
The Temporal Relationship between Depressive Symptoms and Loneliness: The Moderating Role of Self-Compassion
 , , and
, , and
Abstract
1. Introduction
1.1. The Bidirectional Relationship between Loneliness and Depression among the College Student Population
1.2. The Moderating Role of Self-Compassion
1.3. The Current Study
2. Method
2.1. Participants and Procedure
2.2. Measures
2.2.1. Self-Compassion Scale (SCS)
2.2.2. Patient Health Questionnaire-9 (PHQ-9)
2.2.3. UCLA Loneliness Scale-8 (ULS-8)
2.3. Network Analysis
3. Result
3.1. Item Check and Descriptive Statistics
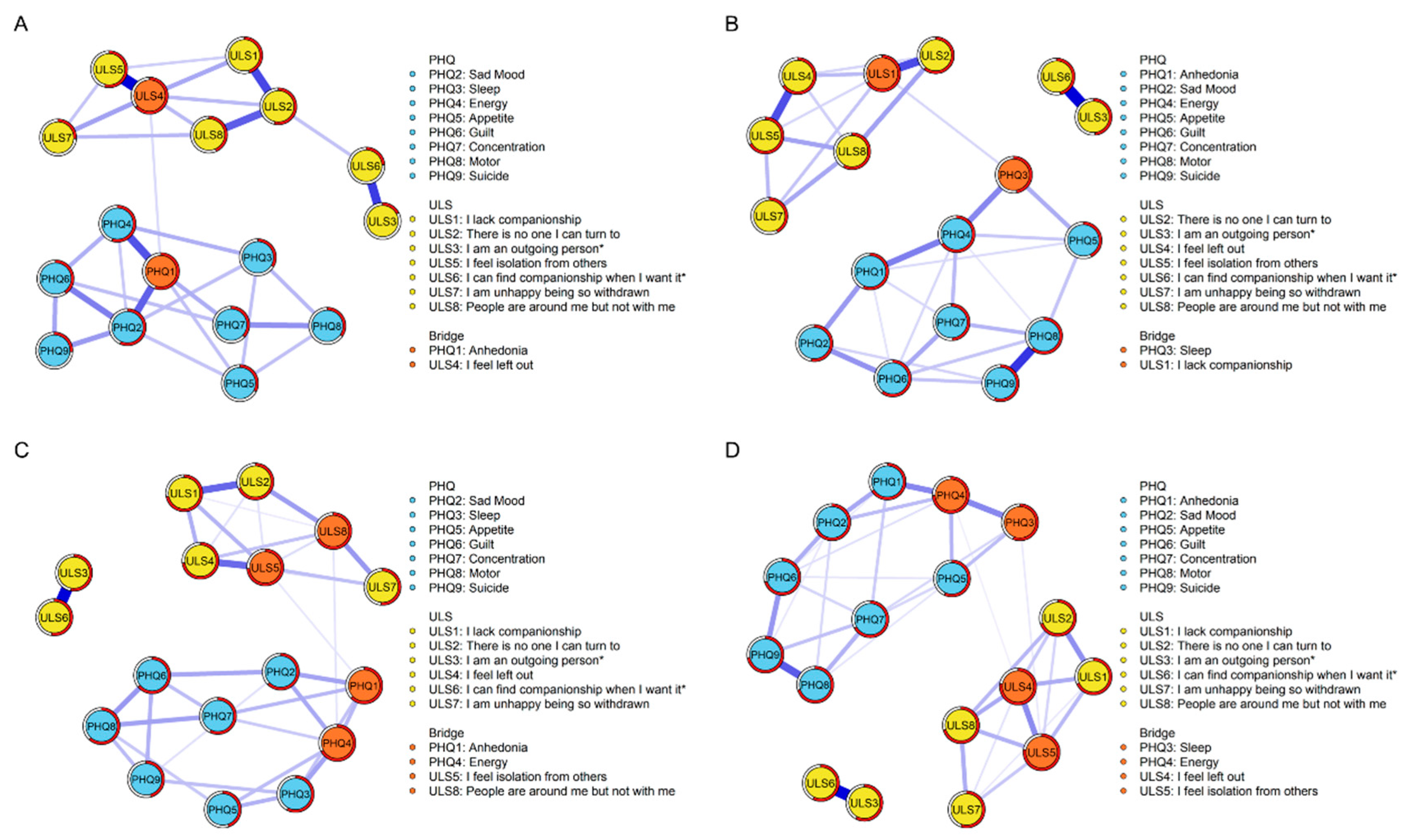
3.2. Contemporaneous Network Structures
3.3. Network Comparison Test
3.4. Temporal Network Structures
3.5. Network Accuracy and Stability
3.6. Unidimensional Loneliness Network Structures
4. Discussion
4.1. The Contemporaneous Symptom Network Structures and t-Test Results between High- and Low-Self-Compassion Groups at Two Time Points
4.2. Cross-Lagged Panel Networks between High- and Low-Self-Compassion Groups
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lépine, J.-P.; Briley, M. The increasing burden of depression. Neuropsychiatr. Dis. Treat. 2011, 7 (Suppl. 1), 3–7. [Google Scholar] [CrossRef] [PubMed]
- Center for Collegiate Mental Health. Annual Reports. 2022. Available online: https://ccmh.psu.edu/annual-reports (accessed on 30 June 2022).
