
Association between Family Functioning, Child Emotional and Behavioral Problems, and Parental Stress during the COVID-19 Pandemic in Thailand

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measurements
2.4. Statistical Analysis
3. Results
3.1. Demographic Data of Participants
3.2. Effect of the COVID-19 Pandemic on Children’s Daily Activities
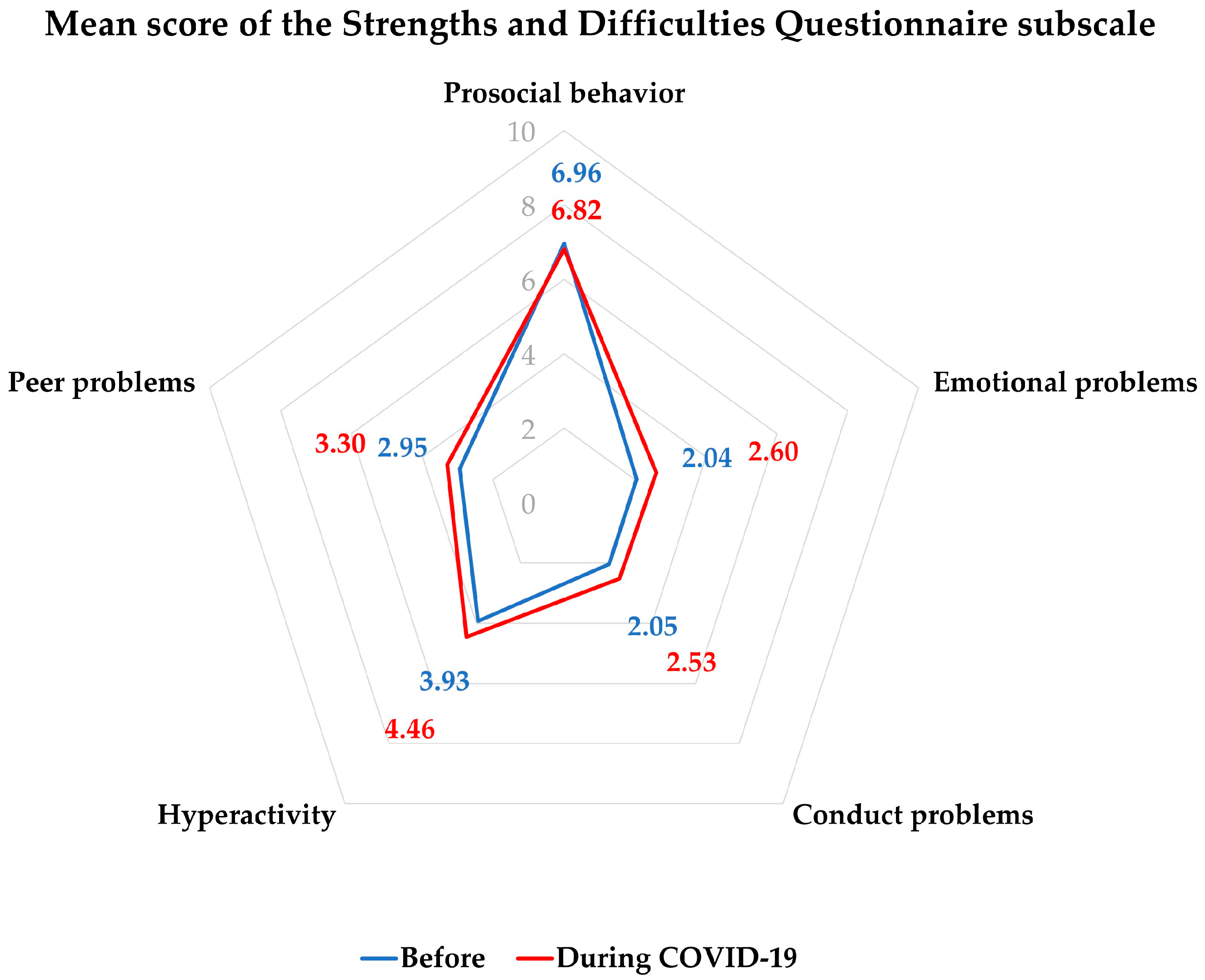
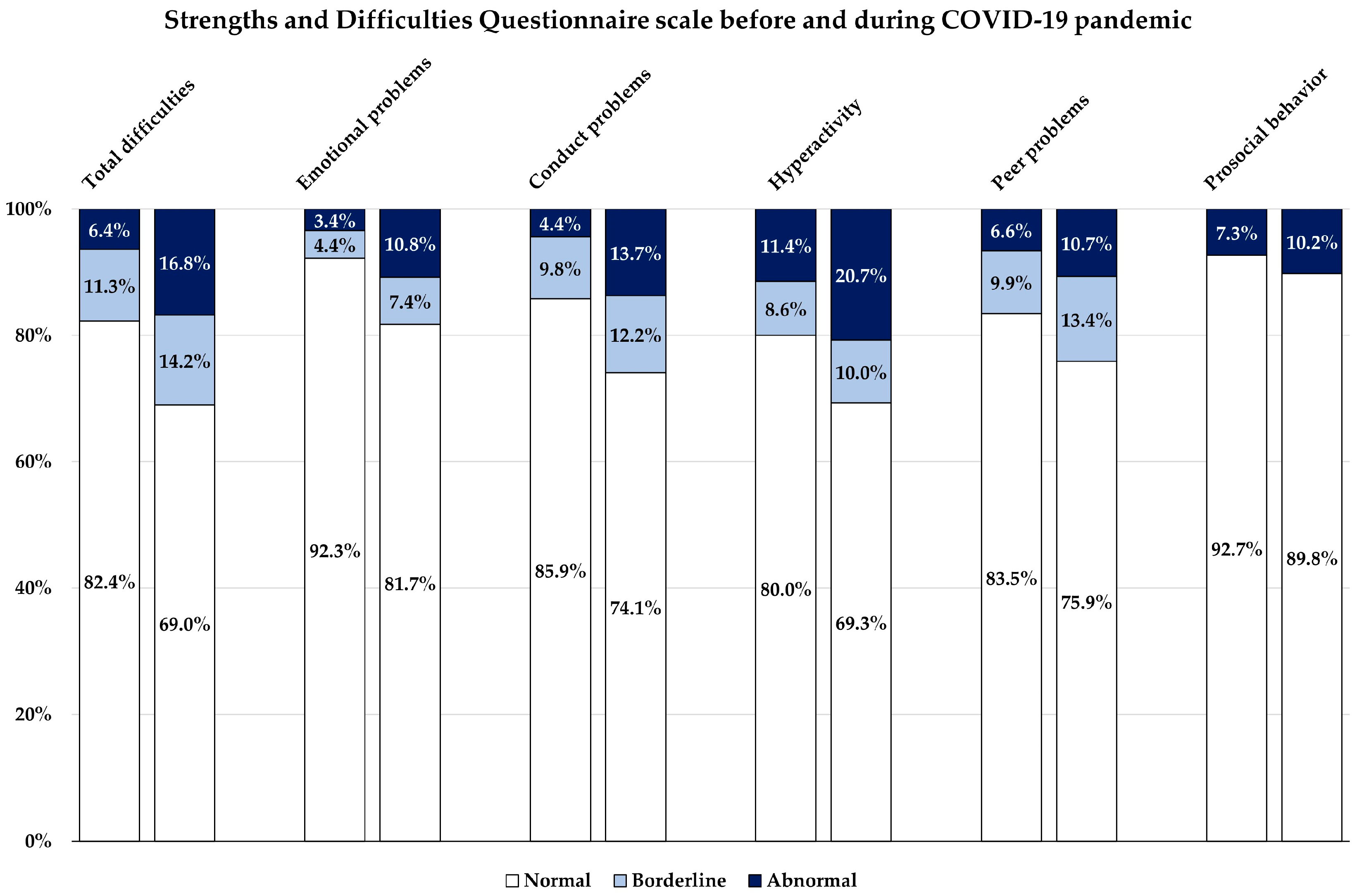
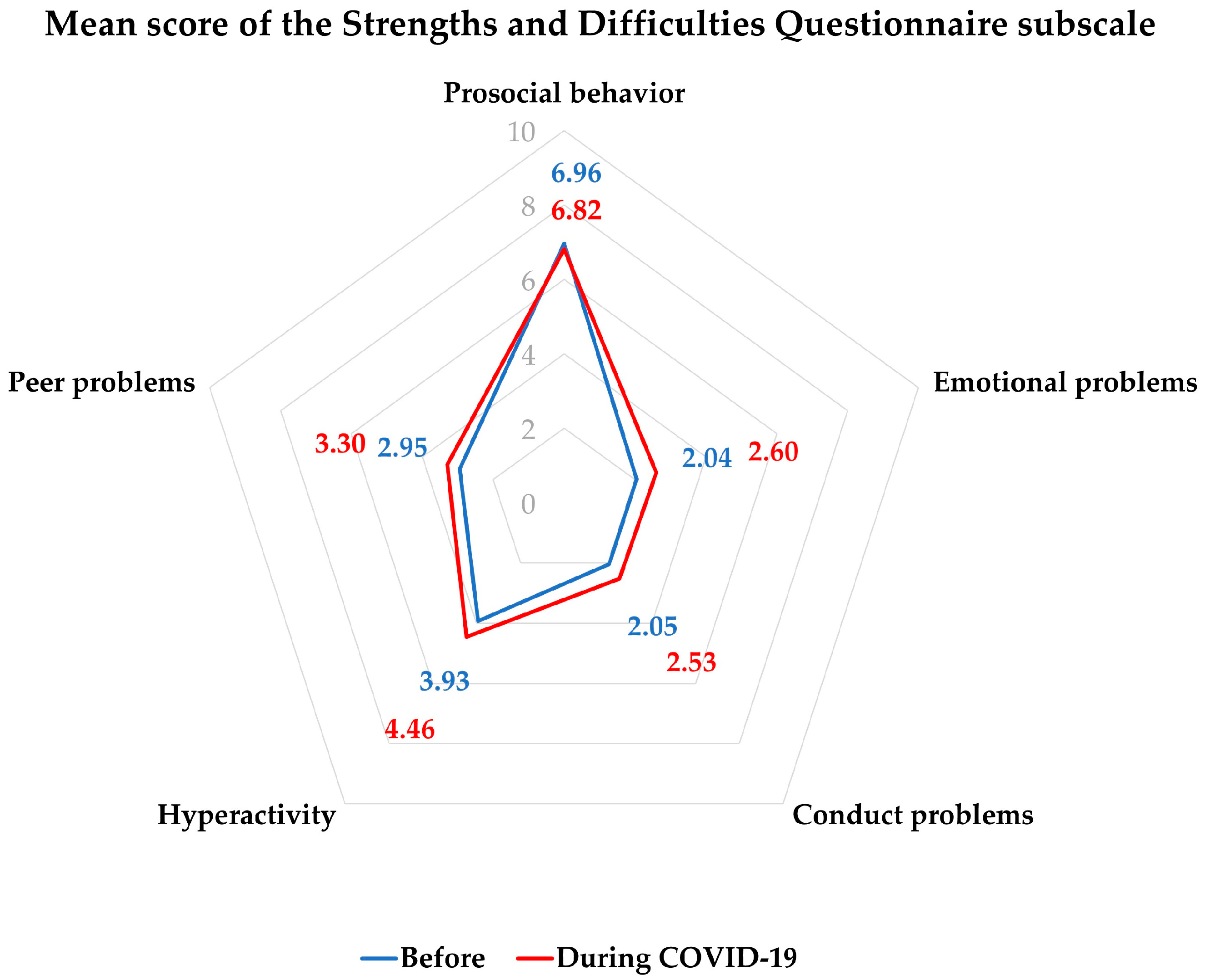
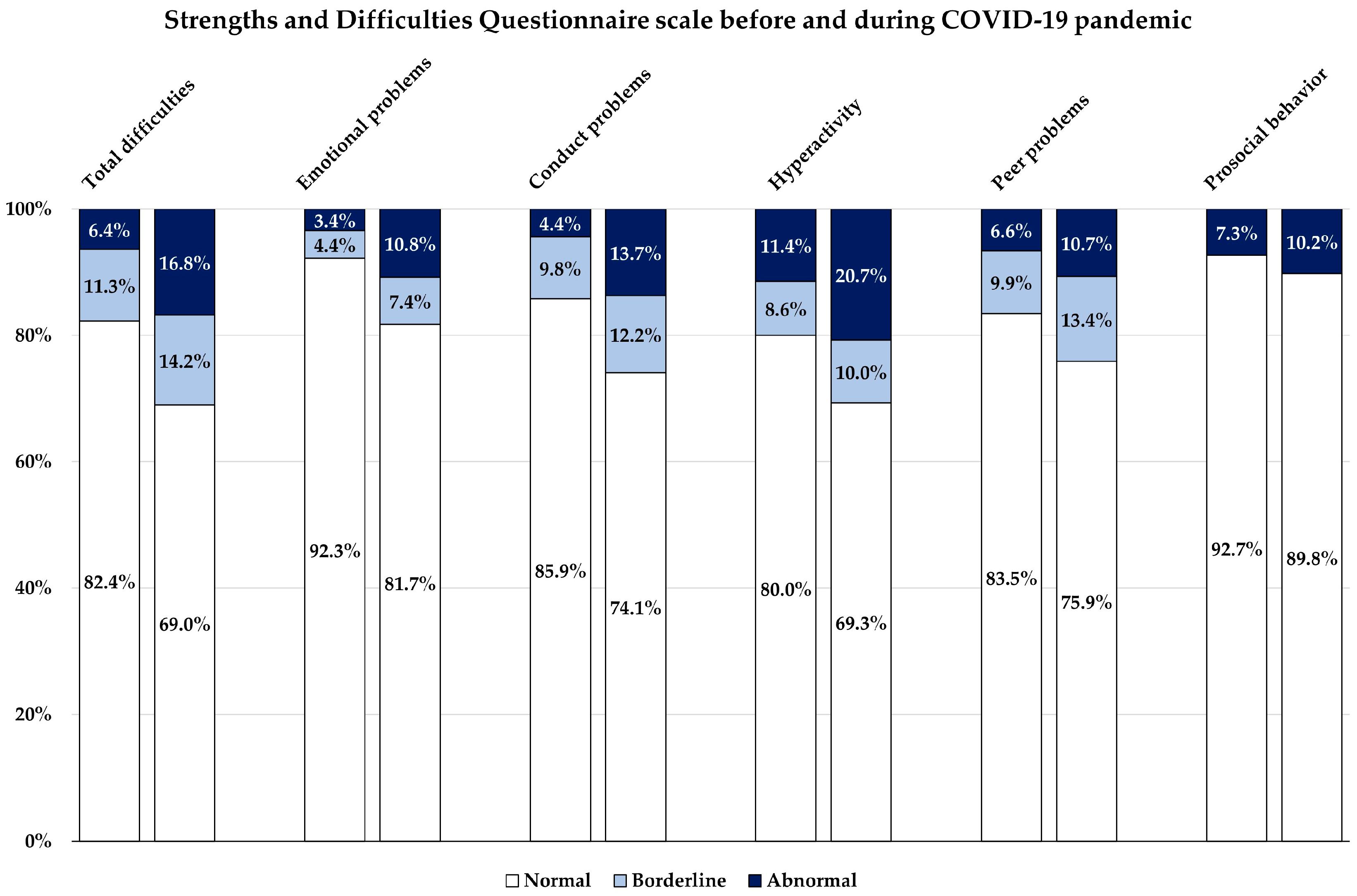
3.3. Emotional and Behavioral Problems Developed Due to the COVID-19 Pandemic
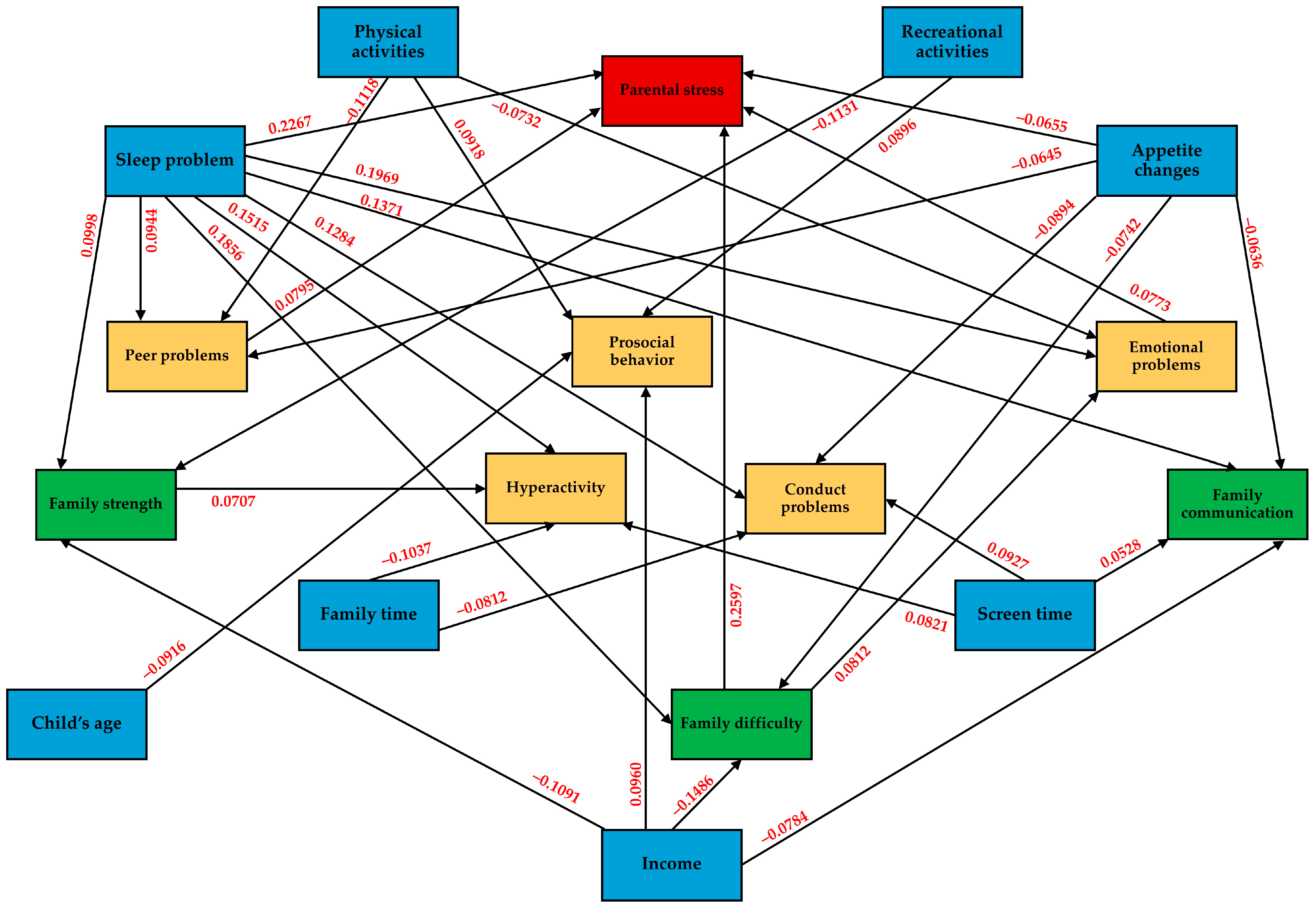
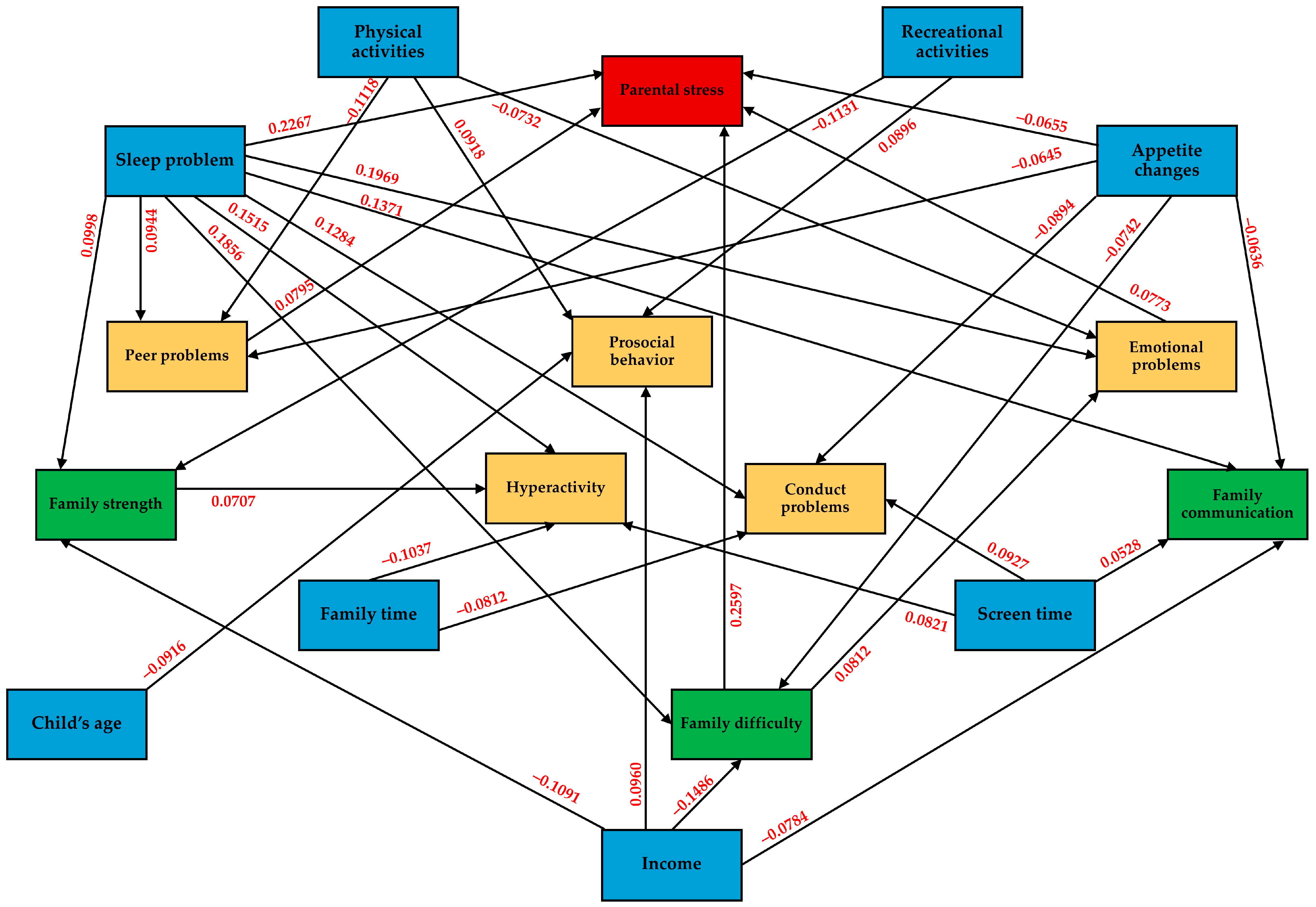
3.4. Association between Parental Stress, Family Functioning, and Children’s Strengths and Difficulties during the COVID-19 Pandemic
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 1 December 2020).
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 1 December 2021).
- Alfano, V.; Ercolano, S. The Efficacy of Lockdown Against COVID-19: A Cross-Country Panel Analysis. Appl. Health Econ. Health Policy 2020, 18, 509–517. [Google Scholar] [CrossRef]
- Trott, M.; Driscoll, R.; Irlado, E.; Pardhan, S. Changes and correlates of screen time in adults and children during the COVID-19 pandemic: A systematic review and meta-analysis. eClinicalMedicine 2022, 48, 101452. [Google Scholar] [CrossRef] [PubMed]
- Meherali, S.; Punjani, N.; Louie-Poon, S.; Abdul Rahim, K.; Das, J.K.; Salam, R.A.; Lassi, Z.S. Mental Health of Children and Adolescents Amidst COVID-19 and Past Pandemics: A Rapid Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 3432. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.; Huang, W.; Pan, H.; Huang, T.; Wang, X.; Ma, Y. Mental Health During the Covid-19 Outbreak in China: A Meta-Analysis. Psychiatr. Q. 2020, 91, 1033–1045. [Google Scholar] [CrossRef] [PubMed]
- Sameer, A.S.; Khan, M.A.; Nissar, S.; Banday, M.Z. Assessment of Mental Health and Various Coping Strategies among general population living Under Imposed COVID-Lockdown Across world: A Cross-Sectional Study. Ethics Med. Public Health 2020, 15, 100571. [Google Scholar] [CrossRef]
- Anand, P.; Patil, R.S.; Puri, P.; Patil, S. The Psychosocial Effects of Lockdown Due to the COVID-19 Pandemic on Children in 2021. Cureus 2024, 16, e53614. [Google Scholar] [CrossRef]
- Christner, N.; Essler, S.; Hazzam, A.; Paulus, M. Children’s psychological well-being and problem behavior during the COVID-19 pandemic: An online study during the lockdown period in Germany. PLoS ONE 2021, 16, e0253473. [Google Scholar] [CrossRef]
