
Relationship between Perceived Pain Interference and Poor Psychological Wellbeing among United States Adults



Abstract
1. Introduction
2. Methods
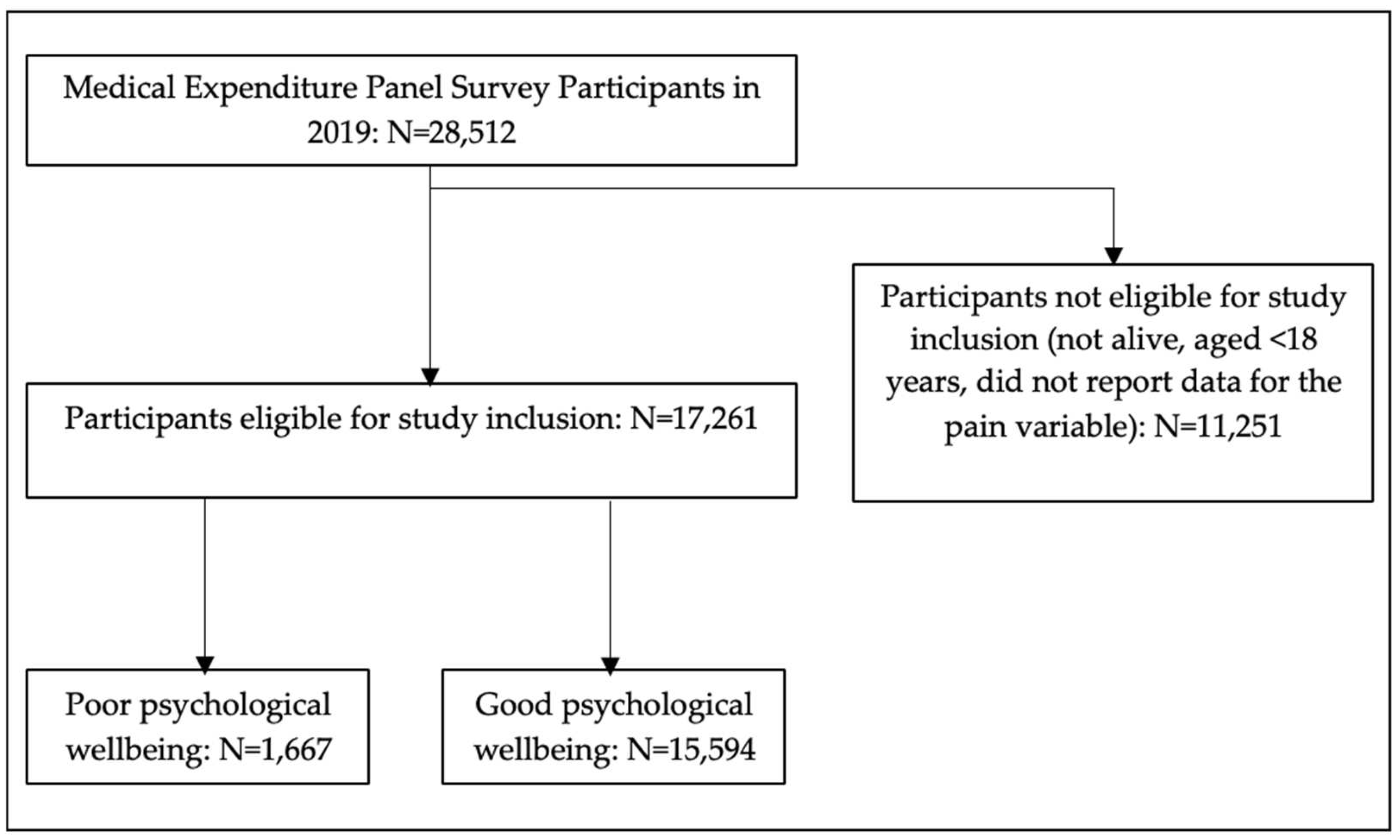
2.1. Study Design, Data Source, and Study Participants
2.2. Independent Variable
2.3. Control Variables
2.4. Dependent Variable
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- About Mental Health. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/mentalhealth/learn/index.htm (accessed on 7 September 2022).
