The Mediating Effect of Depression on the Relationship between Loneliness and Substance Use in Korean Adolescents


Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Study Population
2.2. Measurements
2.2.1. Loneliness
2.2.2. Substance Use
2.2.3. Depression
2.2.4. Participants’ General Characteristics and Smoking- and Drinking-Related Variables
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
3.1. General Characteristics, Loneliness, Depression, and Substance Use
3.2. Differences in Substance Use according to General Characteristics, Loneliness, and Depression
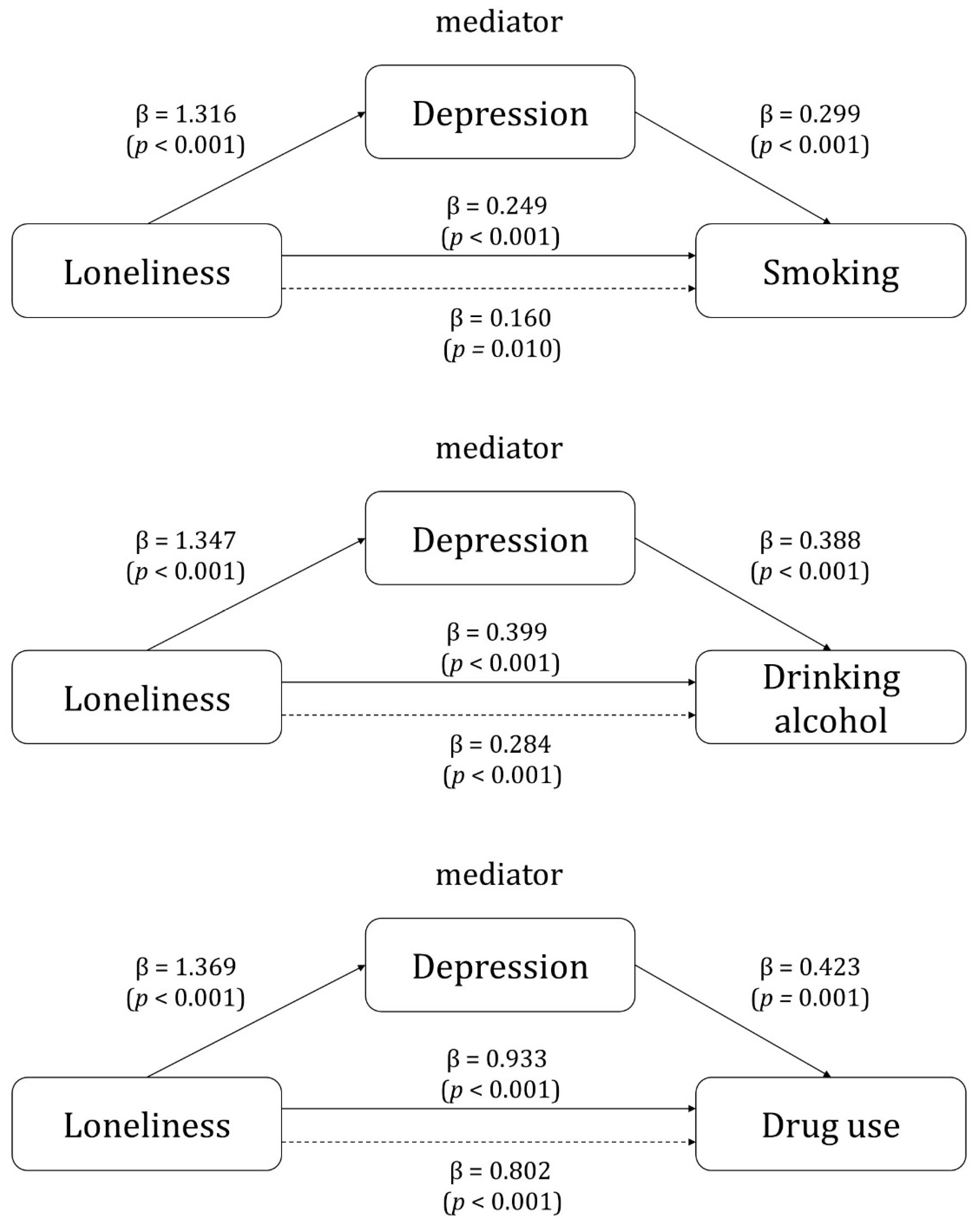
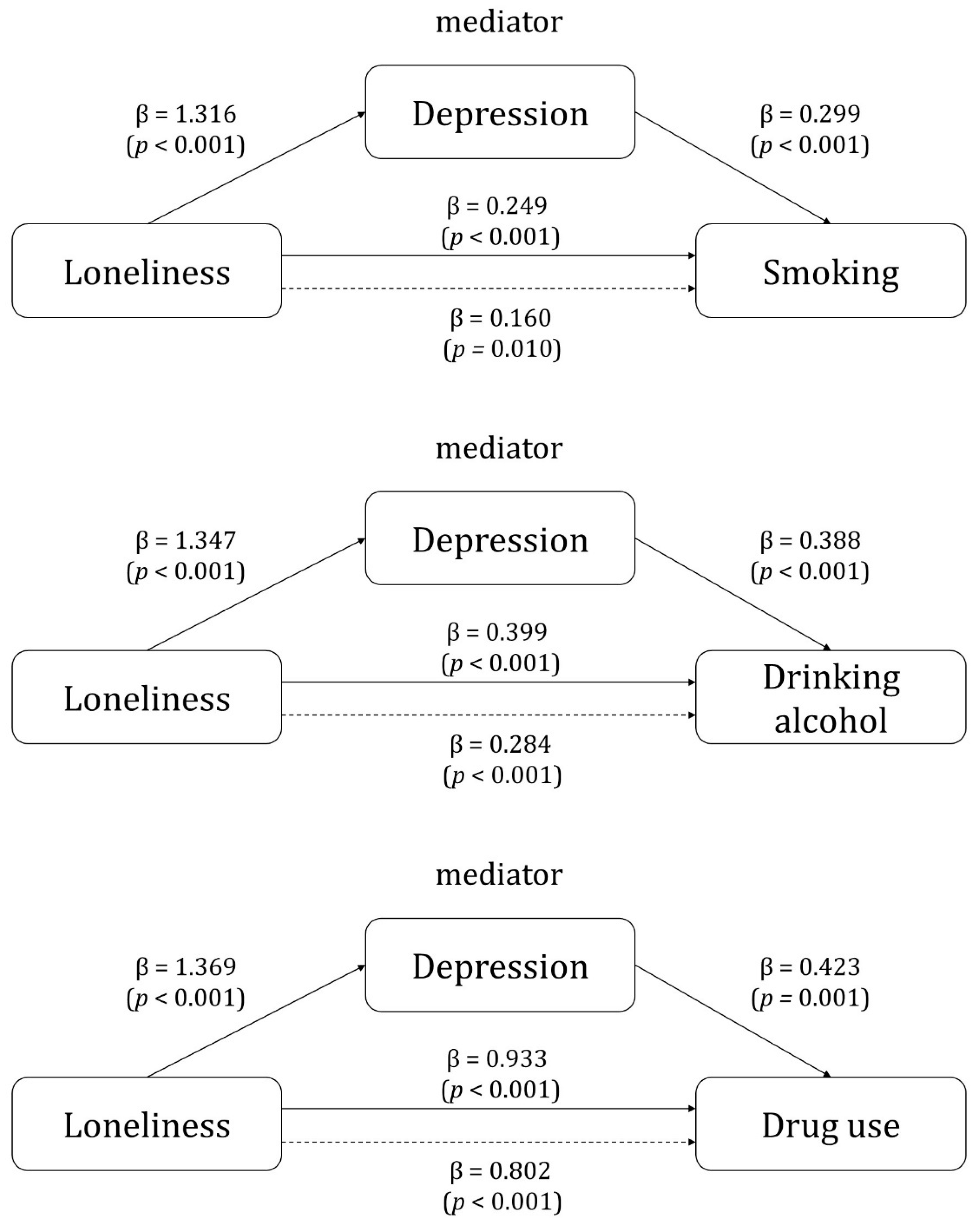
3.3. Mediating Effect of Depression on the Relationship between Loneliness and Substance Use
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chaiton, M.O.; Cohen, J.E.; O’Loughlin, J.; Rehm, J. A systematic review of longitudinal studies on the association between depression and smoking in adolescents. BMC Public Health 2009, 9, 356. [Google Scholar] [CrossRef] [PubMed]
- Griffin, K.W.; Botvin, G.J. Evidence-based interventions for preventing substance use disorders in adolescents. Child Adolesc. Psychiatr. Clin. N. Am. 2010, 19, 505–526. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Kumar, P.; Rashmi; Paul, R.; Dhillon, P. Does substance use by family members and community affect the substance use among adolescent boys? Evidence from UDAYA study, India. BMC Public Health 2021, 21, 1896. [Google Scholar] [CrossRef] [PubMed]
- Ingram, I.; Kelly, P.J.; Deane, F.P.; Baker, A.L.; Dingle, G.A. Perceptions of loneliness among people accessing treatment for substance use disorders. Drug Alcohol. Rev. 2020, 39, 484–494. [Google Scholar] [CrossRef] [PubMed]