- Panda, P.K.; Gupta, J.; Chowdhury, S.R.; Kumar, R.; Meena, A.K.; Madaan, P.; Sharawat, I.K.; Gulati, S. Psychological and Behavioral Impact of Lockdown and Quarantine Measures for COVID-19 Pandemic on Children, Adolescents and Caregivers: A Systematic Review and Meta-Analysis. J. Trop. Pediatr. 2021, 67, fmaa122. [Google Scholar] [CrossRef]
- Marmor, A.; Cohen, N.; Katz, C. Child Maltreatment During COVID-19: Key Conclusions and Future Directions Based on a Systematic Literature Review. Trauma Violence Abus. 2023, 24, 760–775. [Google Scholar] [CrossRef]
- Viner, R.; Russell, S.; Saulle, R.; Croker, H.; Stansfield, C.; Packer, J.; Nicholls, D.; Goddings, A.L.; Bonell, C.; Hudson, L.; et al. School Closures During Social Lockdown and Mental Health, Health Behaviors, and Well-being Among Children and Adolescents During the First COVID-19 Wave: A Systematic Review. JAMA Pediatr. 2022, 176, 400–409. [Google Scholar] [CrossRef]
- Okuyama, J.; Seto, S.; Fukuda, Y.; Funakoshi, S.; Amae, S.; Onobe, J.; Izumi, S.; Ito, K.; Imamura, F. Mental Health and Physical Activity among Children and Adolescents during the COVID-19 Pandemic. Tohoku J. Exp. Med. 2021, 253, 203–215. [Google Scholar] [CrossRef]
- Chen, M.; Bai, Y.; Fu, M.; Huang, N.; Ahmed, F.; Shahid, M.; Wang, X.; Liu, C.; Feng, X.L.; Guo, J. The Associations Between Parental Burnout and Mental Health Symptoms Among Chinese Parents With Young Children During the COVID-19 Pandemic. Front. Psychiatry 2022, 13, 819199. [Google Scholar] [CrossRef] [PubMed]
- von Suchodoletz, A.; Bélanger, J.; Bryan, C.; Ali, R.; Al Nuaimi, S.R. COVID-19’s shadow on families: A structural equation model of parental stress, family relationships, and child wellbeing. PLoS ONE 2023, 18, e0292292. [Google Scholar] [CrossRef] [PubMed]
- Dayton, L.; Kong, X.; Powell, T.W.; Bowie, J.; Rebok, G.; Strickland, J.C.; Latkin, C. Child Mental Health and Sleep Disturbances During the Early Months of the COVID-19 Pandemic in the United States. Fam. Community Health 2022, 45, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Pudpong, N.; Julchoo, S.; Sinam, P.; Uansri, S.; Kunpeuk, W.; Suphanchaimat, R. Family Health among Families with Primary School Children during the COVID Pandemic in Thailand, 2022. Int. J. Environ. Res. Public Health 2022, 19, 15001. [Google Scholar] [CrossRef] [PubMed]
- Limsuwan, N.; Prachason, T.; Wisajun, P. The changes in family functioning and family happiness during the COVID-19 pandemic: The situation in Thailand. Front. Public Health 2022, 10, 1055819. [Google Scholar] [CrossRef] [PubMed]
- Wongpiromsarn, Y.; Wipulakorn, P.; Nuanmanee, S.; Wolfgang, W.; Mongkol, A. Strengths and Difficulties Questionnaire (SDQ) Thai improved version: Change and administration. J. Ment. Health Thai. 2011, 19, 128–134. [Google Scholar]
