


Development and Validation of Standardized Quality of Life Measures for Persons with IDD
 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. The Quality of Life Model
2.1. The Concept of Quality of Life
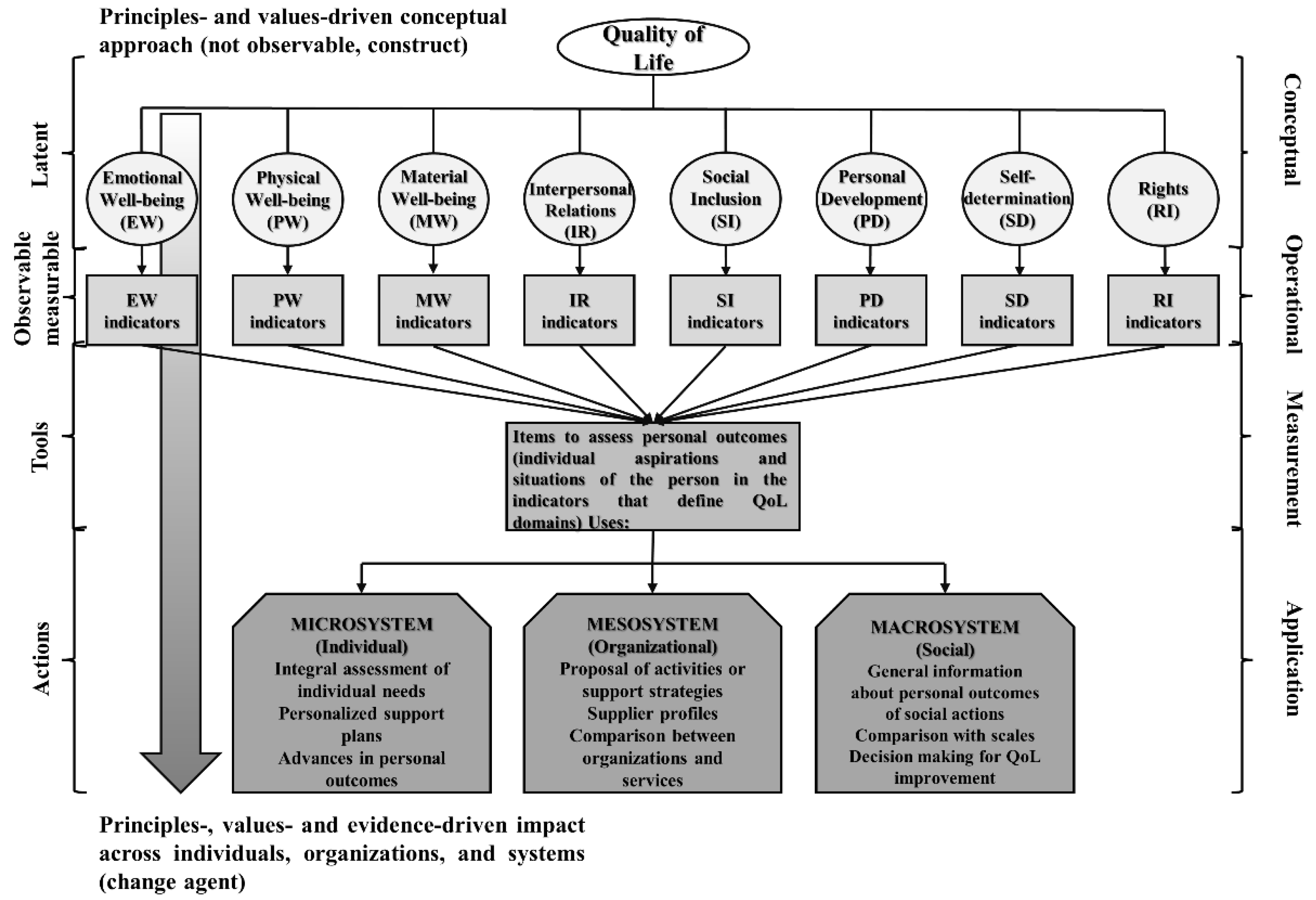
2.2. The Quality of Life Model as an Applied Framework: Measurement Framework and Change Agent
2.2.1. Quality of Life Model as a Measurement Framework
2.2.2. Quality of Life Model as a Change Agent
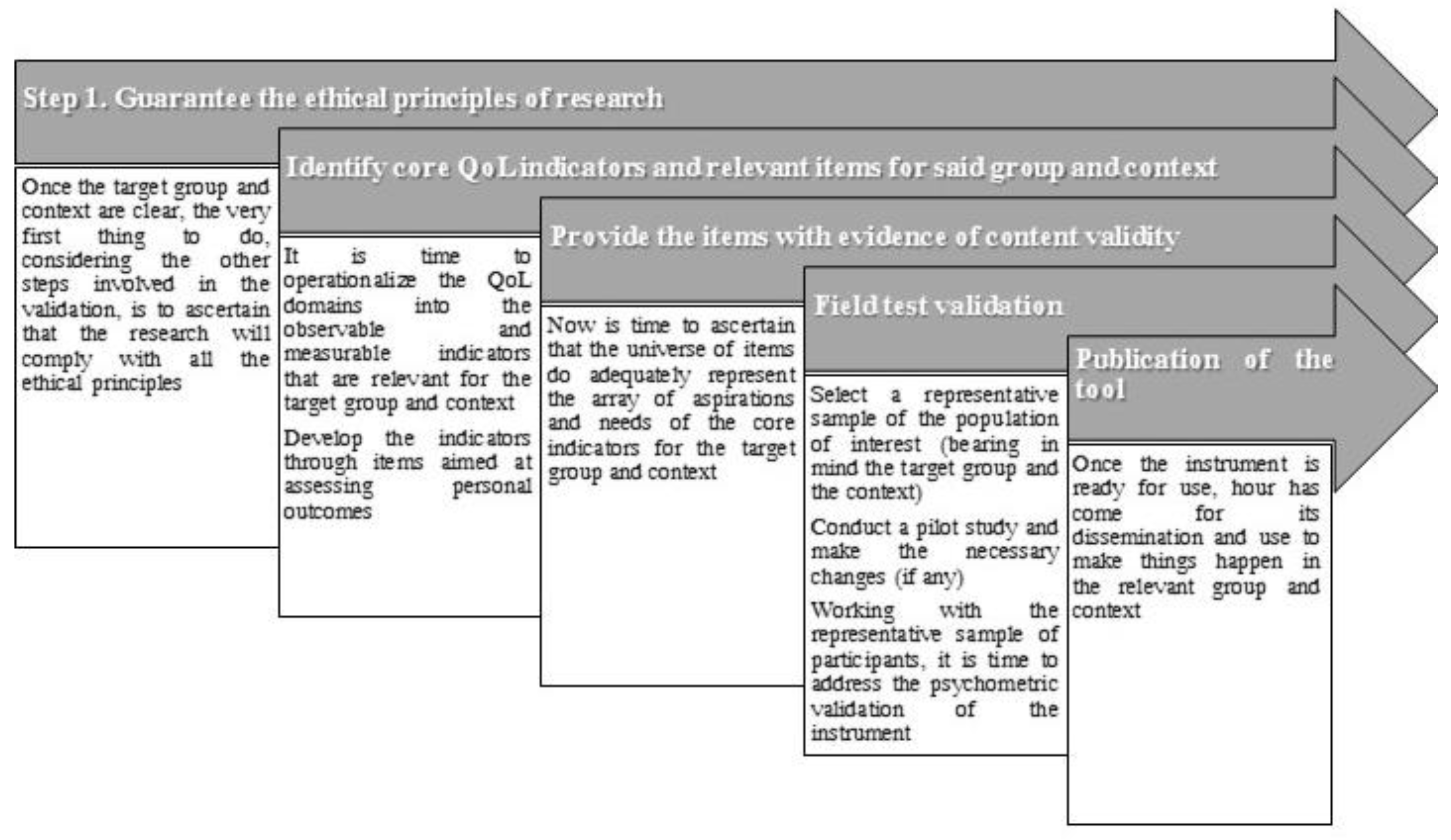
3. Development and Validation of Quality of Life Standardized Measures
3.1. Step 1. Guaranteeing the Ethical Principles of Research
3.2. Step 2. Identifying the Core Quality of Life Indicators and Relevant Items for the Group and Context of Interest
3.3. Providing the Items with Validity Evidence Based on Content
3.4. Field Test Validation
3.4.1. Selection of Participants
3.4.2. Pilot Study
3.4.3. Administration of the Instrument and Analyses of Its Psychometric Properties
- The psychometric properties of the items are used to select a maximum number of items with the best properties for each QoL domain. For this, five criteria are considered [42]: (a) The mean value of the scores for each of the items and their standard deviation; (b) the number of missing data; (c) the corrected homogeneity indexes; (d) the distribution of the responses and (e) the content of the items.