- Li, W.; Zhao, Z.; Chen, D.; Peng, Y.; Lu, Z. Prevalence and associated factors of depression and anxiety symptoms among college students: A systematic review and meta-analysis. J. Child Psychol. Psychiatry 2022, 63, 1222–1230. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, L.M.; Gullone, E. The clinical significance of loneliness: A literature review. Clin. Psychol. Rev. 2006, 26, 695–718. [Google Scholar] [CrossRef]
- Drageset, J.; Espehaug, B.; Kirkevold, M. The impact of depression and sense of coherence on emotional and social loneliness among nursing home residents without cognitive impairment—A questionnaire survey. J. Clin. Nurs. 2012, 21, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Jaremka, L.M.; Fagundes, C.P.; Glaser, R.; Bennett, J.M.; Malarkey, W.B.; Kiecolt-Glaser, J.K. Loneliness predicts pain, depression, and fatigue: Understanding the role of immune dysregulation. Psychoneuroendocrinology 2013, 38, 1310–1317. [Google Scholar] [CrossRef]
- Rich, A.R.; Scovel, M. Causes of Depression in College Students: A Cross-Lagged Panel Correlational Analysis. Psychol. Rep. 1987, 60, 27–30. [Google Scholar] [CrossRef]
- Anderson, C.A.; Horowitz, L.M.; French, R.D. Attributional style of lonely and depressed people. J. Personal. Soc. Psychol. 1983, 45, 127–136. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Hawkley, L.C.; Thisted, R.A. Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago Health, Aging, and Social Relations Study. Psychol. Aging 2010, 25, 453–463. [Google Scholar] [CrossRef]
- Coyne, J.C. Depression and the response of others. J. Abnorm. Psychol. 1976, 85, 186–193. [Google Scholar] [CrossRef]
- Teo, A.R.; Choi, H.; Andrea, S.B.; Valenstein, M.; Newsom, J.T.; Dobscha, S.K.; Zivin, K. Does Mode of Contact with Different Types of Social Relationships Predict Depression in Older Adults? Evidence from a Nationally Representative Survey. J. Am. Geriatr. Soc. 2015, 63, 2014–2022. [Google Scholar] [CrossRef]
- Fried, E.I.; Nesse, R.M. Depression sum-scores don’t add up: Why analyzing specific depression symptoms is essential. BMC Med. 2015, 13, 72. [Google Scholar] [CrossRef] [PubMed]
- Baumeister, R.F.; Leary, M.R. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychol. Bull. 1995, 117, 497–529. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; La Guardia, J.G. What is being optimized?: Self-determination theory and basic psychological needs. In Psychology and the Aging Revolution: How We Adapt to Longer Life; American Psychological Association: Washington, DC, USA, 2000; pp. 145–172. [Google Scholar] [CrossRef]
- McAdams, D.P.; Bryant, F.B. Intimacy Motivation and Subjective Mental Health in a Nationwide Sample. J. Personal. 1987, 55, 395–413. [Google Scholar] [CrossRef] [PubMed]
- Kagan, J. Loneliness: Human Nature and the Need for Social Connection. Am. J. Psychiatry 2009, 166, 375–376. [Google Scholar] [CrossRef]
- Ponzetti, J.J. Loneliness among College Students. Fam. Relat. 1990, 39, 336–340. [Google Scholar] [CrossRef]
- Twenge, J.M.; Spitzberg, B.H.; Campbell, W.K. Less in-person social interaction with peers among U.S. adolescents in the 21st century and links to loneliness. J. Soc. Pers. Relatsh. 2019, 36, 1892–1913. [Google Scholar] [CrossRef]
- Rotenberg, K.J.; Hymel, S. Loneliness in Childhood and Adolescence; Cambridge University Press: Cambridge, UK, 1999. [Google Scholar]
- Orrego, V.O.; Rodriguez, J. Family Communication Patterns and College Adjustment: The Effects of Communication and Conflictual Independence on College Students. J. Fam. Commun. 2001, 1, 175–189. [Google Scholar] [CrossRef]
- Casey, B.J.; Duhoux, S.; Cohen, M.M. Adolescence: What Do Transmission, Transition, and Translation Have to Do with It? Neuron 2010, 67, 749–760. [Google Scholar] [CrossRef]