- Woerner, W.; Nuanmanee, S.; Becker, A.; Wongpiromsarn, Y.; Mongkol, A. Normative data and psychometric properties of the Thai version of the Strengths and Difficulties Questionnaire (SDQ). J. Ment. Health Thai. 2011, 19, 42–57. [Google Scholar]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Carr, A.; Stratton, P. The Score Family Assessment Questionnaire: A Decade of Progress. Fam. Process 2017, 56, 285–301. [Google Scholar] [CrossRef]
- Limsuwan, N.; Prachason, T. Psychometric properties of the SCORE-15 Thai version and its relationship with mental health index. J. Fam. Ther. 2022, 44, 299–312. [Google Scholar] [CrossRef]
- Silpakit, O. Srithanya stress scale. J. Ment. Health Thai. 2012, 16, 177–185. [Google Scholar]
- Schumacker, R.E.; Lomax, R.G. A Beginner’s Guide to Structural Equation Modeling; Psychology Press: London, UK, 2004. [Google Scholar]
- Barrett, P. Structural equation modelling: Adjudging model fit. Personal. Individ. Differ. 2007, 42, 815–824. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Dunton, G.F.; Do, B.; Wang, S.D. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the U.S. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.A.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the COVID-19 virus outbreak on movement and play behaviours of Canadian children and youth: A national survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 85. [Google Scholar] [CrossRef]
- Carroll, N.; Sadowski, A.; Laila, A.; Hruska, V.; Nixon, M.; Ma, D.W.L.; Haines, J.; On Behalf Of The Guelph Family Health Study. The Impact of COVID-19 on Health Behavior, Stress, Financial and Food Security among Middle to High Income Canadian Families with Young Children. Nutrients 2020, 12, 2352. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; Van Horn, R.L. Physical Activity and Sedentary Behavior in Children During the COVID-19 Pandemic: Implications for Mental Health. Curr. Psychiatry Rep. 2022, 24, 493–501. [Google Scholar] [CrossRef]
- Widyastari, D.A.; Saonuam, P.; Pongpradit, K.; Wongsingha, N.; Choolers, P.; Kesaro, S.; Thangchan, W.; Pongpaopattanakul, P.; Phankasem, K.; Musor, M.E.; et al. Results from the Thailand 2022 report card on physical activity for children and youth. J. Exerc. Sci. Fit. 2022, 20, 276–282. [Google Scholar] [CrossRef]
- Hossain, M.M.; Nesa, F.; Das, J.; Aggad, R.; Tasnim, S.; Bairwa, M.; Ma, P.; Ramirez, G. Global burden of mental health problems among children and adolescents during COVID-19 pandemic: An umbrella review. Psychiatry Res. 2022, 317, 114814. [Google Scholar] [CrossRef] [PubMed]
