

Does Motor Imagery Training Improve Service Performance in Tennis Players? A Systematic Review and Meta-Analysis
Abstract
1. Introduction
2. Materials and Methods
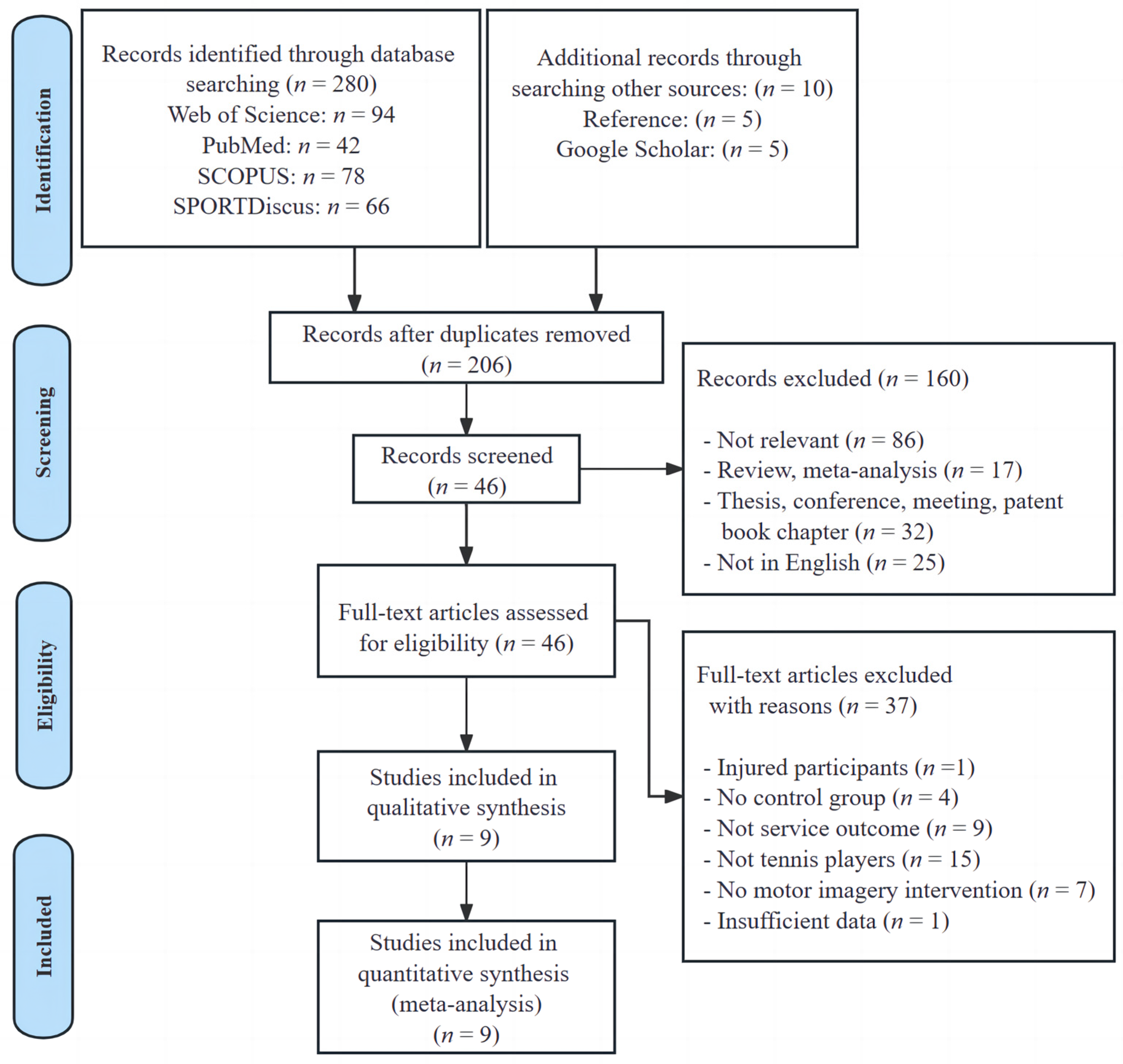
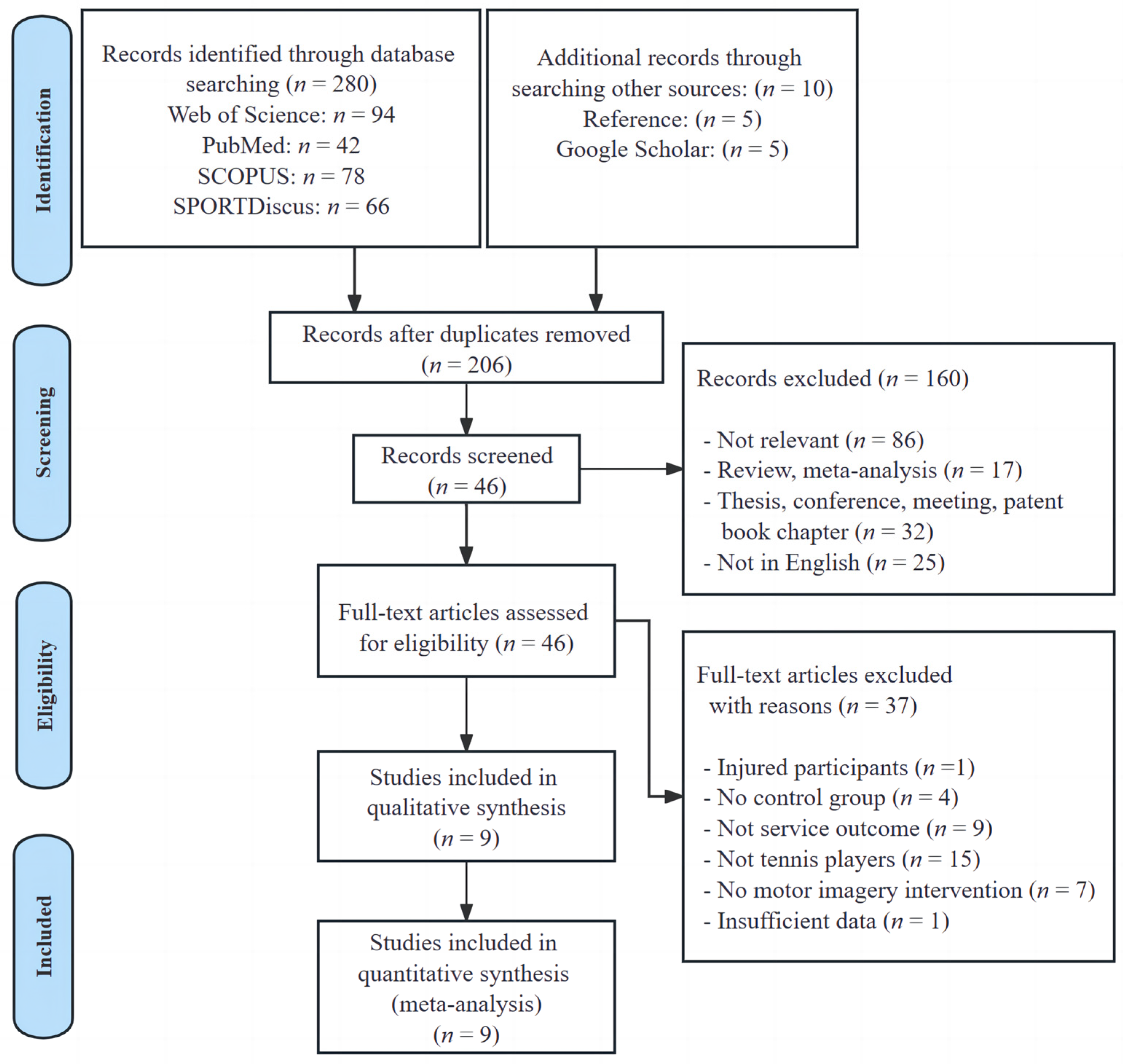
2.1. Search Strategy and Study Selection
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Risk of Bias in Individual Studies and Certainty of the Evidence
2.5. Statistical Analyses
3. Results
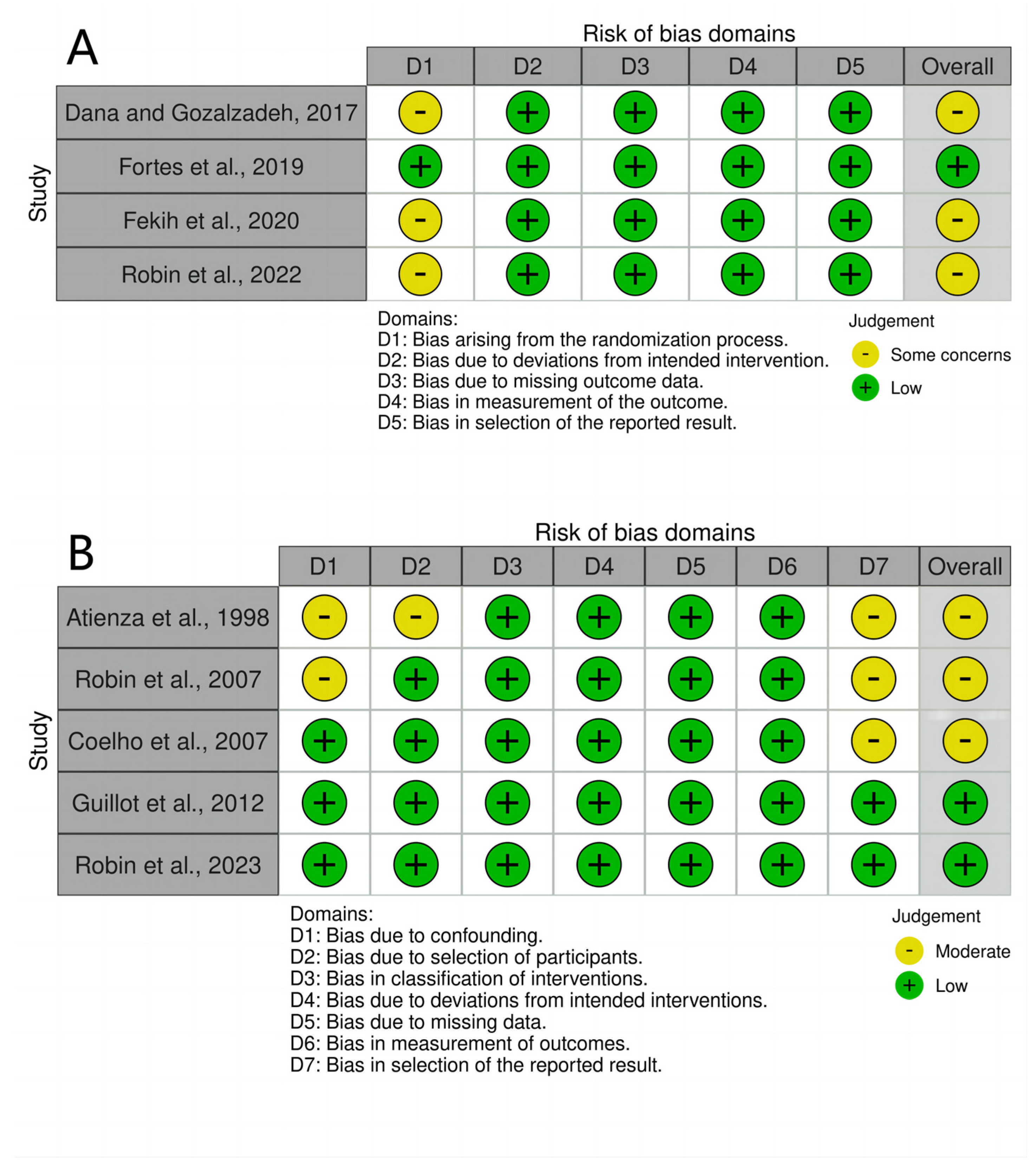
3.1. Risk of Bias in Individual Studies and Certainty of the Evidence
3.2. Study Characteristics
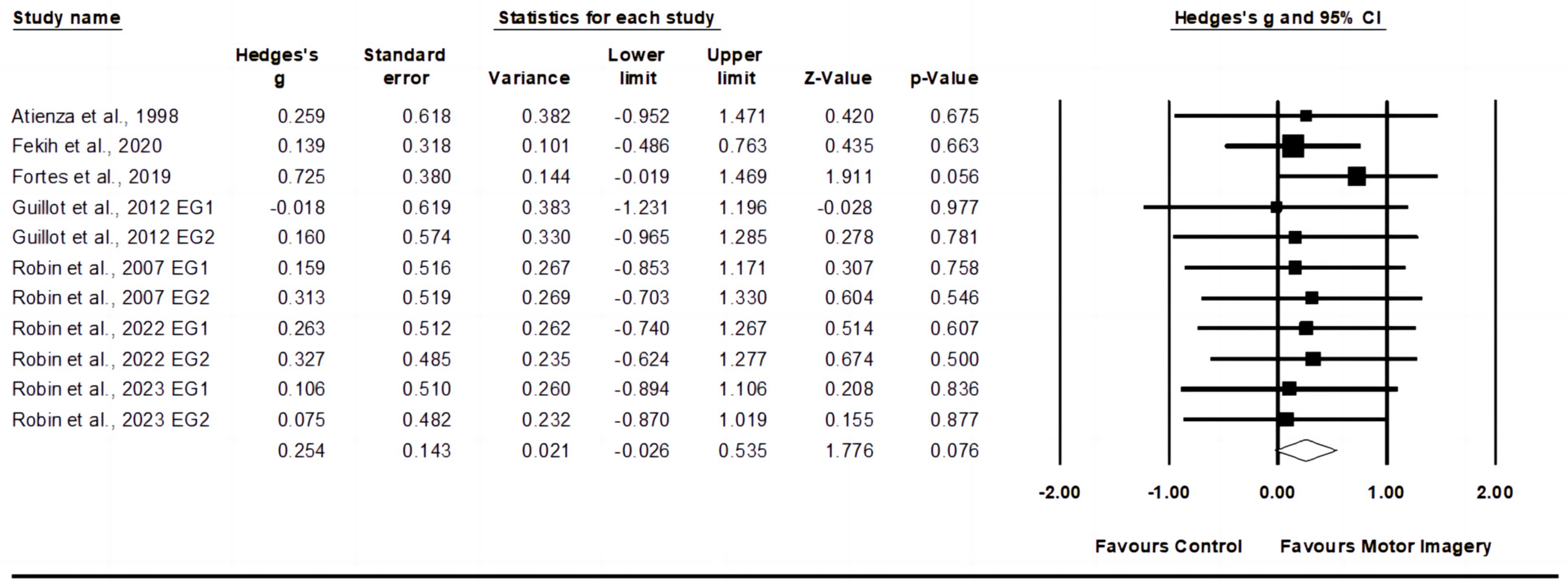
3.3. Effects of Motor Imagery Training on Service Speed
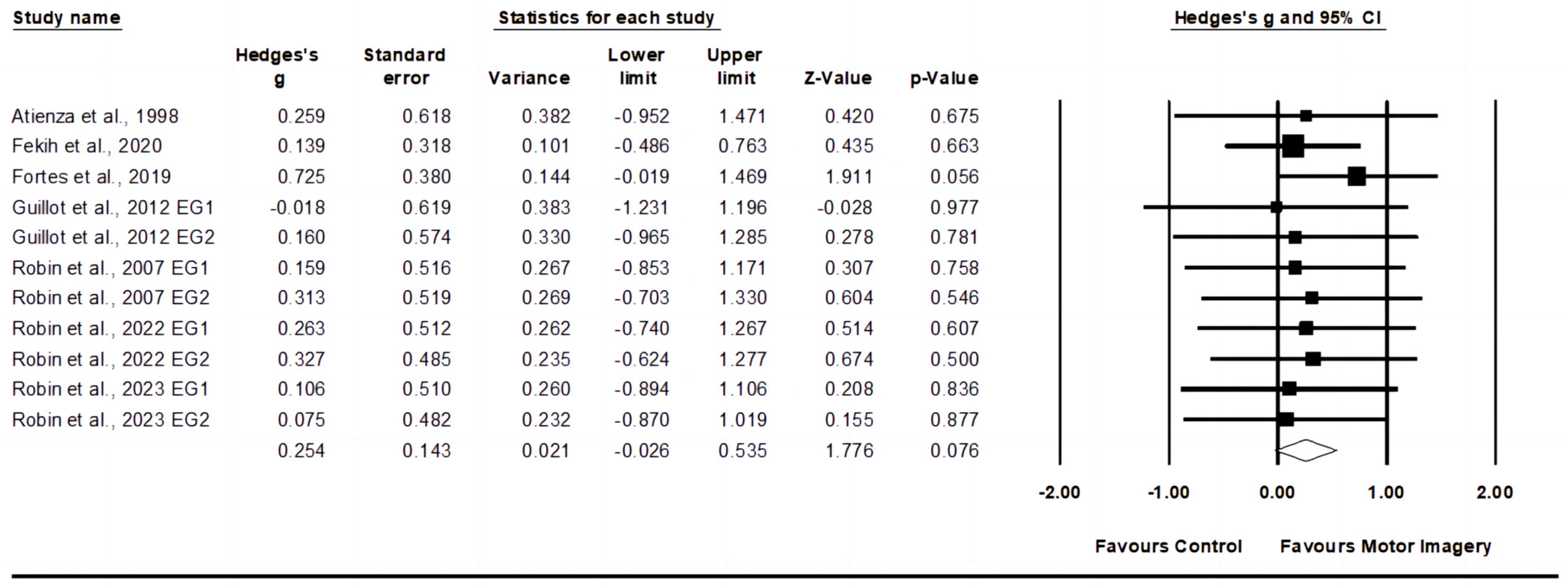
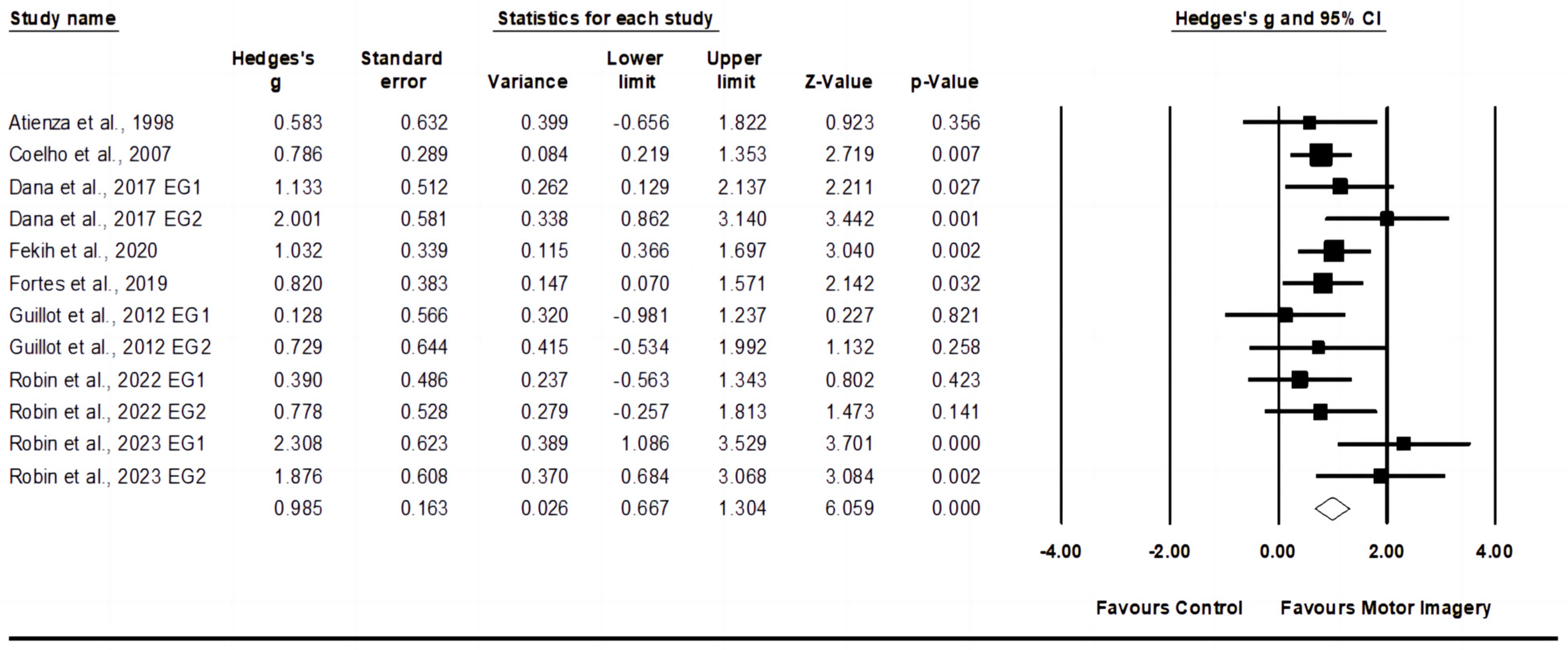
3.4. Effects of Motor Imagery Training on Service Accuracy
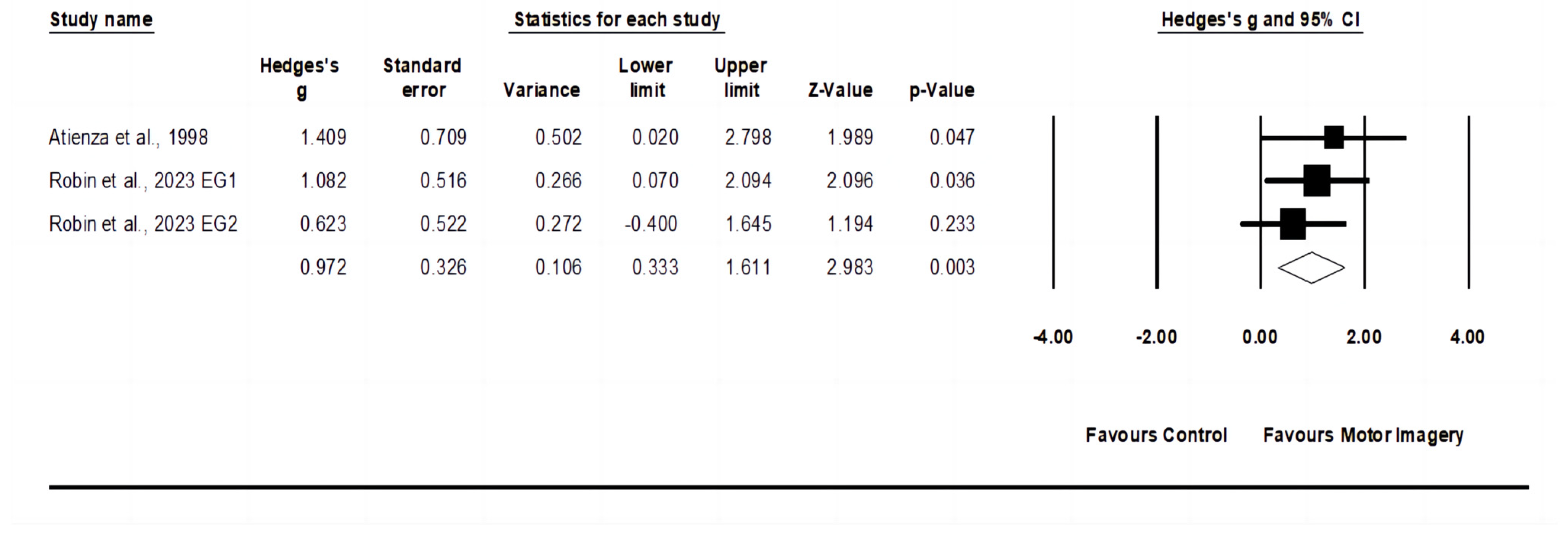
3.5. Effects of Motor Imagery Training on Service Return Accuracy
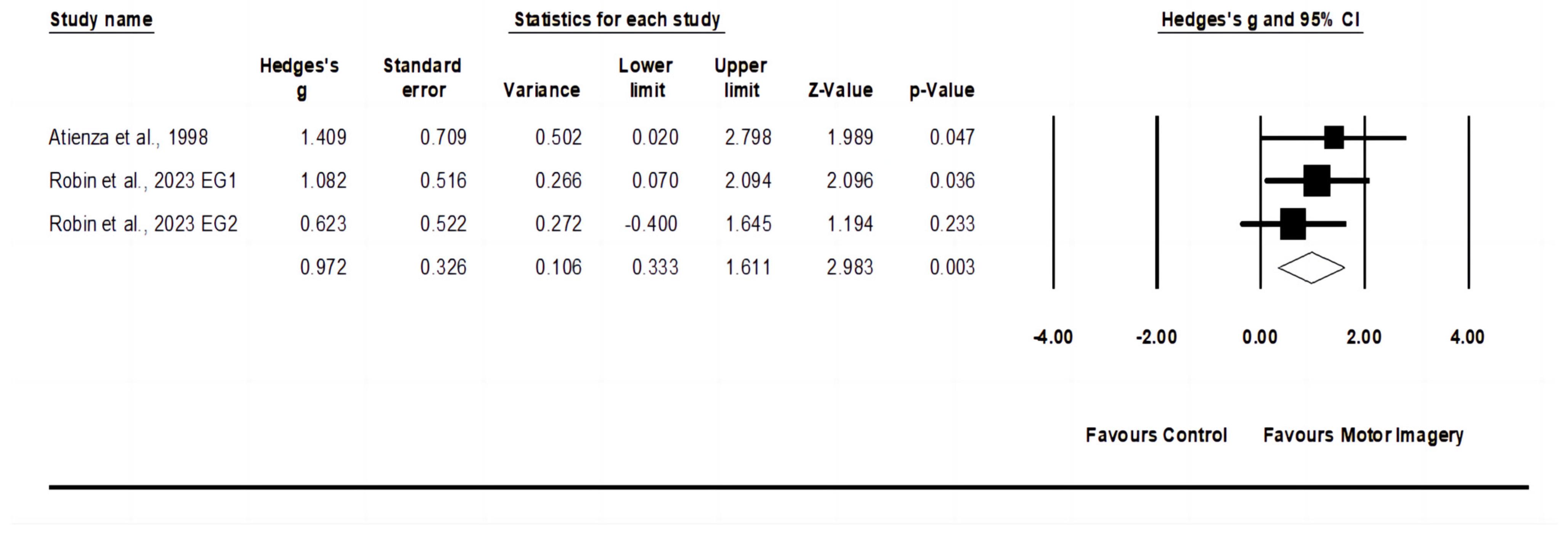
3.6. Effects of Motor Imagery Training on Service Technique
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fett, J.; Oberschelp, N.; Vuong, J.L.; Wiewelhove, T.; Ferrauti, A. Kinematic characteristics of the tennis serve from the ad and deuce court service positions in elite junior players. PLoS ONE 2021, 16, e0252650. [Google Scholar] [CrossRef]
- Whiteside, D.; Reid, M. Spatial characteristics of professional tennis serves with implications for serving aces: A machine learning approach. J. Sports Sci. 2017, 35, 648–654. [Google Scholar] [CrossRef]
- Kovacs, M.; Ellenbecker, T. An 8-stage model for evaluating the tennis serve: Implications for performance enhancement and injury prevention. Sports Health 2011, 3, 504–513. [Google Scholar] [CrossRef]
- Ade, J.; Fitzpatrick, J.; Bradley, P.S. High-intensity efforts in elite soccer matches and associated movement patterns, technical skills and tactical actions. Information for position-specific training drills. J. Sports Sci. 2016, 34, 2205–2214. [Google Scholar] [CrossRef] [PubMed]
- Deng, N.; Soh, K.G.; Abdullah, B.; Huang, D.; Sun, H.; Xiao, W. Effects of physical training programs on female tennis players’ performance: A systematic review and meta-analysis. Front. Physiol. 2023, 14, 1234114. [Google Scholar] [CrossRef] [PubMed]
