
The Father’s Part: A Pilot Evaluation of a Father-Centered Family Intervention Group in Child and Adolescent Psychiatry
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
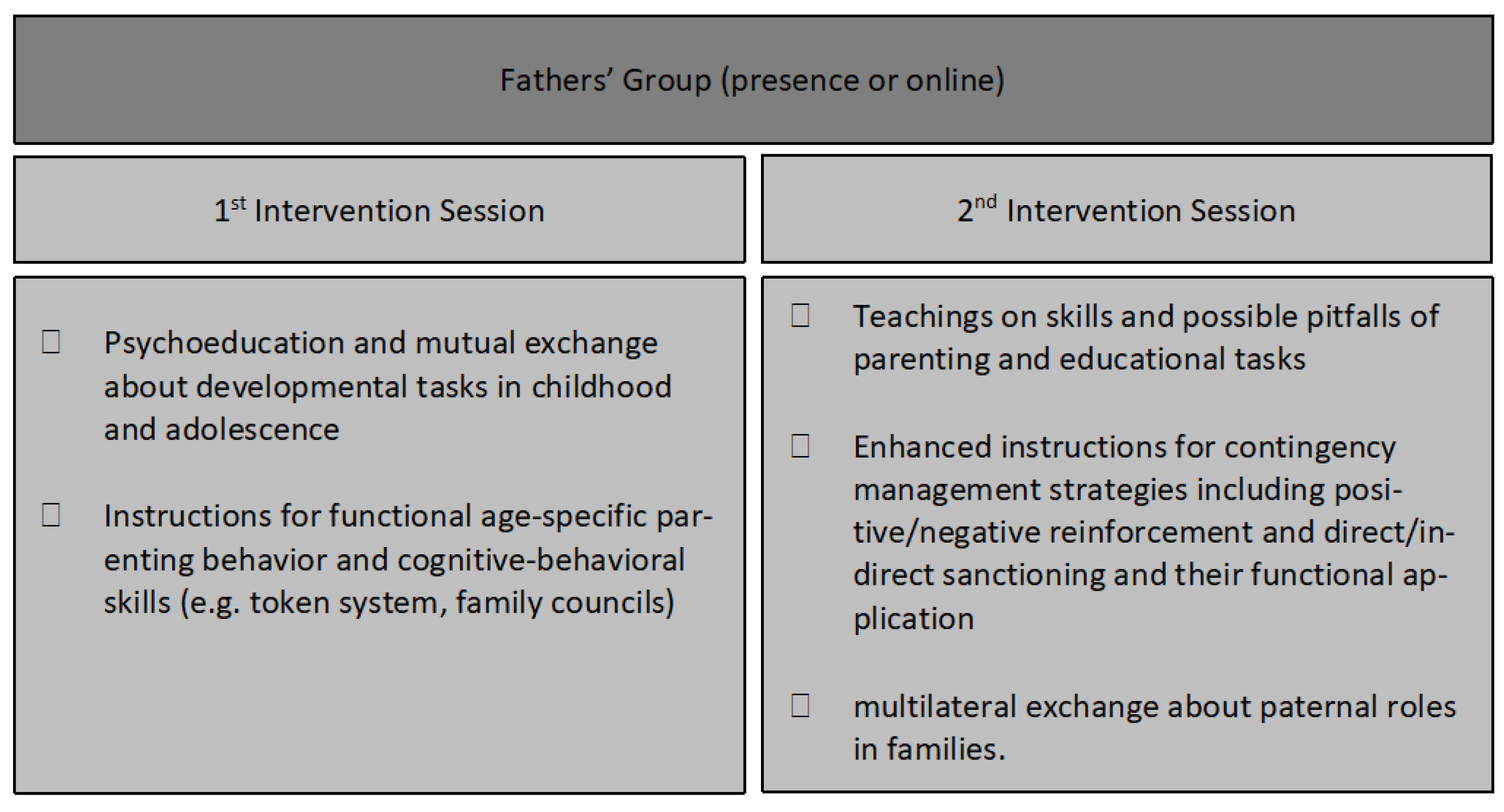
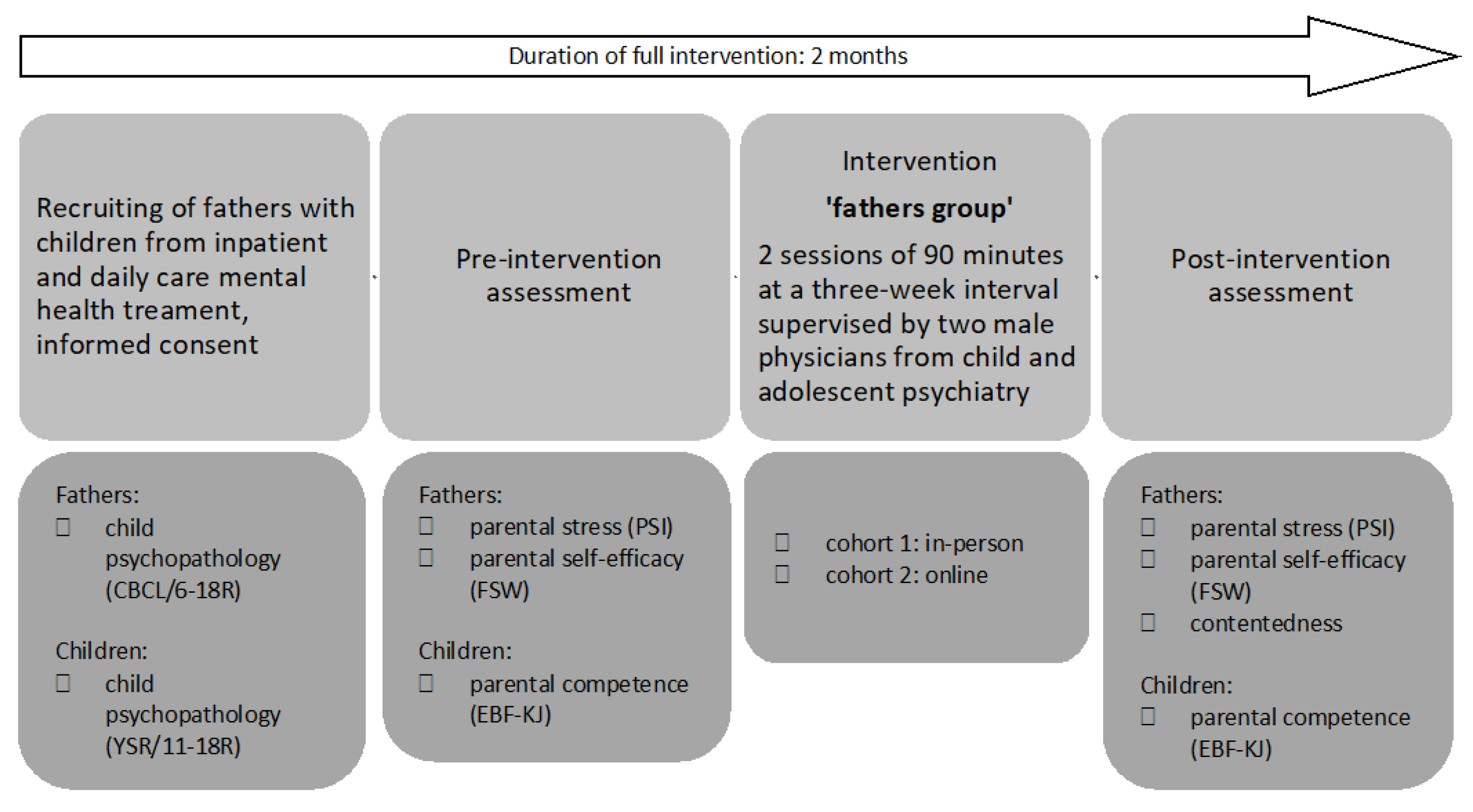
2.1. Intervention and Study Design
2.2. Sample Characteristics
2.3. Data Acquisition
2.4. Statistical Analyses
3. Results
3.1. Child Psychopathology
3.2. Paternal Characteristics
3.3. Participant Satisfaction
4. Discussion
4.1. Father-Group Intervention Effects
4.2. Achieved Power and Required Sample Size: Post-Hoc Analyses
4.3. Presence vs. Online Intervention
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pearce, L.D.; Hayward, G.M.; Chassin, L.; Curran, P.J. The Increasing Diversity and Complexity of Family Structures for Adolescents. J. Res. Adolesc. 2018, 28, 591–608. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Luo, J.; Boele, M.; Windhorst, D.; van Grieken, A.; Raat, H. Parent, child, and situational factors associated with parenting stress: A systematic review. Eur. Child Adolesc. Psychiatry 2022. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, R.; Hiscock, H.; Pan, T.; Devlin, N.; Dalziel, K. The relationship between physical and mental health multimorbidity and children’s health-related quality of life. Qual. Life Res. 2022, 31, 2119–2131. [Google Scholar] [CrossRef] [PubMed]
- Kong, C.; Yasmin, F. Impact of Parenting Style on Early Childhood Learning: Mediating Role of Parental Self-Efficacy. Front. Psychol. 2022, 13, 928629. [Google Scholar] [CrossRef] [PubMed]
- Seiffge-Krenke, I. Neuere Ergebnisse der Vaterforschung. Psychotherapeut 2001, 46, 391–397. [Google Scholar] [CrossRef]
- Gonzalez, J.C.; Klein, C.C.; Barnett, M.L.; Schatz, N.K.; Garoosi, T.; Chacko, A.; Fabiano, G.A. Intervention and Implementation Characteristics to Enhance Father Engagement: A Systematic Review of Parenting Interventions. Clin. Child. Fam. Psychol. Rev. 2023, 26, 445–458. [Google Scholar] [CrossRef]
- Erickson, J. Fathers Don’t Mother and Mothers Don’t Father: What Social Science Research Indicates about the Distinctive Contributions of Mothers and Fathers to Children’s Development. SSRN Electron. J. 2015. [Google Scholar] [CrossRef]
- Yun, Z.; Haimei, H.; Min, W.; Jiawen, Z.; Sumin, T.; Weiyi, T.; Jinli, M.; Li, J.; Jieling, M.; Wei, P.; et al. Family outcome disparities between sexual minority and heterosexual families: A systematic review and meta-analysis. BMJ Glob. Health 2023, 8, e010556. [Google Scholar] [CrossRef]
- Amodia-Bidakowska, A.; Laverty, C.; Ramchandani, P.G. Father-child play: A systematic review of its frequency, characteristics and potential impact on children’s development. Dev. Rev. 2020, 57, 100924. [Google Scholar] [CrossRef]