- Erzen, E.; Çikrikci, Ö. The effect of loneliness on depression: A meta-analysis. Int. J. Soc. Psychiatry 2018, 64, 427–435. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Boivin, M.; Hymel, S.; Bukowski, W.M. The roles of social withdrawal, peer rejection, and victimization by peers in predicting loneliness and depressed mood in childhood. Dev. Psychopathol. 1995, 7, 765–785. [Google Scholar] [CrossRef]
- Cruwys, T.; Dingle, G.A.; Haslam, C.; Haslam, S.A.; Jetten, J.; Morton, T.A. Social group memberships protect against future depression, alleviate depression symptoms and prevent depression relapse. Soc. Sci. Med. 2013, 98, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Toma, C.L.; Chen, J.; Shah, D.V.; Gustafson, D.; Mares, M.-L. Effects of Web-Based Social Connectedness on Older Adults’ Depressive Symptoms: A Two-Wave Cross-Lagged Panel Study. J. Med. Internet Res. 2021, 23, e21275. [Google Scholar] [CrossRef] [PubMed]
- Slavin, L.A.; Rainer, K.L. Gender differences in emotional support and depressive symptoms among adolescents: A prospective analysis. Am. J. Community Psychol. 1990, 18, 407–421. [Google Scholar] [CrossRef]
- Joiner, T.E.; Metalsky, G.I. A prospective test of an integrative interpersonal theory of depression: A naturalistic study of college roommates. J. Personal. Soc. Psychol. 1995, 69, 778–788. [Google Scholar] [CrossRef]
- Teo, A.R. Social isolation associated with depression: A case report of hikikomori. Int. J. Soc. Psychiatry 2013, 59, 339–341. [Google Scholar] [CrossRef]
- Robitaille, A.; Orpana, H.; McIntosh, C.N. Reciprocal Relationship between Social Support and Psychological Distress among a National Sample of Older Adults: An Autoregressive Cross-Lagged Model. Can. J. Aging-Rev. Can. Vieil 2012, 31, 13–24. [Google Scholar] [CrossRef]
- Van Bork, R.; Rhemtulla, M.; Waldorp, L.J.; Kruis, J.; Rezvanifar, S.; Borsboom, D. Latent Variable Models and Networks: Statistical Equivalence and Testability. Multivar. Behav. Res. 2021, 56, 175–198. [Google Scholar] [CrossRef]
- Bringmann, L.F.; Vissers, N.; Wichers, M.; Geschwind, N.; Kuppens, P.; Peeters, F.; Borsboom, D.; Tuerlinckx, F. A Network Approach to Psychopathology: New Insights into Clinical Longitudinal Data. PLoS ONE 2013, 8, e60188. [Google Scholar] [CrossRef]
- Epskamp, S.; van Borkulo, C.D.; van der Veen, D.C.; Servaas, M.N.; Isvoranu, A.-M.; Riese, H.; Cramer, A.O.J. Personalized Network Modeling in Psychopathology: The Importance of Contemporaneous and Temporal Connections. Clin. Psychol. Sci. 2018, 6, 416–427. [Google Scholar] [CrossRef]
- Pauley, G.; McPherson, S. The experience and meaning of compassion and self-compassion for individuals with depression or anxiety. Psychol. Psychother. Theory Res. Pract. 2010, 83, 129–143. [Google Scholar] [CrossRef] [PubMed]
- Neff, K.D.; McGehee, P. Self-compassion and Psychological Resilience Among Adolescents and Young Adults. Self Identity 2010, 9, 225–240. [Google Scholar] [CrossRef]
- MacBeth, A.; Gumley, A. Exploring compassion: A meta-analysis of the association between self-compassion and psychopathology. Clin. Psychol. Rev. 2012, 32, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Raes, F. The Effect of Self-Compassion on the Development of Depression Symptoms in a Non-clinical Sample. Mindfulness 2011, 2, 33–36. [Google Scholar] [CrossRef]
- Allen, A.B.; Leary, M.R. Self-Compassion, Stress, and Coping. Soc. Personal. Psychol. Compass 2010, 4, 107–118. [Google Scholar] [CrossRef]
- Yang, Y.; Guo, Z.; Kou, Y.; Liu, B. Linking Self-Compassion and Prosocial Behavior in Adolescents: The Mediating Roles of Relatedness and Trust. Child Indic. Res. 2019, 12, 2035–2049. [Google Scholar] [CrossRef]
- Inwood, E.; Ferrari, M. Mechanisms of Change in the Relationship between Self-Compassion, Emotion Regulation, and Mental Health: A Systematic Review. Appl. Psychol. Health Well-Being 2018, 10, 215–235. [Google Scholar] [CrossRef]