- Robin, N.; Dominique, L. Mental imagery and tennis: A review, applied recommendations and new research directions. Mov. Sport Sci. Sci. Mot. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Lindsay, R.S.; Larkin, P.; Kittel, A.; Spittle, M. Mental imagery training programs for developing sport-specific motor skills: A systematic review and meta-analysis. Phys. Educ. Sport Pedagog. 2023, 28, 444–465. [Google Scholar] [CrossRef]
- Mulder, T. Motor imagery and action observation: Cognitive tools for rehabilitation. J. Neural Transm. 2007, 114, 1265–1278. [Google Scholar] [CrossRef] [PubMed]
- Vasilyev, A.; Liburkina, S.; Yakovlev, L.; Perepelkina, O.; Kaplan, A. Assessing motor imagery in brain-computer interface training: Psychological and neurophysiological correlates. Neuropsychologia 2017, 97, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Hétu, S.; Grégoire, M.; Saimpont, A.; Coll, M.P.; Eugène, F.; Michon, P.E.; Jackson, P.L. The neural network of motor imagery: An ALE meta-analysis. Neurosci. Biobehav. Rev. 2013, 37, 930–949. [Google Scholar] [CrossRef] [PubMed]
- Jeannerod, M. The representing brain: Neural correlates of motor intention and imagery. Behav. Brain Sci. 1994, 17, 187–202. [Google Scholar] [CrossRef]
- Jeannerod, M. Neural simulation of action: A unifying mechanism for motor cognition. Neuroimage 2001, 14, S103–S109. [Google Scholar] [CrossRef]
- Jeannerod, M. Motor Cognition; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Di Rienzo, F.; Debarnot, U.; Daligault, S.; Saruco, E.; Delpuech, C.; Doyon, J.; Collet, C.; Guillot, A. Online and offline performance gains following motor imagery practice: A comprehensive review of behavioral and neuroimaging studies. Front. Hum. Neurosci. 2016, 10, 315. [Google Scholar] [CrossRef]
- Guillot, A.; Collet, C. Construction of the motor imagery integrative model in sport: A review and theoretical investigation of motor imagery use. Int. Rev. Sport Exerc. Psychol. 2008, 1, 31–44. [Google Scholar] [CrossRef]
- Munzert, J.; Lorey, B. Motor and Visual Imagery in Sports. In Multisensory Imagery; Lacey, S., Lawson, R., Eds.; Springer: New York, NY, USA, 2013. [Google Scholar] [CrossRef]
- Behrendt, F.; Zumbrunnen, V.; Brem, L.; Suica, Z.; Gäumann, S.; Ziller, C.; Gerth, U.; Schuster-Amft, C. Effect of motor imagery training on motor learning in children and adolescents: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 9467. [Google Scholar] [CrossRef] [PubMed]
- Simonsmeier, B.A.; Andronie, M.; Buecker, S.; Frank, C. The effects of imagery interventions in sports: A meta-analysis. Int. Rev. Sport Exerc. Psychol. 2021, 14, 186–207. [Google Scholar] [CrossRef]