- Rajatanavin, N.; Tuangratananon, T.; Suphanchaimat, R.; Tangcharoensathien, V. Responding to the COVID-19 second wave in Thailand by diversifying and adapting lessons from the first wave. BMJ Glob. Health 2021, 6, e006178. [Google Scholar] [CrossRef] [PubMed]
- Stiglic, N.; Viner, R.M. Effects of screentime on the health and well-being of children and adolescents: A systematic review of reviews. BMJ Open 2019, 9, e023191. [Google Scholar] [CrossRef]
- Lund, L.; Sølvhøj, I.N.; Danielsen, D.; Andersen, S. Electronic media use and sleep in children and adolescents in western countries: A systematic review. BMC Public Health 2021, 21, 1598. [Google Scholar] [CrossRef]
- Muppalla, S.K.; Vuppalapati, S.; Reddy Pulliahgaru, A.; Sreenivasulu, H. Effects of Excessive Screen Time on Child Development: An Updated Review and Strategies for Management. Cureus 2023, 15, e40608. [Google Scholar] [CrossRef] [PubMed]
- Hosokawa, R.; Katsura, T. Association between mobile technology use and child adjustment in early elementary school age. PLoS ONE 2018, 13, e0199959. [Google Scholar] [CrossRef]
- Vandekerckhove, M.; Wang, Y.L. Emotion, emotion regulation and sleep: An intimate relationship. AIMS Neurosci. 2018, 5, 1–17. [Google Scholar] [CrossRef]
- Werling, A.M.; Walitza, S.; Grünblatt, E.; Drechsler, R. Media use before, during and after COVID-19 lockdown according to parents in a clinically referred sample in child and adolescent psychiatry: Results of an online survey in Switzerland. Compr. Psychiatry 2021, 109, 152260. [Google Scholar] [CrossRef]
- Li, B.; Ng, K.; Tong, X.; Zhou, X.; Ye, J.; Yu, J.J. Physical activity and mental health in children and youth during COVID-19: A systematic review and meta-analysis. Child Adolesc. Psychiatry Ment. Health 2023, 17, 92. [Google Scholar] [CrossRef]
- Wan, Y.; Zhao, Y.; Song, H. Effects of Physical Exercise on Prosocial Behavior of Junior High School Students. Children 2021, 8, 1199. [Google Scholar] [CrossRef]
- Li, J.; Shao, W. Influence of Sports Activities on Prosocial Behavior of Children and Adolescents: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 6484. [Google Scholar] [CrossRef]
- Moulin, F.; Bailhache, M.; Monnier, M.; Thierry, X.; Vandentorren, S.; Côté, S.M.; Falissard, B.; Simeon, T.; Geay, B.; Marchand, L.; et al. Longitudinal impact of psychosocial status on children’s mental health in the context of COVID-19 pandemic restrictions. Eur. Child Adolesc. Psychiatry 2022, 32, 1073–1082. [Google Scholar] [CrossRef]
- Kerr, M.L.; Rasmussen, H.F.; Fanning, K.A.; Braaten, S.M. Parenting During COVID-19: A Study of Parents’ Experiences Across Gender and Income Levels. Fam. Relat. 2021, 70, 1327–1342. [Google Scholar] [CrossRef]