- Arch, J.J.; Brown, K.W.; Dean, D.J.; Landy, L.N.; Brown, K.D.; Laudenslager, M.L. Self-compassion training modulates alpha-amylase, heart rate variability, and subjective responses to social evaluative threat in women. Psychoneuroendocrinology 2014, 42, 49–58. [Google Scholar] [CrossRef]
- Krieger, T.; Altenstein, D.; Baettig, I.; Doerig, N.; Holtforth, M.G. Self-compassion in depression: Associations with depressive symptoms, rumination, and avoidance in depressed outpatients. Behav. Ther. 2013, 44, 501–513. [Google Scholar] [CrossRef]
- Lyubomirsky, S.; Nolen-Hoeksema, S. Effects of self-focused rumination on negative thinking and interpersonal problem solving. J. Personal. Soc. Psychol. 1995, 69, 176–190. [Google Scholar] [CrossRef]
- Zawadzki, M.J.; Graham, J.E.; Gerin, W. Rumination and anxiety mediate the effect of loneliness on depressed mood and sleep quality in college students. Health Psychol. 2013, 32, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yang, Y.; Wu, H.; Kong, X.; Cui, L. The roles of fear of negative evaluation and social anxiety in the relationship between self-compassion and loneliness: A serial mediation model. Curr. Psychol. 2022, 41, 5249–5257. [Google Scholar] [CrossRef]
- Akin, A. Self-compassion and Loneliness. Int. Online J. Educ. Sci. 2010, 2, 702–718. [Google Scholar]
- Kuyken, W.; Watkins, E.; Holden, E.; White, K.; Taylor, R.S.; Byford, S.; Evans, A.; Radford, S.; Teasdale, J.D.; Dalgleish, T. How does mindfulness-based cognitive therapy work? Behav. Res. Ther. 2010, 48, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, P. An Introduction to Compassion Focused Therapy in Cognitive Behavior Therapy. Int. J. Cogn. Ther. 2010, 3, 97–112. [Google Scholar] [CrossRef]
- Shapira, L.B.; Mongrain, M. The benefits of self-compassion and optimism exercises for individuals vulnerable to depression. J. Posit. Psychol. 2010, 5, 377–389. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F.; Segerstrom, S.C. Optimism. Clin. Psychol. Rev. 2010, 30, 879–889. [Google Scholar] [CrossRef]
- von Känel, R.; Weilenmann, S.; Spiller, T.R. Loneliness is associated with depressive affect, but not with most other symptoms of depression in community-dwelling individuals: A network analysis. Int. J. Environ. Res. Public Health. 2021, 18, 2408. [Google Scholar] [CrossRef]
- Owczarek, M.; Nolan, E.; Shevlin, M.; Butter, S.; Karatzias, T.; McBride, O.; Murphy, J.; Vallieres, F.; Bentall, R.; Martinez, A.; et al. How is loneliness related to anxiety and depression: A population-based network analysis in the early lockdown period. I Int. J. Psychol. 2022, 57, 585–596. [Google Scholar] [CrossRef]
- Ramos-Vera, C.; García O’Diana, A.; Basauri, M.D.; Calle, D.H.; Saintila, J. Psychological impact of COVID-19: A cross-lagged network analysis from the English Longitudinal Study of Aging COVID-19 database. Front. Psychiatry 2023, 14, 258. [Google Scholar] [CrossRef]
- Saltzman, L.Y.; Hansel, T.C.; Bordnick, P.S. Loneliness, isolation, and social support factors in post-COVID-19 mental health. Psychol. Trauma Theory Res. Pract. Policy 2020, 12 (Suppl. 1), S55–S57. [Google Scholar] [CrossRef] [PubMed]
- Neff, K.D. The Development and Validation of a Scale to Measure Self-Compassion. Self Identity 2003, 2, 223–250. [Google Scholar] [CrossRef]
- Chen, J.; Yan, L.; Zhou, L. Reliability and validity of Chinese version of Self-compassion Scale. Chin. J. Clin. Psychol. 2011, 19, 734–736. [Google Scholar]
- Chu, X.-W.; Fan, C.-Y.; Liu, Q.-Q.; Zhou, Z.-K. Cyberbullying victimization and symptoms of depression and anxiety among Chinese adolescents: Examining hopelessness as a mediator and self-compassion as a moderator. Comput. Hum. Behav. 2018, 86, 377–386. [Google Scholar] [CrossRef]
