
Actor–Partner Effects of Personality Traits and Psychological Flexibility on Psychological Distress Among Couples Coping with Cancer

 , , , , and
, , , , and
Abstract
1. Introduction
1.1. Psychological Outcomes Among Couples Coping with Cancer
1.2. Personality Traits, Psychological Flexibility, and Psychological Distress
2. Method
2.1. Study Design and Participants
2.2. Procedure
2.3. Measurements
2.4. Statistical Analysis
3. Results
3.1. Sample Description
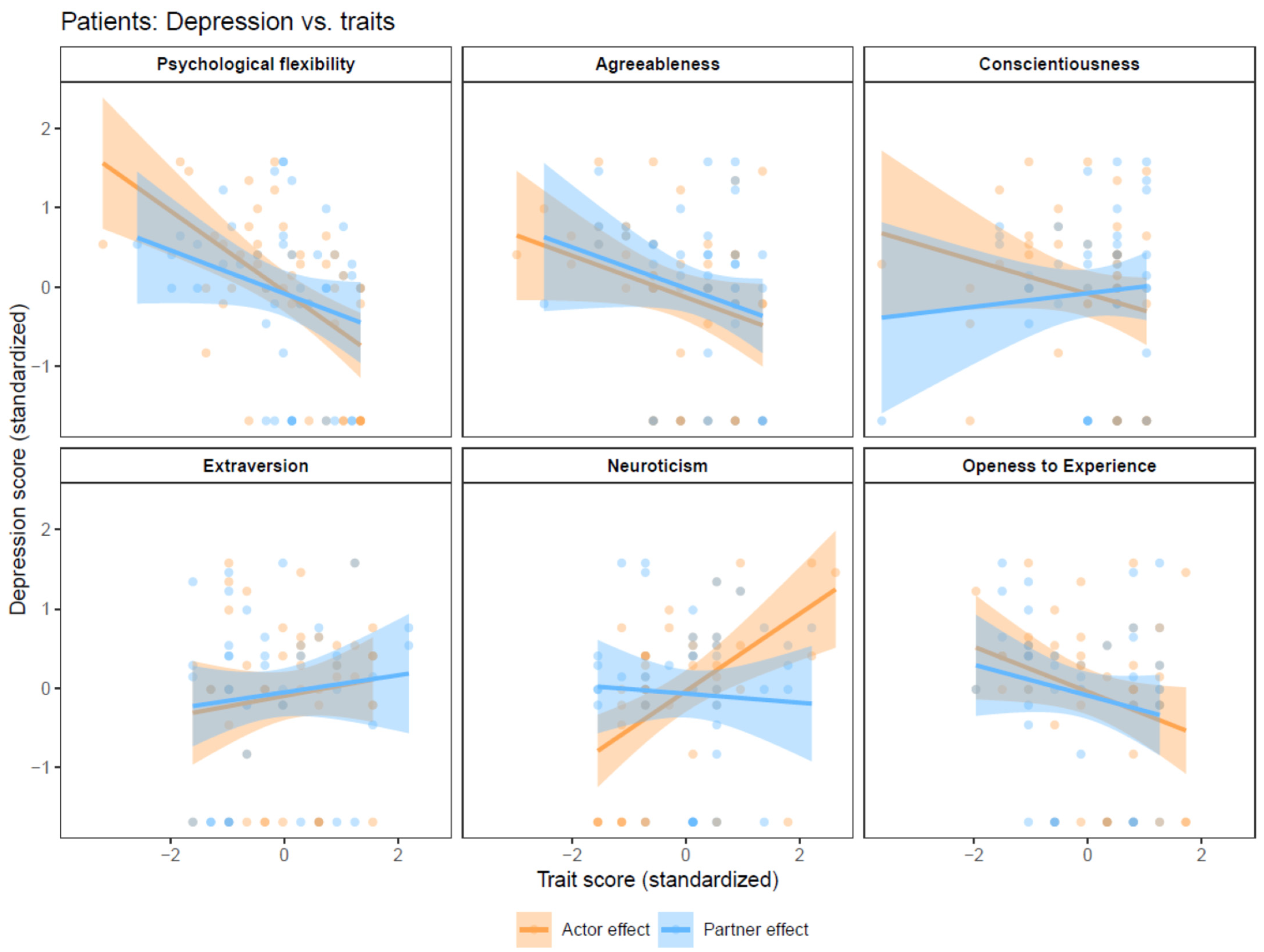
3.2. Patients’ Depression
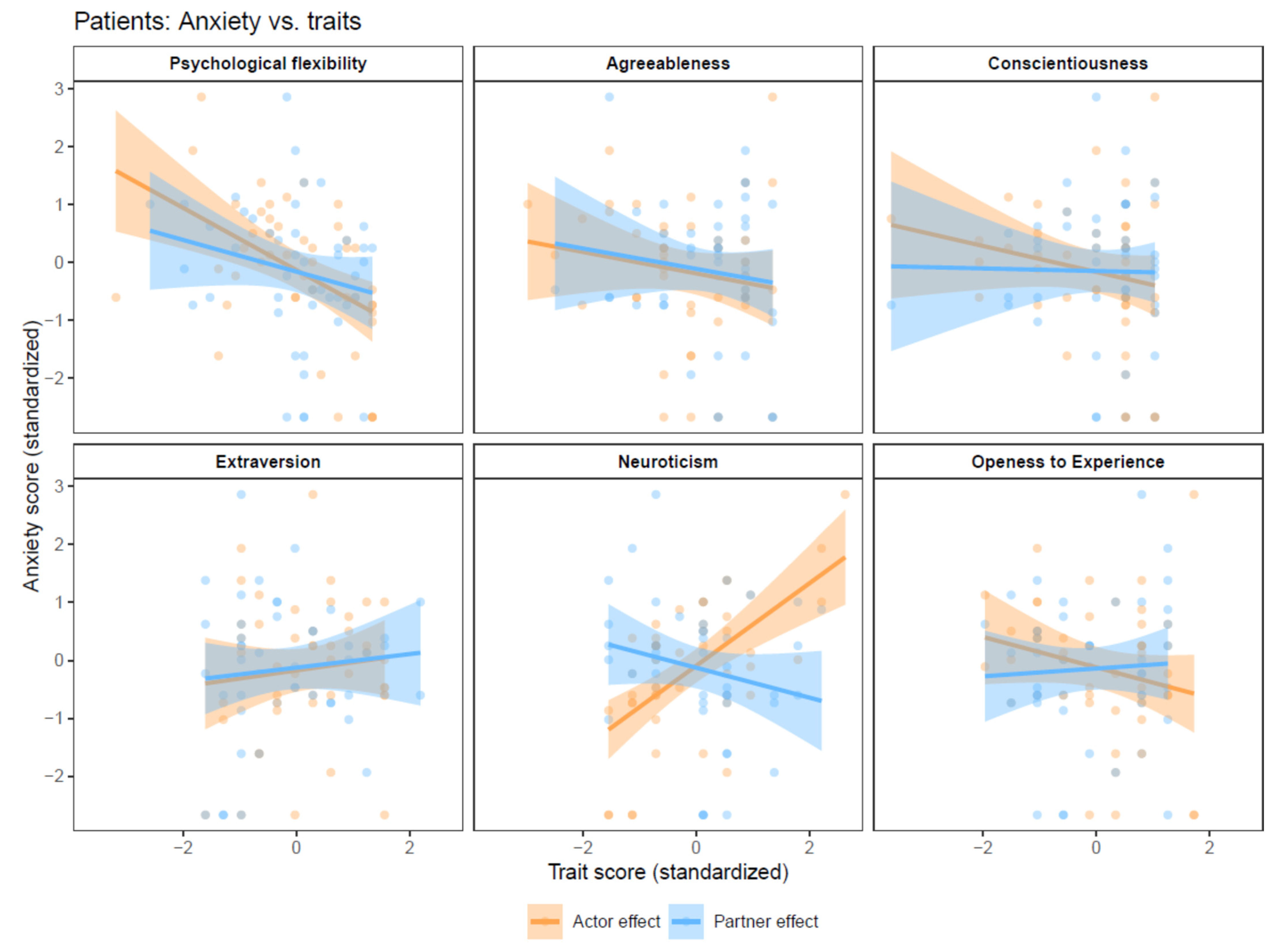
3.3. Patients’ Anxiety
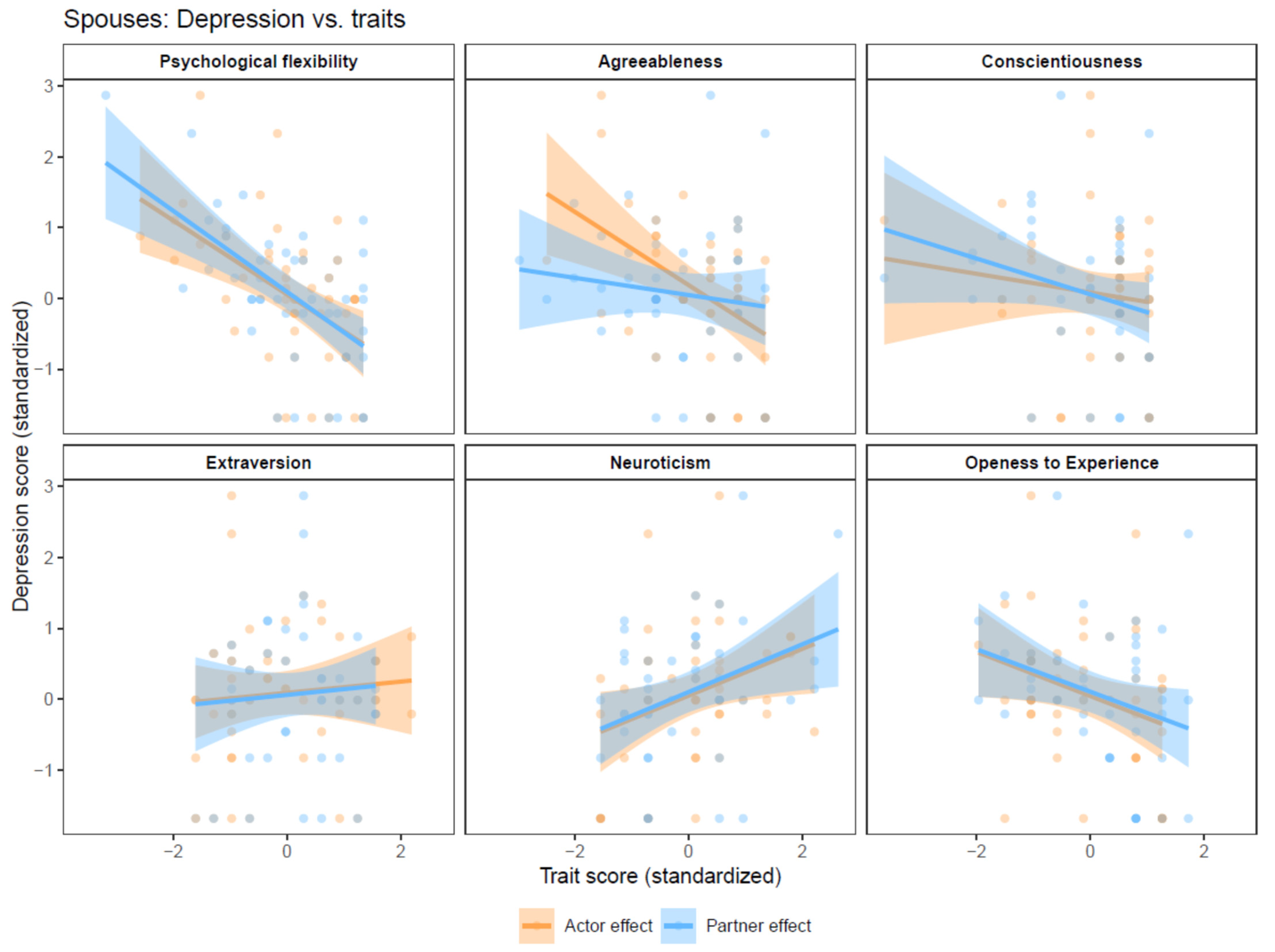
3.4. Spouses’ Depression
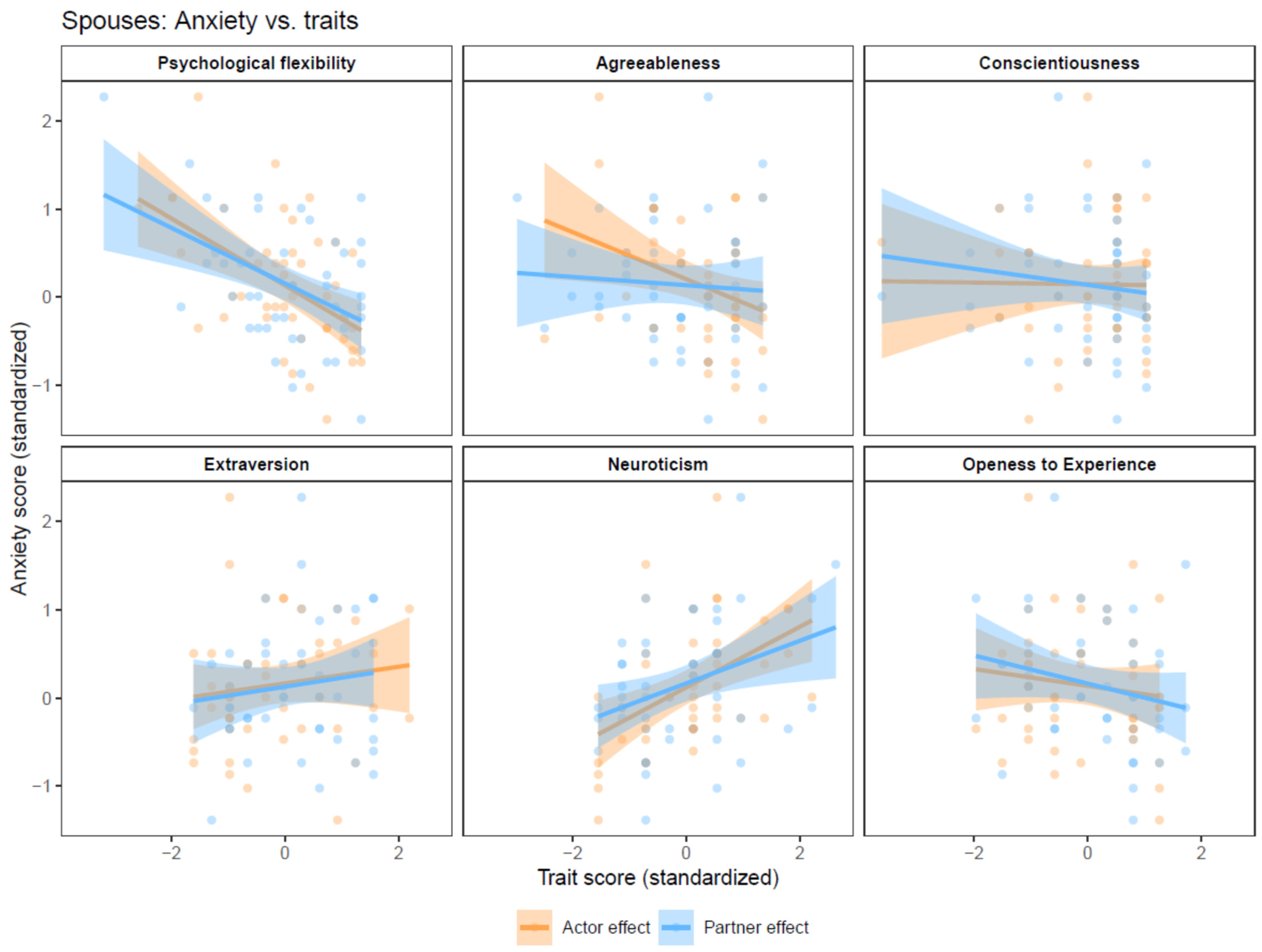
3.5. Spouses’ Anxiety
4. Discussion
5. Limitations
6. Summary and Conclusions of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mehnert, A.; Hartung, T.J.; Friedrich, M.; Vehling, S.; Brähler, E.; Härter, M.; Keller, M.; Schulz, H.; Wegscheider, K.; Weis, J.; et al. One in two cancer patients is significantly distressed: Prevalence and indicators of distress. Psychooncology 2018, 27, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Sun, X.; Yue, H.; Yang, Y.; Feng, D. The dyadic effects of personality traits on depression in advanced lung cancer patients and caregivers: The mediating role of acceptance of illness. Eur. J. Cancer Care 2021, 31, e13538. [Google Scholar] [CrossRef] [PubMed]
- Moser, M.T.; Künzler, A.; Nussbeck, F.; Bargetzi, M.; Znoj, H.J. Higher emotional distress in female partners of cancer patients: Prevalence and patient–partner interdependencies in a 3-year cohort. Psychooncology 2013, 22, 2693–2701. [Google Scholar] [CrossRef]
- Harju, E.; Rantanen, A.; Helminen, M.; Kaunonen, M.; Isotalo, T.; Åstedt-Kurki, P. Marital. relationship and health-related quality of life of patients with prostate cancer and their spouses: A longitudinal clinical study. J. Clin. Nurs. 2018, 27, 2633–2639. [Google Scholar] [CrossRef]
- Pitman, A.; Suleman, S.; Hyde, N.; Hodgkiss, A. Depression and anxiety in patients with cancer. BMJ 2018, 361, k1415. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Ferguson, D.W.; Gill, J.; Paul, J.; Symonds, P. Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: A systematic review and meta-analysis. Lancet Oncol. 2013, 14, 721–732. [Google Scholar] [CrossRef]