- Fazel, F.; Morris, T.; Watt, A.; Maher, R. The effects of different types of imagery delivery on basketball free-throw shooting performance and self-efficacy. Psychol. Sport Exerc. 2018, 39, 29–37. [Google Scholar] [CrossRef]
- Fortes, L.S.; Freitas-Júnior, C.G.; Paes, P.P.; Vieira, L.F.; Nascimento-Júnior, J.R.; Lima-Júnior, D.R.A.A.; Ferreira, M.E. Effect of an eight-week imagery training programme on passing decision-making of young volleyball players. Int. J. Sport Exerc. Psychol. 2020, 18, 120–128. [Google Scholar] [CrossRef]
- Björkstrand, S.; Jern, P. Evaluation of an imagery intervention to improve penalty taking ability in soccer: A study of two junior girls teams. Nord. Psychol. 2013, 65, 290–305. [Google Scholar] [CrossRef]
- Coelho, R.W.; De Campos, W.; Silva, S.G.D.; Okazaki, F.H.A.; Keller, B. Imagery intervention in open and closed tennis motor skill performance. Percept. Mot. Ski. 2007, 105, 458–468. [Google Scholar] [CrossRef]
- Fortes, L.D.S.; Almeida, S.S.; Nascimento Junior, J.R.A.D.; Vieira, L.F.; Lima-Júnior, D.; Ferreira, M.E.C. Effect of motor imagery training on tennis service performance in young tennis athletes. Rev. De Psicol. Del Deporte 2019, 28, 157–168. Available online: https://ddd.uab.cat/record/202439 (accessed on 16 February 2024).
- Robin, N.; Dominique, L.; Toussaint, L.; Blandin, Y.; Guillot, A.; Her, M.L. Effects of motor imagery training on service return accuracy in tennis: The role of imagery ability. Int. J. Sport Exerc. Psychol. 2007, 5, 175–186. [Google Scholar] [CrossRef]
- Guillot, A.; Genevois, C.; Desliens, S.; Saieb, S.; Rogowski, I. Motor imagery and “placebo-racket effects” in tennis serve performance. Psychol. Sport Exerc. 2012, 13, 533–540. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Amir-Behghadami, M.; Janati, A. Population, Intervention, Comparison, Outcomes and Study (PICOS) design as a framework to formulate eligibility criteria in systematic reviews. Emerg. Med. J. 2020, 37, 387. [Google Scholar] [CrossRef]
- Drevon, D.; Fursa, S.R.; Malcolm, A.L. Intercoder reliability and validity of WebPlotDigitizer in extracting graphed data. Behav. Modif. 2016, 41, 323–339. [Google Scholar] [CrossRef]