- The state of Mental Health in America. Available online: https://www.mhanational.org/issues/state-mental-health-america (accessed on 7 September 2022).
- Adult Data. 2022. Available online: https://www.mhanational.org/issues/2022/mental-health-america-adult-data#:~:text=Adult%20Prevalence%20of%20Mental%20Illness%20(AMI)%202022&text=19.86%25%20of%20adults%20are%20experiencing,Jersey%20to%2026.86%25%20in%20Utah (accessed on 7 September 2022).
- CDC Museum COVID-19 Timeline. Available online: https://www.cdc.gov/museum/timeline/covid19.html#:~:text=March%2011%2C%202020,declares%20COVID%2D19%20a%20pandemic (accessed on 7 September 2022).
- Howe, C.Q.; Sullivan, M.D. The missing ‘P’ in pain management: How the current opioid epidemic highlights the need for psychiatric services in chronic pain care. Gen. Hosp. Psychiatry 2014, 36, 99–104. [Google Scholar] [CrossRef] [PubMed]
- IASP Announces Revised Definition of Pain. Available online: https://www.iasp-pain.org/publications/iasp-news/iasp-announces-revised-definition-of-pain/ (accessed on 7 September 2022).
- Vadivelu, N.; Kai, A.M.; Kodumudi, G.; Babayan, K.; Fontes, M.; Burg, M.M. Pain and Psychology—A Reciprocal Relationship. Ochsner J. 2017, 17, 173–180. [Google Scholar] [PubMed]
- Prevalence of Chronic Pain and High-Impact Chronic Pain among Adults—United States. 2016. Available online: https://www.cdc.gov/mmwr/volumes/67/wr/mm6736a2.htm#:~:text=An%20estimated%2020.4%25%20(50.0%20million,adults%2C%20adults%20living%20in%20poverty%2C (accessed on 7 September 2022).
- Axon, D.R.; Bhattacharjee, S.; Warholak, T.L.; Slack, M.K. Xm2 scores for estimating total exposure to multimodal strategies identified by Pharmacists for managing pain: Validity testing and clinical relevance. Pain Res. Manag. 2018, 2018, 2530286. [Google Scholar] [CrossRef] [PubMed]
- Axon, D.R.; Patel, M.J.; Martin, J.R.; Slack, M.K. Use of multidomain management strategies by community dwelling adults with chronic pain: Evidence from a systematic review. Scand. J. Pain 2019, 19, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Hooten, W.M. Chronic Pain and Mental Health Disorders: Shared Neural Mechanisms, Epidemiology, and Treatment. Mayo Clin. Proc. 2019, 91, 955–970. [Google Scholar] [CrossRef]
- Goesling, J.; Lin, L.A.; Clauw, D.J. Psychiatry and Pain Management: At the Intersection of Chronic Pain and Mental Health. Curr. Psychiatry Rep. 2019, 20, 12. [Google Scholar] [CrossRef]
- Axon, D.R.; Chien, J. Predictors of Mental Health Status among Older United States Adults with Pain. Behav. Sci. 2021, 11, 23. [Google Scholar] [CrossRef]
- Axon, D.R.; Chien, J. Assessing healthcare expenditures of older United States adults with pain and poor vs. good mental health status: A cross-sectional study. BMJ Open 2022, 12, e049727. [Google Scholar] [CrossRef]