- Alacacioglu, A.; Tarhan, O.; Alacacioglu, I.; Dirican, A.; Yilmaz, U. Depression and anxiety in cancer patients and their relatives. J. BUON 2013, 18, 767–774. [Google Scholar]
- Hagedoorn, M.; Sanderman, R.; Bolks, H.N.; Tuinstra, J.; Coyne, J.C. Distress in couples coping with cancer: A meta-analysis and critical review of role and gender effects. Psychol. Bull. 2008, 134, 1–30. [Google Scholar] [CrossRef]
- Traa, M.J.; De Vries, J.; Bodenmann, G.; Oudsten, B.L.D. Dyadic coping and relationship functioning in couples coping with cancer: A systematic review. Br. J. Health Psychol. 2014, 20, 85–114. [Google Scholar] [CrossRef]
- Chen, M.; Gong, J.; Cao, Q.; Luo, X.; Li, J.; Li, Q. A literature review of the relationship between dyadic coping and dyadic outcomes in cancer couples. Eur. J. Oncol. Nurs. 2021, 54, 102035. [Google Scholar] [CrossRef]
- Hasson-Ohayon, I.; Goldzweig, G.; Braun, M.; Hagedoorn, M. Beyond ‘being open about it’: A systematic review on cancer related communication within couples. Clin. Psychol. Rev. 2022, 96, 102176. [Google Scholar] [CrossRef] [PubMed]
- Akin-Odanye, E.O.; Adesanya, B.J. The Big-5 personality traits and personal characteristics as predictors of cancer patients’ quality of life. Afr. J. Psychol. Stud. Soc. Issues 2023, 26, 1–15. [Google Scholar]
- Dahl, A.A. Link Between Personality and Cancer. Futur. Oncol. 2010, 6, 691–707. [Google Scholar] [CrossRef] [PubMed]
- Costa, P.T.; McCrae, R.R. Normal personality assessment in clinical practice: The NEO Personality Inventory. Psychol. Assess. 1992, 4, 5–13. [Google Scholar] [CrossRef]
- Archer, R.P.; Smith, S.R. Personality Assessment, 2nd ed; Routledge: New York, NY, USA, 2014; 500p. [Google Scholar] [CrossRef]
- Rochefort, C.; Hoerger, M.; A Turiano, N.; Duberstein, P. Big Five personality and health in adults with and without cancer. J. Health Psychol. 2019, 24, 1494–1504. [Google Scholar] [CrossRef]
- Huang, I.C.; Lee, J.L.; Ketheeswaran, P.; Jones, C.M.; Revicki, D.A.; Wu, A.W. Does personality affect health-related quality of life? A systematic review. PLoS ONE 2017, 12, e0173806. [Google Scholar] [CrossRef]