- Flemyng, E.; Moore, T.H.; Boutron, I.; Higgins, J.P.; Hróbjartsson, A.; Nejstgaard, C.H.; Dwan, K. Using Risk of Bias 2 to assess results from randomised controlled trials: Guidance from Cochrane. BMJ Evid. Based Med. 2023, 28, 260–266. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.J.; Mustafa, R.A.; Brozek, J.; Steingart, K.R.; Leeflang, M.; Murad, M.H.; Bossuyt, P.; Glasziou, P.; Jaeschke, R.; Lange, S.; et al. GRADE guidelines: 21 part 1. Study design, risk of bias, and indirectness in rating the certainty across a body of evidence for test accuracy. J. Clin. Epidemiol. 2020, 122, 129–141. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated August 2022); Cochrane: London, UK, 2022. [Google Scholar]
- Valentine, J.C.; Pigott, T.D.; Rothstein, H.R. How many studies do you need? A primer on statistical power for meta-analysis. J. Educ. Behav. Stat. 2010, 35, 215–247. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P., Green, S., Eds.; The Cochrane Collaboration: Chichester, UK, 2008; pp. 243–296. [Google Scholar] [CrossRef]
- Kontopantelis, E.; Springate, D.A.; Reeves, D. A re-analysis of the Cochrane Library data: The dangers of unobserved heterogeneity in meta-analyses. PLoS ONE 2013, 8, e69930. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef]
- Higgins, J.P.; Deeks, J.J.; Altman, D.G. Special topics in statistics. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P., Green, S., Eds.; The Cochrane Collaboration: Chichester, UK, 2008; pp. 481–529. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta- analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta- analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Dana, A.; Gozalzadeh, E. Internal and External Imagery Effects on Tennis Skills Among Novices. Percept. Mot. Ski. 2017, 124, 1022–1043. [Google Scholar] [CrossRef] [PubMed]
- Fekih, S.; Zguira, M.S.; Koubaa, A.; Masmoudi, L.; Bragazzi, N.L.; Jarraya, M. Effects of motor mental imagery training on tennis service performance during the ramadan fasting: A randomized, controlled trial. Nutrients 2020, 12, 1035. [Google Scholar] [CrossRef] [PubMed]
- Robin, N.; Dominique, L.; Guillet-Descas, E.; Hue, O. Beneficial Effects of Motor Imagery and Self-Talk on Service Performance in Skilled Tennis Players. Front. Psychol. 2022, 13, 6–11. [Google Scholar] [CrossRef]
- Atienza, F.L.; Balaguer, I.; García-Merita, M.L. Video modeling and imaging training on performance of tennis service of 9- to 12-year-old children. Percept. Mot. Ski. 1998, 87, 519–529. [Google Scholar] [CrossRef]
