
A Deep Learning Neural Network to Classify Obesity Risk in Portuguese Adolescents Based on Physical Fitness Levels and Body Mass Index Percentiles: Insights for National Health Policies

 ,
,  ,
,  ,
,  ,
,  , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
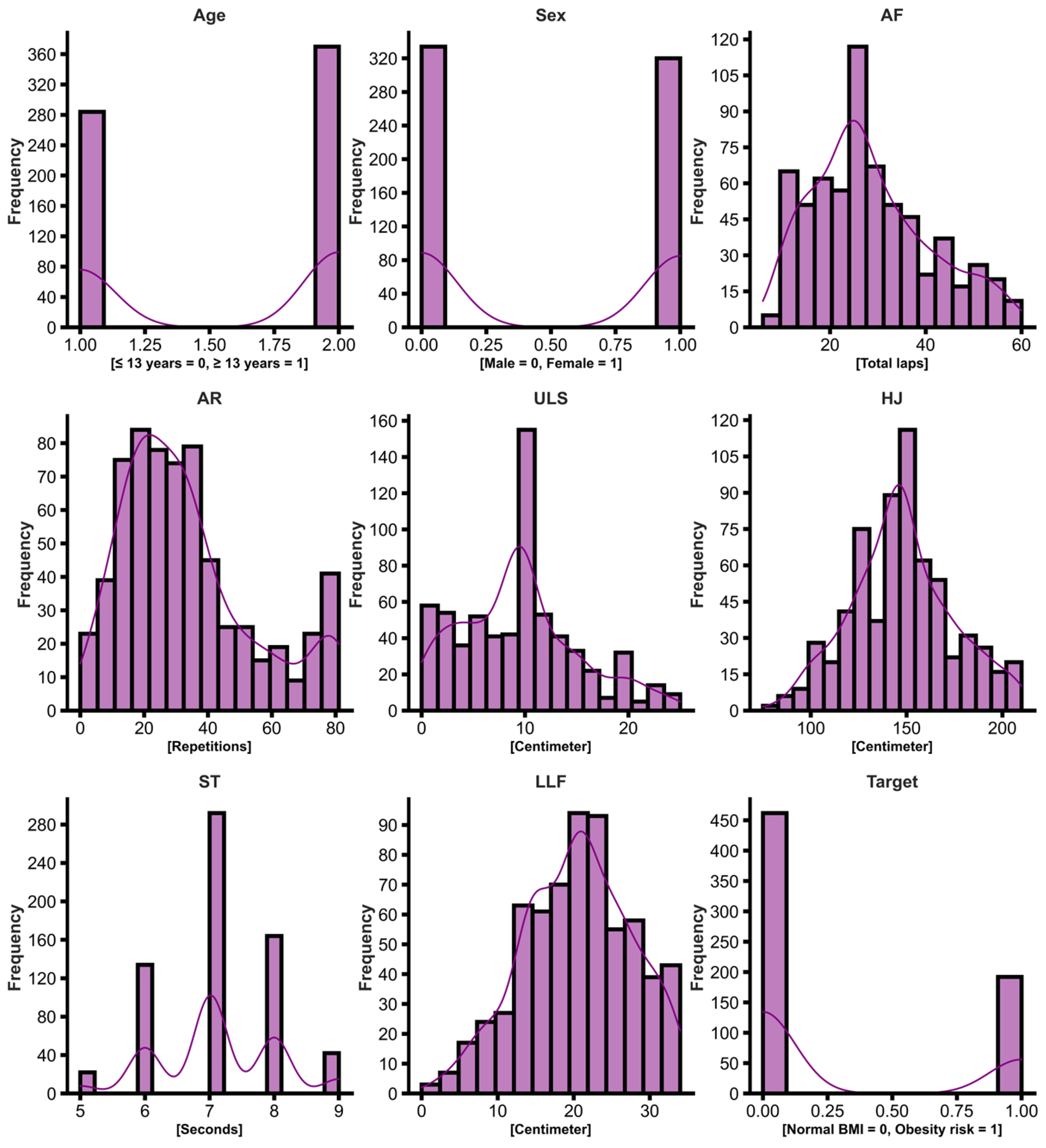
2.2. Dataset
2.3. Data Collection
2.3.1. Body Mass Index Percentiles
2.3.2. Aerobic Fitness
2.3.3. Horizontal Jump
2.3.4. 40-m Sprint Time
2.3.5. Upper Limb Strength
2.3.6. Lower Limb Flexibility
3. Results