- Jaworska, N.; McIntosh, J.; Villeneuve, C.; Thompson, A.; Fisher, D.; Milin, R.; Knott, V. Effects of nicotine on electroencephalography and affect in adolescent females with major depressive disorder: A pilot study. J. Addict. Med. 2011, 5, 123–133. [Google Scholar] [CrossRef]
- Wasil, A.R.; Venturo-Conerly, K.E.; Shinde, S.; Patel, V.; Jones, P.J. Applying network analysis to understand depression and substance use in Indian adolescents. J. Affect. Disord. 2020, 265, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Dewall, C.N.; Pond, R.S., Jr. Loneliness and smoking: The costs of the desire to reconnect. Self Identity 2011, 10, 375–385. [Google Scholar] [CrossRef]
- Nam, E.; Lee, J.; Kwon, M. Associations between habitual drug use and loneliness in Korean adolescents: Secondary data analysis of the 2020 youth health risk behavior web-based survey. J. Korean Soc. Sch. Health 2021, 34, 161–169. [Google Scholar]
- Stickley, A.; Koyanagi, A.; Koposov, R.; Schwab-Stone, M.; Ruchkin, V. Loneliness and health risk behaviours among Russian and U.S. adolescents: A cross-sectional study. BMC Public Health 2014, 14, 366. [Google Scholar] [CrossRef]
- Cena, L.; Trainini, A.; Zecca, S.; Bonetti Zappa, S.; Cunegatti, F.; Buizza, C. Loneliness, affective disorders, suicidal ideation, and the use of psychoactive substances in a sample of adolescents during the COVID-19 pandemic: A cross-sectional study. J. Child Adolesc. Psychiatr. Nurs. 2023, 36, 188–198. [Google Scholar] [CrossRef]
