
The Development of a Pilot App Targeting Short-Term and Prospective Memory in People Diagnosed with Dementia


Abstract
:1. Introduction
2. Literature Review on Computerized Memory Assisting Technologies
2.1. Studies Employing Computer-Based Technology as a Means of Intervention in Healthy Older Adults
2.2. Studies Employing Computer-Based Technology as a Means of Intervention and Rehabilitation of Patients with Dementia
2.3. Studies Based on Errorless Learning
2.3.1. Errorless Learning in Healthy Older Adults
2.3.2. Errorless Learning and Dementia
2.4. Studies on Prospective Memory (PM) through Technological Applications
2.4.1. Prospective Memory and Healthy Older Subjects
2.4.2. Prospective Memory: Comparison of Healthy Subjects and Subjects with Dementia
3. Materials and Methods
3.1. Participants
Participants Recruitment
3.2. Initial Assessment—Screening Tools
3.3. Experimental Design
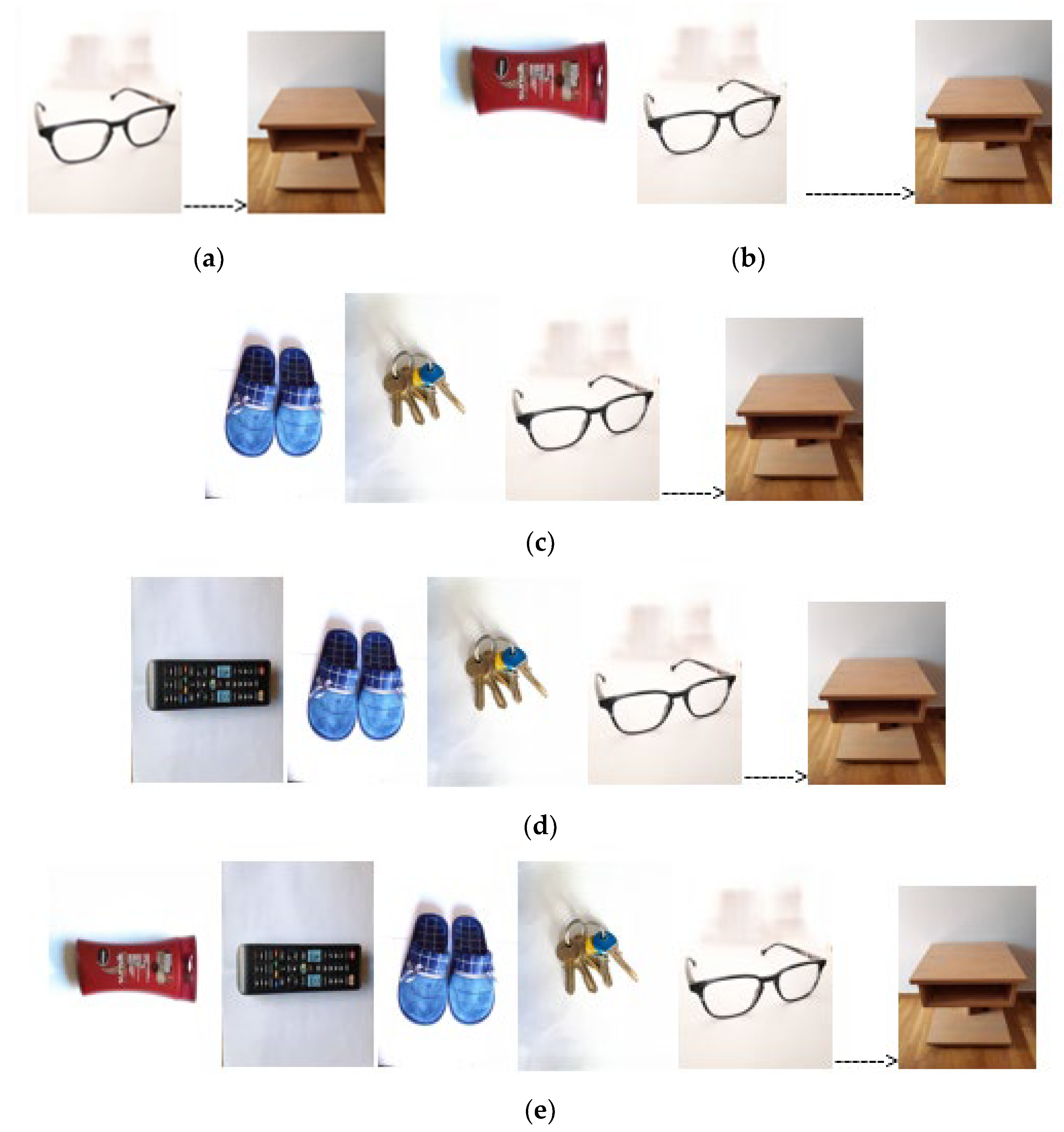
3.3.1. Task 1 Short-Term Memory—Stimuli and Procedure
3.3.2. Task 2 Prospective Memory—Stimuli and Procedure
3.4. Statistical Methods
4. Results
5. Discussion
Limitations
6. Conclusions
7. Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Dementia. Available online: https://www.who.int/health-topics/dementia (accessed on 7 July 2023).
