or indication that discourages the regular use of a mobile phone (e.g., addiction to new technologies).
2.3. Sample Size Calculation
2.4. General Procedure:
2.5. Procedure: Clinical Setting
2.6. Procedure: High School and University Setting
2.7. Randomization and Follow-Up
2.8. Psychometric Assessment
2.9. Implicit Association Test
2.10. Ecological Momentary Assessment
- Suicidality: 4 questions;
- Non-suicidal self-injury: 2 questions;
- Affect: 9 questions;
- Interpersonal experiences: 11 questions;
- Sleep: 4 questions;
- Apetite and eating: 3 questions.
2.11. Assessments: Questionnaires
- Sociodemographic data including gender, age, family socioeconomic status, grade repetition, sexual orientation, number of siblings (including the participant) and child adoption.
- The Columbia Suicide Severity Rating Scale (CSSRS) [34] will be administered to measure suicide ideation and behavior. This scale will be employed both in the basal and the follow-up appointments.
- In addition, we will verify suicide attempts and suicide deaths through the digital medical record (clinical events).
- The Inventory for Depressive Symptomatology—Clinical (IDSC-30) scale [49] will be administered in order to measure depressive signs and symptoms.
- MacLean Screening Instrument for Borderline Personality Disorder [50].
- The Spanish version of the Death/Suicide Implicit Association Test (D/S-IAT) [38]
- Satisfaction surveys (one qualitative and one quantitative satisfaction survey).
2.12. Assessment Criteria
- The occurrence of suicidal behavior as a clinical event (completed suicide, attempted suicide, ED visit for suicidal ideation, ED visit for self-harm),
- Predictive validity of the D/S IAT and SI IAT tests to clinical events recorded during follow-up.
- Acceptability of the project through user-perceived satisfaction.
- Project feasibility measured by participation and retention.
Treatment as Usual (TAU)
2.13. Statistical Analysis
3. Limitations
4. Expected Results
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Ecological Momentary Assessment (EMA) Questionnaire
| Category | Variable | Question | Minimum Value | Maximum Value | Scoring |
| Suicidality (4 questions) | Pasive SI | My wish to live is | No wish to live | Maximum wish lo live | 1–7 |
| My wish to die is | No wish to die | Maximum wish to die | 1–7 | ||
| Do you have thoughts of hurting yourself in some way? | Not at all | Nearly every day | 0–3 | ||
| Active SI | Are you able to keep yourself safe right now? | I definitely can keep myself safe | I definitely cannot keep myself safe | 1–5 | |
| Non-Suicidal Self-Injuries (2 questions) | NSSIs | At any point in the last 24 h, did you harm yourself on purpose? | Yes | No | Yes/No |
| Since the last prompt, have you felt an urge or wanted to harm or injure yourself on purpose? | Not at all | Extremely | 1–5 | ||
| Affect (9 questions) | Psychological pain | I feel psychological pain | No pain | Maximum pain | 1–7 |
| Stress | I feel stressed out today (with pressure, overwhelmed) | No stress | Maximum stress | 1–7 | |
| Restlessness | I feel restless (agitates), with the need to keep moving | No restlessness | Maximum restlessness | 1–7 | |
| Hopelessness | I feel full of hope | No hope | Maximum hope | 1–7 | |
| Self-hatred | I feel hatred or anger towards myself | No hatred | Maximum hatred | 1–7 | |
| Hatred of others | I feel hatred or anger towards others | No hatred | Maximum hatred | 1–7 | |
| Anxiety | At this moment I feel nervous | Very slightly or not at all | Extremely | 1–5 | |
| Sadness | At this moment I feel sad | Very slightly or not at all | Extremely | 1–5 | |
| Happiness | At this moment I feel happy | Very slightly or not at all | Extremely | 1–5 | |