- Robin, N.; Carien, R.; Taktek, K.; Hatchi, V.; Dominique, L. Effects of motor imagery training on service performance in novice tennis players: The role of imagery ability. Int. J. Sport Exerc. Psychol. 2023. [Google Scholar] [CrossRef]
- Kolman, N.S.; Kramer, T.; Elferink-Gemser, M.T.; Huijgen, B.C.; Visscher, C. Technical and tactical skills related to performance levels in tennis: A systematic review. J. Sports Sci. 2019, 37, 108–121. [Google Scholar] [CrossRef]
- Colomar, J.; Corbi, F.; Baiget, E. Improving tennis serve velocity: Review of training methods and recommendations. Strength Cond. J. 2023, 45, 385–394. [Google Scholar] [CrossRef]
- Lebon, F.; Collet, C.; Guillot, A. Benefits of motor imagery training on muscle strength. J. Strength Cond. Res. 2010, 24, 1680–1687. [Google Scholar] [CrossRef] [PubMed]
- Paravlic, A.H.; Slimani, M.; Tod, D.; Marusic, U.; Milanovic, Z.; Pisot, R. Effects and dose–response relationships of motor imagery practice on strength development in healthy adult populations: A systematic review and meta-analysis. Sports Med. 2018, 48, 1165–1187. [Google Scholar] [CrossRef] [PubMed]
- Boschker, M.S.J.; Bakker, F.C.; Rietberg, M.B. Retroactive interference effects of mentally imagined movement speed. J. Sports Sci. 2000, 18, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Jackson, P.L.; Lafleur, M.F.; Malouin, F.; Richards, C.; Doyon, J. Potential role of mental practice using motor imagery in neurologic rehabilitation. Arch. Phys. Med. Rehabil. 2001, 82, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Guillot, A.; Di Rienzo, F.; Pialoux, V.; Simon, G.; Skinner, S.; Rogowski, I. Implementation of motor imagery during specific aerobic training session in young tennis players. PLoS ONE 2015, 10, e0143331. [Google Scholar] [CrossRef] [PubMed]
- Paris-Alemany, A.; La Touche, R.; Agudo-Carmona, D.; Fernández-Carnero, J.; Gadea-Mateos, L.; Suso-Martí, L.; Cuenca-Martínez, F. Visual motor imagery predominance in professional Spanish dancers. Somatosens. Mot. Res. 2019, 36, 179–188. [Google Scholar] [CrossRef]
- Schmidt, R.A.; Wrisberg, C.A. Motor Learning and Performance: A Situation-Based Learning Approach; Human Kinetics: Champaign, IL, USA, 2008. [Google Scholar]
- Yao, W.X.; Ranganathan, V.K.; Allexandre, D.; Siemionow, V.; Yue, G.H. Kinesthetic imagery training of forceful muscle contractions increases brain signal and muscle strength. Front. Hum. Neurosci. 2013, 7, 561. [Google Scholar] [CrossRef]