- Nisa, S.; Rizvi, T. Relationship of personality traits and coping strategies in cancer patients. Natl. J. Multidiscip. Res. Dev. 2017, 2, 436–439. [Google Scholar]
- Hamidou, Z.; Auquier, P.; Leroy, T.; Barlesi, F.; Salas, S.; Chinot, O.; Baumstarck, K. Dyadic effects of coping strategies, time perspectives, and personality on the quality of life of cancer patients and their caregivers. Psychooncology 2018, 27, 590–599. [Google Scholar] [CrossRef]
- Hayes, S.C.; Strosahl, K.; Wilson, K.G.; Bissett, R.T.; Pistorello, J.; Toarmino, D.; Polusny, M.A.; Dykstra, T.A.; Batten, S.V.; Bergan, J.R.; et al. Measuring experiential avoidance: A preliminary test of a working model. Psychol. Rec. 2004, 54, 553–578. [Google Scholar] [CrossRef]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.; Waltz, T.; Zettle, R.D. Preliminary Psychometric Properties of the Acceptance and Action Questionnaire–II: A Revised Measure of Psychological Inflexibility and Experiential Avoidance. Behav. Ther. 2011, 42, 676–688. [Google Scholar] [CrossRef]
- Montiel, C.B.; Moya, T.R.; Venditti, F.; Bernini, O. On the contribution of psychological flexibility to predict adjustment to breast cancer. Psicothema 2016, 28, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Hulbert-Williams, N.J.; Storey, L. Psychological flexibility correlates with patient-reported outcomes independent of clinical or sociodemographic characteristics. Support. Care Cancer 2016, 24, 2513–2521. [Google Scholar] [CrossRef] [PubMed]
- Sened, H.; Bahorski, S.G.; Callahan, L.; Altpeter, M.; Rini, C. Overcoming Barriers to Physical Activity in People with Osteoarthritis: The Role of Empathic Accuracy in Couples’ Planning Discussions. Int. J. Behav. Med. 2020, 27, 235–246. [Google Scholar] [CrossRef] [PubMed]
- Gosling, S.D.; Rentfrow, P.J.; Swann, W.B., Jr. A very brief measure of the Big-Five personality domains. J. Res. Pers. 2003, 37, 504–528. [Google Scholar] [CrossRef]
- Abdel-Rahman, N.; Manor, O.; Elran, E.; Siscovick, D.; Calderon-Margalit, R. Implications of Patient-Reported Outcome Measures among patients with recently diagnosed type 2 diabetes. Isr. J. Health Policy Res. 2024, 13, 6. [Google Scholar] [CrossRef]
- Cook, W.L.; Kenny, D.A. The Actor–Partner Interdependence Model: A model of bidirectional effects in developmental studies. Int. J. Behav. Dev. 2005, 29, 101–109. [Google Scholar] [CrossRef]