- Tao, Y.; Hou, W.; Niu, H.; Ma, Z.; Zheng, Z.; Wang, S.; Liu, X.; Zhang, L. Comparing the centrality symptoms of major depressive disorder samples across junior high school students, senior high school students, college students and elderly adults during city lockdown of COVID-19 pandemic—A network analysis. J. Affect. Disord. 2023, 324, 190–198. [Google Scholar] [CrossRef]
- Wang, S.; Hou, W.; Tao, Y.; Ma, Z.; Li, K.; Wang, Y.; Xu, Z.; Liu, X.; Zhang, L. Mapping network connection among symptoms of anxiety, depression, and sleep disturbance in Chinese high school students. Front. Public Health 2022, 10, 3389. [Google Scholar] [CrossRef]
- Hays, R.D.; DiMatteo, M.R. A Short-Form Measure of Loneliness. J. Personal. Assess 1987, 51, 69–81. [Google Scholar] [CrossRef]
- Wu, C.; Yao, G. Psychometric analysis of the short-form UCLA Loneliness Scale (ULS-8) in Taiwanese undergraduate students. Personal. Individ. Differ. 2008, 44, 1762–1771. [Google Scholar] [CrossRef]
- Epskamp, S.; Fried, E.I. A tutorial on regularized partial correlation networks. Psychol. Methods 2018, 23, 617–634. [Google Scholar] [CrossRef]
- Epskamp, S.; Waldorp, L.J.; Mõttus, R.; Borsboom, D. The Gaussian Graphical Model in Cross-Sectional and Time-Series Data. Multivar. Behav. Res. 2018, 53, 453–480. [Google Scholar] [CrossRef]
- Epskamp, S.; Cramer AO, J.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. qgraph: Network Visualizations of Relationships in Psychometric Data. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar] [CrossRef]
- Friedman, J.H.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Sánchez Hernández, M.O.; Carrasco, M.A.; Holgado-Tello, F.P. Anxiety and Depression Symptoms in Spanish Children and Adolescents: An Exploration of Comorbidity from the Network Perspective. Child Psychiatry Hum. Dev. 2021, 54, 736–749. [Google Scholar] [CrossRef]
- Stadje, R.; Dornieden, K.; Baum, E.; Becker, A.; Biroga, T.; Bösner, S.; Haasenritter, J.; Keunecke, C.; Viniol, A.; Donner-Banzhoff, N. The differential diagnosis of tiredness: A systematic review. BMC Fam. Pract. 2016, 17, 147. [Google Scholar] [CrossRef] [PubMed]
- Cheniaux, E.; Silva, R.D.A.D.; Santana, C.M.; Filgueiras, A. Changes in energy and motor activity: Core symptoms of bipolar mania and depression? Braz. J. Psychiatry 2017, 40, 233–237. [Google Scholar] [CrossRef]
- Akiskal, H.S.; McKinney, W.T., Jr. Overview of Recent Research in Depression: Integration of Ten Conceptual Models Into a Comprehensive Clinical Frame. Arch. Gen. Psychiatry 1975, 32, 285–305. [Google Scholar] [CrossRef]
- Bennabi, D.; Vandel, P.; Papaxanthis, C.; Pozzo, T.; Haffen, E. Psychomotor Retardation in Depression: A Systematic Review of Diagnostic, Pathophysiologic, and Therapeutic Implications. BioMed Res. Int. 2013, 2013, 158746. [Google Scholar] [CrossRef]
- Burton, C.; McKinstry, B.; Szentagotai Tătar, A.; Serrano-Blanco, A.; Pagliari, C.; Wolters, M. Activity monitoring in patients with depression: A systematic review. J. Affect. Disord. 2013, 145, 21–28. [Google Scholar] [CrossRef]
- Cheniaux, E.; Filgueiras, A.; da Silva, R.D.A.; Silveira, L.A.S.; Nunes, A.L.S.; Landeira-Fernandez, J. Increased energy/activity, not mood changes, is the core feature of mania. J. Affect. Disord. 2014, 152–154, 256–261. [Google Scholar] [CrossRef]
- Mickelson, K.D. Perceived Stigma, Social Support, and Depression. Personal. Soc. Psychol. Bull. 2001, 27, 1046–1056. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Fentem, P.H. ABC of Sports Medicine: Benefits of exercise in health and disease. BMJ 1994, 308, 1291–1295. [Google Scholar] [CrossRef] [PubMed]
- Page, R.M.; Hammermeister, J. Shyness and Loneliness: Relationship to the Exercise Frequency of College Students. Psychol. Rep. 1995, 76, 395–398. [Google Scholar] [CrossRef] [PubMed]
- Pels, F.; Kleinert, J. Loneliness and physical activity: A systematic review. Int. Rev. Sport Exerc. Psychol. 2016, 9, 231–260. [Google Scholar] [CrossRef]