- Slimani, M.; Tod, D.; Chaabene, H.; Miarka, B.; Chamari, K. Effects of mental imagery on muscular strength in healthy and patient participants: A systematic review. J. Sports Sci. Med. 2016, 15, 434. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4974856 (accessed on 15 January 2024).
- Miller, B.T.; Clapp, W.C. From vision to decision: The role of visual attention in elite sports performance. Eye Contact Lens 2011, 37, 131–139. [Google Scholar] [CrossRef]
- Hanshaw, G.O.; Sukal, M. Effect of self-talk and imagery on the response time of trained martial artists. Sport Exerc. Perform. Psychol. 2016, 5, 259–265. [Google Scholar] [CrossRef]
- Gelman, R.; Berg, M.; Ilan, Y. A subject-tailored variability-based platform for overcoming the plateau effect in sports training: A narrative review. Int. J. Environ. Res. Public Health 2022, 19, 1722. [Google Scholar] [CrossRef] [PubMed]
- Gillet, E.; Leroy, D.; Thouvarecq, R.; Stein, J.F. A notational analysis of elite tennis serve and serve-return strategies on slow surface. J. Strength Cond. Res. 2009, 23, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Guillot, A.; Louis, M.; Collet, C. Neurophysiological substrates of motor imagery ability. In The Neurophysiological Foundations of Mental and Motor Imagery; Oxford University Press: Oxford, UK, 2010; pp. 109–124. [Google Scholar]
- Anderson, D.I.; Lohse, K.R.; Lopes TC, V.; Williams, A.M. Individual differences in motor skill learning: Past, present and future. Hum. Mov. Sci. 2021, 78, 102818. [Google Scholar] [CrossRef] [PubMed]
- Zapała, D.; Zabielska-Mendyk, E.; Cudo, A.; Jaśkiewicz, M.; Kwiatkowski, M.; Kwiatkowska, A. The role of motor imagery in predicting motor skills in young male soccer players. Int. J. Environ. Res. Public Health 2021, 18, 6316. [Google Scholar] [CrossRef] [PubMed]
- Mizuguchi, N.; Nakata, H.; Uchida, Y.; Kanosue, K. Motor imagery and sport performance. J. Phys. Fit. Sports Med. 2012, 1, 103–111. [Google Scholar] [CrossRef]
- Schuster, C.; Hilfiker, R.; Amft, O.; Scheidhauer, A.; Andrews, B.; Butler, J.; Kischka, U.; Ettlin, T. Best practice for motor imagery: A systematic literature review on motor imagery training elements in five different disciplines. BMC Med. 2011, 9, 75. [Google Scholar] [CrossRef]