- Smith, T.W. Personality as Risk and Resilience in Physical Health. Curr. Dir. Psychol. Sci. 2006, 15, 227–231. [Google Scholar] [CrossRef]
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. lmerTest Package: Tests in Linear Mixed Effects Models. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat Soc. Ser. B Stat. Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Pinheiro, J.C.; Bates, D.M. Linear mixed-effects models: Basic concepts and examples. In Mixed-Effects Models in S and S-Plus; Springer: New York, NY, USA, 2000; pp. 3–56. [Google Scholar]
- İzci, F.; Sarsanov, D.; Erdogan, Z.I.; Ilgun, A.S.; Celebi, E.; Alco, G.; Kocaman, N.; Ordu, C.; Ozturk, A.; Duymaz, T.; et al. Impact of Personality Traits, Anxiety, Depression and Hopelessness Levels on Quality of Life in the Patients with Breast Cancer. Eur. J. Breast Health 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Hoerger, M.; Coletta, M.; Sörensen, S.; Chapman, B.P.; Kaukeinen, K.; Tu, X.; Duberstein, P.R. Personality and Perceived Health in Spousal Caregivers of Patients with Lung Cancer: The Roles of Neuroticism and Extraversion. J. Aging Res. 2016, 2016, 5659793. [Google Scholar] [CrossRef] [PubMed]
- Jylhä, P.; Isometsä, E. The relationship of neuroticism and extraversion to symptoms of anxiety and depression in the general population. Depress. Anxiety 2006, 23, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Komulainen, E.; Meskanen, K.; Lipsanen, J.; Lahti, J.M.; Jylhä, P.; Melartin, T.; Wichers, M.; Isometsä, E.; Ekelund, J. The Effect of Personality on Daily Life Emotional Processes. PLoS ONE 2014, 9, e110907. [Google Scholar] [CrossRef] [PubMed]
- Perry, L.M.; Hoerger, M.; Silberstein, J.; Sartor, O.; Duberstein, P. Understanding the distressed prostate cancer patient: Role of personality. Psychooncology 2017, 27, 810–816. [Google Scholar] [CrossRef]
- Kansiime, R.; Mutto, M.; Rukundo, G.Z.; Niyonzima, N.; Orem, J.; Kizito, S. Personality and Psychological Well-Being among Cancer Caregivers at the Uganda Cancer Institute and Mbarara Regional Referral Hospital. Afr. J. Soc. Sci. Humanit. Res. 2022, 5, 62–75. [Google Scholar] [CrossRef]