- Gijzen MW, M.; Rasing SP, A.; Creemers DH, M.; Smit, F.; Engels RC, M.E.; De Beurs, D. Suicide ideation as a symptom of adolescent depression. A network analysis. J. Affect. Disord. 2021, 278, 68–77. [Google Scholar] [CrossRef]
- Andel, S.A.; Shen, W.; Arvan, M.L. Depending on your own kindness: The moderating role of self-compassion on the within-person consequences of work loneliness during the COVID-19 pandemic. J. Occup. Health Psychol. 2021, 26, 276–290. [Google Scholar] [CrossRef]
- Lyon, T. Self-Compassion as a Predictor of Loneliness: The Relationship Between Self-Evaluation Processes and Perceptions of Social Connection. Honors Theses, Southeastern University, Lakeland, FL, USA, 2015. Available online: https://firescholars.seu.edu/honors/37 (accessed on 31 May 2023).
- Marsh, I.C.; Chan SW, Y.; MacBeth, A. Self-compassion and Psychological Distress in Adolescents—A Meta-analysis. Mindfulness 2018, 9, 1011–1027. [Google Scholar] [CrossRef]
- Terry, M.L.; Leary, M.R. Self-compassion, self-regulation, and health. Self Identity 2011, 10, 352–362. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Kirtley, O.J. The integrated motivational–volitional model of suicidal behaviour. Philos. Trans. R. Soc. B Biol. Sci. 2018, 373, 20170268. [Google Scholar] [CrossRef]
- Tangney, J.P. The Self-Conscious Emotions: Shame, Guilt, Embarrassment and Pride. In Handbook of Cognition and Emotion; John Wiley & Sons Ltd.: Hoboken, NJ, USA,, 1999; pp. 541–568. [Google Scholar] [CrossRef]
- Rostami, S.; Jowkar, B. The relationship between guilt and shame feelings with the dimensions of loneliness: The moderating effect of gender. Int. J. Behav. Sci. 2016, 10, 24–28. [Google Scholar]
- Teroni, F.; Deonna, J.A. Differentiating shame from guilt. Conscious. Cogn. 2008, 17, 725–740. [Google Scholar] [CrossRef] [PubMed]
- Hedman, E.; Ström, P.; Stünkel, A.; Mörtberg, E. Shame and Guilt in Social Anxiety Disorder: Effects of Cognitive Behavior Therapy and Association with Social Anxiety and Depressive Symptoms. PLoS ONE 2013, 8, e61713. [Google Scholar] [CrossRef] [PubMed]
- Maner, J.K.; DeWall, C.N.; Baumeister, R.F.; Schaller, M. Does social exclusion motivate interpersonal reconnection? Resolving the “porcupine problem”. J. Personal. Soc. Psychol. 2007, 92, 42–55. [Google Scholar] [CrossRef]
- Twenge, J.M.; Baumeister, R.F.; DeWall, C.N.; Ciarocco, N.J.; Bartels, J.M. Social exclusion decreases prosocial behavior. J. Personal. Soc. Psychol. 2007, 92, 56–66. [Google Scholar] [CrossRef]
- Beckes, L.; Coan, J.A. Social Baseline Theory: The Role of Social Proximity in Emotion and Economy of Action. Soc. Personal. Psychol. Compass 2011, 5, 976–988. [Google Scholar] [CrossRef]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness Matters: A Theoretical and Empirical Review of Consequences and Mechanisms. Ann. Behav. Med. 2010, 40, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Pizzagalli, D.A. Depression, Stress, and Anhedonia: Toward a Synthesis and Integrated Model. Annu. Rev. Clin. Psychol. 2014, 10, 393–423. [Google Scholar] [CrossRef]
- Pillny, M.; Lincoln, T.M. The demotivating effect of social exclusion: An experimental test of a psychosocial model on the development of negative symptoms in psychosis. Schizophr. Res. 2020, 215, 330–336. [Google Scholar] [CrossRef]
- Barnard, L.K.; Curry, J.F. Self-Compassion: Conceptualizations, Correlates, & Interventions. Rev. Gen. Psychol. 2011, 15, 289–303. [Google Scholar] [CrossRef]
- Neff, K.D.; Vonk, R. Self-Compassion Versus Global Self-Esteem: Two Different Ways of Relating to Oneself. J. Personal. 2009, 77, 23–50. [Google Scholar] [CrossRef]
- Bloch, J. Self-Compassion, Social Connectedness, and Interpersonal Competence. Master’s Thesis, University of Montana, Missoula, MT, USA, 2018. Available online: https://scholarworks.umt.edu/etd/11224 (accessed on 31 May 2023).