- Riany, Y.E.; Morawska, A. Financial and Work Burden, Psychosocial Functioning, and Family Interactions During the COVID-19 Pandemic in Indonesia: Effects on Child Outcomes. Child. Psychiatry Hum. Dev. 2021, 54, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Adegboye, D.; Williams, F.; Collishaw, S.; Shelton, K.; Langley, K.; Hobson, C.; Burley, D.; van Goozen, S. Understanding why the COVID-19 pandemic-related lockdown increases mental health difficulties in vulnerable young children. JCPP Adv. 2021, 1, e12005. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.T.; Henry, D.A.; Del Toro, J.; Scanlon, C.L.; Schall, J.D. COVID-19 Employment Status, Dyadic Family Relationships, and Child Psychological Well-Being. J. Adolesc. Health 2021, 69, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Sum, K.K.; Cai, S.; Law, E.; Cheon, B.; Tan, G.; Loo, E.; Lee, Y.S.; Yap, F.; Chan, J.K.Y.; Daniel, M.; et al. COVID-19-Related Life Experiences, Outdoor Play, and Long-term Adiposity Changes Among Preschool- and School-Aged Children in Singapore 1 Year After Lockdown. JAMA Pediatr. 2022, 176, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Khanijahani, A.; Iezadi, S.; Gholipour, K.; Azami-Aghdash, S.; Naghibi, D. A systematic review of racial/ethnic and socioeconomic disparities in COVID-19. Int. J. Equity Health 2021, 20, 248. [Google Scholar] [CrossRef] [PubMed]
- Zahry, N.R.; Ling, J.; Robbins, L.B. Mental health and lifestyle behavior changes during COVID-19 among families living in poverty: A descriptive phenomenological study. J. Child Adolesc. Psychiatr. Nurs. 2024, 37, e12447. [Google Scholar] [CrossRef] [PubMed]
- Marcus, S.M.; Marcus, T.S. Infrastructural Inequality and Household COVID-19 Vulnerability in a South African Urban Settlement. J. Urban Health 2022, 99, 571–581. [Google Scholar] [CrossRef]
- Li, W.; Wang, Z.; Wang, G.; Ip, P.; Sun, X.; Jiang, Y.; Jiang, F. Socioeconomic inequality in child mental health during the COVID-19 pandemic: First evidence from China. J. Affect. Disord. 2021, 287, 8–14. [Google Scholar] [CrossRef]
- MacKenzie, N.E.; Keys, E.; Hall, W.A.; Gruber, R.; Smith, I.M.; Constantin, E.; Godbout, R.; Stremler, R.; Reid, G.J.; Hanlon-Dearman, A.; et al. Children’s Sleep During COVID-19: How Sleep Influences Surviving and Thriving in Families. J. Pediatr. Psychol. 2021, 46, 1051–1062. [Google Scholar] [CrossRef]
- Wang, P.; Sun, X.; Li, W.; Wang, Z.; He, S.; Zhai, F.; Xin, Y.; Pan, L.; Wang, G.; Jiang, F.; et al. Mental Health of Parents and Preschool-Aged Children During the COVID-19 Pandemic: The Mediating Role of Harsh Parenting and Child Sleep Disturbances. Front. Psychiatry 2021, 12, 746330. [Google Scholar] [CrossRef]