- Klimova, B. Computer-based cognitive training in aging. Front. Aging Neurosci. 2016, 8, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kalaria, R.N.; Maestre, G.E.; Arizaga, R.; Friedland, R.P.; Galasko, D.; Hall, K.; Luchsinger, J.A.; Ogunniyi, A.; Perry, E.K.; Potocnik, F.; et al. Alzheimer’s disease and vascular dementia in developing countries: Prevalence, management, and risk factors. Lancet. Neurol. 2008, 7, 812–826. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.C.; Wu, Y.T.; Prina, M. World Alzheimer Report 2015—The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International (ADI): London, UK, 2015. [Google Scholar]
- Salthouse, T.A. When does age-related cognitive decline begin? Neurobiol. Aging. 2009, 30, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Duncan, J.; Chylinski, D.; Mitchell, D.J.; Bhandari, A. Complexity and compositionality in fluid intelligence. Proc. Natl. Acad. Sci. USA 2017, 114, 5295–5299. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T.A.; Babcock, R.L. Decomposing adult age differences in working memory. Develop. Psychol. 1991, 27, 763–776. [Google Scholar] [CrossRef]
- Jorge, A.; Magalhães, R.; Machado, A.; Gonçalves, O.F.; Sampaio, A.; Petrosyan, A. Non-pharmacological cognitive intervention for aging and dementia: Current perspectives. World J. Clin. Cases. 2013, 1, 233–241. [Google Scholar] [CrossRef]
- Hartshorne, J.K.; Germine, L.T. When does cognitive functioning peak? The asynchronous rise and fall of different cognitive abilities across the life span. Psychol. Sci. 2015, 26, 433–443. [Google Scholar] [CrossRef]
- Cattell, R.B. The measurement of adult intelligence. Psychol. Bulletin. 1943, 40, 153–193. [Google Scholar] [CrossRef]
- Wechsler, D. The Measurement of Adult Intelligence, 3rd ed.; Williams & Wilkins Co.: Baltimore, MD, USA, 1944. [Google Scholar] [CrossRef]
- Wechsler, D. WAIS-3, WMS-3: Wechsler Adult Intelligence Scale, Wechsler Memory Scale: Technical Manual; The Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar] [CrossRef]
- McDonough, I.M.; Bischof, G.N.; Kennedy, K.M.; Rodrigue, K.M.; Farrell, M.E.; Park, D.C. Discrepancies between fluid and crystallized ability in healthy adults: A behavioral marker of preclinical Alzheimer’s disease. Neurobiol. Aging 2016, 46, 68–75. [Google Scholar] [CrossRef]
- King, D.L.O.; Henson, R.N.; Kievit, R.; Wolpe, N.; Brayne, C.; Tyler, L.K.; Rowe, J.B.; Cam-CAN; Tsvetanov, K.A. Distinct components of cardiovascular health are linked with age-related differences in cognitive abilities. Sci. Rep. 2023, 13, 978. [Google Scholar] [CrossRef]
- Schubert, A.L.; Hagemann, D.; Löffler, C.; Frischkorn, G.T. Disentangling the effects of processing speed on the association between age differences and fluid intelligence. J. Intell. 2019, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Cadar, D. Cognitive ageing. In Geriatrics Health; Çakmur, H., Ed.; IntechOpen: London, UK, 2018; pp. 49–65. [Google Scholar]
- Mitchell, D.J.; Mousley, A.L.S.; Shafto, M.A.; Duncan, J. Neural contributions to reduced fluid intelligence across the adult lifespan. J. Neurosci. 2023, 43, 293–307. [Google Scholar] [CrossRef] [PubMed]
- Cabeza, R.; Grady, C.L.; Nyberg, L.; McIntosh, A.R.; Tulving, E.; Kapur, S. Age-related differences in neural activity during memory encoding and retrieval: A positron emission tomography study. J. Neurosci. 1997, 17, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Cabeza, R.; Anderson, N.D.; Houle, S.; Mangels, J.A.; Nyberg, L. Age-Related Differences in Neural Activity during Item and Temporal-Order Memory Retrieval: A Positron Emission Tomography Study. J. Cogn. Neurosci. 2020, 12, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Rosen, H.J.; Gorno–Tempini, M.L.; Goldman, W.P.; Perry, R.J.; Schuff, N.; Weiner, M.; Feiwell, R.; Kramer, J.H.; Miller, B.L. Patterns of brain atrophy in frontotemporal dementia and semantic dementia. Neurology 2002, 58, 198–208. [Google Scholar] [CrossRef]