- Regarding the analyses of the evidence of validity and reliability, validity analyses must focus, above all, on validity evidence based on internal structure (i.e., analyzing the structure of the tool using confirmatory factor analysis) and on validity evidence in relation to other variables. Reliability must consider at least an internal consistency coefficient (e.g., Cronbach’s alpha, ordinal alpha, or Omega coefficient) and, if possible, the inter-rater reliability (e.g., through intraclass correlation coefficient) [53,54,55,56,57,58].
3.5. Publication of the Tool
4. Using the Tool: Assessment of Personal Outcomes and Uses of the Information Gathered
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. Convention on the Rights of Persons with Disabilities. 2006. Available online: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities/convention-on-the-rights-of-persons-with-disabilities-2.html (accessed on 18 April 2023).
- Courtenay, K.; Perera, B. COVID-19 and people with intellectual disability: Impacts of a pandemic. Ir. J. Psychol. Med. 2020, 37, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Crespo, M.; Verdugo, M.Á.; Navas, P.; Martínez, T.; Amor, A.M. Impact of COVID-19 on people with intellectual and developmental disabilities, their families, support professionals and organizations. Siglo Cero. 2021, 52, 11–36. (In Spanish) [Google Scholar]
- Amor, A.M.; Hagiwara, M.; Shogren, K.A.; Thompson, J.R.; Verdugo, M.Á.; Burke, K.M.; Aguayo, V. International perspectives and trends in research on inclusive education: A systematic review. Int. J. Incl. Educ. 2019, 23, 1277–1295. [Google Scholar] [CrossRef]
- Hagiwara, M.; Amor, A.M.; Shogren, K.A.; Thompson, J.R.; Verdugo, M.Á.; Burke, K.M.; Uyanik, K.; Aguayo, V. International trends in inclusive education intervention research: A literature review. Educ. Train. Autism Dev. Disabil. 2019, 54, 3–17. [Google Scholar]
- Schalock, R.L.; Verdugo, M.Á. Handbook on Quality of Life for Human Service Practitioners; American Association on Mental Retardation: Washington, DC, USA, 2002. [Google Scholar]
- Alcedo, M.Á.; Aguado, A.L.; Arias, B.; González, M.; Rozada, C. Quality of Life Scale for persons with disabilities who are ageing: Preliminary study. Interv. Psicosoc. 2008, 17, 153–167. (In Spanish) [Google Scholar]
- Van Hecke, N.; Claes, C.; Vanderplasschen, W.; De Maeyer, J.; De Witte, N.; Vandevelde, S. Conceptualisation and measurement of quality of life based on Schalock and Verdugo’s model: A cross-disciplinary review of the literature. Soc. Indic. Res. 2018, 137, 335–351. [Google Scholar] [CrossRef]
- Amor, A.M.; Fernández, M.; Verdugo, M.Á.; Aza, A.; Schalock, R.L. Shaping the faces of the prism: Rights, supports, and quality of life for enhancing inclusive education opportunities in students with intellectual disability. In Inclusive Education: Unity in Diversity; Glodkowska, J., Ed.; Akademia Pedagogiki Specjalnej: Warsaw, Poland, 2020; pp. 58–88. [Google Scholar]