- Gu, H.; Bao, X.; Xia, T. Basic psychological need frustration and adolescent non-suicidal self-injury: Testing a moderated mediation model of depression and self-compassion. Curr. Psychol. 2022. [Google Scholar] [CrossRef]
- Gilbert, P. The origins and nature of compassion focused therapy. Br. J. Clin. Psychol. 2014, 53, 6–41. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low-SC Group (N = 752) | High-SC Group (N = 750) | t-Test | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Skew | Kurtosis | Mean | SD | Skew | Kurtosis | p | Cohen’s d | ||
| T1 | PHQ1 | 1.54 | 0.76 | 1.51 | 2.05 | 1.36 | 0.62 | 1.76 | 3.05 | <0.001 | 0.25 |
| PHQ2 | 1.46 | 0.69 | 1.62 | 2.76 | 1.31 | 0.58 | 1.87 | 3.15 | <0.001 | 0.23 | |
| PHQ3 | 1.36 | 0.71 | 2.15 | 4.14 | 1.28 | 0.56 | 2.13 | 4.49 | 0.017 | 0.12 | |
| PHQ4 | 1.53 | 0.71 | 1.33 | 1.66 | 1.35 | 0.60 | 1.66 | 2.52 | <0.001 | 0.27 | |
| PHQ5 | 1.43 | 0.71 | 1.79 | 3.05 | 1.33 | 0.62 | 2.01 | 4.05 | 0.006 | 0.14 | |
| PHQ6 | 1.37 | 0.68 | 1.98 | 3.80 | 1.25 | 0.55 | 2.38 | 5.75 | <0.001 | 0.21 | |
| PHQ7 | 1.49 | 0.74 | 1.57 | 2.05 | 1.35 | 0.66 | 1.98 | 3.57 | <0.001 | 0.20 | |
| PHQ8 | 1.19 | 0.51 | 3.23 | 11.57 | 1.22 | 0.54 | 2.75 | 7.86 | 0.249 | −0.06 | |
| PHQ9 | 1.08 | 0.35 | 5.68 | 36.84 | 1.13 | 0.42 | 3.91 | 16.90 | 0.015 | −0.13 | |
| ULS1 | 2.19 | 0.95 | 0.12 | −1.12 | 1.72 | 0.87 | 0.76 | −0.79 | <0.001 | 0.52 | |
| ULS2 | 1.93 | 0.90 | 0.47 | −0.92 | 1.67 | 0.84 | 0.85 | −0.56 | <0.001 | 0.30 | |
| ULS3 | 0.60 | 0.78 | 1.29 | 1.27 | 1.18 | 1.18 | 0.51 | −1.25 | <0.001 | −0.58 | |
| ULS4 | 2.14 | 0.87 | 0.12 | −0.99 | 1.69 | 0.85 | 0.75 | −0.93 | <0.001 | 0.53 | |
| ULS5 | 2.21 | 0.90 | 0.05 | −1.01 | 1.74 | 0.86 | 0.62 | −1.10 | <0.001 | 0.54 | |
| ULS6 | 0.74 | 0.86 | 1.02 | 0.32 | 1.32 | 1.17 | 0.35 | −1.35 | <0.001 | −0.56 | |
| ULS7 | 2.01 | 0.92 | 0.42 | −0.89 | 1.74 | 0.87 | 0.76 | −0.65 | <0.001 | 0.30 | |
| ULS8 | 1.85 | 0.89 | 0.70 | −0.48 | 1.63 | 0.81 | 0.87 | −0.64 | <0.001 | 0.26 | |
| T2 | PHQ1 | 1.53 | 0.76 | 1.52 | 2.02 | 1.37 | 0.68 | 1.95 | 3.48 | <0.001 | 0.22 |
| PHQ2 | 1.39 | 0.63 | 1.78 | 3.42 | 1.30 | 0.59 | 2.09 | 4.28 | <0.001 | 0.14 | |
| PHQ3 | 1.48 | 0.78 | 1.73 | 2.46 | 1.40 | 0.77 | 2.04 | 3.51 | 0.017 | 0.10 | |
| PHQ4 | 1.56 | 0.77 | 1.45 | 1.93 | 1.38 | 0.67 | 1.89 | 3.43 | <0.001 | 0.25 | |
| PHQ5 | 1.43 | 0.77 | 1.88 | 2.84 | 1.32 | 0.64 | 2.17 | 4.51 | 0.006 | 0.15 | |
| PHQ6 | 1.34 | 0.67 | 2.18 | 4.66 | 1.26 | 0.59 | 2.54 | 6.58 | <0.001 | 0.13 | |