3.1. Convolutional Neural Network Developing
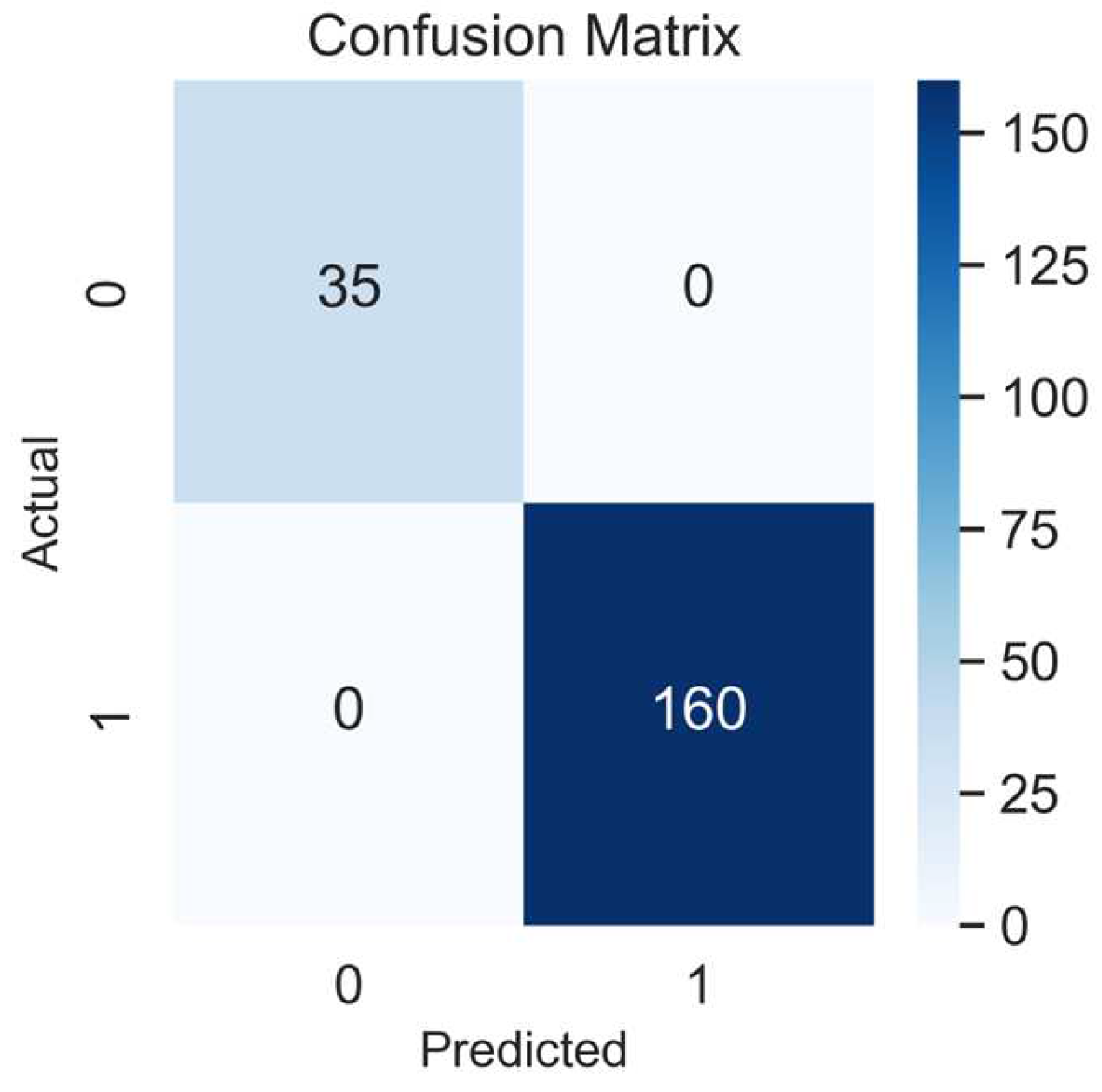
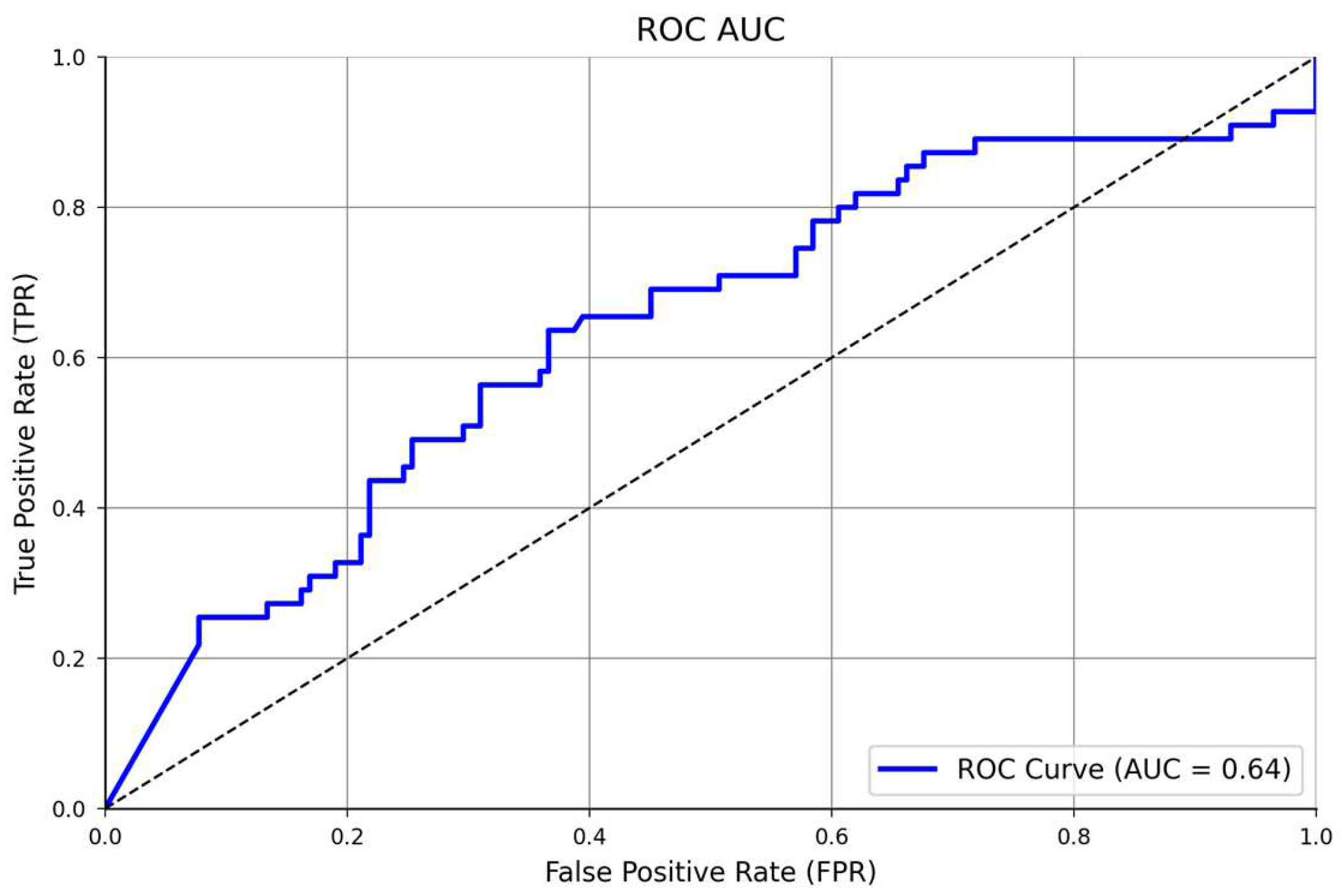
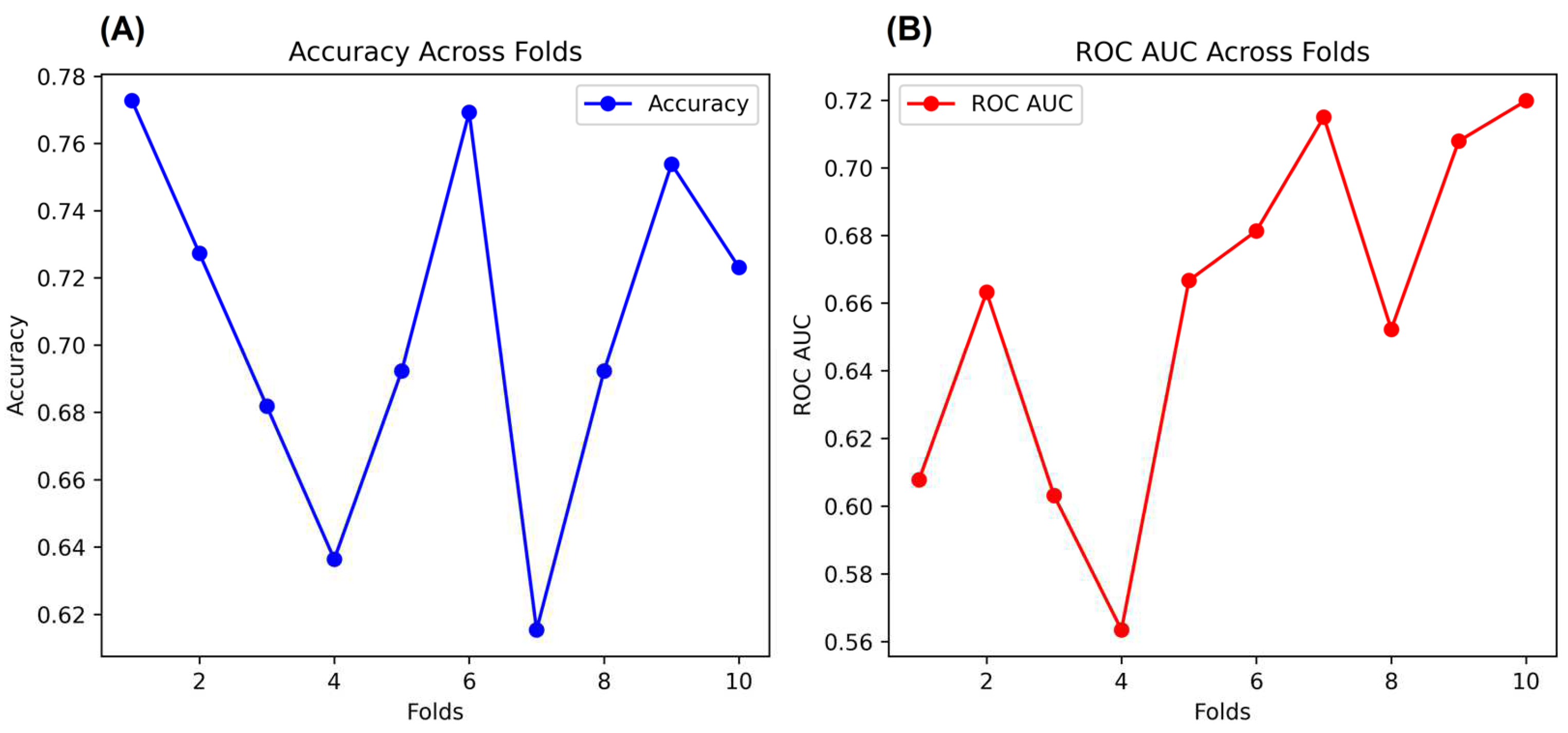
3.2. NNET Validation
4. Discussion
Study Limitations and Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chopra, M.; Galbraith, S.; Darnton-Hill, I. A Global Response to a Global Problem: The Epidemic of Overnutrition. Bull. World Health Organ. 2002, 80, 952–958. [Google Scholar]
- Graça, P.; Gregório, M.J.; de Sousa, S.M.; Brás, S.; Penedo, T.; Carvalho, T.; Bandarra, N.M.; Lima, R.M.; Simão, A.P.; Goiana-da-Silva, F.; et al. A New Interministerial Strategy for the Promotion of Healthy Eating in Portugal: Implementation and Initial Results. Health Res. Policy Syst. 2018, 16, 102. [Google Scholar] [CrossRef]
- World Obesity. Economic Impact of Overweight and Obesity Set to Reach 3.3% of Global GDP by 2060. Available online: https://www.worldobesity.org/news/economic-cost-of-overweight-and-obesity-set-to-reach-3.3-of-global-gdp-by-2060 (accessed on 22 May 2023).