- Gutchess, A.H.; Welsh, R.C.; Hedden, T.; Bangert, A.; Minear, M.; Liu, L.L.; Park, D.C. Aging and the Neural Correlates of Successful Picture Encoding: Frontal Activations Compensate for Decreased Medial-Temporal Activity. J. Cogn. Neurosci. 2005, 17, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Dennis, N.A.; Hayes, S.M.; Prince, S.E.; Madden, D.J.; Huettel, S.A.; Cabeza, R. Effects of aging on the neural correlates of successful item and source memory encoding. J. Exp. Psychol. Learn. Mem. Cogn. 2008, 34, 791–808. [Google Scholar] [CrossRef]
- Tucker-Drob, E.M.; de la Fuente, J.; Köhncke, Y.; Brandmaier, A.M.; Nyberg, L.; Lindenberger, U. A strong dependency between changes in fluid and crystallized abilities in human cognitive aging. Sci. Adv. 2022, 8, eabj2422. [Google Scholar] [CrossRef]
- Matsuda, O.; Saito, M. Crystallized and fluid intelligence in elderly patients with mild dementia of the Alzheimer type. Int. Psychogeriatr. 1998, 10, 147–154. [Google Scholar] [CrossRef]
- Matsuda, O.; Saito, M.; Kato, M.; Azami, H.; Shido, E. Wechsler Adult Intelligence Scale-III profile in the early stages of Alzheimer’s disease: Performance in subtests sensitive to and resistant to normal decline with ageing. Psychogeriatrics 2015, 15, 1–6. [Google Scholar] [CrossRef]
- Schmid, N.S.; Taylor, K.I.; Foldi, N.S.; Berres, M.; Monsch, A.U. Neuropsychological signs of Alzheimer’s disease 8 years prior to diagnosis. J. Alzheimer’s Dis. 2013, 34, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Saddichha, S.; Pandey, V. Alzheimer’s and non-Alzheimer’s dementia: A critical review of pharmacological and nonpharmacological strategies. J. Alzheimer’s Dis. Other Dement. 2008, 23, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Canu, E.; Sarasso, E.; Filippi, M.; Agosta, F. Effects of pharmacological and nonpharmacological treatments on brain functional magnetic resonance imaging in Alzheimer’s disease and mild cognitive impairment: A critical review. Alzheimer’s Res. Ther. 2018, 10, 1–26. [Google Scholar] [CrossRef]
- Meyer, C.; O’Keefe, F. Non-pharmacological interventions for people with dementia: A review of reviews. Dementia 2020, 19, 1927–1954. [Google Scholar] [CrossRef]
- Burley, C.V.; Burns, K.; Brodaty, H. Pharmacological and nonpharmacological approaches to reduce disinhibited behaviors in dementia: A systematic review. Int. Psychogeriatr. 2022, 34, 335–351. [Google Scholar] [CrossRef]
- Berg-Weger, M.; Stewart, D.B. Non-pharmacologic interventions for persons with dementia. Mol. Med. 2017, 114, 116–119. [Google Scholar]
- Zucchella, C.; Sinforiani, E.; Tamburin, S.; Federico, A.; Mantovani, E.; Bernini, S.; Casale, R.; Bartolo, M. The multidisciplinary approach to Alzheimer’s disease and dementia. A narrative review of non-pharmacological treatment. Front. Neurol. 2018, 9, 1058. [Google Scholar] [CrossRef]
- Cammisuli, D.M.; Danti, S.; Bosinelli, F.; Cipriani, G. Non-pharmacological interventions for people with Alzheimer’s Disease: A critical review of the scientific literature from the last ten years. Eur. Ger. Med. 2016, 7, 57–64. [Google Scholar] [CrossRef]
- Valenzuela, M.J. Brain reserve and the prevention of dementia. Curr. Opin. Psychiatry 2008, 21, 296–302. [Google Scholar] [CrossRef]
- Chaldogeridis, A.; Tsiatsos, T.; Gialaouzidis, M.; Tsolaki, M. Comparing data from a computer based intervention program for patients with Alzheimer’s disease. In Virtual, Augmented and Mixed Reality, Applications of Virtual and Augmented Reality, Proceedings of the 6th International Conference, VAMR 2014, Crete, Greece, 22–27 June 2014; Springer: Cham, Switzerland, 2014; pp. 258–266. [Google Scholar] [CrossRef]
- Rute-Pérez, S.; Rodríguez-Domínguez, C.; Vélez-Coto, M.; Pérez-García, M.; Caracuel, A. Effectiveness of Computerized Cognitive Training by VIRTRAEL on Memory and Executive Function in Older People: A Pilot Study. Brain Sci. 2023, 13, 684. [Google Scholar] [CrossRef]
- Huppert, F.A.; Beardsall, L. Prospective memory impairment as an early indicator of dementia. J. Clin. Exp. Neuropsychol. 1993, 15, 805–821. [Google Scholar] [CrossRef]