- Lacourse, M.G.; Orr, E.L.; Cramer, S.C.; Cohen, M.J. Brain activation during execution and motor imagery of novel and skilled sequential hand movements. Neuroimage 2005, 27, 505–519. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcomes | Certainty Assessment | No of Participants and Studies | Certainty of the Evidence (GRADE) | ||||
|---|---|---|---|---|---|---|---|
| Risk of Bias | Inconsistency | Indirectness | Imprecision | Risk of Publication Bias | |||
| Service speed follow-up: range 4 to 24 weeks | Serious a | Not serious | Not serious | Serious b | Not serious | 192 (7 studies) | ⨁⨁◯◯LOW |
| Service accuracy follow-up: range 4 to 24 weeks | Serious a | Not serious | Not serious | Serious b | Not serious | 237 (8 studies) | ⨁⨁◯◯LOW |
| Service return accuracy follow-up: 8 weeks | Serious a | Not serious | Not serious | Serious b | Not serious | 78 (2 studies) | ⨁⨁◯◯LOW |
| Service technique follow-up: 24 weeks | Serious a | Not serious | Not serious | Serious b | Not serious | 41 (2 studies) | ⨁◯◯◯VERY LOW |
| Study | Population Characteristics | Intervention | Type of Exercise | Outcome (s) | |||
|---|---|---|---|---|---|---|---|
| n | Sex | Age | Level | ||||
| Atienza et al., 1998 [43] | 12 | Female | 9–12 years | Tennis school | Freq: 2 times/week Time: 15 min Length: 24 weeks | EG1: physical practice +video EG2: physical practice +video + imagery training CG: physical practice | EG1: service speed ↑, service accuracy →, Service technique ↑; EG2: Service speed →, service accuracy →, service technique ↑ |
| Robin et al., 2007 [24] | 30 | Male | 19 ± 2.5 years | Regional or national level ≥7 years | Freq:1 time/week Time: 3 min Length: 8 weeks | EG1: motor imagery + physical training (good imagers) EG2: motor imagery + physical training (poor imagers) CG: reading a magazine | EG1: service speed →, service return accuracy ↑; EG2: service speed →, service return accuracy ↑ |
| Coelho et al., 2007 [22] | 48 | Male | 16–18 years | National | Freq: 3 times/week Time: 25 min Length: 8 weeks | EG: imagery + technical practice CG: technical practice | Service accuracy ↑, service return accuracy → |
| Guillot et al., 2012 [25] | 22 | Mixed | EG1: 14.25 ± 2.60 years EG2:14.43 ± 3.05 years CG: 16.29 ± 5.50 years | 3.0 ± 1.2 years | Freq: 2 times/week Time: 15 min Length: 6 weeks | EG1: motor imagery EG2: imagery + placebo racket CG: physical practice | EG1: service speed →, service accuracy ↑; EG2: service speed →, service accuracy ↑ |