| Interpersonal experiences (11 questions) | Thwarted belongingness | I wish there was a trusted person with whom I can talk about all my personal issues | Not at all | Absolutely | 1–7 |
| I feel like an outsider | Not at all | Absolutely | 1–7 | ||
| Lack of recognition | I wish I received more recognition and love from others | Not at all | Absolutely | 1–7 | |
| Lack of independence | I have the impression that important people around me want to decide for me what I should think and do | Not at all | Absolutely | 1–7 | |
| Criticism | Since the last prompt have you felt insulted or criticized? | Not at all | Extremely | 1–5 | |
| Thwarted belongingness | Since the last prompt have you felt rejected, abandoned, excluded or left out? | Not at all | Extremely | 1–5 | |
| Perceived burdensomeness | I believe I am contributing to the well-being of my family/friends | Not at all | Absolutely | 1–7 | |
| believe I am contributing to the well-being of the people around me | Not at all | Absolutely | 1–7 | ||
| I feel disconnected from other people | Not at all | Absolutely | 1–7 | ||
| I feel like a burden to others | Not at all true for me | Very true for me | 1–7 | ||
| I feel useless | Not at all true for me | Very true for me | 1–7 | ||
| Sleep (4 questions) | Sleep maintenance | Last night I had trouble staying sleep | None | Very severe | 0–4 |
| Sleep-derived quality of life | Others think that sleep problems affect my quality of life | Not at all | Absolutely | 0–4 | |
| Sleep dissatisfaction | Today I am satisfied with my sleep | Very unsatisfied | Very satisfied | 0–4 | |
| Sleep-derived interference with daily activity | My sleep problems are interfering with my daily activity | Not at all | Very much | 0–4 | |
| Appetite and eating (3 questions) | Appetite | In the last few days, I have been hungry | Never | All the time | 0–4 |
| Taste | In the last days when I eat, the food tastes | Very bad | Very good | 0–4 | |
| Number of meals | In the last few days, I usually do | Less than one meal a day | More thn three meals a day | 0–4 |
References
- Orben, A.; Lucas, R.E.; Fuhrmann, D.; Kievit, R.A. Trajectories of adolescent life satisfaction. R. Soc. Open Sci. 2022, 9, 211808. [Google Scholar] [CrossRef] [PubMed]
- Plataforma Nacional para el Estudio y la Prevención del Suicidio. Detección de la Conducta Suicida en el Contexto Educativo: The Episam-School Study. 2023. Available online: https://www.plataformanacionalsuicidio.es/estudios-de-cohorte/detection-of-suicidal-behavior-in-the-educational-context-the-episam-school-study (accessed on 7 December 2023).
- Kieling, C.; Baker-Henningham, H.; Belfer, M.; Conti, G.; Ertem, I.; Omigbodun, O.; Rohde, L.A.; Srinath, S.; Ulkuer, N.; Rahman, A. Child and adolescent mental health worldwide: Evidence for action. Lancet 2011, 378, 1515–1525. [Google Scholar] [CrossRef] [PubMed]
- Meherali, S.; Punjani, N.; Louie-Poon, S.; Abdul Rahim, K.; Das, J.K.; Salam, R.A.; Lassi, Z.S. Mental Health of Children and Adolescents Amidst COVID-19 and Past Pandemics: A Rapid Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 3432. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- WHO. Suicide. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 12 September 2022).
- Hinze, V.; Ford, T.; Gjelsvik, B.; Byford, S.; Cipriani, A.; Montero-Marin, J.; Ganguli, P. Service use and costs in adolescents with pain and suicidality: A cross-sectional study. EClinicalMedicine 2022, 55, 101778. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Available online: https://www.cdc.gov/injury/wisqars/LeadingCauses.html (accessed on 1 December 2023).
- WHO. Self-Inflicted Injuries. [Internet]. WHO Mortality Database. Available online: https://platform.who.int/mortality/themes/theme-details/topics/indicator-groups/indicator-group-details/MDB/self-inflicted-injuries (accessed on 4 April 2023).