- Maylor, E.A.; Smith, G.; Sala, S.D.; Logie, R.H. Prospective and retrospective memory in normal aging and dementia: An experimental study. Mem. Cogn. 2002, 30, 871–884. [Google Scholar] [CrossRef]
- Thompson, C.; Henry, J.D.; Rendell, P.G.; Withall, A.; Broadaty, H. Prospective memory function in mild cognitive impairment and early dementia. J. Int. Neuropsychol. Soc. 2010, 16, 318–325. [Google Scholar] [CrossRef]
- Lecouvey, G.; Morand, A.; Gonneaud, J.; Piolino, P.; Orriols, E.; Pélerin, A.; Desgranges, B. An impairment of prospective memory in mild Alzheimer’s disease: A ride in a virtual town. Front. Psychol. 2019, 10, 241. [Google Scholar] [CrossRef] [PubMed]
- Clare, L.; Wilson, B.A.; Carter, G.; Breen, K.; Gosses, A.; Hodges, J.R. Intervening with everyday memory problems in dementia of Alzheimer type: An errorless learning approach. J. Clin. Exp. Neuropsychol. 2000, 22, 132–146. [Google Scholar] [CrossRef] [PubMed]
- Clare, L.; Linden, D.E.J.; Woods, R.T.; Whitaker, R.; Evans, S.J.; Parkinson, C.H.; van Paasschen, J.; Nelis, S.M.; Hoare, Z.; Yuen, K.S.L.; et al. Goal-oriented cognitive rehabilitation for people with early-stage Alzheimer disease: A single-blind randomized controlled trial of clinical efficacy. Am. J. Geriatr. Psychiatry 2010, 18, 928–939. [Google Scholar] [CrossRef] [PubMed]
- Jokel, R.; Rochon, E.; Anderson, N.D. Errorless learning of computer-generated words in a patient with semantic dementia. Neuropsychol. Rehabil. 2010, 20, 16–41. [Google Scholar] [CrossRef]
- Ball, K.; Beerch, D.; Jobe, J.B. Effects of Cognitive Training Interventions with Older Adults: A Randomized Controlled Trial. JAMA 2002, 288, 2271–2281. [Google Scholar] [CrossRef]
- Willis, S.L.; Tennstedt, S.L.; Marsiske, M.P.; Ball, K.; Elias, J.; Koepke, K.M.; Morris, J.N.; Rebok, G.W.; Unverzagt, F.W.; Stoddard, A.M.; et al. Long-term Effects of Cognitive Training on Everyday Functional Outcomes in Older Adults. JAMA 2006, 296, 2805–2814. [Google Scholar] [CrossRef]
- Gates, N.; Valenzuela, M. Cognitive Exercise and Its Role in Cognitive Function in Older Adults. Curr. Psychiatry Rep. 2010, 12, 20–27. [Google Scholar] [CrossRef]
- Smart, C.M.; Karr, J.E.; Areshenkoff, C.N.; Rabin, L.A.; Hudon, C.; Gates, N.; Ali, J.I.; Arenaza-Urquijo, E.M.; Buckley, R.F.; Chetelat, G.; et al. Non-Pharmacologic Interventions for Older Adults with Subjective Cognitive Decline: Systematic Review, Meta-Analysis, and Preliminary Recommendations. Neuropsychol. Rev. 2017, 27, 245–257. [Google Scholar] [CrossRef]
- Lustig, C.; Shah, P.; Seidler, R.; Reuter-Lorenz, P.A. Aging, training, and the brain: A review and future directions. Neuropsychol. Rev. 2009, 19, 504–522. [Google Scholar] [CrossRef]
- Shao, Y.; Mang, J.; Li, P.L.; Wang, J.; Deng, T.; Xu, Z.X. Computer-Based Cognitive Programs for Improvement of Memory, Processing Speed and Executive Function during Age-Related Cognitive Decline: A Meta-Analysis. PLoS ONE 2015, 10, e0130831. [Google Scholar] [CrossRef] [PubMed]
- Hill, N.T.; Mowszowski, L.; Naismith, S.L.; Chadwick, V.L.; Valenzuela, M.; Lampit, A. Computerized cognitive training in older adults with mild cognitive impairment or dementia: A systematic review and meta-analysis. Am. J. Psychiatry 2017, 174, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Gavelin, H.M.; Lampit, A.; Hallock, H.; Sabatés, J.; Bahar-Fuchs, A. Cognition-Oriented Treatments for Older Adults: A Systematic Overview of Systematic Reviews. Neuropsychol. Rev. 2020, 30, 167–193. [Google Scholar] [CrossRef] [PubMed]
- Lampit, A.; Hallock, H.; Suo, C.; Naismith, S.L.; Valenzuela, M. Cognitive training-induced short-term functional and long-term structural plastic change is related to gains in global cognition in healthy older adults: A pilot study. Front. Aging Neurosci. 2015, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.; Hock, C.; Muller-Spahn, F. Computer-based Cognitive Training in Alzheimer’s Disease Patients. Ann. N. Y. Acad. Sci. 1996, 777, 249–254. [Google Scholar] [CrossRef]