- Lyyra, N.; Junttila, N.; Tynjälä, J.; Villberg, J.; Välimaa, R. Loneliness, subjective health complaints, and medicine use among Finnish adolescents 2006–2018. Scand. J. Public Health 2022, 50, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- Park, H.G.; Jeong, S.; Kwon, M. Factors related to depression according to the degree of loneliness in adolescents with severe friend-relationship stress. Healthcare 2023, 11, 1354. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, M.; Olsson, C.A.; Jorm, A.F.; Romaniuk, H.; Patton, G.C. Association of adolescent symptoms of depression and anxiety with daily smoking and nicotine dependence in young adulthood: Findings from a 10-year longitudinal study. Addiction 2010, 105, 1652–1659. [Google Scholar] [CrossRef]
- Korea Disease Control and Prevention Agency. The 17th Korea Youth Risk Behavior Web-Based Survey 2021. Available online: https://www.kdca.go.kr/yhs/ (accessed on 1 September 2023).
- Park, S.Y. Predictive factors of substance misuse and abuse in South Korean adolescents: A secondary data analysis of the 2021 Youth Risk Behavior Web-based Survey. Child Health Nurs. Res. 2024, 30, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Lee, H. Associations between binge drinking experience, depressive mood, and suicidality in adolescents: Based on the 2021 Korea Youth Risk Behavior Web-based Survey. J. Affect. Disord. 2023, 323, 386–391. [Google Scholar] [CrossRef]
- Ministry of Education; Korea Disease Control and Prevention Agency. Korea Youth Risk Behavior Web-Based Survey Raw Data Usage Guidelines. Available online: https://www.kdca.go.kr/yhs/ (accessed on 1 September 2023).