- Sethna, V.; Perry, E.; Domoney, J.; Iles, J.; Psychogiou, L.; Rowbotham, N.E.L.; Stein, A.; Murray, L.; Ramchandani, P.G. Father-Child Interactions at 3 Months and 24 Months: Contributions to Children’s Cognitive Development at 24 Months. Infant. Ment. Health J. 2017, 38, 378–390. [Google Scholar] [CrossRef]
- Mestermann, S.; Arndt, M.; Fasching, P.A.; Beckmann, M.W.; Kratz, O.; Moll, G.H.; Kornhuber, J.; Eichler, A.; on behalf of the IMAC-Mind-Consortium. The Father’s Part: Influences of Paternal Psychopathology and Parenting Behavior on Child and Adolescent Well-Being. Healthcare 2023, 11, 2119. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, N.J.; Volling, B.L.; Barr, R. Fathers Are Parents, Too! Widening the Lens on Parenting for Children’s Development. Child Dev. Perspect. 2018, 12, 152–157. [Google Scholar] [CrossRef]
- Foster, D.; Rodrigues, M.; Somir, I.; Aziz, T.; Patel, R.; Ragunathan, S.; Sokolovic, N.; Jenkins, J. Paternal Positivity and Child Mental Health: A Meta-Analysis. J. Child Fam. Stud. 2022, 31, 2556–2570. [Google Scholar] [CrossRef]
- Sarkadi, A.; Kristiansson, R.; Oberklaid, F.; Bremberg, S. Fathers’ involvement and children’s developmental outcomes: A systematic review of longitudinal studies. Acta Paediatr. 2008, 97, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Stracke, M.; Heinzl, M.; Müller, A.D.; Gilbert, K.; Thorup, A.A.E.; Paul, J.L.; Christiansen, H. Mental Health Is a Family Affair-Systematic Review and Meta-Analysis on the Associations between Mental Health Problems in Parents and Children during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2023, 20, 4485. [Google Scholar] [CrossRef] [PubMed]
- Rudolf, M.; Eickhorst, A.; Doege, D.; Cierpka, M. Väter in den Frühen Hilfen–trotz Belastung Vertrauen in die eigenen Kompetenzen? Kindh. Entwickl. 2015, 24, 115–122. [Google Scholar] [CrossRef]
- Halme, N.; Tarkka, M.-T.; Nummi, T.; Astedt-Kurki, P. The Effect of Parenting Stress on Fathers’ Availability and Engagement. Child Care Pract. 2006, 12, 13–26. [Google Scholar] [CrossRef]
- Wittkowski, A.; Garrett, C.; Calam, R.; Weisberg, D. Self-Report Measures of Parental Self-Efficacy: A Systematic Review of the Current Literature. J. Child Fam. Stud. 2017, 26, 2960–2978. [Google Scholar] [CrossRef]
- Ardelt, M.; Eccles, J. Effects of Mothers’ Parental Efficacy Beliefs and Promotive Parenting Strategies on Inner-City Youth. J. Fam. Issues 2001, 22, 944–972. [Google Scholar] [CrossRef]
- Albanese, A.M.; Russo, G.R.; Geller, P.A. The role of parental self-efficacy in parent and child well-being: A systematic review of associated outcomes. Child Care Health Dev. 2019, 45, 333–363. [Google Scholar] [CrossRef]
- Carless, B.; Melvin, G.A.; Tonge, B.J.; Newman, L.K. The role of parental self-efficacy in adolescent school-refusal. J. Fam. Psychol. 2015, 29, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.L.; Prinz, R.J. Potential roles of parental self-efficacy in parent and child adjustment: A review. Clin. Psychol. Rev. 2005, 25, 341–363. [Google Scholar] [CrossRef] [PubMed]