- Schreiber, M.; Schweizer, A.; Lutz, K.; Kalveram, K.T.; Jäncke, L. Potential of an interactive computer-based training in the rehabilitation of dementia: An initial study. Neuropsychol. Rehabil. 1999, 9, 155–167. [Google Scholar] [CrossRef]
- Cipriani, G.; Bianchetti, A.; Trabucchi, M. Outcomes of a computer-based cognitive rehabilitation program on Alzheimer’s disease patients compared with those on patients affected by mild cognitive impairment. Arch. Gerontol. Geriatr. 2006, 43, 327–335. [Google Scholar] [CrossRef]
- Talassi, E.; Guerrecshi, M.; Feriani, M.; Fedi, V.; Bianchetti, A.; Trabucchi, M. Effectiveness of a cognitive rehabilitation program in mild dementia (MD) and mild cognitive impairment (MCI): A case control study. Arch. Gerontol. Geriatr. 2007, 44, 391–399. [Google Scholar] [CrossRef]
- Vaportzis, E.; Martin, M.; Gow, A.J. A Tablet for Healthy Ageing: The Effect of a Tablet Computer Training Intervention on Cognitive Abilities in Older Adults. Am. J. Geriatr. Psychiatry 2016, 25, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Kwak, Y.T. Improvement of cognitive function after computer-based cognitive training in early stage of Alzheimer’s dementia. Dement. Neurocogn. Disord. 2017, 16, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Kallio, E.L.; Öhman, H.; Kautiainen, H.; Hietanen, M.; Pitkälä, K. Cognitive training interventions for patients with Alzheimer’s disease: A systematic review. J. Alzheimers Dis. 2017, 56, 1349–1372. [Google Scholar] [CrossRef]
- Oh, S.J.; Ryu, J.N. The effect of brain-computer interface-based cognitive training in patients with dementia. J. Korean Soc. Phys. Med. 2018, 13, 59–65. [Google Scholar] [CrossRef]
- Kang, M.J.; Kim, S.M.; Han, S.E.; Bae, J.H.; Yu, W.J.; Park, M.Y.; Ku, S.; Yang, Y.S. Effect of Paper-Based Cognitive Training in Early Stage of Alzheimer’s Dementia. Dement. Neurocogn. Disord. 2019, 18, 62–68. [Google Scholar] [CrossRef]
- Polat, B.S.A.; Sarılar, A.C. The effects of computer-based cognitive training program on reaction times of patients with early stage Alzheimer’s disease and traumatic brain injury: Cognitive Training in TBI and AD. Med. Sci. Disc. 2002, 9, 107–111. [Google Scholar] [CrossRef]
- Fabian, C.G.; Chang, E.C. Where do we go from here? Future directions, challenges, and considerations. In Handbook of Adult Psychopathology in Asians: Theory, Diagnosis, and Treatment, 1st ed.; Chang, E.C., Ed.; Oxford University Press: Oxford, UK, 2012; pp. 435–446. [Google Scholar]
- Loi, S.M.; Mazur, A.; Huppert, D.; Hoy, B.; Swan, J.; Lautenschlager, T. A pilot study using “apps” as a novel strategy for the management of challenging behaviors seen in people living in residential care. Int. Psychogeriatr. 2016, 29, 1–7. [Google Scholar] [CrossRef]
- Tak, S.H.; Zhang, H.; Patel, H.; Hong, S.H. Computer Activities for Persons with Dementia. Gerontologists 2015, 55, 40–49. [Google Scholar] [CrossRef]
- Kerkhof, Y.J.F.; Graff, M.J.L.; Bergsma, A.; de Vocht, H.H.M.; Dröes, R.M. Better self-management and meaningful activities thanks to tablets? Development of a person-centered program to support people with mild dementia and their carers through use of hand-held touch screen devices. Int. Psychogeriatr. 2016, 28, 1917–1929. [Google Scholar] [CrossRef]
- Maresova, P.; Klimova, B. Supporting Technologies for Old People with Dementia: A Review. IFAC-Pap. Line 2015, 48, 129–134. [Google Scholar] [CrossRef]
- Dethlefs, N.; Milders, M.; Cuayáhuitl, H.; Al-Salkini, T.; Douglas, L. A natural language-based presentation of cognitive stimulation to people with dementia in assistive technology: A pilot study. Inform. Health Soc. Care 2017, 42, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Galante, E.; Venturini, G.; Fiaccadori, C. Computer-based cognitive intervention for dementia: Preliminary results of a randomized clinical trial. G. Ital. Med. Lav. Ergon. 2007, 29, B26–B32. [Google Scholar] [PubMed]
- Brill, E.; Krebs, C.; Falkner, M.; Peter, J.; Henke, K.; Züst, M.; Minkova, L.; Brem, A.K.; Klöppe, S. Can a serious game-based cognitive training attenuate cognitive decline related to Alzheimer’s disease? Protocol for a randomized controlled trial. BMC Psychiatry 2022, 22, 552. [Google Scholar] [CrossRef]