- Fernández, M. Assessment of Quality of Life in Persons with Acquired Brain Injury. Ph.D. Thesis, University of Salamanca, Salamanca, Spain, 2019. [Google Scholar]
- Schalock, R.L.; Gardner, J.F.; Bradley, V.J. Quality of Life for People with Intellectual and Other Developmental Disabilities: Applications across Individuals, Organizations, Communities, and Systems; American Association on Intellectual and Developmental Disabilities: Washington, DC, USA, 2007. [Google Scholar]
- Schalock, R.L.; Verdugo, M.Á.; Jenaro, C.; Wang, M.; Wehmeyer, M.L.; Jiancheng, X.; Lachapelle, Y. Cross-cultural study of quality of life indicators. Am. J. Ment. Retard. 2005, 110, 298–311. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Schalock, R.L.; Verdugo, M.Á.; Jenaro, C. Examining the factor structure and hierarchical nature of the quality of life construct. Am. J. Intellect. Dev. Disabil. 2010, 115, 218–233. [Google Scholar] [CrossRef] [PubMed]
- Heras, I.; Amor, A.M.; Verdugo, M.Á.; Calvo, M.I. Operasionalisation of quality of life for students with intellectual and developmental disabilities to improve their inclusion. Res. Dev. Disabil. 2021, 119, 104093. [Google Scholar] [CrossRef] [PubMed]
- Gómez, L.E.; Monsalve, A.; Morán, M.L.; Alcedo, M.Á.; Lombardi, M.; Schalock, R.L. Measurable indicators of CRPD for people with intellectual and developmental disabilities within the quality of life framework. Int. J. Environ. Res. Public Health 2020, 17, 5123. [Google Scholar] [CrossRef]
- Gómez, L.E.; Morán, M.L.; Al-Halabí, S.; Swerts, C.; Verdugo, M.Á.; Schalock, R.L. Quality of life and the International Convention on the Rights of Persons with Disabilities: Consensus indicators for assessment. Psicothema 2022, 34, 182–191. [Google Scholar] [PubMed]
- Sabeh, E.N.; Verdugo, M.Á.; Prieto, G.; Contini, E.N. CVI-CVIP: Quality of Life Assessment Questionnaire in Childhood; CEPE: Madrid, Spain, 2009. (In Spanish) [Google Scholar]
- Gómez-Vela, M.; Verdugo, M.Á. CCVA: Questionnaire for Assessing Quality of Life in Adolescent Students; CEPE: Madrid, Spain, 2009. (In Spanish) [Google Scholar]
- Gómez, L.E.; Alcedo, M.Á.; Verdugo, M.Á.; Arias, B.; Fontanil, Y.; Arias, V.B.; Monsalve, A.; Morán, M.L. KidsLife Scale: Assessment of Quality of Life of Children and Adolescents with Intellectual Disability; Publicaciones INICO: Salamanca, Spain, 2016. (In Spanish) [Google Scholar]
- Gómez, L.E.; Verdugo, M.Á.; Rodríguez, M.; Arias, B.; Morán, M.L.; Mosalve, A.; Fontanil, Y. KidsLife-Down Scale: Assessment of Quality of Life of Children and Adolescents with Down Syndrome; Publicaciones INICO: Salamanca, Spain, 2017. (In Spanish) [Google Scholar]
- Gómez, L.E.; Morán, M.L.; Alcedo, M.Á.; Verdugo, M.Á.; Arias, V.B.; Fontanil, Y.; Monsalve, A. KidsLife-TEA Scale: Assessment of Quality of Life of Children and Adolescents with Autism Spectrum Disorder and Intellectual Disability; Publicaciones INICO: Salamanca, Spain, 2018. (In Spanish) [Google Scholar]
- Verdugo, M.Á.; Gómez, L.E.; Arias, B. Assessment of Quality of Life in Elder Population: FUMAT Scale; Publicaciones INICO: Salamanca, Spain, 2009. (In Spanish) [Google Scholar]