- Toivonen, K.I.; Tamagawa, R.; Speca, M.; Stephen, J.; Carlson, L.E. Open to Exploration? Association of Personality Factors With Complementary Therapy Use After Breast Cancer Treatment. Integr. Cancer Ther. 2018, 17, 785–792. [Google Scholar] [CrossRef]
- Li, H.; Wu, J.; Ni, Q.; Zhang, J.; Wang, Y.; He, G. Systematic Review and Meta—Analysis of Effectiveness of Acceptance and Commitment Therapy in Patients With Breast Cancer. Nurs. Res. 2021, 70, E152–E160. [Google Scholar] [CrossRef]
- Lv, J.; Wu, X.; Yue, H.; Cui, X. Study on the correlation between postoperative mental flexibility, negative emotions, and quality of life in patients with thyroid cancer. Gland Surg. 2021, 10, 2471–2476. [Google Scholar] [CrossRef]
- Luchetti, M.; Terracciano, A.; Stephan, Y.; Aschwanden, D.; Sutin, A.R. Personality and psychological health in caregivers of older relatives: A case-control study. Aging Ment. Health 2020, 25, 1692–1700. [Google Scholar] [CrossRef]
- Hoth, K.F.; Christensen, A.J.; Ehlers, S.L.; Raichle, K.A.; Lawton, W.J. A Longitudinal Examination of Social Support, Agreeableness and Depressive Symptoms in Chronic Kidney Disease. J. Behav. Med. 2007, 30, 69–76. [Google Scholar] [CrossRef]
- Badr, H.; Carmack, C.L.; Kashy, D.A.; Cristofanilli, M.; Revenson, T.A. Dyadic coping in metastatic breast cancer. Health Psychol. 2010, 29, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Linden, W.; Vodermaier, A.; MacKenzie, R.; Greig, D. Anxiety and depression after cancer diagnosis: Prevalence rates by cancer type, gender, and age. J. Affect. Disord. 2012, 141, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Pasek, M.; Suchocka, L. A Model of Social Support for a Patient–Informal Caregiver Dyad. BioMed Res. Int. 2022, 2022, 4470366. [Google Scholar] [CrossRef] [PubMed]
- González-Fernández, S.; Fernández-Rodríguez, C. Acceptance and Commitment Therapy in Cancer: Review of Applications and Findings. Behav. Med. 2018, 45, 255–269. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Independent Variable | APIM Effect | Dependent Variable | B (95% CI) | PUnadjusted | PAdjusted Across Model | PAdjusted Across All |
|---|---|---|---|---|---|---|
| Neuroticism | ||||||
| Patient’s neuroticism | Actor | Patient’s depression | 0.49 (0.24,0.74) | 0.000 | 0.001 | 0.003 |