- Greicius, M.D.; Srivastava, G.; Reiss, A.L.; Menon, V. Default-mode network activity distinguishes Alzheimer’s disease from healthy aging: Evidence from functional MRI. Proc. Natl. Acad. Sci. USA 2004, 101, 4637–4642. [Google Scholar] [CrossRef]
- Griffanti, L.; Dipasquale, O.; Laganà, M.M.; Nemni, R.; Clerici, M.; Smith, S.M.; Baselli, G.; Baglio, F. Effective artifact removal in resting state fMRI data improves detection of DMN functional connectivity alteration in Alzheimer’s disease. Front. Hum. Neurosci. 2015, 9, 449. [Google Scholar] [CrossRef] [PubMed]
- Hafkemeijer, A.; van der Grond, J.; Rombouts, S.A. Imaging the default mode network in aging and dementia. Biochim. Biophys. Acta 2012, 1822, 431–441. [Google Scholar] [CrossRef]
- Yildirim, E.; Buyukiscan, S.E. Default Mode Network Connectivity in Alzheimer’s Disease. Turk. J. Psychiatry 2019, 30, 279–286. [Google Scholar] [CrossRef]
- Baddeley, A.; Wilson, B.A. When implicit learning fails: Amnesia and the problem of error elimination. Neuropsychologia 1994, 32, 53–68. [Google Scholar] [CrossRef]
- Kessels, R.P.; De Haan, E.H. Mnemonic strategies in older people: A comparison of errorless and errorful learning. Age Ageing 2003, 32, 529–533. [Google Scholar] [CrossRef]
- Fish, J.; Manly, T.; Kopelman, M.D.; Morris, R.G. Errorless learning of prospective memory tasks: An experimental investigation in people with memory disorders. Neuropsychol. Rehabil. 2015, 25, 159–188. [Google Scholar] [CrossRef]
- Clare, L.; Wilson, B.A.; Carter, G.; Hodges, J.R.; Adams, M. Long-term maintenance of treatment gains following a cognitive rehabilitation intervention in early dementia of Alzheimer type: A single case study. Neuropsychol. Rehabil. 2001, 11, 477–494. [Google Scholar] [CrossRef]
- Haslam, C.; Moss, Z.; Hodder, K. Are two methods better than one? Evaluating the effectiveness of combining errorless learning with vanishing cues. J. Clin. Exp. Neuropsychol. 2010, 32, 973–985. [Google Scholar] [CrossRef] [PubMed]
- De Werd, M.M.; Boelen, D.; Rikkert, M.G.O.; Kessels, R.P. Errorless learning of everyday tasks in people with dementia. Clin. Interv. Aging. 2013, 8, 1177–1190. [Google Scholar] [CrossRef]
- Dunn, J.; Clare, L. Learning face–name associations in early-stage dementia: Comparing the effects of errorless learning and effortful processing. Neuropsychol. Rehabil. 2007, 17, 735–754. [Google Scholar] [CrossRef]
- Druks, J.; Garrard, P.; Hodges, J.; Robinson, S. The treatment of object naming, definition and object use in semantic dementia: The effectiveness of errorless learning. Aphasiology 2009, 23, 749–775. [Google Scholar] [CrossRef]
- Squires, E.J.; Hunkin, N.M.; Parkin, A.J. Errorless learning of novel associations in amnesia. Neuropsychologia 1997, 35, 1103–1111. [Google Scholar] [CrossRef]
- Hunkin, N.M.; Squires, E.J.; Parkin, A.J.; Tidy, J.A. Are the benefits of errorless learning dependent on implicit memory? Neuropsychologia 1998, 36, 25–36. [Google Scholar] [CrossRef]
- Tailby, R.; Haslam, C. An investigation of errorless learning in memory-impaired patients: Improving the technique and clarifying theory. Neuropsychologia 2003, 41, 1230–1240. [Google Scholar] [CrossRef]
- Lee, G.Y.; Yip, C.C.; Yu, E.C.; Man, D.W. Evaluation of a computer-assisted errorless learning-based memory training program for patients with early Alzheimer’s disease in Hong Kong: A pilot study. Clin. Interv. Aging. 2013, 8, 623–633. [Google Scholar] [CrossRef]
- Lee, Y.G. Evaluation of a Computer-Assisted Errorless Learning-Based Memory Training Program for Patients with Early Dementia. Ph.D. Thesis, The Hong Kong Polytechnic University, Hong Kong, China, 2014. [Google Scholar]
- Haslam, C.; Cruwys, T.; Haslam, S.A. “The we’s have it”: Evidence for the distinctive benefits of group engagement in enhancing cognitive health in aging. Soc. Sci. Med. 2014, 120, 57–66. [Google Scholar] [CrossRef]