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Savolainen, I.; Oksanen, A.; Kaakinen, M.; Sirola, A.; Paek, H.J. The role of perceived loneliness in youth addictive behaviors: Cross-national survey study. JMIR Ment. Health 2020, 7, e14035. [Google Scholar] [CrossRef]
- Kim, H. Combined effects of smartphone overdependence and stress on depression and suicide-related behaviors among high school students. Healthcare 2022, 10, 1671. [Google Scholar] [CrossRef]
- Thapar, A.; Collishaw, S.; Pine, D.S.; Thapar, A.K. Depression in adolescence. Lancet 2012, 379, 1056–1067. [Google Scholar] [CrossRef]
- McClure-Thomas, C.; Lim, C.; Sebayang, S.; Fausiah, F.; Gouda, H.; Leung, J. Perceived loneliness, peer, and parental relationship with smoking: A cross-sectional analysis of adolescents across South-East Asia. Asia Pac. J. Public Health 2022, 34, 770–777. [Google Scholar] [CrossRef]
- Groenman, A.P.; Janssen, T.W.P.; Oosterlaan, J. Childhood psychiatric disorders as risk factor for subsequent substance abuse: A meta-analysis. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 556–569. [Google Scholar] [CrossRef] [PubMed]
- Khantzian, E.J. The self-medication hypothesis of addictive disorders: Focus on heroin and cocaine dependence. Am. J. Psychiatry 1985, 142, 1259–1264. [Google Scholar] [CrossRef] [PubMed]
- Dyal, S.R.; Valente, T.W. A systematic review of loneliness and smoking: Small effects, big implications. Subst. Use Misuse 2015, 50, 1697–1716. [Google Scholar] [CrossRef] [PubMed]
- Berberian, S.; Patock-Peckham, J.A.; Guarino, K.; Gupta, T.; Sanabria, F.; Infurna, F. Does loneliness before the age of twelve indirectly affect impaired control over drinking, alcohol use, and problems through perceived stress? Addict. Behav. Rep. 2022, 16, 100448. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, J.T.; Hawkley, L.C.; Ernst, J.M.; Burleson, M.; Berntson, G.G.; Nouriani, B.; Spiegel, D. Loneliness within a nomological net: An evolutionary perspective. J. Res. Pers. 2006, 40, 1054–1085. [Google Scholar] [CrossRef]
- Matthews, T.; Danese, A.; Wertz, J.; Odgers, C.L.; Ambler, A.; Moffitt, T.E.; Arseneault, L. Social isolation, loneliness and depression in young adulthood: A behavioural genetic analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 339–348. [Google Scholar] [CrossRef]
- Horigian, V.E.; Schmidt, R.D.; Feaster, D.J. Loneliness, mental health, and substance use among US young adults during COVID-19. J. Psychoact. Drugs 2021, 53, 1–9. [Google Scholar] [CrossRef]
- Espada, J.P.; Sussman, S.; Medina, T.B.H.; Alfonso, J.P. Relation between substance use and depression among Spanish adolescents. Int. J. Psychol. Psychol. Ther. 2011, 11, 79–90. [Google Scholar]
- Turner, S.; Mota, N.; Bolton, J.; Sareen, J. Self-medication with alcohol or drugs for mood and anxiety disorders: A narrative review of the epidemiological literature. Depress. Anxiety 2018, 35, 851–860. [Google Scholar] [CrossRef]
- Kupfer, D.J. The pharmacological management of depression. Dialogues Clin. Neuroscl. 2005, 7, 191–205. [Google Scholar] [CrossRef]
- Farooqui, M.; Shoaib, S.; Afaq, H.; Quadri, S.; Zaina, F.; Baig, A.; Liaquat, A.; Sarwar, Z.; Younus, S. Bidirectionality of smoking and depression in adolescents: A systematic review. Trends Psychiatry Psychother. 2023, 45, e20210429. [Google Scholar] [CrossRef] [PubMed]
- Danneel, S.; Geukens, F.; Maes, M.; Bastin, M.; Bijttebier, P.; Colpin, H.; Verschueren, K.; Goossens, L. Loneliness, social anxiety symptoms, and depressive symptoms in adolescence: Longitudinal distinctiveness and correlated change. J. Youth Adolesc. 2020, 49, 2246–2264. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Assessment |