- Murdock, K. An Examination of Parental Self-Efficacy Among Mothers and Fathers. Psychol. Men Masculinity 2013, 14, 314–323. [Google Scholar] [CrossRef]
- Sevigny, P.R.; Loutzenhiser, L. Predictors of parenting self-efficacy in mothers and fathers of toddlers. Child Care Health Dev. 2010, 36, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.Y.; Lim, S.A. Paternal self-efficacy, fathering, and children’s behavioral problems in Korea. J. Child Fam. Stud. 2019, 28, 851–859. [Google Scholar] [CrossRef]
- Lamb, M. How do fathers influence children’s development? Let me count the ways. In The Role of the Father in Child Development; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010; pp. 1–26. [Google Scholar]
- Darling, N.; Steinberg, L. Parenting Style as Context: An Integrative Model. Psychol. Bull. 1993, 113, 487–496. [Google Scholar] [CrossRef]
- Gil-Madrona, P.; Romero-Martínez, S.J.; Roz-Faraco, C.C. Extracurricular Physical Activities and the Condition of Being an Only Child as a Conditioning Factor in the Psychomotor Development of 5-Year-Old Children. Front. Pediatr. 2021, 9, 684418. [Google Scholar] [CrossRef]
- Belsky, J.; Robins, E.; Gamble, W. The Determinants of Parental Competence. In Beyond The Dyad; Lewis, M., Ed.; Springer: Boston, MA, USA, 1984; pp. 251–279. [Google Scholar]
- Reparaz, C.; Rivas, S.; Osorio, A.; Garcia-Zavala, G. A Parental Competence Scale: Dimensions and Their Association With Adolescent Outcomes. Front. Psychol. 2021, 12, 652884. [Google Scholar] [CrossRef]
- McBride, B.A. Stress and Fathers’ Parental Competence: Implications for Family Life and Parent Educators. Fam. Relat. 1989, 38, 385–389. [Google Scholar] [CrossRef]
- Garthus-Niegel, S.; Kittel-Schneider, S. Fathers and peripartum mental illness: The neglected parent? Nervenarzt 2023, 94, 779–785. [Google Scholar] [CrossRef]
- Fagan, J.; Barnett, M. The Relationship between Maternal Gatekeeping, Paternal Competence, Mothers’ Attitudes about the Father Role, and Father Involvement. J. Fam. Issues 2003, 24, 1020–1043. [Google Scholar] [CrossRef]
- Davison, K.K.; Charles, J.N.; Khandpur, N.; Nelson, T.J. Fathers’ Perceived Reasons for Their Underrepresentation in Child Health Research and Strategies to Increase Their Involvement. Matern. Child Health J. 2017, 21, 267–274. [Google Scholar] [CrossRef]
- Phares, V.; Lopez, E.; Fields, S.; Kamboukos, D.; Duhig, A.M. Are fathers involved in pediatric psychology research and treatment? J. Pediatr. Psychol. 2005, 30, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Petermann, U.; Petermann, F.; Franz, M. Erziehungskompetenz und Elterntraining. Kindh. Entwickl. 2010, 19, 67–71. [Google Scholar] [CrossRef]