- De Groot, J.C.; De Leeuwe, F.E.; Oudkerk, M.; Van Gtjnt, J.; Hofman, A.; Jolles, J.; Breteler, M.M.B. Periventricular cerebral white matter lesions predict rate of cognitive decline. Ann. Neurol. 2002, 52, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Maylor, E.A. Does prospective memory decline with age? In Prospective Memory: Theory and Applications, 1st ed.; Brandimonte, M., Einstein, G.O., McDaniel, M.A., Eds.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1996; pp. 173–197. [Google Scholar]
- Papagno, C.; Allegra, A.; Cardaci, M. Times estimation in Alzheimer’s disease and the role of the central executive. Brain Cogn. 2004, 54, 18–23. [Google Scholar] [CrossRef]
- Keller, J.N. Age–related neuropathology, cognitive decline and Alzheimer’s disease. Ageing Res. Rev. 2006, 5, 1–13. [Google Scholar] [CrossRef]
- Zimmermann, T.D.; Meier, B. The effect of implementation intentions on prospective memory performance across the lifespan. Appl. Cogn. Psychol. 2010, 24, 645–658. [Google Scholar] [CrossRef]
- Park, D.; Morrell, R.; Frieske, D.; Kincaid, D. Medication adherence behaviors in older adults: Effects of external cognitive supports. Psychol. Aging 1992, 7, 252–256. [Google Scholar] [CrossRef]
- Einstein, G.O.; McDaniel, M.A. Normal aging and prospective memory. J. Exp. Psychol. Learn. Mem. Cogn. 1990, 16, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Ellis, J. Memory for naturally-occurring intentions: Investigating pulses and steps. In Practical Aspects of Memory: Current Research and Issues; Gruneberg, M.M., Morris, P.E., Sykes, R.N., Eds.; Wiley: Chichester, UK, 1988; pp. 371–376. [Google Scholar]
- Rose, N.S.; Rendell, P.G.; Hering, A.; Kliegel, M.; Bidelman, G.M.; Craik, F.I. Cognitive and neural plasticity in older adults’ prospective memory following training with the Virtual Week computer game. Front. Hum. Neurosci. 2015, 9, 592. [Google Scholar] [CrossRef] [PubMed]
- Waldum, E.R.; Dufault, C.L.; McDaniel, M.A. Prospective Memory Training: Outlining a New Approach. J. Appl. Gerontol. 2016, 35, 1211–1234. [Google Scholar] [CrossRef]
- Hering, A.; Kliegel, M.; Rendell, P.G.; Craik, F.I.M.; Rose, N.S. Prospective Memory Is a Key Predictor of Functional Independence in Older Adults. J. Int. Neuropsychol. Soc. 2018, 24, 640–645. [Google Scholar] [CrossRef]
- Tse, Z.C.; Cao, Y.; Ogilvie, J.M.; Chau, B.K.; Ng, D.H.; Shum, D.H. Prospective Memory Training in Older Adults: A Systematic Review and Meta-Analysis. Neuropsychol. Rev. 2022, 33, 1–26. [Google Scholar] [CrossRef]
- Tsang, A.P.L.; Au, A.; Ming Lo, H.H. Prospective Memory Training for Healthy Older Adults: A Systematic Review. Clin. Gerontol. 2022, 45, 486–502. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.A.; Byrne, P.; Rodgers, S.E.; Maden, M.A. Systematic review of smartphone and tablet use by older adults with and without cognitive impairment. Innov. Aging 2022, 6, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Shelton, J.T.; Lee, J.H.; Scullin, M.K.; Rose, N.S.; Rendell, P.G.; McDaniel, M.A. Improving prospective memory in healthy older adults and individuals with very mild Alzheimer’s disease. J. Am. Geriatr. Soc. 2016, 64, 1307–1312. [Google Scholar] [CrossRef] [PubMed]
- Duro, D.; Simoes, M.R.; Ponciano, E.; Santana, E. Validation studies of the Portuguese experimental version of the Montreal Cognitive Assessment (MoCA): Confirmatory factor analysis. J. Neurol. 2010, 257, 728–734. [Google Scholar] [CrossRef]
- McAvinue, L.P.; Golemme, M.; Castorina, M.; Tatti, E.; Pigni, F.M.; Salomone, S.; Brennan, S.; Robertson, I.H. An evaluation of a working memory training scheme in older adults. Front. Aging Neurosci. 2013, 5, 20.1–20.19. [Google Scholar] [CrossRef]
- Hyer, L.; Scott, C.; Atkinson, M.M.; Mullen, C.M.; Lee, A.; Johnson, A.; Mckenzie, L.C. Cognitive training program to improve working memory in older adults with MCI. Clin. Gerontol. 2016, 39, 410–427. [Google Scholar] [CrossRef]
- Walton, C.C.; Kavanagh, A.; Downey, L.A.; Lomas, J.; Camfield, D.A.; Stough, C. Online cognitive training in healthy older adults: A preliminary study on the effects of single versus multi—domain training. Transl. Neurosci. 2015, 6, 13–19. [Google Scholar] [CrossRef]