| PHQ7 | 1.37 | 0.69 | 1.92 | 3.23 | 1.28 | 0.60 | 2.25 | 4.69 | <0.001 | 0.15 | |
| PHQ8 | 1.21 | 0.55 | 2.94 | 9.07 | 1.20 | 0.52 | 2.98 | 9.63 | 0.249 | 0.02 | |
| PHQ9 | 1.13 | 0.47 | 4.07 | 17.85 | 1.16 | 0.48 | 3.45 | 12.93 | 0.015 | −0.06 | |
| ULS1 | 2.01 | 0.94 | 0.33 | −1.12 | 1.77 | 0.87 | 0.61 | −1.04 | <0.001 | 0.27 | |
| ULS2 | 1.89 | 0.89 | 0.49 | −0.93 | 1.70 | 0.85 | 0.76 | −0.77 | <0.001 | 0.21 | |
| ULS3 | 0.90 | 0.99 | 0.91 | −0.22 | 1.15 | 1.16 | 0.53 | −1.20 | <0.001 | −0.23 | |
| ULS4 | 2.01 | 0.90 | 0.29 | −1.12 | 1.77 | 0.87 | 0.61 | −1.04 | <0.001 | 0.27 | |
| ULS5 | 2.08 | 0.91 | 0.14 | −1.23 | 1.77 | 0.86 | 0.55 | −1.17 | <0.001 | 0.34 | |
| ULS6 | 0.96 | 1.00 | 0.75 | −0.55 | 1.26 | 1.17 | 0.38 | −1.35 | <0.001 | −0.28 | |
| ULS7 | 2.05 | 0.94 | 0.37 | −0.97 | 1.82 | 0.92 | 0.69 | −0.76 | <0.001 | 0.25 | |
| ULS8 | 1.84 | 0.87 | 0.61 | −0.73 | 1.68 | 0.84 | 0.81 | −0.68 | <0.001 | 0.19 | |
| Edge Invariance | Global Invariance | |
|---|---|---|
| High-SC—low-SC (first time) | M = 0.35 | S = 0.67 |
| p < 0.001 | p = 0.002 | |
| High-SC—low-SC (second time) | M = 0.17 | S = 0.22 |
| p = 0.51 | p = 0.16 | |
| High-SC (longitudinal) | M = 0.38 | S = 0.54 |
| p < 0.001 | p = 0.006 | |
| Low-SC (longitudinal) | M = 0.26 | S = 0.08 |
| p = 0.03 | p = 0.57 |
| EI (First Time) | EI (Second Time) | OEI | IEI | |
|---|---|---|---|---|
| High-SC group | 0.595 | 0.439 | 0.263 | 0.407 |
| Low-SC group | 0.439 | 0.594 | 0.364 | 0.379 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, S.; Tang, Q.; Lv, Y.; Tao, Y.; Liu, X.; Zhang, L.; Liu, G. The Temporal Relationship between Depressive Symptoms and Loneliness: The Moderating Role of Self-Compassion. Behav. Sci. 2023, 13, 472. https://doi.org/10.3390/bs13060472
Wang S, Tang Q, Lv Y, Tao Y, Liu X, Zhang L, Liu G. The Temporal Relationship between Depressive Symptoms and Loneliness: The Moderating Role of Self-Compassion. Behavioral Sciences. 2023; 13(6):472. https://doi.org/10.3390/bs13060472
Chicago/Turabian StyleWang, Shujian, Qihui Tang, Yichao Lv, Yanqiang Tao, Xiangping Liu, Liang Zhang, and Gang Liu. 2023. "The Temporal Relationship between Depressive Symptoms and Loneliness: The Moderating Role of Self-Compassion" Behavioral Sciences 13, no. 6: 472. https://doi.org/10.3390/bs13060472
APA StyleWang, S., Tang, Q., Lv, Y., Tao, Y., Liu, X., Zhang, L., & Liu, G. (2023). The Temporal Relationship between Depressive Symptoms and Loneliness: The Moderating Role of Self-Compassion. Behavioral Sciences, 13(6), 472. https://doi.org/10.3390/bs13060472