- Verdugo, M.Á.; Arias, B.; Gómez, L.E.; Schalock, R.L. GENCAT Scale Quality of Life Assessment Form; GENCAT Scale Quality of Life Assessment User’s Manual; Departament d’Acció Social i Ciutadania, Generalitat de Catalunya: Barcelona, Spain, 2009. (In Spanish) [Google Scholar]
- Verdugo, M.Á.; Gómez, L.E.; Arias, B.; Schalock, R.L. Integral Scale. In Objective and Subjective Assessment of Quality of Life of Persons with Intellectual Disability; CEPE: Madrid, Spain, 2009. (In Spanish) [Google Scholar]
- Verdugo, M.Á.; Gómez, L.E.; Arias, B.; Santamaría, M.; Clavero, D.; Tamarit, J. INICO-FEAPS Scale: Integral Assessment of Quality of Life of Persons with Intellectual or Developmental Disability; Publicaciones INICO: Salamanca, Spain, 2013. (In Spanish) [Google Scholar]
- Verdugo, M.Á.; Gómez, L.E.; Arias, B.; Santamaría, M.; Navallas, E.; Fernández, S.; Hierro, I. San Martín Scale: Quality of Life Assessment for Persons with Significant Disabilities; Fundación Obra San Martín: Santander, Spain, 2014. [Google Scholar]
- Verdugo, M.Á.; Gómez, L.E.; Fernández, M.; Aguayo, V.; Arias, B. CAVIDACE Scale of Assessment of Quality of Life; User’s Manual; Publicaciones INICO: Salamanca, Spain, 2018. (In Spanish) [Google Scholar]
- Verdugo, M.Á.; Aza, A.; Orgaz, M.B.; Fernández, M.; Gómez, L.E.; Amor, A.M. CAVIDACE Scale: Assessment of Quality of Life of Persons with Brain Injury; Self-report; Publicaciones INICO: Salamanca, Spain, 2020. (In Spanish) [Google Scholar]
- Henao, C.P.; Verdugo, M.Á.; Córdoba, L. Colombian Version of the INICO-FEAPS Scale for the Assessment of Quality of Life in Persons with Intellectual Disability; Publicaciones INICO: Salamanca, Spain, 2017. (In Spanish) [Google Scholar]
- Stone, M.M.; Kash, S.; Butler, T.; Callahan, K.; Verdugo, M.Á.; Gómez, L.E. Validation of English language adaptations of the KidsLife and San Martín Scale for assessing quality of life with individuals on the autism spectrum receiving residential care. J. Dev. Phys. Disabil. 2020, 32, 131–154. [Google Scholar] [CrossRef]
- Amor, A.M.; Verdugo, M.Á. Quality of life and its role for guiding practices in the social and educational services from a systems perspective. Men Disabil. Soc. 2018, 41, 15–27. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Gómez, L.E.; Peña, E.; Arias, B.; Verdugo, M.Á. Impact of individual and organizational variables on quality of life. Soc. Indic. Res. 2016, 125, 649–664. [Google Scholar] [CrossRef]
- Schalock, R.L.; Verdugo, M.Á. The impact of the quality of life concept on the field of intellectual disability. In The Oxford Handbook of Positive Psychology and Disability; Wehmeyer, M.L., Ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- European Association of Service Providers for Persons with Disabilities. Inclusive Education: The Way Forward. IE+ Policy Recommendations. Available online: https://www.easpd.eu/fileadmin/user_upload/Projects/4.25_Policy_Recommendations_FINAL.pdf (accessed on 17 April 2023).