- Medical Expenditure Panel Survey Background. Available online: https://meps.ahrq.gov/data_stats/download_data/pufs/h216/h216cb.pdf (accessed on 7 September 2022).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2018, 61, 344–349. [Google Scholar] [CrossRef]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef]
- Björnsdóttir, S.V.; Jónsson, S.H.; Valdimarsdóttir, U.A. Mental health indicators and quality of life among individuals with musculoskeletal chronic pain: A nationwide study in Iceland. Scand. J. Rheumatol. 2014, 43, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Serbic, D.; Zhao, J.; He, J. The role of pain, disability and perceived social support in psychological and academic functioning of university students with pain: An observational study. Int. J. Adolesc. Med. Health 2020, 33, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Elkana, O.; Conti, Y.; Heyman, O.; Hamdan, S.; Franko, M.; Vatine, J.J. The associations between executive functions and different aspects of perceived pain, beyond the influence of depression, in rehabilitation setting. Neuropsychol. Rehabil. 2020, 30, 1303–1317. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.H.; Stevens, C.; Wong, S.; Yasui, M.; Chen, J.A. The prevalence and predictors of mental health diagnoses and suicide among U.S. college students: Implications for addressing disparities in service use. Depress. Anxiety 2019, 36, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Cook, B.L.; Trinh, N.H.; Li, Z.; Hou, S.S.; Progovac, A.M. Trends in Racial-Ethnic Disparities in Access to Mental Health Care, 2004–2012. Psychiatr. Serv. 2017, 68, 9–16. [Google Scholar] [CrossRef]
- Desai, M.U.; Paranamana, N.; Restrepo-Toro, M.; O’Connell, M.; Davidson, L.; Stanhope, V. Implicit organizational bias: Mental health treatment culture and norms as barriers to engaging with diversity. Am. Psychol. 2021, 76, 78–90. [Google Scholar] [CrossRef]
- Shields-Zeeman, L.; Collin, D.F.; Batra, A.; Hamad, R. How does income affect mental health and health behaviors? A quasi-experimental study of the earned income tax credit. J. Epidemiol. Community Health 2021, 75, 929–935. [Google Scholar] [CrossRef]
- Tibber, M.S.; Walji, F.; Kirkbride, J.B.; Huddy, V. The association between income inequality and adult mental health at the subnational level-a systematic review. Soc. Psychiatry Psychiatr. Epidemiol. 2022, 57, 1–24. [Google Scholar] [CrossRef]
- Lee, D.C.; Liang, H.; Shi, L. The convergence of racial and income disparities in health insurance in the United States. Int. J. Equity Health 2021, 20, 96. [Google Scholar] [CrossRef]
- Jun, H.; Aguila, E. Private Insurance and Mental Health among Older Adults with Multiple Chronic Conditions: A Longitudinal Analysis by Race and Ethnicity. Int. J. Environ. Res. Public Health 2021, 18, 2615. [Google Scholar] [CrossRef]