- Destri, K.; Alves, J.; Gregório, M.J.; Dias, S.S.; Henriques, A.R.; Mendonça, N.; Canhão, H.; Rodrigues, A.M. Obesity-Attributable Costs of Absenteeism among Working Adults in Portugal. BMC Public Health 2022, 22, 978. [Google Scholar] [CrossRef]
- WHO. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 22 May 2023).
- WHO. Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 25 March 2023).
- Active Healthy Kids Global Alliance. Portugal: Active Healthy Kids Global Alliance. Available online: https://www.activehealthykids.org/portugal/ (accessed on 25 March 2023).
- Cao, Y.; Zhu, L.; Liu, J. Effects of Aerobic Exercise on Obese Children with Metabolic Syndrome: A Systematic Review and Meta-Analysis. J. Pediatr. Endocrinol. Metab. 2021, 34, 1069–1079. [Google Scholar] [CrossRef] [PubMed]
- Nooijen, C.F.J.; Galanti, M.R.; Engström, K.; Möller, J.; Forsell, Y. Effectiveness of Interventions on Physical Activity in Overweight or Obese Children: A Systematic Review and Meta-Analysis Including Studies with Objectively Measured Outcomes. Obes. Rev. 2017, 18, 195–213. [Google Scholar] [CrossRef] [PubMed]
- Cox, A.; Fairclough, S.J.; Kosteli, M.-C.; Noonan, R.J. Efficacy of School-Based Interventions for Improving Muscular Fitness Outcomes in Adolescent Boys: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 543–560. [Google Scholar] [CrossRef]
- Chen, J.; Zhou, Y.; Pan, X.; Li, X.; Long, J.; Zhang, H.; Zhang, J. Associations between Health-Related Physical Fitness and Cardiovascular Disease Risk Factors in Overweight and Obese University Staff. Int. J. Environ. Res. Public Health 2020, 17, 9031. [Google Scholar] [CrossRef] [PubMed]
- Räisänen, L.; Lommi, S.; Engberg, E.; Kolho, K.; Viljakainen, H. Central Obesity in School-aged Children Increases the Likelihood of Developing Paediatric Autoimmune Diseases. Pediatr. Obes. 2022, 17, e12857. [Google Scholar] [CrossRef] [PubMed]
- Basu, T.; Selman, A.; Reddy, A.P.; Reddy, P.H. Current Status of Obesity: Protective Role of Catechins. Antioxidants 2023, 12, 474. [Google Scholar] [CrossRef]
- Silva, C.; Vilas, C.; Pereira, B.; Rosário, P.; Fuentes, S.; Magalhães, P. Changes in Physical Fitness Parameters in a Portuguese Sample of Adolescents during the COVID-19 Pandemic: A One-Year Longitudinal Study. Int. J. Environ. Res. Public Health 2023, 20, 3422. [Google Scholar] [CrossRef]
- da Encarnação, S.G.A.; Moreira, O.C.; Fazolo, S.L.; de Oliveira, C.E.P.; da Encarnação, I.G.A.; Carneiro-Júnior, M.A. COVID-19 and Social Distancing of the Elderly: The Importance of Physical Exercise. Int. J. Phys. Educ. Fit. Sport. 2021, 10, 88–108. [Google Scholar] [CrossRef]
- Henriques-Neto, D.; Magalhães, J.P.; Hetherington-Rauth, M.; Santos, D.A.; Baptista, F.; Sardinha, L.B. Physical Fitness and Bone Health in Young Athletes and Nonathletes. Sports Health 2020, 12, 441–448. [Google Scholar] [CrossRef]
- FITescola. Available online: https://fitescola.dge.mec.pt/home.aspx (accessed on 16 June 2022).
- UNESCO. Science for Development: The Approach of a Small Island State-UNESCO Digital Library. Available online: https://unesdoc.unesco.org/ark:/48223/pf0000120956 (accessed on 22 May 2023).