|---|---|
| General characteristics | |
| Age | In which year and month were you born? |
| Gender | Male or female |
| School | 1st, 2nd, or 3rd year of middle school or high school |
| Residential area † | Metropolis, mid-sized city, or rural area |
| Economic status | What is your household’s financial situation? Possible responses are high, middle-high, middle, middle-low, or low. |
| Academic achievement | How has your academic performance been in the past 12 months? Possible responses are high, middle-high, middle, middle-low, or low. |
| Living with family | What is your current living situation? Possible responses are living with family, living with relatives, boarding house/living alone, dormitory, or youth facilities. |
| Perceived health status | How do you perceive your usual health status? Possible responses are very healthy, healthy, fair, unhealthy, or very unhealthy. |
| Sleep satisfaction | In the last 7 days, did you have enough sleep time to recover from fatigue? Possible responses are very sufficient, sufficient, fair, insufficient, or very insufficient. |
| Stress | How much stress do you usually feel? Possible responses are very high, high, moderate, low, or none. |
| Sexual intercourse | Have you ever had sexual intercourse? Yes or no |
| Smoking-related variables | |
| Exposure to smoking advertisements | In the last 30 days, have you seen any smoking advertisements? Possible responses are magazines, internet, convenience store, supermarket, or not seen. |
| Exposure to anti-smoking campaigns | In the last 12 months, have you seen or heard any anti-smoking campaigns? Possible responses are TV, radio, TV program/news, internet, newspaper, subway/bus stop, or not seen. |
| Exposure to secondhand smoke | During the last 7 days, on how many days did you inhale secondhand smoke at home, school, or indoors? Possible responses are between 0 and 7 days per week. |
| Experience of smoking cessation education | In the last 12 months, have you received smoking prevention or cessation education at school? Yes or no |
| Smoking in family | Please indicate if anyone in your family currently smokes. Possible responses are none, father, mother, siblings, or grandparents |
| Smoking in close friends | Do you have any close friends who smoke? Possible responses are none, a few, many, or everyone |
| Drinking-related variables | |
| Experience of alcohol education | In the last 12 months, have you received any alcohol education at school? Yes or no |
| Allowing drinking at home | Have your parents or relatives ever encouraged (allowed) you to drink alcohol at home? Yes or no |
| Exposure to alcohol advertisements | In the last 30 days, on how many days have you seen alcohol advertisements on the television, internet, social media, posters, and so on? Possible responses are 1 day/month, 2~3 days/month, 1~2 days/week, 3~4 days/week, 5~6 days/week, 7 days, or not seen. |
| Variable | Categories | n † (%) ‡ or M ± SD ‡ |
|---|---|---|
| Independent variable | ||
| Loneliness | No | 44,837 (84.1) |
| Yes | 8473 (15.9) | |
| Dependent variables | ||
| Smoking | Yes | 2666 (5.1) |
| No | 50,644 (94.9) | |
| Drinking alcohol | Binge-drinking | 2534 (4.9) |
| Non-binge-drinking | 14,896 (28.0) | |
| Non-drinking | 35,880 (67.1) | |
| Drug use | Yes | 384 (0.7) |
| No | 52,926 (99.3) | |
| Mediating variable | ||
| Depression | Yes | 14,239 (26.7) |