- Balboni, G.; Coscarelli, A.; Giunti, G.; Schalock, R.L. The assessment of quality of life of adults with intellectual disability: The use of self-report and report of others assessment strategies. Res. Dev. Disabil. 2013, 34, 4248–4254. [Google Scholar] [CrossRef] [PubMed]
- Arscott, K.; Dagnan, D.; Kroese, B.S. Consent to psychological research by people with an intellectual disability. J. Appl. Res. Intellect. Disabil. 1998, 11, 77–83. [Google Scholar] [CrossRef]
- Cleaver, S.; Ouelette-Kuntz, H.; Sakar, A. Participation in intellectual disability research: A review of 20 years of studies. J. Intellect. Disabil. Res. 2010, 54, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Iacono, T.; Murray, V. Issues of informed consent in conducting medical research involving people with intellectual disability. J. Appl. Res. Intellect. Disabil. 2003, 16, 41–51. [Google Scholar] [CrossRef]
- McDonald, K.E.; Conroy, N.E.; Olick, R.S. Is it worth it? Benefits in research with adults with intellectual disability. Intellect. Dev. Disabil. 2016, 54, 440–453. [Google Scholar] [CrossRef]
- Minkler, M.; Fadem, P.; Perry, M.; Blum, K.; Moore, L.; Rogers, J. Ethical dilemmas in participatory action research: A case study from the disability community. Health Educ. Behav. 2002, 29, 14–29. [Google Scholar] [CrossRef]
- Fernández, M.; Verdugo, M.Á.; Gómez, L.E.; Aguayo, V.; Arias, B. Core indicators to assess quality of life in population with brain injury. Soc. Indic. Res. 2018, 137, 813–828. [Google Scholar] [CrossRef]
- Gómez, L.E.; Arias, B.; Verdugo, M.Á.; Tassé, M.J.; Brown, I. Operationalisation of quality of life for adults with severe disabilities. J. Intellect. Disabil. Res. 2015, 59, 925–941. [Google Scholar] [CrossRef] [PubMed]
- Reguant-Álvarez, M.; Torrado-Fonseca, M. The Delphi method. Rev. Innov. Recer. Educ. 2016, 9, 87–102. (In Spanish) [Google Scholar]
- Popham, W.J. The seductive allure of data. Educ. Leadersh. 2003, 60, 48–51. [Google Scholar]
- Bangdiwala, K. Using SAS software graphical procedures for the observer agreement chart. In Proceedings of the 12 SAS Users Group International Conference, Dallas, TX, USA, 8–11 February 1987. [Google Scholar]
- Muñiz, J.; Fonseca-Pedrero, E. Ten steps for test development. Psicothema 2019, 31, 7–16. (In Spanish) [Google Scholar]
- Cochran, W.G. Sampling Techniques, 3rd ed.; John Wiley & Sons: New York, NY, USA, 1977; pp. 72–88. [Google Scholar]
- Marrugat, J.; Vila, J.; Pavesi, M. Maximum uncertainty principle: Absolute or relative error in the sample size calculation? Gac. Sanit. 1999, 13, 491–492. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Suárez, P.; Alonso, J.C. On the maximum uncertainty principle, sample size and other sampling considerations. Gac. Sanit. 1999, 13, 243–246. (In Spanish) [Google Scholar]
- Ferrando, P.J.; Anguiano, C. Factorial analysis as a research technique in psychology. Papeles Psicol. 2010, 31, 18–33. (In Spanish) [Google Scholar]
- Verdugo, M.Á.; Schalock, R.L.; Gómez, L.E.; Arias, B. Development of context-focused multidimensional quality of life scales: The Gencat Scale. Siglo Cero. 2007, 38, 57–72. (In Spanish) [Google Scholar]
- American Educational Research Association; American Psychological Association; National Council on Measurement in Education. Standards for Educational and Psychological Testing: National Council on Measurement in Education, 7th ed.; American Educational Research Association: Washington, DC, USA, 2014. [Google Scholar]
- McCoach, D.B.; Gable, R.K.; Madura, J.P. Instrument Development in the Affective Domain, 3rd ed.; Springer: New York, NY, USA, 2013; pp. 209–248. [Google Scholar]
- Prieto, G.; Delgado, A.R. Reliability and validity. Papeles Psicol. 2010, 31, 67–74. (In Spanish) [Google Scholar]
- Rios, J.; Wells, C. Validity evidence based on internal structure. Psicothema 2014, 26, 108–116. [Google Scholar] [PubMed]
- Sierci, S.; Faulkner-Bond, M. Validity evidence based on test content. Psicothema 2014, 26, 100–107. [Google Scholar]
- Thompson, J.R.; Schalock, R.L.; Tassé, M.J. Evidence for the Reliability and Validity of the Supports Intensity Scales. Available online: https://www.aaidd.org/docs/default-source/sis-docs/evidence-for-the-reliabilityandvalidity-of-the-sis.pdf?sfvrsn=7ed3021_0 (accessed on 18 April 2023).
- International Test Commission. The ICT Guidelines for Translating and Adapting Tests. Available online: https://www.intestcom.org/files/guideline_test_adaptation_2ed.pdf (accessed on 18 April 2023).