- Zhao, J.; Xu, J.; He, Y.; Xiang, M. Children and adolescents’ sleep patterns and their associations with mental health during the COVID-19 pandemic in Shanghai, China. J. Affect. Disord. 2022, 301, 337–344. [Google Scholar] [CrossRef]
- Philippe, K.; Chabanet, C.; Issanchou, S.; Monnery-Patris, S. Child eating behaviors, parental feeding practices and food shopping motivations during the COVID-19 lockdown in France: (How) did they change? Appetite 2021, 161, 105132. [Google Scholar] [CrossRef]
- Kamaleddine, A.N.; Antar, H.A.; Ali, B.T.A.; Hammoudi, S.F.; Lee, J.; Lee, T.; Bhang, S.Y.; Chung, S.; Salameh, P. Effect of Screen Time on Physical and Mental Health and Eating Habits During COVID-19 Lockdown in Lebanon. Psychiatry Investig. 2022, 19, 220–228. [Google Scholar] [CrossRef]
- Radwan, A.; Radwan, E.; Radwan, W. Eating habits among primary and secondary school students in the Gaza Strip, Palestine: A cross-sectional study during the COVID-19 pandemic. Appetite 2021, 163, 105222. [Google Scholar] [CrossRef] [PubMed]
- Brakspear, L.; Boules, D.; Nicholls, D.; Burmester, V. The Impact of COVID-19-Related Living Restrictions on Eating Behaviours in Children and Adolescents: A Systematic Review. Nutrients 2022, 14, 3657. [Google Scholar] [CrossRef] [PubMed]
- Juli, M.R.; Juli, R.; Juli, G.; Juli, L. Eating Disorders: The Role of the Family in Development and Maintenance of Children’s Problems in the Pandemic Period. Psychiatr. Danub. 2022, 34, 122–128. [Google Scholar] [PubMed]
- Krom, H.; van Mameren, J.; Remijn, L.; de Nennie, K.; Dumont, E.; van der Gaag, E.; van Leeuwen, M.C.C.; Mulkens, S.; Schakelaar, C.; Kindermann, A. Impact of COVID-19 Pandemic on Young Children With Feeding and Eating Problems and Disorders and Their Families. J. Pediatr. Gastroenterol. Nutr. 2022, 75, 529–534. [Google Scholar] [CrossRef] [PubMed]
- González, L.M.; Lammert, A.; Phelan, S.; Ventura, A.K. Associations between parenting stress, parent feeding practices, and perceptions of child eating behaviors during the COVID-19 pandemic. Appetite 2022, 177, 106148. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Tee, M.; Roy, A.E.; Fardin, M.A.; Srichokchatchawan, W.; Habib, H.A.; Tran, B.X.; Hussain, S.; Hoang, M.T.; Le, X.T.; et al. The impact of COVID-19 pandemic on physical and mental health of Asians: A study of seven middle-income countries in Asia. PLoS ONE 2021, 16, e0246824. [Google Scholar] [CrossRef] [PubMed]
- Bureau of Information and Communication Technology, Ministry of Education. Educational Statistics 2020; Bureau of Information and Communication Technology, Ministry of Education: Bangkok, Thailand, 2021; pp. 38–39.