| No | 39,071 (73.3) | |
| General characteristics | ||
| Age | 15.24 ± 0.02 | |
| Gender | Male | 27,644 (51.7) |
| Female | 25,666 (48.3) | |
| School | Middle school | 29,064 (50.7) |
| High school | 24,246 (49.3) | |
| Residential area | Metropolis | 26,701 (49.9) |
| Mid-sized city | 23,487 (45.6) | |
| Rural area | 3122 (4.5) | |
| Economic status | High | 21,067 (40.3) |
| Middle | 26,226 (48.8) | |
| Low | 6017 (10.9) | |
| Academic achievement | High | 20,028 (37.3) |
| Middle | 16,433 (31.0) | |
| Low | 16,849 (31.7) | |
| Living with family | Yes | 50,990 (96.2) |
| No | 2320 (3.8) | |
| Perceived health status | Unhealthy | 4860 (9.2) |
| Fair | 13,848 (26.0) | |
| Healthy | 34,602 (64.8) | |
| Sleep satisfaction | Sufficient | 12,480 (22.9) |
| Fair | 17,393 (32.4) | |
| Insufficient | 23,437 (44.7) | |
| Stress | High | 20,598 (38.7) |
| Moderate | 22,592 (42.6) | |
| Low | 10,120 (18.7) | |
| Sexual intercourse | Yes | 2759 (5.4) |
| No | 50,551 (94.6) | |
| Smoking-related variables | ||
| Exposure to smoking advertisements | Yes | 18,147 (33.8) |
| No | 35,163 (66.2) | |
| Exposure to anti-smoking campaigns | Yes | 38,678 (72.7) |
| No | 14,632 (27.3) | |
| Exposure to secondhand smoke | Yes | 28,354 (53.3) |
| No | 24,956 (46.7) | |
| Experience of smoking cessation education | Yes | 34,508 (63.1) |
| No | 18,802 (36.9) | |
| Smoking in family | Yes | 28,069 (51.6) |
| No | 25,241 (48.4) | |
| Smoking in close friends | Yes | 16,375 (31.2) |
| No | 36,935 (68.8) | |
| Drinking-related variables | ||
| Experience of alcohol education | Yes | 18,103 (32.9) |
| No | 35,207 (67.1) | |
| Allowing drinking at home | Yes | 17,903 (33.8) |
| No | 35,407 (66.2) | |
| Exposure to alcohol advertisements | <1/week | 27,611 (51.5) |
| ≥1/week | 25,699 (48.5) | |
| Variable | Categories | Smoking | Rao–Scott χ2 Test or t | p | Drinking Alcohol | Rao–Scott χ2 Test or t | p | Drug Use | Rao–Scott χ2 Test or t | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | Binge-Drinking | Non-Binge-Drinking | Non-Drinking | Yes | No | ||||||||
| n † (%) ‡ or M ± SD ‡ | n † (%) ‡ or M ± SD ‡ | n † (%) ‡ or M ± SD ‡ | n † (%) ‡ or M ± SD ‡ | n † (%) ‡ or M ± SD ‡ | n † (%) ‡ or M ± SD ‡ | n † (%) ‡ or M ± SD ‡ | ||||||||
| Loneliness | No | 1950 (72.9) | 42,887 (84.7) | 271.13 | <0.001 | 1789 (70.6) | 11,930 (80.0) | 31,118 (86.7) | 345.21 | <0.001 | 223 (55.9) | 44,614 (84.3) | 228.99 | <0.001 |
| Yes | 716 (27.1) | 7757 (15.3) | 745 (29.4) | 2966 (20.0) | 4762 (13.3) | 161 (44.1) | 8312 (15.7) | |||||||
| Depression | Yes | 1184 (44.2) | 13,055 (25.8) | 385.42 | <0.001 | 1182 (47.1) | 4810 (32.0) | 8247 (23.0) | 412.20 | <0.001 | 196 (52.3) | 14,043 (26.5) | 130.32 | <0.001 |
| No | 1482 (55.8) | 37,589 (74.2) | 1352 (52.9) | 10,086 (68.0) | 27,633 (77.0) | 188 (47.7) | 38,883 (73.5) | |||||||
| Age | 16.30 ± 0.04 | 15.18 ± 0.02 | 24.16 | <0.001 | 16.46 ± 0.03 | 15.77 ± 0.02 | 14.93 ± 0.02 | 1045.49 | <0.001 | 15.48 ± 0.09 | 15.64 ± 0.02 | 1.78 | 0.075 | |
| Gender | Male | 1826 (69.7) | 25,818 (50.7) | 197.93 | <0.001 | 1373 (56.0) | 8885 (59.7) | 17,386 (48.1) | 144.86 | <0.001 | 227 (56.2) | 27,417 (51.7) | 3.03 | 0.082 |
| Female | 840 (30.3) | 24,826 (49.3) | 1161 (44.0) | 6011 (40.3) | 18,494 (51.9) | 157 (43.38) | 25,509 (48.3) | |||||||
| School | Middle school | 668 (22.3) | 28,396 (52.3) | 499.57 | <0.001 | 529 (17.8) | 6187 (37.0) | 22,348 (58.9) | 872.95 | <0.001 | 188 (46.8) | 28,876 (50.8) | 2.38 | 0.124 |
| High school | 1998 (77.7) | 22,248 (47.7) | 2005 (82.2) | 8709 (63.0) | 13,532 (41.1) | 196 (53.2) | 24,050 (49.2) | |||||||