| Spouse’s neuroticism | Actor | Spouse’s depression | 0.38 (0.12,0.64) | 0.006 | 0.011 | 0.026 |
| Spouse’s neuroticism | Partner | Patient’s depression | 0.00 (−0.26,0.26) | 0.99 | 0.99 | 0.99 |
| Patient’s neuroticism | Partner | Spouse’s depression | 0.37 (0.13,0.62) | 0.005 | 0.011 | 0.022 |
| Extraversion | ||||||
| Patient’s extraversion | Actor | Patient’s depression | 0.08 (−0.24,0.41) | 0.63 | 0.97 | 0.73 |
| Spouse’s extraversion | Actor | Spouse’s depression | 0.04 (−0.25,0.34) | 0.78 | 0.97 | 0.85 |
| Spouse’s extraversion | Partner | Patient’s depression | 0.10 (−0.20,0.39) | 0.53 | 0.97 | 0.73 |
| Patient’s extraversion | Partner | Spouse’s depression | 0.08 (−0.24,0.41) | 0.63 | 0.97 | 0.73 |
| Agreeableness | ||||||
| Patient’s agreeableness | Actor | Patient’s depression | −0.24 (−0.49,0.01) | 0.07 | 0.12 | 0.18 |
| Spouse’s agreeableness | Actor | Spouse’s depression | −0.49 (−0.78,−0.19) | 0.002 | 0.010 | 0.012 |
| Spouse’s agreeableness | Partner | Patient’s depression | −0.29 (−0.58,0.01) | 0.06 | 0.12 | 0.18 |
| Patient’s agreeableness | Partner | Spouse’s depression | −0.14 (−0.39,0.11) | 0.29 | 0.36 | 0.46 |
| Conscientiousness | ||||||
| Patient’s conscientiousness | Actor | Patient’s depression | −0.21 (−0.48,0.06) | 0.14 | 0.34 | 0.27 |
| Spouse’s conscientiousness | Actor | Spouse’s depression | −0.11 (−0.41,0.19) | 0.48 | 0.69 | 0.72 |
| Spouse’s conscientiousness | Partner | Patient’s depression | 0.09 (−0.20,0.39) | 0.55 | 0.69 | 0.73 |
| Patient’s conscientiousness | Partner | Spouse’s depression | −0.25 (−0.52,0.02) | 0.08 | 0.34 | 0.18 |
| Openness to experiences | ||||||
| Patient’s openness to experiences | Actor | Patient’s depression | −0.26 (−0.56,0.04) | 0.10 | 0.33 | 0.21 |
| Spouse’s openness to experiences | Actor | Spouse’s depression | −0.23 (−0.54,0.08) | 0.15 | 0.33 | 0.28 |
| Spouse’s openness to experiences | Partner | Patient’s depression | −0.08 (−0.38,0.23) | 0.64 | 0.80 | 0.73 |
| Patient’s openness to experiences | Partner | Spouse’s depression | −0.20 (−0.50,0.10) | 0.20 | 0.33 | 0.34 |
| Psychological flexibility | ||||||
| Patient’s psychological flexibility | Actor | Patient’s depression | −0.52 (−0.78,−0.26) | <0.001 | 0.001 | 0.003 |