{kind=link}
{kind=link}
{kind=link}
| Demographic | n (%) or Mean [SD] |
|---|---|
| Caregiver characteristics | |
| Father | 46 (4.9) |
| Mother | 837 (88.9) |
| Others | 59 (6.2) |
| Region (missing = 1) | |
| Central | 687 (73.0) |
| North | 118 (12.5) |
| Northeast | 55 (5.8) |
| South | 81 (8.6) |
| Education level | |
| Undergraduate | 111 (11.8) |
| Bachelor’s degree | 540 (57.3) |
| Higher degree | 291 (30.9) |
| Household income (USD/month) a | |
| <300 | 31 (3.3) |
| 300–900 | 236 (25.1) |
| 901–1500 | 233 (24.7) |
| 1501–3000 | 221 (23.5) |
| >3000 | 221 (23.5) |
| Sex of child | |
| Male | 491 (52.1) |
| Female | 451 (47.9) |
| Type of schools | |
| Private | 567 (60.2) |
| Government | 263 (27.9) |
| Demonstrate | 57 (6.1) |
| International | 50 (5.3) |
| Psychiatric diagnosis of child | |
| Yes | 151 (16.0) |
| No | 791 (84) |
| Age of children (years) [Min = 5, Max = 15] | 8.54 [1.87] |
| Effects | n (%) or Mean [SD] |
|---|---|
| COVID-19 infection | |
| Child infected | 1 (0.1) |
| Parent infected | 1 (0.1) |
| Child quarantined due to being in a high-risk group | 13 (1.4) |
| Parent quarantined due to being in high-risk group | 21 (2.2) |
| Sleep problems | |
| The problem has just presented or with more severity | 243 (25.8) |
| The problem presented before and with equal severity | 113 (12.0) |
| Problem presented before but with less severity | 9 (1.0) |
| Appetite | |
| Decrease | 475 (50.4) |
| Increase | 365 (38.7) |
| Same | 102 (10.8) |
| Physical activities | |
| <1 h/day | 548 (58.2) |
| 1–2 h/day | 303 (32.2) |
| >2 h/day | 91 (9.7) |
| Recreational activities | |
| <1 h/day | 292 (31.0) |
| 1–2 h/day | 351 (37.3) |
| >2 h/day | 299 (31.7) |
| Family time | |
| <1 h/day | 340 (36.1) |
| 1–2 h/day | 337 (35.8) |
| >2 h/day | 265 (28.1) |
| Screen time during COVID-19 pandemic | |
| Increased from before pandemic | 811 (86.1) |
| Decreased from before pandemic | 101 (10.7) |
| Same as before pandemic | 30 (3.2) |
| Duration of screen time | |
| <3 h/day | 291 (30.9) |
| 3–5 h/day | 297 (31.5) |
| >5 h/day | 213 (22.6) |
| >7 h/day | 141 (15.0) |
| Online classes | |
| No | 149 (15.8) |
| 1–3 h/day | 480 (50.9) |
| 3–5 h/day | 238 (25.3) |
| 5–7 h/day | 75 (8) |
| Parental supervision during screen time | |
| No | 48 (5.1) |
| Sometimes | 278 (29.5) |
| Often | 356 (37.8) |
| Always | 260 (27.6) |
| SDQ Scale (Range) | n (%) or Mean [SD] | p-Value a | |
|---|---|---|---|
| Before | After | ||
| Total difficulties (0–40) | 10.98 [4.81] | 12.90 [5.88] | <0.001 * |
| Normal (0–15) | 776 (82.4%) | 650 (69.0%) | <0.001 * |
| Borderline (16–18) | 106 (11.3%) | 134 (14.2%) | |
| Abnormal (19–40) | 60 (6.4%) | 158 (16.8%) | |
| Emotional problems (0–10) | 2.04 [1.69] | 2.60 [2.13] | <0.001 * |
| Normal (0–4) | 869 (92.3%) | 770 (81.7%) | <0.001 * |
| Borderline (5) | 41 (4.4%) | 70 (7.4%) | |
| Abnormal (6–10) | 32 (3.4%) | 102 (10.8%) | |
| Conduct problems (0–10) | 2.05 [1.41] | 2.53 [1.75] | <0.001 * |
| Normal (0–3) | 809 (85.9%) | 698 (74.1%) | <0.001 * |
| Borderline (4) | 92 (9.8%) | 115 (12.2%) | |
| Abnormal (5–10) | 41 (4.4%) | 129 (13.7%) | |
| Hyperactivity (0–10) | 3.93 [2.12] | 4.46 [2.42] | <0.001 * |
| Normal (0–5) | 754 (80.0%) | 653 (69.3%) | <0.001 * |
| Borderline (6) | 81 (8.6%) | 94 (10.0%) | |
| Abnormal (7–10) | 107 (11.4%) | 195 (20.7%) | |
| Peer problems (0–10) | 2.95 [1.61] | 3.30 [1.72] | <0.001 * |
| Normal (0–4) | 787 (83.5%) | 715 (75.9%) | <0.001 * |
| Borderline (5) | 93 (9.9%) | 126 (13.4%) | |
| Abnormal (6–10) | 62 (6.6%) | 101 (10.7%) | |
| Prosocial behavior (0–10) | 6.96 [1.89] | 6.82 [1.98] | <0.001 * |
| Normal (5–10) | 873 (92.7%) | 846 (89.8%) | <0.001 * |
| Abnormal (0–4) | 69 (7.3%) | 97 (10.2%) | |
| Variables | β | (95% CI) | p-Value |
|---|---|---|---|
| Parental stress | |||
| Emotional problems change | 0.0773 | (0.0099, 0.1446) | 0.025 * |
| Conduct problems change | 0.0208 | (−0.0521, 0.0936) | 0.576 |
| Hyperactivity change | 0.0633 | (−0.0059, 0.1326) | 0.073 |
| Peer problems change | 0.0795 | (0.0183, 0.1408) | 0.011 * |
| Family strength | 0.0491 | (−0.0114, 0.1095) | 0.111 |
| Family difficulty | 0.2597 | (0.1867, 0.3327) | <0.001 * |
| Family communication | −0.0364 | (−0.1117, 0.0389) | 0.343 |
| Child’s age | −0.0522 | (−0.1108, 0.0063) | 0.080 |
| Psychiatric diagnosis | 0.0489 | (−0.0077, 0.1054) | 0.090 |
| Sleep problems | 0.2267 | (0.1692, 0.2842) | <0.001 * |
| Appetite changes | −0.0655 | (−0.1224, −0.0086) | 0.024 * |
| Physical activities ≥ 1 h/day | −0.0317 | (−0.0894, 0.0260) | 0.282 |
| Screen time ≥ 3 h/day | 0.0472 | (−0.0118, 0.1061) | 0.117 |
| Emotional problems change | |||
| Family difficulty | 0.0812 | (0.0064, 0.1560) | 0.033 * |
| Family communication | 0.0077 | (−0.0647, 0.0801) | 0.834 |