{kind=link}
{kind=link}
| QoL Domain | Description | Indicators for People with IDD | Rights Aligned |
|---|---|---|---|
| EW | To be calm and safe, relaxed, and not to be overwhelmed and nervous | Satisfaction, self-concept, self-esteem, positive feelings, and lack of distress or negative feelings | Arts. 16 (freedom from exploitation, violence, and abuse) and 17 (protecting the integrity of the person) |
| IR | Having relations with different people, having clearly identified friends, and getting on well with others (acquaintances, neighbors, partners, etc.) | Social interactions, having identified friends, familiar interactions and relations, positive social contacts, relationships, communication, and sexuality | Art. 23 (respect for home and the family) |
| MW | Having enough money to buy whatever one needs and/or wants, having a proper household or workplace, having access to adequate services | Housing, workplace, employment status, salary (pension, income), belongings, savings, material goods, and access to services | Arts. 27 (work and employment) and 28 (adequate standard of living and social protection) |
| PD | Having the possibility of learning different things, accessing knowledge, developing new skills and personal competence (cognitive, social, and practical), and having the possibility of self-realization | Limitations/capacities, access to information and communication technologies, teaching-learning opportunities, educational status, work-related skills (or other activities), and functional abilities | Art. 24 (education) |
| PW | Being healthy, feeling fit, having good healthy habits | Health status, health care, healthy habits (e.g., rest and sleep, hygiene, eating or physical exercise), and activities of daily living (e.g., self-care, mobility) | Arts. 25 (health) and 26 (habilitation and rehabilitation) |
| SD | Being able to self-decide and having the opportunities to choose the things that one considers relevant according to one’s own values and beliefs, choosing one’s life, employment, leisure time, living, and the people to be with | Goals and personal values, decisions and choices, and autonomy/personal control | Arts. 14 (liberty and security of person) and 21 (freedom of expression and opinion, and access to information) |
| SI | Going to different places in the city or neighborhood where other people go, participating in different activities on equal foot with others, performing an active role in the community, and feeling part of society and having the support of others | Inclusion, participation, accessibility, supports, recognition, and community roles | Arts. 8 (awareness-raising), 9 (accessibility), 18 (liberty of movement and nationality), 19 (living independently and being included in the community), 20 (Personal mobility), 29 (participation in political and public life), and 30 (participation in cultural life, recreation, leisure and sport) |
| RI | Being considered and treated equally with other people, including having access to the same opportunities, being respected (i.e., personality, opinions, wishes, privacy, etc.), and knowledge of one’s own rights and exercise of them | Respect, intimacy, confidentiality, knowledge and exercise of rights (e.g., respect, dignity, equality), and legal guarantees (e.g., access or due process) | Arts. 5 (equality and non-discrimination), 6 (women with disabilities), 7 (children with disabilities), 10 (right to life), 11 (situations of risk and humanitarian emergencies), 12 (equal recognition before law), 13 (access to justice), 15 (freedom from torture or cruel, inhuman or degrading treatment or punishment), and 22 (respect for privacy) |
| Assessment Instrument | Target Group | Assessment Approach |
|---|---|---|
| CVI-CVIP: Quality of life Assessment Questionnaire in Childhood [17] | Children with and without special educational needs aged 8–11 years | Self-report and report of others |
| CCVA: Questionnaire for Assessing Quality of Life in Adolescent Students [18] | Adolescents with and without special educational needs between 12 and 18 years old | Report of others |
| KidsLife [19] | Children, adolescents, and youth with IDD | Report of others |
| KidsLife-Down [20] | Children, adolescents, and youth with Down syndrome | Report of others |
| KidsLife TEA [21] | Children, adolescents, and youth with autism spectrum disorder and ID | Report of others |
| FUMAT Scale [22] | Elderly persons recipient of social services | Report of others |
| GENCAT Scale [23] | Adults who receive social services | Report of others |
| Integral Scale [24] | Adults with IDD | Self-report and report of others |
| INICO-FEAPS Scale [25] | Adults with IDD | Self-report and report of others |
| San Martin Scale [26] | Adults with IDD and extensive and pervasive support needs | Report of others |
| CAVIDACE Scale [27] | Adults with brain injury | Report of others |
| CAVIDACE Scale—Self report version [28] | Adults with brain injury | Self-report |
| Quality of Life Index for Inclusive Education—Primary Education Version [14] | Students with IDD, behavioral and emotional concerns, and learning difficulties enrolled in primary, general education (6–12 years old) | Report of others |