- Lundahl, B.; Risser, H.J.; Lovejoy, M.C. A meta-analysis of parent training: Moderators and follow-up effects. Clin. Psychol. Rev. 2006, 26, 86–104. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Torres, L.P.; Alonso-Esteban, Y.; Alcantud-Marín, F. Early Intervention with Parents of Children with Autism Spectrum Disorders: A Review of Programs. Children 2020, 7, 294. [Google Scholar] [CrossRef]
- Blackman, A.L.; Jimenez-Gomez, C.; Shvarts, S. Comparison of the efficacy of online versus in-vivo behavior analytic training for parents of children with autism spectrum disorder. Behav. Anal. Res. Pract. 2020, 20, 13–23. [Google Scholar] [CrossRef]
- Zarakoviti, E.; Shafran, R.; Papadimitriou, D.; Bennett, S.D. The Efficacy of Parent Training Interventions for Disruptive Behavior Disorders in Treating Untargeted Comorbid Internalizing Symptoms in Children and Adolescents: A Systematic Review. Clin. Child Fam. Psychol. Rev. 2021, 24, 542–552. [Google Scholar] [CrossRef]
- Eyberg, S.; Bussing, R. Parent–Child Interaction Therapy for Preschool Children with Conduct Problems. In Clinical Handbook of Assessing and Treating Conduct Problems in Youth; Springer: Berlin/Heidelberg, Germany, 2010; pp. 139–162. [Google Scholar]
- Fabiano, G.A.; Pelham, W.E.; Cunningham, C.E.; Yu, J.; Gangloff, B.; Buck, M.; Linke, S.; Gormley, M.; Gera, S. A waitlist-controlled trial of behavioral parent training for fathers of children with ADHD. J. Clin. Child. Adolesc. Psychol. 2012, 41, 337–345. [Google Scholar] [CrossRef]
- Rojas, L.M.; Bahamon, M.; Lebron, C.; Montero-Zamora, P.; Pardo, M.; Wakefield, M.; Tapia, M.; Estrada, Y.; Schwartz, S.J.; Pantin, H. A Feasibility Trial of an Online-Only, Family-Centered Preventive Intervention for Hispanics: E-Familias Unidas. J. Prim. Prev. 2021, 42, 97–124. [Google Scholar] [CrossRef]
- Hudson, D.B.; Campbell-Grossman, C.; Fleck, M.O.; Elek, S.M.; Shipman, A. Effects of the New Fathers Network on first-time fathers’ parenting self-efficacy and parenting satisfaction during the transition to parenthood. Issues Compr. Pediatr. Nurs. 2003, 26, 217–229. [Google Scholar] [CrossRef] [PubMed]
- Mingebach, T.; Kamp-Becker, I.; Christiansen, H.; Weber, L. Meta-meta-analysis on the effectiveness of parent-based interventions for the treatment of child externalizing behavior problems. PLoS ONE 2018, 13, e0202855. [Google Scholar] [CrossRef] [PubMed]
- Schwenck, C.; Reichert, A. Plan E—Eltern Stark Machen! Modulares Training für Eltern von Psychisch Kranken Kindern und Jugendlichen. Mit Online-Materialien; Beltz: Weinheim, Germany, 2012. [Google Scholar]
- Achenbach, T.M. Child Behavior Checklist. In Encyclopedia of Clinical Neuropsychology; Kreutzer, J.S., DeLuca, J., Caplan, B., Eds.; Springer: New York, NY, USA, 2011; pp. 546–552. [Google Scholar]
- Döpfner, M.; Plück, J.; Kinnen, C. CBCL/6-18R, TRF/6-18R, YSR/11-18R: Deutsche Schulalter-Formen der Child Behavior Checklist von Thomas M. Achenbach; Hogrefe: Göttingen, Germany, 2014. [Google Scholar]
- Abidin, R.R. Parenting Stress Index: Manual, 3rd ed.; Psychological Assessment Resources: Lutz, FL, USA, 1995. [Google Scholar]