- Blunt, E.O.; Maclean, J.C.; Popovici, I.; Marcus, S.C. Public insurance expansions and mental health care availability. Health Serv. Res. 2020, 55, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.; Griffith, L.E.; Gruneir, A.; Kanters, D.; Markle-Reid, M.; Ploeg, J. Functional limitations in people with multimorbidity and the association with mental health conditions: Baseline data from the Canadian Longitudinal Study on Aging (CLSA). PLoS ONE 2021, 16, e0255907. [Google Scholar] [CrossRef] [PubMed]
- Portela, D.; Almada, M.; Midão, L.; Costa, E. Instrumental Activities of Daily Living (iADL) Limitations in Europe: An Assessment of SHARE Data. Int. J. Environ. Res. Public Health 2020, 17, 7387. [Google Scholar] [CrossRef] [PubMed]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Taylor, G.; McNeill, A.; Girling, A.; Farley, A.; Lindson-Hawley, N.; Aveyard, P. Change in mental health after smoking cessation: Systematic review and meta-analysis. BMJ 2014, 348, g1151. [Google Scholar] [CrossRef]
- Fiske, A.; Wetherell, J.L.; Gatz, M. Depression in older adults. Annu. Rev. Clin. Psychol. 2019, 5, 363–389. [Google Scholar] [CrossRef]
- Kamiya, Y.; Doyle, M.; Henretta, J.C.; Timonen, V. Depressive symptoms among older adults: The impact of early and later life circumstances and marital status. Aging Ment. Health 2013, 17, 349–357. [Google Scholar] [CrossRef]
- Siva Kumar, F.D.; Vaingankar, J.A.; Sambasivam, R.; Abdin, E.; Jeyagurunathan, A.; Seow, E.; Picco, L.; Chong, S.A.; Subramaniam, M. Marital Status and Positive Mental Health of Psychiatric Outpatients. Ann. Acad. Med. Singap. 2019, 48, 429–434. [Google Scholar] [CrossRef]
- Nam, G.E.; Eum, M.J.; Huh, Y.; Jung, J.H.; Choi, M.J. The Association Between Employment Status and Mental Health in Young Adults: A Nationwide Population-Based Study in Korea. J. Affect. Disord. 2021, 295, 1184–1189. [Google Scholar] [CrossRef]
- Arias-de la Torre, J.; Molina, A.J.; Fernández-Villa, T.; Artazcoz, L.; Martín, V. Mental health, family roles and employment status inside and outside the household in Spain. Gac. Sanit. 2019, 33, 235–241. [Google Scholar] [CrossRef]
- Ohrnberger, J.; Fichera, E.; Sutton, M. The relationship between physical and mental health: A mediation analysis. Soc. Sci. Med. 1982, 195, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Meyer, O.L.; Castro-Schilo, L.; Aguilar-Gaxiola, S. Determinants of mental health and self-rated health: A model of socioeconomic status, neighborhood safety, and physical activity. Am. J. Public Health 2014, 104, 1734–1741. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total n = 17,261 Weighted Percent (95% CI) | Poor Psychological Wellbeing n = 1667 Weighted Percent (95% CI) | Good Psychological Wellbeing n = 15,594. Weighted Percent (95% CI) | p |
|---|---|---|---|---|
| Pain interference: | <0.0001 | |||
| Extreme | 2.0(1.8, 2.3) | 10.1 (8.5,11.9) | 1.3 (1.1, 1.5) | |
| Quite a bit | 5.8 (5.4, 6.2) | 18.9 (16.8, 21.0) | 4.6 (4.2, 5.0) | |
| Moderate | 7.2 (6.7, 7.7) | 13.5 (11.6, 15.3) | 6.7 (6.2, 7.1) | |
| Little | 21.5 (20.7, 22.2) | 23.8 (21.5, 26.1) | 21.2 (20.5, 22.0) | |
| No pain | 63.5 (62.5, 64.4) | 33.7 (30.7, 36.6) | 66.2 (65.2, 67.2) | |