| Residential area | Metropolis | 1214 (46.3) | 25,487 (50.1) | 3.88 | 0.026 | 1070 (43.3) | 6956 (46.8) | 18,675 (51.8) | 20.66 | <0.001 | 185 (46.1) | 26,516 (50.0) | 2.22 | 0.111 |
| Mid-sized city | 1289 (49.2) | 22,198 (45.4) | 1272 (51.3) | 6882 (47.9) | 15,333 (44.2) | 178 (50.4) | 23,309 (45.6) | |||||||
| Rural area | 163 (4.5) | 2959 (4.5) | 192 (5.4) | 1058 (5.3) | 1872 (4.0) | 21 (3.5) | 3101 (4.4) | |||||||
| Economic status | High | 955 (36.8) | 20,112 (40.5) | 93.01 | < 0.001 | 891 (36.3) | 5397 (36.9) | 14,779 (42.1) | 93.08 | <0.001 | 151 (39.0) | 20,916 (40.3) | 16.52 | <0.001 |
| Middle | 1198 (44.1) | 25,028 (49.1) | 1170 (45.8) | 7396 (49.5) | 17,660 (48.7) | 156 (41.1) | 26,070 (48.8) | |||||||
| Low | 513 (19.1) | 5504 (10.4) | 473 (17.9) | 2103 (13.6) | 3441 (9.2) | 77 (19.9) | 5940 (10.8) | |||||||
| Academic achievement | High | 586 (21.8) | 19,442 (38.1) | 260.62 | <0.001 | 667 (26.1) | 4696 (31.3) | 14,665 (40.6) | 186.60 | <0.001 | 154 (38.8) | 19,874 (37.3) | 9.27 | <0.001 |
| Middle | 674 (25.4) | 15,759 (31.3) | 675 (27.4) | 4583 (30.9) | 11,175 (31.3) | 88 (21.6) | 16,345 (31.1) | |||||||
| Low | 1406 (52.8) | 15,443 (30.6) | 1192 (46.5) | 5617 (37.8) | 10,040 (28.1) | 142 (39.6) | 16,707 (31.7) | |||||||
| Living with family | Yes | 2441 (92.0) | 48,549 (96.5) | 65.84 | <0.001 | 2306 (91.5) | 14,145 (95.5) | 34,539 (96.9) | 63.88 | <0.001 | 332 (86.8) | 50,658 (96.3) | 69.67 | <0.001 |
| No | 225(8.0) | 2095 (3.5) | 228 (8.5) | 751 (4.5) | 1341 (3.1) | 52 (13.2) | 2268 (3.7) | |||||||
| Perceived health status | Unhealthy | 330 (12.3) | 4530 (9.0) | 15.30 | <0.001 | 310 (11.9) | 1620 (11.0) | 2930 (8.3) | 27.58 | <0.001 | 85 (23.5) | 4775 (9.1) | 47.95 | <0.001 |
| Fair | 635 (24.7) | 13,213 (26.1) | 624 (24.8) | 3880 (26.0) | 9344 (26.0) | 108 (27.9) | 13,740 (26.0) | |||||||
| Healthy | 1701 (63.0) | 32,901 (64.9) | 1600 (63.3) | 9396 (63.0) | 23,606 (65.7) | 191 (48.6) | 34,411 (64.9) | |||||||
| Sleep satisfaction | Sufficient | 415 (16.1) | 12,065 (23.3) | 78.49 | <0.001 | 371 (15.3) | 2936 (19.5) | 9173 (24.9) | 119.97 | <0.001 | 62 (15.5) | 12,418 (23.0) | 26.83 | <0.001 |
| Fair | 727 (27.0) | 16,666 (32.6) | 649 (24.9) | 4695 (31.1) | 12,049 (33.4) | 90 (21.0) | 17,303 (32.4) | |||||||
| Insufficient | 1524 (56.9) | 21,913 (44.1) | 1514 (59.8) | 7265 (49.4) | 14,658 (41.7) | 232 (63.5) | 23,205 (44.6) | |||||||
| Stress | High | 1310 (48.8) | 19,288 (38.1) | 52.77 | <0.001 | 1240 (49.1) | 6415 (42.8) | 12,943 (36.2) | 74.89 | <0.001 | 239 (61.2) | 20,359 (38.5) | 39.55 | <0.001 |
| Moderate | 945 (35.4) | 21,647 (43.0) | 906 (35.4) | 5988 (40.3) | 15,698 (44.0) | 105 (27.6) | 22,487 (42.7) | |||||||
| Low | 411 (15.8) | 9709 (18.9) | 388 (15.6) | 2493 (16.9) | 7239 (19.8) | 40 (11.2) | 10,080 (18.8) | |||||||
| Sexual intercourse | Yes | 974 (37.1) | 1785 (3.7) | 5087.37 | <0.001 | 805 (32.3) | 1273 (8.8) | 681 (2.0) | 2270.76 | <0.001 | 91 (25.1) | 2668 (5.2) | 246.98 | <0.001 |
| No | 1692 (62.9) | 48,859 (96.3) | 1729 (67.7) | 13,623 (91.2) | 35,199 (98.0) | 293 (74.9) | 50,258 (94.8) | |||||||
| Smoking-related variables | ||||||||||||||
| Exposure to smoking advertisements | Yes | 1911 (71.7) | 33,252 (65.9) | 37.82 | <0.001 | - | - | - | - | - | - | - | - | - |
| No | 755 (28.3) | 17,392 (34.1) | - | - | - | |||||||||
| Exposure to anti-smoking campaigns | Yes | 1894 (71.1) | 26,784 (72.8) | 3.58 | 0.059 | - | - | - | - | - | - | - | - | - |
| No | 772 (28.9) | 13,860 (27.2) | - | - | - | |||||||||