- Corbett, A.; Owen, A.; Hampshire, A.; Grahn, J.; Stenton, R.; Dajani, S.; Ballard, C. The effect of an online cognitive training package in healthy older adults: An online randomized controlled trial. J. Am. Med. Dir. Assoc. 2015, 16, 990–997. [Google Scholar] [CrossRef]
- Charness, N. Predicting the use of technology: Findings from the center for research and education on aging and technology enhancement (CREATE). Gerontechnology 2005, 3, 230. [Google Scholar] [CrossRef]
- Charness, N.; Boissy, P.; Demiris, G.; Krupinski, E.A.; Lai, A.M.; Lopez, A.M. How human factors can influence the elderly in the use of telemedicine. Telemed. e-Health 2010, 16, 860–866. [Google Scholar] [CrossRef]
- Charness, N.; Best, R.; Souders, D. Memory function and supportive technology. Gerontechnology 2012, 11, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Trenorden, K.I.; Hull, M.J.; Lampit, A.; Greaves, D.; Keageet, H.A.D. Older adults’ experiences of a computerised cognitive training intervention: A mixed methods study. Austr. J. Psychol. 2022, 74, e2036581.1–e2036581.9. [Google Scholar] [CrossRef]
- Cahill, S.; Macijauskiene, J.; Nygård, A.M.; Faulkner, J.P.; Hagen, I. Technology in dementia care. Technol. Disabil. 2007, 19, 55–60. [Google Scholar] [CrossRef]
- Bjørneby, S.; Duff, P.; Mäki, O. Developing assistive technology for people with dementia. In Assistive Technology—Shaping the Future; Craddock, G.M., McCormack, L.P., Reilly, R.B., Knops, T.P., Eds.; IOS Press: Amsterdam, The Netherlands, 2003; pp. 781–786. [Google Scholar]
- Dieltein, C.S.; Bock, B.N.O.L. Recommendations on the Design of Serious Games for People with Dementia. EAI Endorsed Trans. Serious Games 2019, 5, e5.1–e5.12. [Google Scholar] [CrossRef]
- Gates, N.J.; Vernooij, R.W.; Di Nisio, M.; Karim, S.; March, E.; Martinez, G.; Rutjes, A.W. Computerised cognitive training for preventing dementia in people with mild cognitive impairment. Cochrane Database Syst. Rev. 2019, 3, CD012279. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Patients | Healthy Controls | |||
|---|---|---|---|---|
| Variable | Range | Mean (SD) | Range | Mean (SD) |
| Age | 63–85 | 76.53 (6.62) | 67–83 | 75.29 (5.40) |
| MoCA * | 5–20 | 11.87 (4.39) | 25–30 | 27.36 (1.50) |
| Object/place relation * | 12–28 | 17.07 (5.20) | 23–28 | 25.50 (1.61) |
| Medication * | 13–24 | 17.00 (3.91) | 23–29 | 26.71 (1.86) |
| Nutrition * | 12–28 | 17.53 (4.41) | 23–29 | 26.79 (1.76) |
| Faces * | 11–28 | 17.47 (5.18) | 24–30 | 27.21 (1.93) |
| Object/Place Relation | Meditation | Nutrition | Faces | |
|---|---|---|---|---|
| MoCA (patients with dementia) | 0.687 ** | 0.522 * | 0.695 ** | 0.719 ** |
| MoCA (healthy controls) | 0.911 *** | 0.966 *** | 0.905 *** | 0.779 *** |
| Age (patients with dementia) | −0.700 ** | −0.476 | −0.414 | −0.293 |
| Age (healthy controls) | −0.819 *** | −0.877 *** | −0.877 *** | −0.81 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nanousi, V.; Kalogeraki, K.; Smyrnaiou, A.; Tola, M.; Bokari, F.; Georgopoulos, V.C. The Development of a Pilot App Targeting Short-Term and Prospective Memory in People Diagnosed with Dementia. Behav. Sci. 2023, 13, 752. https://doi.org/10.3390/bs13090752
Nanousi V, Kalogeraki K, Smyrnaiou A, Tola M, Bokari F, Georgopoulos VC. The Development of a Pilot App Targeting Short-Term and Prospective Memory in People Diagnosed with Dementia. Behavioral Sciences. 2023; 13(9):752. https://doi.org/10.3390/bs13090752
Chicago/Turabian StyleNanousi, Vicky, Konstantina Kalogeraki, Aikaterini Smyrnaiou, Manila Tola, Foteini Bokari, and Voula Chris Georgopoulos. 2023. "The Development of a Pilot App Targeting Short-Term and Prospective Memory in People Diagnosed with Dementia" Behavioral Sciences 13, no. 9: 752. https://doi.org/10.3390/bs13090752
APA StyleNanousi, V., Kalogeraki, K., Smyrnaiou, A., Tola, M., Bokari, F., & Georgopoulos, V. C. (2023). The Development of a Pilot App Targeting Short-Term and Prospective Memory in People Diagnosed with Dementia. Behavioral Sciences, 13(9), 752. https://doi.org/10.3390/bs13090752