- Sarker, I.H. AI-Based Modeling: Techniques, Applications and Research Issues towards Automation, Intelligent and Smart Systems. SN Comput. Sci. 2022, 3, 158. [Google Scholar] [CrossRef]
- Shahid, M.; Kim, J. Exercise May Affect Metabolism in Cancer-Related Cognitive Impairment. Metabolites 2020, 10, 377. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Hu, X. Early Warning Method for Public Health Emergency under Artificial Neural Network in the Context of Deep Learning. Front. Psychol. 2021, 12, 594031. [Google Scholar] [CrossRef] [PubMed]
- Unpingco, J. Python for Probability, Statistics, and Machine Learning; Springer: Berlin/Heidelberg, Germany, 2016; Volume 1. [Google Scholar]
- Zeng, D.; Cao, Z.; Neill, D.B. Artificial Intelligence–Enabled Public Health Surveillance—From Local Detection to Global Epidemic Monitoring and Control. In Artificial Intelligence in Medicine; Academic Press: Cambridge, MA, USA, 2021; pp. 437–453. [Google Scholar] [CrossRef]
- Zheng, Z.; Ruggiero, K. Using Machine Learning to Predict Obesity in High School Students. In Proceedings of the 2017 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Kansas City, MO, USA, 13–16 November 2017; pp. 2132–2138. [Google Scholar]
- Wiechmann, P.; Lora, K.; Branscum, P.; Fu, J. Identifying Discriminative Attributes to Gain Insights Regarding Child Obesity in Hispanic Preschoolers Using Machine Learning Techniques. In Proceedings of the 2017 IEEE 29th International Conference on Tools with Artificial Intelligence (ICTAI), Boston, MA, USA, 6–8 November 2017; pp. 11–15. [Google Scholar]
- Pang, X.; Forrest, C.B.; Lê-Scherban, F.; Masino, A.J. Prediction of Early Childhood Obesity with Machine Learning and Electronic Health Record Data. Int. J. Med. Inform. 2021, 150, 104454. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Zhan, W.; Wei, M.; Chen, Q. Associations between Different Dietary Vitamins and the Risk of Obesity in Children and Adolescents: A Machine Learning Approach. Front. Endocrinol. 2022, 12, 1972. [Google Scholar] [CrossRef]
- Allen, B.; Lane, M.; Steeves, E.A.; Raynor, H. Using Explainable Artificial Intelligence to Discover Interactions in an Ecological Model for Obesity. Int. J. Environ. Res. Public Health 2022, 19, 9447. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.; Lee, S.; Oh, C. Age-Specific Risk Factors for the Prediction of Obesity Using a Machine Learning Approach. Front. Public Health 2023, 10, 998782. [Google Scholar] [CrossRef] [PubMed]
- Gülü, M.; Yagin, F.H.; Yapici, H.; Irandoust, K.; Dogan, A.A.; Taheri, M.; Szura, E.; Barasinska, M.; Gabrys, T. Is Early or Late Biological Maturation Trigger Obesity? A Machine Learning Modeling Research in Turkey Boys and Girls. Front. Nutr. 2023, 10, 1139179. [Google Scholar] [CrossRef]
- Da Encarnação, S.G.A.; Flores, P.; Magalhães, D.; Afonso, G.; Pereira, A.; Fonseca, R.B.; Ribeiro, J.; Silva-Santos, S.; Teixeira, J.E.; Monteiro, A.M.; et al. The Influence of Abdominal Adiposity and Physical Fitness on Obesity Status of Portuguese Adolescents. Int. J. Environ. Res. Public Health 2022, 19, 11213. [Google Scholar] [CrossRef] [PubMed]
- CDC. BMI for Children and Teens. Available online: https://www.cdc.gov/obesity/basics/childhood-defining.html (accessed on 13 March 2023).
- WHO. Adolescent Health. Available online: https://www.who.int/southeastasia/health-topics/adolescent-health (accessed on 12 August 2022).
- Python. Available online: https://www.python.org/ (accessed on 13 March 2023).
- WHO Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. World Health Organ. Tech. Rep. Ser. 2000, 894, 1–253.
- Funder, D.C.; Ozer, D.J. Evaluating Effect Size in Psychological Research: Sense and Nonsense. Adv. Methods Pract. Psychol. Sci. 2019, 2, 156–168. [Google Scholar] [CrossRef]
- Bradley, A.P. The Use of the Area under the ROC Curve in the Evaluation of Machine Learning Algorithms. Pattern Recognit. 1997, 30, 1145–1159. [Google Scholar] [CrossRef]
- Kandel, I.; Castelli, M. The Effect of Batch Size on the Generalizability of the Convolutional Neural Networks on a Histopathology Dataset. ICT Express 2020, 6, 312–315. [Google Scholar] [CrossRef]
- Refaeilzadeh, P.; Tang, L.; Liu, H. Cross-Validation. In Encyclopedia of Database Systems; Liu, L., Özsu, M.T., Eds.; Springer: Boston, MA, USA, 2009; pp. 532–538. ISBN 978-0-387-39940-9. [Google Scholar]
- Loos, R.J.F.; Yeo, G.S.H. The Genetics of Obesity: From Discovery to Biology. Nat. Rev. Genet. 2022, 23, 120–133. [Google Scholar] [CrossRef]
- Nicolaidis, S. Environment and Obesity. Metabolism 2019, 100, 153942. [Google Scholar] [CrossRef]