- Kliem, S.; Kessemeier, Y.; Heinrichs, N.; Döpfner, M.; Hahlweg, K. Der Fragebogen zur Selbstwirksamkeit in der Erziehung (FSW). Diagnostica 2014, 60, 35–45. [Google Scholar] [CrossRef]
- Titze, K.; Lehmkuhl, U. Elternbildfragebogen für Kinder und Jugendliche (EBF-KJ). Diagnostica 2010, 56, 2. [Google Scholar] [CrossRef]
- Tröster, H. Eltern-Belastungs-Inventar (EBI), Deutsche Version des Parenting Stress Index (PSI) von R. R. Abidin; Hogrefe: Göttingen, Germany, 2011. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; revised ed.; Lawrence Erlbaum Associates, Inc.: Hillsdale, NJ, USA, 1977. [Google Scholar]
- Serdar, C.C.; Cihan, M.; Yücel, D.; Serdar, M.A. Sample size, power and effect size revisited: Simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Med. 2021, 31, 010502. [Google Scholar] [CrossRef] [PubMed]
- Lechowicz, M.; Jiang, Y.; Tully, L.; Burn, M.; Collins, D.; Hawes, D.; Lenroot, R.; Anderson, V.; Doyle, F.; Piotrowska, P.; et al. Enhancing Father Engagement in Parenting Programs: Translating Research into Practice Recommendations. Aust. Psychol. 2019, 54, 83–89. [Google Scholar] [CrossRef]
- Quetsch, L.B.; Girard, E.I.; McNeil, C.B. The impact of incentives on treatment adherence and attrition: A randomized controlled trial of Parent-Child Interaction Therapy with a primarily Latinx, low-income population. Child. Youth Serv. Rev. 2020, 112, 104886. [Google Scholar] [CrossRef]
- Tully, L.A.; Collins, D.A.J.; Piotrowska, P.J.; Mairet, K.S.; Hawes, D.J.; Moul, C.; Lenroot, R.K.; Frick, P.J.; Anderson, V.A.; Kimonis, E.R.; et al. Examining Practitioner Competencies, Organizational Support and Barriers to Engaging Fathers in Parenting Interventions. Child Psychiatry Hum. Dev. 2018, 49, 109–122. [Google Scholar] [CrossRef]
- Niec, L.N.; Barnett, M.L.; Gering, C.L.; Triemstra, K.; Solomon, D.T. Differences in mothers’ and fathers’ readiness for change in parent training. Child Fam. Behav. Ther. 2015, 37, 224–235. [Google Scholar] [CrossRef]
- Tiano, J.D.; Grate, R.M.; McNeil, C.B. Comparison of mothers’ and fathers’ opinions of parent–child interaction therapy. Child Fam. Behav. Ther. 2013, 35, 110–131. [Google Scholar] [CrossRef]
- Addis, M.E.; Mahalik, J.R. Men, masculinity, and the contexts of help seeking. Am. Psychol. 2003, 58, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Burgdorf, V.; Szabó, M.; Abbott, M.J. The Effect of Mindfulness Interventions for Parents on Parenting Stress and Youth Psychological Outcomes: A Systematic Review and Meta-Analysis. Front. Psychol. 2019, 10, 1336. [Google Scholar] [CrossRef] [PubMed]
- Theule, J.; Cheung, K.; Aberdeen, K. Children’s ADHD Interventions and Parenting Stress: A Meta-Analysis. J. Child Fam. Stud. 2018, 27, 2744–2756. [Google Scholar] [CrossRef]