| Predisposing: | ||||
| Age (years) | 0.0012 | |||
| ≥65 | 21.1 (20.2, 22.1) | 25.3 (22.7, 27.9) | 20.8 (19.8, 21.7) | |
| 40–64 | 41.2 (40.2, 42.2) | 39.8 (37.0, 42.5) | 41.3 (40.3, 42.3) | |
| 18–39 | 37.6 (36.6, 38.7) | 35.0 (31.9, 38.0) | 37.9 (36.8, 39.0) | |
| Sex | <0.0001 | |||
| Male | 48.3 (47.7, 48.9) | 42.6 (39.7, 45.4) | 48.8 (48.2, 49.4) | |
| Female | 51.7 (51.1, 52.3) | 57.4 (54.6, 60.3) | 51.2 (50.6, 51.8) | |
| Race | 0.6259 | |||
| White | 77.9 (76.4, 79.4) | 78.5 (75.9, 81.1) | 77.9 (76.3, 79.4) | |
| Not white | 22.1 (20.6, 23.6) | 21.5 (18.9, 24.1) | 22.1 (20.6, 23.7) | |
| Ethnicity | 0.8514 | |||
| Hispanic | 16.6 (14.9, 18.3) | 16.4 (13.6, 19.1) | 16.6 (14.9, 18.3) | |
| Not Hispanic | 83.4 (81.7, 85.1) | 83.6 (80.9, 86.4) | 83.4 (81.7, 85.1) | |
| Enabling: | ||||
| Marriage status | <0.0001 | |||
| Married | 52.1 (50.9, 53.3) | 37.2 (34.0, 40.5) | 53.5 (52.3, 54.6) | |
| Other | 47.9 (46.7, 49.1) | 62.8 (59.5, 66.0) | 46.5 (45.4, 47.7) | |
| Income status | <0.0001 | |||
| Poor/low | 26.1 (24.9, 27.4) | 46.0 (42.3, 49.7) | 24.3 (23.1, 25.6) | |
| Moderate/high | 73.9 (72.6, 75.1) | 54.0 (50.3, 57.7) | 75.7 (74.4, 76.9) | |
| Education status | <0.0001 | |||
| Up to and including high school | 39.5 (38.0, 41.1) | 52.6 (49.4, 55.9) | 38.3 (36.8, 39.8) | |
| More than high school | 60.5 (58.9, 62.0) | 47.4 (44.1, 50.6) | 61.7 (60.2, 63.1) | |
| Employment status | <0.0001 | |||
| Employed | 68.0 (67.0, 69.0) | 46.7 (43.4, 50.0) | 70.0 (69.0, 71.0) | |
| Not employed | 32.0 (31.0, 33.0) | 53.3 (50.0, 56.6) | 30.0 (29.0, 31.0) | |
| Health insurance | <0.0001 | |||
| Private | 68.8 (67.4, 70.3) | 49.2 (45.8, 52.6) | 70.6 (69.3, 72.0) | |
| Public | 23.6 (22.5, 24.8) | 45.0 (41.7, 48.3) | 21.7 (20.6, 22.7) | |
| Not insured | 7.5 (6.7, 8.3) | 5.8 (4.3, 7.2) | 7.7 (6.8, 8.5) | |
| Need: | ||||
| IADL Limitation | <0.0001 | |||
| Yes | 3.2 (2.9, 3.5) | 15.7 (13.6, 17.7) | 2.0 (1.8, 2.3) | |
| No | 96.8 (96.5, 97.1) | 84.3 (82.3, 86.4) | 98.0 (97.7, 98.2) | |
| ADL Limitation | <0.0001 | |||
| Yes | 1.9 (1.6, 2.1) | 10.3 (8.6, 12.0) | 1.1 (0.9, 1.3) | |
| No | 98.1 (97.9, 98.4) | 89.7 (88.0, 91.4) | 98.9 (98.7, 99.1) | |
| Number of chronic diseases | <0.0001 | |||
| ≥2 | 42.0 (41.0, 43.1) | 63.6 (60.7, 66.5) | 40.1 (39.0, 41.1) | |
| <2 | 58.0 (56.9, 59.0) | 36.4 (33.5, 39.3) | 59.9 (58.9, 61.0) | |
| Overall health | <0.0001 | |||
| Good | 88.1 (87.4, 88.8) | 40.8 (37.6, 43.9) | 92.4 (91.9, 92.9) | |
| Poor | 11.9 (11.2, 12.6) | 59.2 (56.1, 62.4) | 7.6 (7.1, 8.1) | |
| Regular exercise | <0.0001 | |||
| Yes | 51.0 (49.8, 52.2) | 31.2 (28.3, 34.0) | 52.8 (51.6, 54.0) | |
| No | 49.0 (47.8, 50.2) | 68.8 (66.0, 71.7) | 47.2 (46.0, 48.4) | |
| Smoking status | <0.0001 | |||
| Yes | 14.0 (13.2, 14.9) | 24.2 (21.5, 27.0) | 13.1 (12.3, 13.9) | |
| No | 86.0 (85.1, 86.8) | 75.8 (73.0, 78.5) | 86.9 (86.1, 87.7) |
| Factor | Model 1 OR (95% CI) | Model 2 OR (95% CI) | Model 3 OR (95% CI) | Model 4 OR (95% CI) |