- Shalitin, S.; Giannini, C. Obesity, Metabolic Syndrome, and Nutrition. World Rev. Nutr. Diet. 2022, 125, 41–63. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, L.D.; Zuelch, M.L.; Dimitratos, S.M.; Scherr, R.E. Adolescent Obesity: Diet Quality, Psychosocial Health, and Cardiometabolic Risk Factors. Nutrients 2020, 12, 43. [Google Scholar] [CrossRef]
- Jepsen, S.; Suvan, J.; Deschner, J. The Association of Periodontal Diseases with Metabolic Syndrome and Obesity. Periodontology 2000 2020, 83, 125–153. [Google Scholar] [CrossRef]
- Apovian, C.M.; Aronne, L.J.; Bessesen, D.H.; McDonnell, M.E.; Murad, M.H.; Pagotto, U.; Ryan, D.H.; Still, C.D. Endocrine Society Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2015, 100, 342–362. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; Taggart, F.M.; Kandala, N.-B.; Currie, A.; Peile, E.; Stranges, S.; Miller, M.A. Meta-Analysis of Short Sleep Duration and Obesity in Children and Adults. Sleep 2008, 31, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, J.E.; Bragada, J.A.; Bragada, J.P.; Coelho, J.P.; Pinto, I.G.; Reis, L.P.; Fernandes, P.O.; Morais, J.E.; Magalhães, P.M. Structural Equation Modelling for Predicting the Relative Contribution of Each Component in the Metabolic Syndrome Status Change. Int. J. Environ. Res. Public Health 2022, 19, 3384. [Google Scholar] [CrossRef] [PubMed]
- Aubert, S.; Barnes, J.D.; Abdeta, C.; Abi Nader, P.; Adeniyi, A.F.; Aguilar-Farias, N.; Andrade Tenesaca, D.S.; Bhawra, J.; Brazo-Sayavera, J.; Cardon, G.; et al. Global Matrix 3.0 Physical Activity Report Card Grades for Children and Youth: Results and Analysis From 49 Countries. J. Phys. Act. Health 2018, 15, S251–S273. [Google Scholar] [CrossRef]
- Miotto, R.; Wang, F.; Wang, S.; Jiang, X.; Dudley, J.T. Deep Learning for Healthcare: Review, Opportunities and Challenges. Brief. Bioinform. 2017, 19, 1236–1246. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Henao-Mejia, J.; Henrickson, S.E. Obesity and Immune Status in Children. Curr. Opin. Pediatr. 2020, 32, 805–815. [Google Scholar] [CrossRef]
- Cristi-Montero, C.; Courel-Ibáñez, J.; Ortega, F.B.; Castro-Piñero, J.; Santaliestra-Pasias, A.; Polito, A.; Vanhelst, J.; Marcos, A.; Moreno, L.M.; Ruiz, J.R. Mediation Role of Cardiorespiratory Fitness on the Association between Fatness and Cardiometabolic Risk in European Adolescents: The HELENA Study. J. Sport. Health Sci. 2021, 10, 360–367. [Google Scholar] [CrossRef]
- Hsu, C.-S.; Chang, S.-T.; Nfor, O.N.; Lee, K.-J.; Ho, C.-C.; Liu, C.-C.; Lee, S.-S.; Liaw, Y.-P. Association of Metabolic Syndrome with Aerobic Exercise and LPL Rs3779788 Polymorphism in Taiwan Biobank Individuals. Diabetes Metab. Syndr. Obes. 2021, 14, 3997–4004. [Google Scholar] [CrossRef]
- Henriksson, H.; Henriksson, P.; Tynelius, P.; Ekstedt, M.; Berglind, D.; Labayen, I.; Ruiz, J.R.; Lavie, C.J.; Ortega, F.B. Cardiorespiratory Fitness, Muscular Strength, and Obesity in Adolescence and Later Chronic Disability Due to Cardiovascular Disease: A Cohort Study of 1 Million Men. Eur. Heart J. 2020, 41, 1503–1510. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Is Muscular Fitness Associated with Future Health Benefits in Children and Adolescents? A Systematic Review and Meta-Analysis of Longitudinal Studies. Sports Med. 2019, 49, 1079–1094. [Google Scholar] [CrossRef]
- Joensuu, L.; Rautiainen, I.; Äyrämö, S.; Syväoja, H.J.; Kauppi, J.-P.; Kujala, U.M.; Tammelin, T.H. Precision Exercise Medicine: Predicting Unfavourable Status and Development in the 20-m Shuttle Run Test Performance in Adolescence with Machine Learning. BMJ Open Sport Exerc. Med. 2021, 7, e001053. [Google Scholar] [CrossRef] [PubMed]
- Tishukaj, F.; Shalaj, I.; Gjaka, M.; Ademi, B.; Ahmetxhekaj, R.; Bachl, N.; Tschan, H.; Wessner, B. Physical Fitness and Anthropometric Characteristics among Adolescents Living in Urban or Rural Areas of Kosovo. BMC Public Health 2017, 17, 711. [Google Scholar] [CrossRef]
- Fraser, B.J.; Rollo, S.; Sampson, M.; Magnussen, C.G.; Lang, J.J.; Tremblay, M.S.; Tomkinson, G.R. Health-Related Criterion-Referenced Cut-Points for Musculoskeletal Fitness Among Youth: A Systematic Review. Sports Med. 2021, 51, 2629–2646. [Google Scholar] [CrossRef]
- de Almeida-Neto, P.F.; Oliveira, V.M.M.; de Matos, D.G.; dos Santos, Í.K.; Baxter-Jones, A.; Pinto, V.C.M.; de Macêdo Cesário, T.; Aidar, F.J.; Dantas, P.M.S.; de Araújo Tinôco Cabral, B.G. Factors Related to Lower Limb Performance in Children and Adolescents Aged 7 to 17 Years: A Systematic Review with Meta-Analysis. PLoS ONE 2021, 16, e0258144. [Google Scholar] [CrossRef] [PubMed]