- Cooley, M.; Veldorale-Griffin, A.; Petren, R.; Mullis, A. Parent–Child Interaction Therapy: A Meta-Analysis of Child Behavior Outcomes and Parent Stress. J. Fam. Social. Work. 2014, 17, 191. [Google Scholar] [CrossRef]
- Curley, K.; Colman, R.; Rushforth, A.; Kotera, Y. Stress Reduction Interventions for Parents of Children with Autism Spectrum Disorder: A Focused Literature Review. Youth 2023, 3, 246–260. [Google Scholar] [CrossRef]
- Tarver, J.; Palmer, M.; Webb, S.; Scott, S.; Slonims, V.; Simonoff, E.; Charman, T. Child and parent outcomes following parent interventions for child emotional and behavioral problems in autism spectrum disorders: A systematic review and meta-analysis. Autism 2019, 23, 1630–1644. [Google Scholar] [CrossRef] [PubMed]
- Farley, R.; de Diaz, N.A.N.; Emerson, L.M.; Simcock, G.; Donovan, C.; Farrell, L.J. Mindful Parenting Group Intervention for Parents of Children with Anxiety Disorders. Child Psychiatry Human Dev. 2023. [Google Scholar] [CrossRef]
- Chien, W.T.; Norman, I. The effectiveness and active ingredients of mutual support groups for family caregivers of people with psychotic disorders: A literature review. Int. J. Nurs. Stud. 2009, 46, 1604–1623. [Google Scholar] [CrossRef]
- Neece, C.L.; Green, S.A.; Baker, B.L. Parenting stress and child behavior problems: A transactional relationship across time. Am. J. Intellect. Dev. Disabil. 2012, 117, 48–66. [Google Scholar] [CrossRef]
- May, F.S.; McLean, L.A.; Anderson, A.; Hudson, A.; Cameron, C.; Matthews, J. Father participation with mothers in the Signposts program: An initial investigation. J. Intellect. Dev. Disabil. 2013, 38, 39–47. [Google Scholar] [CrossRef]
- Lundahl, B.W.; Tollefson, D.; Risser, H.; Lovejoy, M.C. A Meta-Analysis of Father Involvement in Parent Training. Res. Soc. Work. Pract. 2008, 18, 97–106. [Google Scholar] [CrossRef]
- Cowan, P.A.; Cowan, C.P.; Pruett, M.K.; Pruett, K.; Wong, J.J.; LaRossa, R. Promoting Fathers’ Engagement with Children: Preventive Interventions for Low-Income Families. J. Marriage Fam. 2009, 71, 663–679. [Google Scholar] [CrossRef]
- Schlack, R.; Petermann, F. Prevalence and gender patterns of mental health problems in German youth with experience of violence: The KiGGS study. BMC Public Health 2013, 13, 628. [Google Scholar] [CrossRef] [PubMed]
- Salonen, A.H.; Kaunonen, M.; Astedt-Kurki, P.; Järvenpää, A.L.; Isoaho, H.; Tarkka, M.T. Effectiveness of an internet-based intervention enhancing Finnish parents’ parenting satisfaction and parenting self-efficacy during the postpartum period. Midwifery 2011, 27, 832–841. [Google Scholar] [CrossRef] [PubMed]
- Wittkowski, A.; Dowling, H.; Smith, D.M. Does Engaging in a Group-Based Intervention Increase Parental Self-efficacy in Parents of Preschool Children? A Systematic Review of the Current Literature. J. Child Fam. Stud. 2016, 25, 3173–3191. [Google Scholar] [CrossRef]