| Dana & Gozalzadeh, 2017 [40] | 36 | Male | 15–18 years | Novices | Freq: 3 times/week Time: 15 min Length: 6 weeks | EG1: internal imagery EG2: external imagery CG: physical practice | EG1: service accuracy ↑; EG2: service accuracy ↑ |
| Fortes et al., 2019 [23] | 28 | Male | 15–16 years | ≥2 years | Freq: 3 times/week Time: 10 min Length: 8 weeks | EG: motor imagery + physical/technical training CG: videos (Olympic history) + physical/technical training | Service speed ↑, service accuracy ↑ |
| Fekih et al., 2020 [41] | 38 | Male | EG: 16.9 ± 0.6 years CG: 16.7 ± 0.8 years | Tennis clubs EG: 5.4 ± 1.3 years CG: 5.7 ± 1.2 years | Freq: 3 times/week Time: 10 min Length: 4 weeks | EG: motor imagery CG: videos about the history of the Olympic Games | Service speed →, service accuracy↑ |
| Robin et al., 2022 [42] | 33 | Mixed | 15.9 ± 2.1 years | Regional and national 9.5 ± 1.8 years | Freq: 2 times/week Time: NR Length: 10 weeks | EG1: motor imagery EG2: motor imagery+ self-talk CG: physical practice | EG1: service speed →, service accuracy ↑; EG2: service speed →, service accuracy ↑ |
| Robin et al., 2023 [44] | 33 | Mixed | 9–13 years | Novice 1–2 years | Freq: 1 time/week Time: NR Length: 24 weeks | EG1: motor imagery + physical training (good imagers) EG2: motor imagery + physical training (poor imagers) CG: reading a magazine | EG1: service speed ↑, service accuracy ↑, service technique ↑; EG1: service speed ↑, service accuracy ↑, service technique ↑ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deng, N.; Soh, K.G.; Abdullah, B.B.; Huang, D. Does Motor Imagery Training Improve Service Performance in Tennis Players? A Systematic Review and Meta-Analysis. Behav. Sci. 2024, 14, 207. https://doi.org/10.3390/bs14030207
Deng N, Soh KG, Abdullah BB, Huang D. Does Motor Imagery Training Improve Service Performance in Tennis Players? A Systematic Review and Meta-Analysis. Behavioral Sciences. 2024; 14(3):207. https://doi.org/10.3390/bs14030207
Chicago/Turabian StyleDeng, Nuannuan, Kim Geok Soh, Borhannudin Bin Abdullah, and Dandan Huang. 2024. "Does Motor Imagery Training Improve Service Performance in Tennis Players? A Systematic Review and Meta-Analysis" Behavioral Sciences 14, no. 3: 207. https://doi.org/10.3390/bs14030207
APA StyleDeng, N., Soh, K. G., Abdullah, B. B., & Huang, D. (2024). Does Motor Imagery Training Improve Service Performance in Tennis Players? A Systematic Review and Meta-Analysis. Behavioral Sciences, 14(3), 207. https://doi.org/10.3390/bs14030207