- Petrovics, P.; Sandor, B.; Palfi, A.; Szekeres, Z.; Atlasz, T.; Toth, K.; Szabados, E. Association between Obesity and Overweight and Cardiorespiratory and Muscle Performance in Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 134. [Google Scholar] [CrossRef] [PubMed]
- Méndez-Hernández, L.D.; Ramírez-Moreno, E.; Barrera-Gálvez, R.; Cabrera-Morales, M.d.C.; Reynoso-Vázquez, J.; Flores-Chávez, O.R.; Morales-Castillejos, L.; Cruz-Cansino, N.d.S.; Jiménez-Sánchez, R.C.; Arias-Rico, J. Effects of Strength Training on Body Fat in Children and Adolescents with Overweight and Obesity: A Systematic Review with Meta-Analysis. Children 2022, 9, 995. [Google Scholar] [CrossRef]
- Deforche, B.; Lefevre, J.; De Bourdeaudhuij, I.; Hills, A.P.; Duquet, W.; Bouckaert, J. Physical Fitness and Physical Activity in Obese and Nonobese Flemish Youth. Obes. Res. 2003, 11, 434–441. [Google Scholar] [CrossRef]
- Wearing, S.C.; Hennig, E.M.; Byrne, N.M.; Steele, J.R.; Hills, A.P. The Impact of Childhood Obesity on Musculoskeletal Form. Obes. Rev. 2006, 7, 209–218. [Google Scholar] [CrossRef]
- Bolados, C.C.; Ferrari, G.; Suárez-Reyes, M.; Quintiliano Scarpelli Dourado, D.; Diaz-Peña, H.; Pizarro, T. Muscular Strength of Upper and Lower Limbs and Self-Esteem in Chilean SchoolChildren: Independent Associations with Body Composition Indicators. Int. J. Environ. Res. Public Health 2021, 18, 361. [Google Scholar] [CrossRef]
- Lopez-Jaramillo, P.; Lopez-Lopez, J.P.; Camila Tole, M.; Cohen, D.D. Muscular Strength in Risk Factors for Cardiovascular Disease and Mortality: A Narrative Review. Anatol. J. Cardiol. 2022, 26, 598–607. [Google Scholar] [CrossRef]
- van Sluijs, E.M.F.; Ekelund, U.; Crochemore-Silva, I.; Guthold, R.; Ha, A.; Lubans, D.; Oyeyemi, A.L.; Ding, D.; Katzmarzyk, P.T. Physical Activity Behaviours in Adolescence: Current Evidence and Opportunities for Intervention. Lancet 2021, 398, 429–442. [Google Scholar] [CrossRef]
- Ajisafe, T. Association between 90° Push-up and Cardiorespiratory Fitness: Cross-Sectional Evidence of Push-up as a Tractable Tool for Physical Fitness Surveillance in Youth. BMC Pediatr. 2019, 19, 458. [Google Scholar] [CrossRef] [PubMed]
- Stathokostas, L.; McDonald, M.W.; Little, R.M.D.; Paterson, D.H. Flexibility of Older Adults Aged 55–86 Years and the Influence of Physical Activity. J. Aging Res. 2013, 2013, 743843. [Google Scholar] [CrossRef] [PubMed]
- de Lima, T.R.; Martins, P.C.; Moraes, M.S.; Silva, D.A.S. Association of Flexibility with Sociodemographic Factors, Physical Activity, Muscle Strength, and Aerobic Fitness in Adolescents from Southern Brazil. Rev. Paul. Pediatr. 2019, 37, 202–208. [Google Scholar] [CrossRef]
- Pate, R.; Oria, M.; Pillsbury, L. Health-Related Fitness Measures for Youth: Flexibility. In Fitness Measures and Health Outcomes in Youth; National Academies Press: Washington, DC, USA, 2012. [Google Scholar]
- Brown, K.A.; Patel, D.R.; Darmawan, D. Participation in Sports in Relation to Adolescent Growth and Development. Transl. Pediatr. 2017, 6, 150–159. [Google Scholar] [CrossRef]
- Molina-García, C.; Jiménez-García, J.D.; Velázquez-Díaz, D.; Ramos-Petersen, L.; López-del-Amo-Lorente, A.; Martínez-Sebastián, C.; Álvarez-Salvago, F. Overweight and Obesity: Its Impact on Foot Type, Flexibility, Foot Strength, Plantar Pressure and Stability in Children from 5 to 10 Years of Age: Descriptive Observational Study. Children 2023, 10, 696. [Google Scholar] [CrossRef]
- Schwartz, M.W.; Seeley, R.J.; Zeltser, L.M.; Drewnowski, A.; Ravussin, E.; Redman, L.M.; Leibel, R.L. Obesity Pathogenesis: An Endocrine Society Scientific Statement. Endocr. Rev. 2017, 38, 267–296. [Google Scholar] [CrossRef]
- Donti, O.; Konrad, A.; Panidi, I.; Dinas, P.C.; Bogdanis, G.C. Is There a “Window of Opportunity” for Flexibility Development in Youth? A Systematic Review with Meta-Analysis. Sports Med.-Open 2022, 8, 88. [Google Scholar] [CrossRef]
- Bataweel, E.A.; Ibrahim, A.I. Balance and Musculoskeletal Flexibility in Children with Obesity: A Cross-Sectional Study. Ann. Saudi Med. 2020, 40, 120–125. [Google Scholar] [CrossRef]
- Burt Solorzano, C.M.; McCartney, C.R. Obesity and the Pubertal Transition in Girls and Boys. Reproduction 2010, 140, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Voelker, D.K.; Reel, J.J.; Greenleaf, C. Weight Status and Body Image Perceptions in Adolescents: Current Perspectives. Adolesc. Health Med. Ther. 2015, 6, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Pojskic, H.; Eslami, B. Relationship between Obesity, Physical Activity, and Cardiorespiratory Fitness Levels in Children and Adolescents in Bosnia and Herzegovina: An Analysis of Gender Differences. Front. Physiol. 2018, 9, 1734. [Google Scholar] [CrossRef] [PubMed]