- Boyraz, G.; Sayger, T.V. Psychological Well-Being Among Fathers of Children With and Without Disabilities: The Role of Family Cohesion, Adaptability, and Paternal Self-Efficacy. Am. J. Men’s Health 2010, 5, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M.; Gerke, D.-C. Associations of Parenting Styles with Self-Esteem in Children and Adolescents: A Meta-Analysis. J. Child Fam. Stud. 2019, 28, 2017–2035. [Google Scholar] [CrossRef]
- Trahan, M. Paternal Self-Efficacy and Father Involvement: A Bi-Directional Relationship. Psychol. Men Masculinity 2017, 19, 624. [Google Scholar] [CrossRef]
- Mascaro, J.S.; Rentscher, K.E.; Hackett, P.D.; Mehl, M.R.; Rilling, J.K. Child gender influences paternal behavior, language, and brain function. Behav. Neurosci. 2017, 131, 262–273. [Google Scholar] [CrossRef]
- Trautmann-Villalba, P.; Laucht, M.; Schmidt, M. Interaktion zwischen Kleinkindern und ihren Vätern. Monatsschrift Kinderheilkd. 2003, 151, 613–620. [Google Scholar] [CrossRef]
- Meunier, J.-C.; Roskam, I.; Browne, D. Relations between parenting and child behavior: Exploring the child’s personality and parental self-efficacy as third variables. Int. J. Behav. Dev. 2011, 35, 246–259. [Google Scholar] [CrossRef]
- Ruiz-Zaldibar, C.; Serrano-Monzó, I.; Mujika, A. Parental competence programs to promote positive parenting and healthy lifestyles in children: A systematic review. J. Pediatr. 2018, 94, 238–250. [Google Scholar] [CrossRef] [PubMed]
- Titze, K.; Schenck, S.; Zulauf-Logoz, M.; Lehmkuhl, U. Assessing the Quality of the Parent–Child Relationship: Validity and Reliability of the Child–Parent Relationship Test (ChiP-C). J. Child Fam. Stud. 2014, 23, 917–933. [Google Scholar] [CrossRef]
- Kraemer, H.C.; Mintz, J.; Noda, A.; Tinklenberg, J.; Yesavage, J.A. Caution regarding the use of pilot studies to guide power calculations for study proposals. Arch. Gen. Psychiatry 2006, 63, 484–489. [Google Scholar] [CrossRef]
- MacKinnon, A.L.; Silang, K.; Penner, K.; Zalewski, M.; Tomfohr-Madsen, L.; Roos, L.E. Promoting Mental Health in Parents of Young Children Using eHealth Interventions: A Systematic Review and Meta-analysis. Clin. Child Fam. Psychol. Rev. 2022, 25, 413–434. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Cohort 1 (Presence, n = 8) | Cohort 2 (Online, n = 8) | ||||
|---|---|---|---|---|---|
| M/N (SD/%) | t (df)/χ2 (df) | p | |||
| Fathers | |||||
| Age [y] | 51.0 (5.3) | 48.4 (7.2) | 0.83 (14) | 0.42 | |
| Years of school attendance | ≥12 <12 | 5 (62.5) 3 (37.5) | 5 (62.5) 3 (37.5) | ||
| Single-parent raising | 0 (0) | 0 (0) | 0 | - | |
| Current partnership | yes no | 6 (75.0) 2 (25.0) | 8 (100.0) 0 (0) | 2.29 (1) | 0.13 |
| Number of children | 1 2 3 4 | 0 (0) 6 (75) 1 (12.5) 1 (12.5) | 1(12.5) 2 (25.0) 4 (50.0) 1 (12.5) | 4.8 (3) | 0.19 |
| Children | |||||
| Age [y] | 14.3 (1.9) | 15.1 (2.5) | −0.79 (14) | 0.44 | |
| Sex | Female Male | 5 (62.5) 3 (37.5) | 7 (87.5) 1 (12.5) | 1.33 (1) | 0.25 |
| Treatment setting | Inpatient Daily-care | 7 (87.5) 1 (12.5) | 7 (87.5) 1 (12.5) | 0.00 (1) 0.00 (1) | 1.00 1.00 |