|---|---|---|---|---|
| Pain interference: | ||||
| Extreme | 15.4 (12.2, 19.5) | 18.5 (14.7, 23.3) | 11.3 (8.9, 14.4) | 2.0(1.4, 2.9) |
| Quite a bit | 8.1 (6.7, 9.8) | 9.7 (7.9, 12.0) | 7.0 (5.6, 8.6) | 2.3 (1.8, 2.9) |
| Moderate | 4.0 (3.3, 4.8) | 4.7 (3.9, 5.7) | 3.8 (3.1, 4.6) | 1.8 (1.4, 2.3) |
| Little | 2.2 (1.9, 2.6) | 2.4 (2.1, 2.9) | 2.3 (2.0, 2.7) | 1.6 (1.3, 1.9) |
| No pain | Reference | |||
| Predisposing: | ||||
| Age (years) | ||||
| ≥65 | 0.6 (0.5, 0.7) | 0.5 (0.4, 0.6) | 0.4 (0.3, 0.5) | |
| 40–64 | 0.7 (0.6, 0.8) | 0.7 (0.6, 0.9) | 0.5 (0.5, 0.7) | |
| 18–39 | Reference | |||
| Sex | ||||
| Male | 0.9 (0.8, 1.0) | 0.9 (0.8, 1.1) | 0.9 (0.8, 1.0) | |
| Female | Reference | |||
| Race | ||||
| White | 1.0 (0.9, 1.2) | 1.2 (1.0, 1.5) | 1.3 (1.1, 1.6) | |
| Not white | Reference | |||
| Ethnicity | ||||
| Hispanic | 1.2 (1.0, 1.4) | 1.0 (0.8, 1.2) | 1.0 (0.8, 1.2) | |
| Not Hispanic | Reference | |||
| Enabling: | ||||
| Marriage status | ||||
| Married | 0.6 (0.6, 0.7) | 0.7 (0.6, 0.8) | ||
| Other | Reference | |||
| Income status | ||||
| Poor/low | 1.4 (1.2, 1.7) | 1.3 (1.1, 1.5) | ||
| Moderate/high | Reference | |||
| Education status | ||||
| Up to and including high school | 1.2 (1.0, 1.3) | 1.1 (0.9, 1.3) | ||
| More than high school | Reference | |||
| Employment status | ||||
| Employed | 0.6 (0.5, 0.7) | 0.8 (0.7, 1.0) | ||
| Not employed | Reference | |||
| Health insurance status | ||||
| Private | 1.2 (0.9, 1.6) | 1.2 (0.9, 1.6) | ||
| Public | 1.8 (1.3, 2.4) | 1.5 (1.1, 2.0) | ||
| not insured | Reference | |||
| Need: | ||||
| IADL Limitation | ||||
| Yes | 1.8 (1.3, 2.4) | |||
| No | Reference | |||
| ADL Limitation | ||||
| Yes | 1.8 (1.3, 2.6) | |||
| No | Reference | |||
| Number of chronic diseases | ||||
| ≥2 | 1.3 (1.0, 1.6) | |||
| <2 | Reference | |||
| Overall health | ||||
| Good | 0.1 (0.1, 0.1) | |||
| Poor | Reference | |||
| Regular exercise | ||||
| Yes | 0.7 (0.6, 0.8) | |||
| No | Reference | |||
| Smoking status | ||||
| Yes | 1.3 (1.1, 1.6) | |||
| No | Reference | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Axon, D.R.; Kim, A. Relationship between Perceived Pain Interference and Poor Psychological Wellbeing among United States Adults. Behav. Sci. 2023, 13, 240. https://doi.org/10.3390/bs13030240
Axon DR, Kim A. Relationship between Perceived Pain Interference and Poor Psychological Wellbeing among United States Adults. Behavioral Sciences. 2023; 13(3):240. https://doi.org/10.3390/bs13030240
Chicago/Turabian StyleAxon, David R., and Ann Kim. 2023. "Relationship between Perceived Pain Interference and Poor Psychological Wellbeing among United States Adults" Behavioral Sciences 13, no. 3: 240. https://doi.org/10.3390/bs13030240
APA StyleAxon, D. R., & Kim, A. (2023). Relationship between Perceived Pain Interference and Poor Psychological Wellbeing among United States Adults. Behavioral Sciences, 13(3), 240. https://doi.org/10.3390/bs13030240