| Property | Source | Interpretation Foundations |
|---|---|---|
| Reliability: Consistency or stability of measurements when the measurement process is repeated | Internal consistency reliability: Extent to which the items correlate with one another | Strong correlations indicate that an assessment scale’s items have a robust relationship with one another and are, therefore, measuring different aspects of the same construct |
| Split half reliability: Linear relationship between half of the items on a scale with the other half | A high correlation between the two halves suggests that items on the scale are measuring the same construct | |
| Test-retest reliability: Evaluates the consistency of a scale score over short periods of time | Strong correlations between scores from two separate and independent administrations completed following the same conditions at different time points suggest that the construct being assessed is stable | |
| Interrater reliability: Consistency of scale scores across assessors | If two separate and independent administrations of an assessment involve different evaluators and the correlations found between the scores in the two administrates are high, then the outcomes of the measure are trustworthy regardless of the administrator | |
| Validity: Refers to the degree to which evidence and theory support interpretations of test scores for intended uses of the tests | Evidence based on content: The extent to which the items on an assessment adequately represent the universe of items that could be associated with the construct of interest | Content validity should be established when the measure is developed, when subscales are conceptualized, and items are written. Foundations are provided in Section 3.3 |
| Evidence based on internal structure: The degree to which the relationships between the items and test components conform to the construct on which the proposed interpretations of test scores are based | Support for a standardized instrument’s internal structure comes from research findings that demonstrate a strong relationship between the construct being measured and an assessment scale’s test items and the subscale scores. Statistical analyses revealing that the items share variance in ways that match the defined construct reflect positively on an instrument’s internal structure | |
| Evidence based on relation to other variables: The extent to which test-derived scores are related to measures of other variables that are theoretically associated (directly or inversely) with the construct assessed by the test | Evidence based on relation to other variables is established by collecting data that show that constructs that theoretically should be related are, in fact, related. The expected relationships may be of different types. For example, the traditionally called “convergent validity” focuses on convergent relationships. Convergent evidence provides support that a measure is correlated with other variables that claim to measure the same (or a similar) construct. Conversely, evidence on discriminate validity is established when gathering evidence that shows that constructs that theoretically should have no relationship with one another, in fact, have low correlations. In some cases, the instrument may be designed to predict a future characteristic or behavior. The test-criterion relationship may be assessed at the same time (concurrent), for example, by comparing two key groups that the instrument should identify as different, or by assessing the relationship of the instrument to a variable assessed at a later time (predictive) | |
| External validity: Refers to the extent to which results from a study using the tool can be generalized to other settings and people | It is important to assess the extent to which the scores obtained through the implementation of said instrument maintain evidence of good validity and reliability when applied to other settings and people, or in other countries and languages |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amor, A.M.; Verdugo, M.Á.; Fernández, M.; Aza, A.; Sánchez-Gómez, V.; Wolowiec, Z. Development and Validation of Standardized Quality of Life Measures for Persons with IDD. Behav. Sci. 2023, 13, 452. https://doi.org/10.3390/bs13060452
Amor AM, Verdugo MÁ, Fernández M, Aza A, Sánchez-Gómez V, Wolowiec Z. Development and Validation of Standardized Quality of Life Measures for Persons with IDD. Behavioral Sciences. 2023; 13(6):452. https://doi.org/10.3390/bs13060452
Chicago/Turabian StyleAmor, Antonio M., Miguel Á. Verdugo, María Fernández, Alba Aza, Victoria Sánchez-Gómez, and Zofia Wolowiec. 2023. "Development and Validation of Standardized Quality of Life Measures for Persons with IDD" Behavioral Sciences 13, no. 6: 452. https://doi.org/10.3390/bs13060452
APA StyleAmor, A. M., Verdugo, M. Á., Fernández, M., Aza, A., Sánchez-Gómez, V., & Wolowiec, Z. (2023). Development and Validation of Standardized Quality of Life Measures for Persons with IDD. Behavioral Sciences, 13(6), 452. https://doi.org/10.3390/bs13060452