- Yagin, F.H.; Gülü, M.; Gormez, Y.; Castañeda-Babarro, A.; Colak, C.; Greco, G.; Fischetti, F.; Cataldi, S. Estimation of Obesity Levels with a Trained Neural Network Approach Optimized by the Bayesian Technique. Appl. Sci. 2023, 13, 3875. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Boys ( ± SD) | Girls ( ± SD) |
|---|---|---|
| Age (Years) | 14.6 ± 2.2 | 13.01 ± 2.06 |
| Weight | 54.45 ± 15.75 | 58.51 ± 15.49 |
| Height | 158.37 ± 11.60 | 167.4 ± 79.8 |
| AF (Laps) | 31 ± 13.4 | 25.7 ± 10.12 |
| ULS (Repetition) | 10.86 ± 5.86 | 7.87 ± 5.08 |
| HJ (Centimeter) | 156.84 ± 27.23 | 137.89 ± 22.22 |
| 40-m ST (Seconds) | 6.82 ± 0.95 | 7.41 ± 0.75 |
| LLF (Centimeter) | 18.29 ± 6.88 | 22.67 ± 6.62 |
| classifier = Sequential() |
| classifier.add(Dense(activation = “relu”, input_dim = 7, |
| units = 4, kernel_initializer = “uniform”)) |
| classifier.add(Dense(activation = “relu”, units = 8, |
| kernel_initializer = “uniform”)) |
| classifier.add(Dense(activation = “sigmoid”, units = 1, |
| kernel_initializer = “uniform”)) |
| classifier.compile(optimizer = ‘adam’, loss = ‘binary_crossentropy’, |
| metrics = [‘accuracy’]) |
| Layer (Type) | Output Shape | Parameters |
|---|---|---|
| dense (Dense) | (None, 4) | 32 |
| dense_1 (Dense) | (None, 8) | 40 |
| dense_2 (Dense) | (None, 1) | 9 |
| Total Parameters: 81 | ||
| Trainable Parameters: 81 | ||
| Non-Trainable Parameters: 0 |
| Epochs | Processing Time | Accuracy Loss | Accuracy |
|---|---|---|---|
| 1/24 | 0 s 3 ms/step | 0.5188 | 0.7505 |
| 2/24 | 0 s 4 ms/step | 0.5188 | 0.7462 |
| 3/24 | 0 s 3 ms/step | 0.5191 | 0.7505 |
| 4/24 | 0 s 4 ms/step | 0.5192 | 0.7527 |
| 5/24 | 0 s 3 ms/step | 0.5187 | 0.7484 |
| 6/24 | 0 s 3 ms/step | 0.5191 | 0.7418 |
| 7/24 | 0 s 3 ms/step | 0.5186 | 0.7505 |
| 8/24 | 0 s 3 ms/step | 0.5190 | 0.7505 |
| 9/24 | 0 s 2 ms/step | 0.5186 | 0.7549 |
| 10/24 | 0 s 3 ms/step | 0.5189 | 0.7462 |
| 11/24 | 0 s 3 ms/step | 0.5185 | 0.7440 |
| 12/24 | 0 s 3 ms/step | 0.5155 | 0.7502 |
| 13/24 | 0 s 2 ms/step | 0.5187 | 0.7505 |
| 14/24 | 0 s 2 ms/step | 0.5190 | 0.7505 |
| 15/24 | 0 s 3 ms/step | 0.5182 | 0.7484 |
| 16/24 | 0 s 2 ms/step | 0.5186 | 0.7505 |
| 17/24 | 0 s 2 ms/step | 0.5185 | 0.7527 |
| 18/24 | 0 s 3 ms/step | 0.5187 | 0.7484 |
| 19/24 | 0 s 3 ms/step | 0.5184 | 0.7505 |
| 20/24 | 0 s 4 ms/step | 0.5187 | 0.7484 |
| 21/24 | 0 s 4 ms/step | 0.5181 | 0.7484 |
| 22/24 | 0 s 4 ms/step | 0.5185 | 0.7484 |
| 23/24 | 0 s 3 ms/step | 0.5183 | 0.7527 |
| 24/24 | 0 s 4 ms/step | 0.5184 | 0.7527 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forte, P.; Encarnação, S.; Monteiro, A.M.; Teixeira, J.E.; Hattabi, S.; Sortwell, A.; Branquinho, L.; Amaro, B.; Sampaio, T.; Flores, P.; et al. A Deep Learning Neural Network to Classify Obesity Risk in Portuguese Adolescents Based on Physical Fitness Levels and Body Mass Index Percentiles: Insights for National Health Policies. Behav. Sci. 2023, 13, 522. https://doi.org/10.3390/bs13070522
Forte P, Encarnação S, Monteiro AM, Teixeira JE, Hattabi S, Sortwell A, Branquinho L, Amaro B, Sampaio T, Flores P, et al. A Deep Learning Neural Network to Classify Obesity Risk in Portuguese Adolescents Based on Physical Fitness Levels and Body Mass Index Percentiles: Insights for National Health Policies. Behavioral Sciences. 2023; 13(7):522. https://doi.org/10.3390/bs13070522
Chicago/Turabian StyleForte, Pedro, Samuel Encarnação, António Miguel Monteiro, José Eduardo Teixeira, Soukaina Hattabi, Andrew Sortwell, Luís Branquinho, Bruna Amaro, Tatiana Sampaio, Pedro Flores, and et al. 2023. "A Deep Learning Neural Network to Classify Obesity Risk in Portuguese Adolescents Based on Physical Fitness Levels and Body Mass Index Percentiles: Insights for National Health Policies" Behavioral Sciences 13, no. 7: 522. https://doi.org/10.3390/bs13070522
APA StyleForte, P., Encarnação, S., Monteiro, A. M., Teixeira, J. E., Hattabi, S., Sortwell, A., Branquinho, L., Amaro, B., Sampaio, T., Flores, P., Silva-Santos, S., Ribeiro, J., Batista, A., Ferraz, R., & Rodrigues, F. (2023). A Deep Learning Neural Network to Classify Obesity Risk in Portuguese Adolescents Based on Physical Fitness Levels and Body Mass Index Percentiles: Insights for National Health Policies. Behavioral Sciences, 13(7), 522. https://doi.org/10.3390/bs13070522