| Psychiatric diagnosis | 0.0210 | (−0.0324, 0.0743) | 0.441 |
| Sleep problems | 0.1969 | (0.1351, 0.2587) | <0.001 * |
| Appetite changes | −0.0478 | (−0.1102, 0.0145) | 0.133 |
| Physical activities ≥ 1 h/day | −0.0732 | (−0.1355, −0.0109) | 0.021* |
| Recreational activities ≥ 1 h/day | −0.0241 | (−0.0851, 0.0370) | 0.439 |
| Screen time ≥ 3 h/day | 0.0467 | (−0.0146, 0.1081) | 0.136 |
| Conduct problems change | |||
| Family strength | 0.0417 | (−0.0147, 0.0981) | 0.147 |
| Family difficulty | 0.0413 | (−0.0303, 0.1129) | 0.259 |
| Family communication | 0.0070 | (−0.0610, 0.0749) | 0.841 |
| Sleep problems | 0.1284 | (0.0659, 0.1909) | <0.001 * |
| Appetite changes | −0.0894 | (−0.1516, −0.0272) | 0.005 * |
| Physical activities ≥ 1 h/day | −0.0096 | (−0.0735, 0.0543) | 0.769 |
| Recreational activities ≥ 1 h/day | −0.0497 | (−0.1159, 0.0165) | 0.141 |
| Family time ≥ 1 h/day | −0.0812 | (−0.1424, −0.0199) | 0.009 * |
| Screen time ≥ 3 h/day | 0.0927 | (0.0311, 0.1543) | 0.003 * |
| Hyperactivity change | |||
| Family strength | 0.0707 | (0.0134, 0.1280) | 0.016 * |
| Family difficulty | 0.0054 | (−0.0544, 0.0652) | 0.860 |
| Sleep problems | 0.1515 | (0.0893, 0.2138) | <0.001 * |
| Appetite changes | −0.0408 | (−0.1033, 0.0217) | 0.201 |
| Physical activities ≥ 1 h/day | −0.0505 | (−0.1144, 0.0134) | 0.121 |
| Recreational activities ≥ 1 h/day | −0.0186 | (−0.0859, 0.0487) | 0.587 |
| Family time ≥ 1 h/day | −0.1037 | (−0.1678, −0.0396) | 0.002 * |
| Screen time ≥ 3 h/day | 0.0821 | (0.0199, 0.1443) | 0.010 * |
| Peer problems change | |||
| Sleep problems | 0.0944 | (0.0312, 0.1577) | 0.003 * |
| Appetite changes | −0.0645 | (−0.1280, −0.0011) | 0.046 * |
| Physical activities ≥ 1 h/day | −0.1118 | (−0.1743, −0.0493) | <0.001 * |
| Prosocial behavior change | |||
| Income > 900 USD | 0.0960 | (0.0404, 0.1516) | 0.001 * |
| Child’s age | −0.0916 | (−0.1502, −0.0331) | 0.002 * |
| Sleep problems | −0.0566 | (−0.1195, 0.0062) | 0.077 |
| Appetite changes | 0.0610 | (−0.0018, 0.1239) | 0.057 |
| Physical activities ≥ 1 h/day | 0.0918 | (0.0273, 0.1563) | 0.005 * |
| Recreational activities ≥ 1 h/day | 0.0896 | (0.0221, 0.1572) | 0.009 * |
| Family time ≥ 1 h/day | 0.0232 | (−0.0443, 0.0906) | 0.500 |
| Screen time ≥ 3 h/day | −0.0048 | (−0.0682, 0.0586) | 0.882 |
| Family strength | |||
| Income > 900 USD | −0.1091 | (−0.1710, −0.0473) | 0.001 * |
| Sleep problems | 0.0998 | (0.0372, 0.1624) | 0.002 * |
| Appetite changes | −0.0362 | (−0.0995, 0.0270) | 0.261 |
| Physical activities ≥ 1 h/day | −0.0476 | (−0.1087, 0.0134) | 0.126 |
| Recreational activities ≥ 1 h/day | −0.1131 | (−0.1794, −0.0468) | 0.001 * |
| Family time ≥ 1 h/day | −0.0220 | (−0.0890, 0.0450) | 0.521 |
| Screen time ≥ 3 h/day | 0.0234 | (−0.0402, 0.0869) | 0.471 |
| Family difficulty | |||
| Income > 900 USD | −0.1486 | (−0.2092, −0.0880) | <0.001 * |
| Child’s age | −0.0297 | (−0.0792, 0.0199) | 0.241 |
| Psychiatric diagnosis | 0.0423 | (−0.0061, 0.0907) | 0.087 |
| Sleep problems | 0.1856 | (0.1247, 0.2465) | <0.001 * |
| Appetite changes | −0.0742 | (−0.1363, −0.0121) | 0.019 * |
| Recreational activities ≥ 1 h/day | −0.0346 | (−0.0843, 0.0151) | 0.173 |
| Family communication | |||
| Income > 900 USD | −0.0784 | (−0.1409, −0.0159) | 0.014 * |
| Sleep problems | 0.1371 | (0.0745, 0.1996) | <0.001 * |
| Appetite changes | −0.0636 | (−0.1270, −0.0003) | 0.049 * |
| Screen time ≥ 3 h/day | 0.0528 | (0.0027, 0.1028) | 0.039 * |
| RMSEA | 0.017 | ||
| SRMR | 0.019 | ||
| CFI | 0.995 | ||
| TLI | 0.985 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jetiyanuwat, S.; Kawilapat, S.; Narkpongphun, A.; Pojanapotha, P. Association between Family Functioning, Child Emotional and Behavioral Problems, and Parental Stress during the COVID-19 Pandemic in Thailand. Behav. Sci. 2024, 14, 270. https://doi.org/10.3390/bs14040270
Jetiyanuwat S, Kawilapat S, Narkpongphun A, Pojanapotha P. Association between Family Functioning, Child Emotional and Behavioral Problems, and Parental Stress during the COVID-19 Pandemic in Thailand. Behavioral Sciences. 2024; 14(4):270. https://doi.org/10.3390/bs14040270
Chicago/Turabian StyleJetiyanuwat, Sawitree, Suttipong Kawilapat, Assawin Narkpongphun, and Pichaya Pojanapotha. 2024. "Association between Family Functioning, Child Emotional and Behavioral Problems, and Parental Stress during the COVID-19 Pandemic in Thailand" Behavioral Sciences 14, no. 4: 270. https://doi.org/10.3390/bs14040270
APA StyleJetiyanuwat, S., Kawilapat, S., Narkpongphun, A., & Pojanapotha, P. (2024). Association between Family Functioning, Child Emotional and Behavioral Problems, and Parental Stress during the COVID-19 Pandemic in Thailand. Behavioral Sciences, 14(4), 270. https://doi.org/10.3390/bs14040270