| In-Person Cohort | Online Cohort | ||||||
|---|---|---|---|---|---|---|---|
| M (SD) | T ≥ 64 | M (SD) | T ≥ 64 | t (df) | |d| | p | |
| n(%) | n(%) | ||||||
| Father rating | n = 5 | n = 4 | |||||
| Internalizing | 66.60 (10.02) | 3 (60) | 70.00 (7.35) | 3 (75) | −0.57 (7) | 0.40 | 0.590 |
| Externalizing | 57.80 (11.03) | 1 (20) | 53.25 (6.40) | 0 (0) | 0.73 (7) | 0.50 | 0.491 |
| Total Problems | 63.60 (13.16) | 2 (40) | 62.00 (6.33) | 2 (50) | 0.22 (7) | 0.16 | 0.831 |
| Offspring rating | n = 8 | n = 5 | |||||
| Internalizing | 71.88 (3.83) | 8 (100) | 78.60 (12.46) | 5 (100) | −1.17 (11) | 0.79 | 0.300 |
| Externalizing | 50.13 (10.11) | 0 (0) | 51.00 (2.55) | 0 (0) | −0.19 (11) | 0.11 | 0.855 |
| Total Problems | 65.00 (4.31) | 6 (75) | 66.20 (8.08) | 3 (60) | −0.35 (11) | 0.21 | 0.731 |
| Pre-Intervention (t1) | Post-Intervention (t2) | ||||
|---|---|---|---|---|---|
| M (SD) | M (SD) | t (df) | |d| | p | |
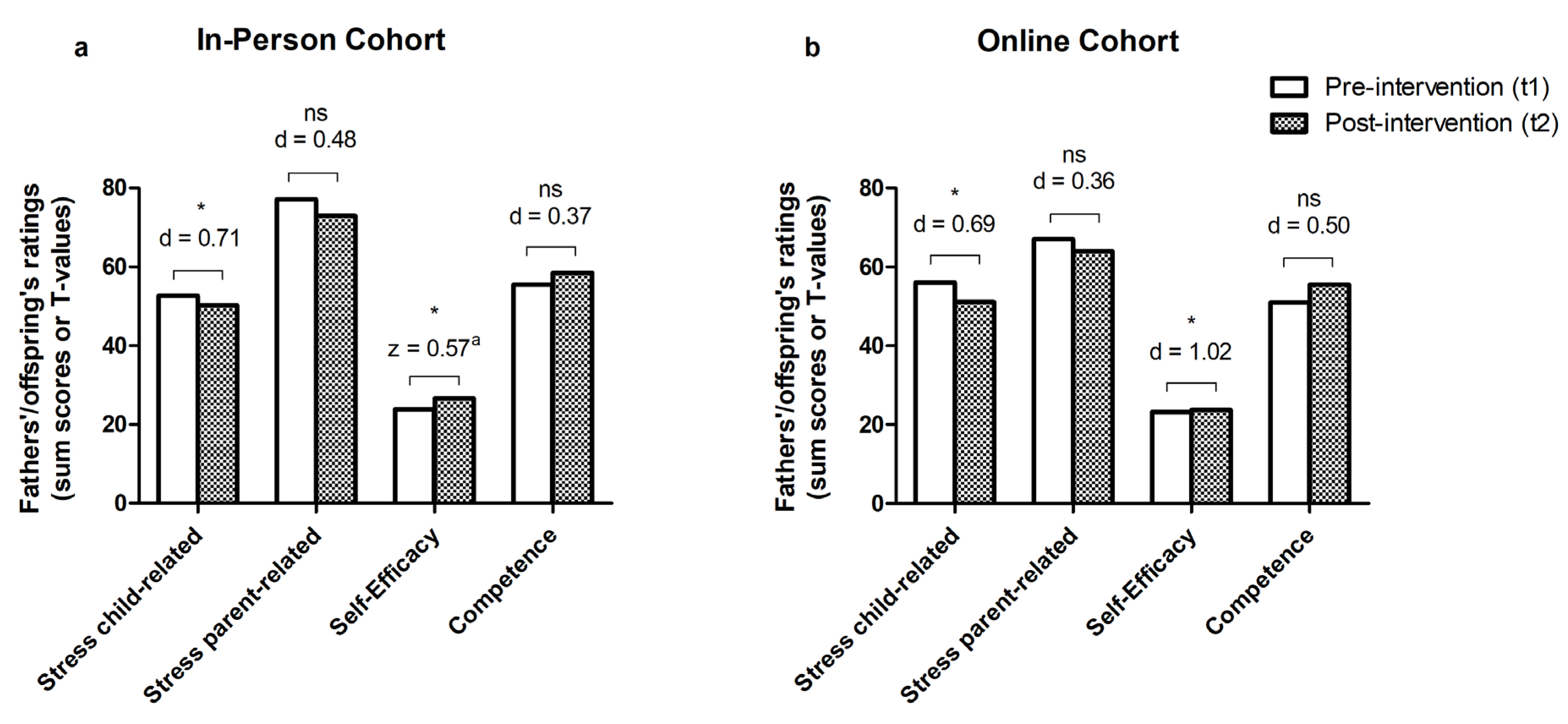
| In-person cohort Paternal | |||||
| Stress child-related | 52.63 (20.47) | 50.25 (18.34) | 2.01 (7) | 0.71 | 0.042 |
| Stress parent-related | 77.13 (25.81) | 72.88 (27.59) | 1.36 (7) | 0.48 | 0.108 |
| Self-efficacy | 23.88 (5.16) | 26.63 (4.47) | −2.56 | 0.57 a | 0.006 |
| Competence | 55.50 (12.88) | 58.50 (14.00) | −1.04 (7) | 0.37 | 0.167 |
| Online cohort Paternal | |||||
| Stress child-related | 56.00 (10.85) | 51.13 (12.12) | 1.94 (7) | 0.69 | 0.047 |
| Stress parent-related | 67.00 (14.80) | 64.00 (16.91) | 1.02 (7) | 0.36 | 0.171 |
| Self-efficacy | 23.25 (3.77) | 25.75 (3.15) | −2.89 (7) | 1.02 | 0.012 |
| Competence | 51.00 (11.19) | 55.50 (17.23) | −1.41 (7) | 0.50 | 0.101 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mestermann, S.; Kleinöder, J.M.; Arndt, M.; Krämer, J.; Eichler, A.; Kratz, O. The Father’s Part: A Pilot Evaluation of a Father-Centered Family Intervention Group in Child and Adolescent Psychiatry. Behav. Sci. 2024, 14, 13. https://doi.org/10.3390/bs14010013
Mestermann S, Kleinöder JM, Arndt M, Krämer J, Eichler A, Kratz O. The Father’s Part: A Pilot Evaluation of a Father-Centered Family Intervention Group in Child and Adolescent Psychiatry. Behavioral Sciences. 2024; 14(1):13. https://doi.org/10.3390/bs14010013
Chicago/Turabian StyleMestermann, Stefan, Jonas Markus Kleinöder, Marie Arndt, Josef Krämer, Anna Eichler, and Oliver Kratz. 2024. "The Father’s Part: A Pilot Evaluation of a Father-Centered Family Intervention Group in Child and Adolescent Psychiatry" Behavioral Sciences 14, no. 1: 13. https://doi.org/10.3390/bs14010013
APA StyleMestermann, S., Kleinöder, J. M., Arndt, M., Krämer, J., Eichler, A., & Kratz, O. (2024). The Father’s Part: A Pilot Evaluation of a Father-Centered Family Intervention Group in Child and Adolescent Psychiatry. Behavioral Sciences, 14(1), 13. https://doi.org/10.3390/bs14010013