| Spouse’s psychological flexibility | Actor | Spouse’s depression | −0.28 (−0.56,0.01) | 0.07 | 0.12 | 0.18 |
| Spouse’s psychological flexibility | Partner | Patient’s depression | 0.02 (−0.27,0.31) | 0.88 | 0.89 | 0.92 |
| Patient’s psychological flexibility | Partner | Spouse’s depression | −0.44 (−0.70,−0.18) | 0.002 | 0.004 | 0.012 |
| Independent Variable | APIM Effect | Dependent Variable | B (95% CI) | PUnadjusted | PAdjusted Across Model | PAdjusted Across All |
|---|---|---|---|---|---|---|
| Neuroticism | ||||||
| Patient’s neuroticism | Actor | Patient’s anxiety | 0.70 (0.48,0.93) | <0.001 | <0.001 | <0.001 |
| Spouse’s neuroticism | Actor | Spouse’s anxiety | 0.39 (0.15,0.62) | 0.002 | 0.006 | 0.019 |
| Spouse’s neuroticism | Partner | Patient’s anxiety | −0.18 (−0.42,0.05) | 0.14 | 0.18 | 0.38 |
| Patient’s neuroticism | Partner | Spouse’s anxiety | 0.27 (0.05,0.50) | 0.021 | 0.034 | 0.10 |
| Extraversion | ||||||
| Patient’s extraversion | Actor | Patient’s anxiety | 0.07 (−0.26,0.39) | 0.70 | 0.98 | 0.87 |
| Spouse’s extraversion | Actor | Spouse’s anxiety | 0.04 (−0.26,0.33) | 0.81 | 0.98 | 0.89 |
| Spouse’s extraversion | Partner | Patient’s anxiety | 0.12 (−0.17,0.41) | 0.42 | 0.98 | 0.68 |
| Patient’s extraversion | Partner | Spouse’s anxiety | 0.12 (−0.21,0.44) | 0.48 | 0.98 | 0.69 |
| Agreeableness | ||||||
| Patient’s agreeableness | Actor | Patient’s anxiety | −0.15 (−0.42,0.12) | 0.28 | 0.46 | 0.51 |
| Spouse’s agreeableness | Actor | Spouse’s anxiety | −0.22 (−0.53,0.09) | 0.17 | 0.46 | 0.40 |
| Spouse’s agreeableness | Partner | Patient’s anxiety | −0.22 (−0.53,0.09) | 0.18 | 0.46 | 0.40 |
| Patient’s agreeableness | Partner | Spouse’s anxiety | −0.08 (−0.34,0.19) | 0.59 | 0.73 | 0.78 |
| Conscientiousness | ||||||
| Patient’s conscientiousness | Actor | Patient’s anxiety | −0.21 (−0.49,0.06) | 0.14 | 0.69 | 0.38 |
| Spouse’s conscientiousness | Actor | Spouse’s anxiety | 0.01 (−0.29,0.31) | 0.96 | 0.96 | 0.96 |
| Spouse’s conscientiousness | Partner | Patient’s anxiety | −0.02 (−0.32,0.28) | 0.90 | 0.96 | 0.94 |
| Patient’s conscientiousness | Partner | Spouse’s anxiety | −0.10 (−0.38,0.18) | 0.49 | 0.96 | 0.69 |
| Openness to experiences | ||||||
| Patient’s openness to experiences | Actor | Patient’s anxiety | −0.37 (−0.67,−0.07) | 0.021 | 0.10 | 0.10 |