- Victor, S.E.; Klonsky, E.D. Correlates of suicide attempts among self-injurers: A meta-analysis. Clin. Psychol. Rev. 2014, 34, 282–297. [Google Scholar] [CrossRef]
- Goldberg, S.; Israelashvili, M. The distinction between exclusivity and comorbidity within NSSI. Sch. Psychol. Q. 2017, 32, 156–172. [Google Scholar] [CrossRef]
- Bostwick, J.M.; Pabbati, C.; Geske, J.R.; McKean, A.J. Suicide Attempt as a Risk Factor for Completed Suicide: Even More Lethal Than We Knew. Am. J. Psychiatry 2016, 173, 1094–1100. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ghanbari, B.; Malakouti, S.K.; Nojomi, M.; Alavi, K.; Khaleghparast, S. Suicide Prevention and Follow-Up Services: A Narrative Review. Glob. J. Health Sci. 2015, 8, 145–153. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Porras-Segovia, A.; Díaz-Oliván, I.; Gutiérrez-Rojas, L.; Dunne, H.; Moreno, M.; Baca-García, E. Apps for Depression: Are They Ready to Work? Curr. Psychiatry Rep. 2020, 22, 11. [Google Scholar] [CrossRef] [PubMed]
- Manning, V.; Whelan, D.; Piercy, H. The current evidence for substance use disorder apps. Curr. Opin. Psychiatry 2022, 35, 237–245. [Google Scholar] [CrossRef]
- Ananth, S. Sleep apps: Current limitations and challenges. Sleep Sci. 2021, 14, 83–86. [Google Scholar] [CrossRef]
- Anderson, M.; Jiang, J. Teens, Social Media & Technology 2018. Pew Research Center, Recent and Detailed Report of Changes in Trends in Teen Use of Social Media and Technology. 31 May 2018. Available online: http://assets. pewresearch.org/wp-content/uploads/sites/14/2018/05/31102617/PI_2018.05.31_TeensTech_FINAL.pdf (accessed on 27 June 2018).
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological Momentary Assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef]
- McDevitt-Murphy, M.E.; Luciano, M.T.; Zakarian, R.J. Use of ecological momentary assessment and intervention in treatment with adults. Focus 2018, 16, 370–375. [Google Scholar] [CrossRef]
- Berrouiguet, S.; Perez-Rodriguez, M.M.; Larsen, M.; Baca-García, E.; Courtet, P.; Oquendo, M. From eHealth to iHealth: Transition to Participatory and Personalized Medicine in Mental Health. J. Med. Internet Res. 2018, 20, e2. [Google Scholar] [CrossRef]
- Stanley, B.; Brown, G.K. Safety planning intervention: A brief intervention to mitigate suicide risk. Cogn. Behav. Pract. 2012, 19, 256–264. [Google Scholar] [CrossRef]
- Ferguson, M.; Rhodes, K.; Loughhead, M.; McIntyre, H.; Procter, N. The Effectiveness of the Safety Planning Intervention for Adults Experiencing Suicide-Related Distress: A Systematic Review. Arch. Suicide Res. 2022, 26, 1022–1045. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Park, J.M.; Finn, C.T.; Deliberto, T.L.; Dour, H.J.; Banaji, M.R. Measuring the suicidal mind: Implicit cognition predicts suicidal behavior. Psychol. Sci. 2010, 21, 511–517. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nock, M.K.; Banaji, M.R. Assessment of self-injurious thoughts using a behavioral test. Am. J. Psychiatry 2007, 164, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Banaji, M.R. Prediction of suicide ideation and attempts among adolescents using a brief performance-based test. J. Consult. Clin. Psychol. 2007, 75, 707–715. [Google Scholar] [CrossRef]
- Moreno, M.; Gutiérrez-Rojas, L.; Porras-Segovia, A. Implicit Cognition Tests for the Assessment of Suicide Risk: A Systematic Review. Curr. Psychiatry Rep. 2022, 24, 141–159. [Google Scholar] [CrossRef]
- Jiménez-Muñoz, L.; Peñuelas-Calvo, I.; Díaz-Oliván, I.; Gutiérrez-Rojas, L.; Baca-García, E.; Porras-Segovia, A. Suicide Prevention in Your Pocket: A Systematic Review of Ecological Momentary Interventions for the Management of Suicidal Thoughts and Behaviors. Harv. Rev. Psychiatry 2022, 30, 85–99. [Google Scholar] [CrossRef]