| Exposure to secondhand smoke | Yes | 1849 (69.4) | 26,505 (52.4) | 295.38 | <0.001 | - | - | - | - | - | - | - | - | - |
| No | 817 (30.6) | 24,139 (47.6) | - | - | - | |||||||||
| Experience of smoking cessation education | Yes | 1584 (57.8) | 32,924 (63.4) | 32.62 | <0.001 | - | - | - | - | - | - | - | - | - |
| No | 1082 (42.2) | 17,720 (36.6) | - | - | - | |||||||||
| Smoking in family | Yes | 1729 (64.3) | 26,340 (50.9) | 164.72 | <0.001 | - | - | - | - | - | - | - | - | - |
| No | 937 (35.7) | 24,304 (49.1) | - | - | - | |||||||||
| Smoking in close friends | Yes | 2485 (93.3) | 13,890 (27.8) | 4575.01 | <0.001 | - | - | - | - | - | - | - | - | - |
| No | 181 (6.7) | 36,754 (72.2) | - | - | - | |||||||||
| Drinking-related variables | ||||||||||||||
| Experience of alcohol education | Yes | - | - | - | - | 748 (28.6) | 4699 (30.4) | 12,656 (34.3) | 39.69 | <0.001 | - | - | - | - |
| No | 1786 (71.4) | 10,197 (69.6) | 23,224 (65.7) | |||||||||||
| Allowing drinking at home | Yes | - | - | - | - | 1613 (63.2) | 8711 (58.7) | 7579 (21.2) | 3571.29 | <0.001 | - | - | - | - |
| No | 921 (36.8) | 6185 (41.3) | 28,301 (78.8) | |||||||||||
| Exposure to alcohol advertisements | < 1/week | - | - | - | - | 1370 (53.9) | 7782 (51.8) | 18,459 (51.2) | 3.70 | 0.026 | - | - | - | - |
| ≥ 1/week | 1164 (46.1) | 7114 (48.2) | 17,421 (48.8) | |||||||||||
| Variables | Step | Independent Variables | Dependent Variables | B | SE | AOR | p | Model Fit | Nagelkerke R2 | Sobel Test |
|---|---|---|---|---|---|---|---|---|---|---|
| Wald F (p) | Z (p) | |||||||||
| Smoking † | 1 | Loneliness | Depression | 1.316 | 0.029 | 3.727 | <0.001 | 357.32 (<0.001) | 0.287 | 5.30 (<0.001) |
| 2 | Loneliness | Smoking | 0.249 | 0.060 | 1.283 | <0.001 | 174.81 (<0.001) | 0.378 | ||
| 3 | Loneliness | Smoking | 0.160 | 0.062 | 1.174 | 0.010 | 168.75 (<0.001) | 0.380 | ||
| Depression | Smoking | 0.299 | 0.056 | 1.349 | <0.001 | |||||
| Drinking alcohol ‡ | 1 | Loneliness | Depression | 1.347 | 0.029 | 3.845 | <0.001 | 399.57 (<0.001) | 0.276 | 13.24 (<0.001) |
| 2 | Loneliness | Drinking alcohol | 0.729 | 0.057 | 2.073 | <0.001 | 232.60 (<0.001) | 0.293 | ||
| 3 | Loneliness | Drinking alcohol | 0.492 | 0.060 | 1.636 | <0.001 | 228.36 (<0.001) | 0.298 | ||
| Depression | Drinking alcohol | 0.801 | 0.058 | 2.228 | <0.001 | |||||
| Drug use ∥ | 1 | Loneliness | Depression | 1.369 | 0.029 | 3.933 | <0.001 | 632.61 (<0.001) | 0.272 | 3.64 (<0.001) |
| 2 | Loneliness | Drug use | 0.933 | 0.124 | 2.543 | <0.001 | 39.18 (<0.001) | 0.093 | ||
| 3 | Loneliness | Drug use | 0.802 | 0.128 | 2.230 | <0.001 | 36.57 (<0.001) | 0.096 | ||
| Depression | Drug use | 0.423 | 0.116 | 1.527 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H. The Mediating Effect of Depression on the Relationship between Loneliness and Substance Use in Korean Adolescents. Behav. Sci. 2024, 14, 241. https://doi.org/10.3390/bs14030241
Kim H. The Mediating Effect of Depression on the Relationship between Loneliness and Substance Use in Korean Adolescents. Behavioral Sciences. 2024; 14(3):241. https://doi.org/10.3390/bs14030241
Chicago/Turabian StyleKim, Hyesun. 2024. "The Mediating Effect of Depression on the Relationship between Loneliness and Substance Use in Korean Adolescents" Behavioral Sciences 14, no. 3: 241. https://doi.org/10.3390/bs14030241
APA StyleKim, H. (2024). The Mediating Effect of Depression on the Relationship between Loneliness and Substance Use in Korean Adolescents. Behavioral Sciences, 14(3), 241. https://doi.org/10.3390/bs14030241