| Spouse’s openness to experiences | Actor | Spouse’s anxiety | −0.05 (−0.37,0.26) | 0.74 | 0.75 | 0.87 |
| Spouse’s openness to experiences | Partner | Patient’s anxiety | 0.24 (−0.07,0.56) | 0.14 | 0.36 | 0.38 |
| Patient’s openness to experiences | Partner | Spouse’s anxiety | −0.13 (−0.43,0.18) | 0.43 | 0.71 | 0.68 |
| Psychological flexibility | ||||||
| Patient’s psychological flexibility | Actor | Patient’s anxiety | −0.56 (−0.85,−0.28) | <0.001 | 0.001 | 0.003 |
| Spouse’s psychological flexibility | Actor | Spouse’s anxiety | −0.28 (−0.60,0.03) | 0.08 | 0.21 | 0.33 |
| Spouse’s psychological flexibility | Partner | Patient’s anxiety | 0.05 (−0.26,0.36) | 0.76 | 0.93 | 0.87 |
| Patient’s psychological flexibility | Partner | Spouse’s anxiety | −0.18 (−0.46,0.11) | 0.23 | 0.38 | 0.46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bar-Moshe-Lavi, L.; Hertz-Palmor, N.; Sella-Shalom, K.; Braun, M.; Pizem, N.; Shacham-Shmueli, E.; Rafaeli, E.; Hasson-Ohayon, I. Actor–Partner Effects of Personality Traits and Psychological Flexibility on Psychological Distress Among Couples Coping with Cancer. Behav. Sci. 2024, 14, 1161. https://doi.org/10.3390/bs14121161
Bar-Moshe-Lavi L, Hertz-Palmor N, Sella-Shalom K, Braun M, Pizem N, Shacham-Shmueli E, Rafaeli E, Hasson-Ohayon I. Actor–Partner Effects of Personality Traits and Psychological Flexibility on Psychological Distress Among Couples Coping with Cancer. Behavioral Sciences. 2024; 14(12):1161. https://doi.org/10.3390/bs14121161
Chicago/Turabian StyleBar-Moshe-Lavi, Leegal, Nimrod Hertz-Palmor, Keren Sella-Shalom, Michal Braun, Noam Pizem, Einat Shacham-Shmueli, Eshkol Rafaeli, and Ilanit Hasson-Ohayon. 2024. "Actor–Partner Effects of Personality Traits and Psychological Flexibility on Psychological Distress Among Couples Coping with Cancer" Behavioral Sciences 14, no. 12: 1161. https://doi.org/10.3390/bs14121161
APA StyleBar-Moshe-Lavi, L., Hertz-Palmor, N., Sella-Shalom, K., Braun, M., Pizem, N., Shacham-Shmueli, E., Rafaeli, E., & Hasson-Ohayon, I. (2024). Actor–Partner Effects of Personality Traits and Psychological Flexibility on Psychological Distress Among Couples Coping with Cancer. Behavioral Sciences, 14(12), 1161. https://doi.org/10.3390/bs14121161