- Stallard, P.; Porter, J.; Grist, R. A smartphone app (BlueIce) for young people who self-harm: Open phase 1 pre-post trial. JMIR Mhealth Uhealth 2018, 6, e32. [Google Scholar] [CrossRef] [PubMed]
- Kennard, B.D.; Goldstein, T.; Foxwell, A.A.; McMakin, D.L.; Wolfe, K.; Biernesser, C.; Moorehead, A.; Douaihy, A.; Zullo, L.; Wentroble, E.; et al. As Safe as Possible (ASAP): A brief app-supported inpatient intervention to prevent postdischarge suicidal behavior in hospitalized, suicidal adolescents. Am. J. Psychiatry 2018, 175, 864–872, Erratum in Am. J. Psychiatry 2019, 176, 764. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.W.; Chang, H.J.; Kim, J.A. Development and feasibility of a safety plan mobile application for adolescent suicide attempt survivors. Comput. Inform. Nurs. 2020, 38, 382–392. [Google Scholar] [CrossRef] [PubMed]
- McManama O’Brien, K.H.; LeCloux, M.; Ross, A.; Gironda, C.; Wharff, E.A. A pilot study of the acceptability and usability of a smartphone application intervention for suicidal adolescents and their parents. Arch. Suicide Res. 2017, 21, 254–264. [Google Scholar] [CrossRef]
- Muscara, F.; Ng, O.; Crossley, L.; Lu, S.; Kalisch, L.; Melvin, G.; Gronow, S.; Prakash, C.; Anderson, V. The feasibility of using smartphone apps to manage self-harm and suicidal acts in adolescents admitted to an inpatient mental health ward. Digit. Health 2020, 6, 2055207620975315. [Google Scholar] [CrossRef]
- Morgiève, M.; Genty, C.; Azé, J.; Dubois, J.; Leboyer, M.; Vaiva, G.; Berrouiguet, S.; Courtet, P. A digital companion, the emma app, for ecological momentary assessment and prevention of suicide: Quantitative case series study. JMIR Mhealth Uhealth 2020, 8, e15741. [Google Scholar] [CrossRef] [PubMed]
- Nuij, C.; van Ballegooijen, W.; Ruwaard, J.; De Beurs, D.; Mokkenstorm, J.; van Duijn, E.; de Winter, R.F.P.; O’Connor, R.C.; Smit, J.H.; Riper, H.; et al. Smartphone-based safety planning and self-monitoring for suicidal patients: Rationale and study protocol of the CASPAR (continuous assessment for suicide prevention and research) study. Internet Interv. 2018, 13, 16–23. [Google Scholar] [CrossRef]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S.; et al. The Columbia-Suicide Severity Rating Scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am. J. Psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef]
- Porras-Segovia, A.; De Granda-Beltrán, A.M.; Gallardo, C.; Abascal-Peiró, S.; Barrigón, M.L.; Artés-Rodríguez, A.; López-Castroman, J.; Courtet, P.; Baca-García, E. Smartphone-based safety plan for suicidal crisis: The SmartCrisis 2.0 pilot study. J. Psychiatr. Res. 2024, 169, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Bryan, C.J.; May, A.M.; Rozek, D.C.; Williams, S.R.; Clemans, T.A.; Mintz, J.; Leeson, B.; Burch, T.S. Use of crisis management interventions among suicidal patients: Results of a randomized controlled trial. Depress. Anxiety 2018, 35, 619–628. [Google Scholar] [CrossRef] [PubMed]
- Paykel, E.S.; Myers, J.K.; Lindenthal, J.J.; Tanner, J. Suicidal feelings in the general population: A prevalence study. Br. J. Psychiatry 1974, 124, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Klonsky, E.D.; Glenn, C.R. Assessing the functions of non-suicidal self-injury: Psychometric properties of the Inventory of Statements About Self-injury (ISAS). J. Psychopathol. Behav. Assess. 2009, 31, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Moreno, M.; Porras-Segovia, A.; Lopez-Castroman, J.; Peñuelas-Calvo, I.; Díaz-Oliván, I.; Barrigón, M.L.; Baca-García, E. Validation of the Spanish version of the Death/Suicide Implicit Association Test for the assessment of suicidal behavior. J. Affect. Disord. Rep. 2020, 1, 100012. [Google Scholar] [CrossRef]
- Greenwald, A.G.; Nosek, B.A.; Banaji, M.R. Understanding and using the implicit association test: I. An improved scoring algorithm. J. Personal. Soc. Psychol. 2003, 85, 197. [Google Scholar] [CrossRef]
- Fartacek, C.; Schiepek, G.; Kunrath, S.; Fartacek, R.; Plöderl, M. Real-time monitoring of non-linear suicidal dynamics: Methodology and a demonstrative case report. Front. Psychol. 2016, 7, 130. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Van Orden, K.A.; Cukrowicz, K.C.; Witte, T.K.; Joiner, T.E., Jr. Thwarted belongingness and perceived burdensomeness: Construct validity and psychometric properties of the interpersonal needs questionnaire. Psychol. Assess. 2012, 24, 197–215. [Google Scholar] [CrossRef]
- Kleiman, E.M.; Turner, B.J.; Fedor, S.; Beale, E.E.; Huffman, J.C.; Nock, M.K. Examination of real-time fluctuations in suicidal ideation and its risk factors: Results from two ecological momentary assessment studies. J. Abnorm. Psychol. 2017, 126, 726–738. [Google Scholar] [CrossRef]
- Czyz, E.K.; Glenn, C.R.; Busby, D.; King, C.A. Daily patterns in nonsuicidal self-injury and coping among recently hospitalized youth at risk for suicide. Psychiatry Res. 2019, 281, 112588. [Google Scholar] [CrossRef] [PubMed]
- Oquendo, M.A.; Galfalvy, H.C.; Choo, T.H.; Kandlur, R.; Burke, A.K.; Sublette, M.E.; Miller, J.M.; Mann, J.J.; Stanley, B.H. Highly variable suicidal ideation: A phenotypic marker for stress induced suicide risk. Mol. Psychiatry 2021, 26, 5079–5086. [Google Scholar] [CrossRef] [PubMed]
- Victor, S.E.; Scott, L.N.; Stepp, S.D.; Goldstein, T.R. I want you to want me: Interpersonal stress and affective experiences as within-person predictors of nonsuicidal self-injury and suicide urges in daily life. Suicide Life-Threat. Behav. 2019, 49, 1157–1177. [Google Scholar] [CrossRef] [PubMed]
- Rush, A.J.; Gullion, C.M.; Basco, M.R.; Jarrett, R.B.; Trivedi, M.H. The Inventory of Depressive Symptomatology (IDS): Psychometric properties. Psychol. Med. 1996, 26, 477–486. [Google Scholar] [CrossRef]
- Zanarini, M.C.; Vujanovic, A.A.; Parachini, E.A.; Boulanger, J.L.; Frankenburg, F.R.; Hennen, J. A screening measure for BPD: The McLean screening instrument for borderline personality disorder (MSI-BPD). J. Personal. Disord. 2003, 17, 568–573. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abascal-Peiró, S.; Peñuelas-Calvo, I.; Alacreu-Crespo, A.; Sáiz, P.A.; De la Torre-Luque, A.; Ruiz-Veguilla, M.; Barrigón, M.L.; Courtet, P.; López-Castroman, J.; Baca-García, E.; et al. Digital Platform for the Prevention of Suicidal Behaviour and Non-Suicidal Self-Injuries in Adolescents: The SmartCrisis-Teen Study Protocol. Behav. Sci. 2024, 14, 740. https://doi.org/10.3390/bs14090740
Abascal-Peiró S, Peñuelas-Calvo I, Alacreu-Crespo A, Sáiz PA, De la Torre-Luque A, Ruiz-Veguilla M, Barrigón ML, Courtet P, López-Castroman J, Baca-García E, et al. Digital Platform for the Prevention of Suicidal Behaviour and Non-Suicidal Self-Injuries in Adolescents: The SmartCrisis-Teen Study Protocol. Behavioral Sciences. 2024; 14(9):740. https://doi.org/10.3390/bs14090740
Chicago/Turabian StyleAbascal-Peiró, Sofía, Inmaculada Peñuelas-Calvo, Adrian Alacreu-Crespo, Pilar Alejandra Sáiz, Alejandro De la Torre-Luque, Miguel Ruiz-Veguilla, María Luisa Barrigón, Philippe Courtet, Jorge López-Castroman, Enrique Baca-García, and et al. 2024. "Digital Platform for the Prevention of Suicidal Behaviour and Non-Suicidal Self-Injuries in Adolescents: The SmartCrisis-Teen Study Protocol" Behavioral Sciences 14, no. 9: 740. https://doi.org/10.3390/bs14090740
APA StyleAbascal-Peiró, S., Peñuelas-Calvo, I., Alacreu-Crespo, A., Sáiz, P. A., De la Torre-Luque, A., Ruiz-Veguilla, M., Barrigón, M. L., Courtet, P., López-Castroman, J., Baca-García, E., & Porras-Segovia, A. (2024). Digital Platform for the Prevention of Suicidal Behaviour and Non-Suicidal Self-Injuries in Adolescents: The SmartCrisis-Teen Study Protocol. Behavioral Sciences, 14(9), 740. https://doi.org/10.3390/bs14090740