
Depression and Anxiety among Undergraduate Health Science Students: A Scoping Review of the Literature



Abstract
:1. Introduction
2. Methods
2.1. Searching for Relevant Studies
2.2. Study Selection
2.3. Data Charting and Extraction Process
2.4. Collating, Summarizing, and Reporting the Results
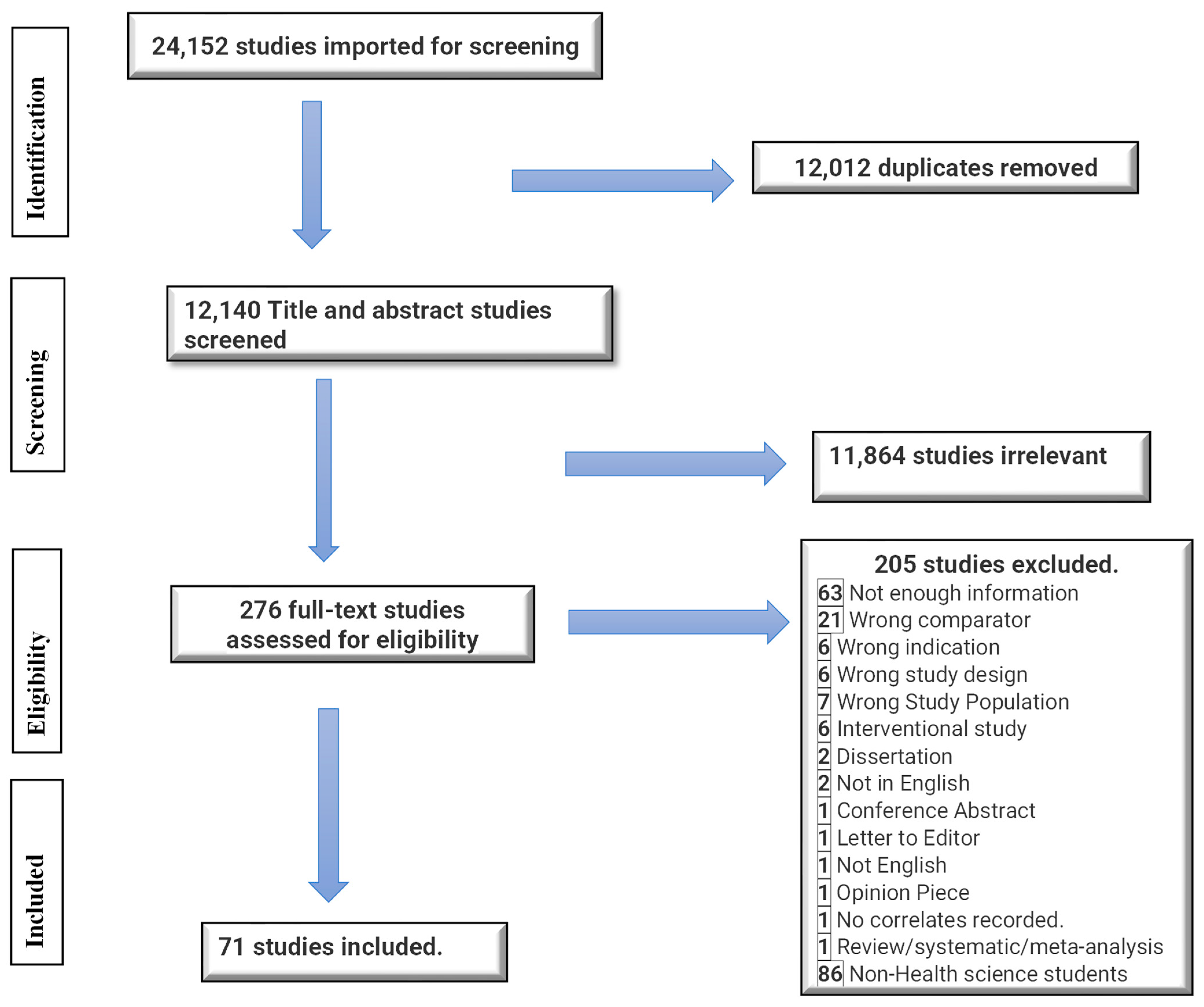
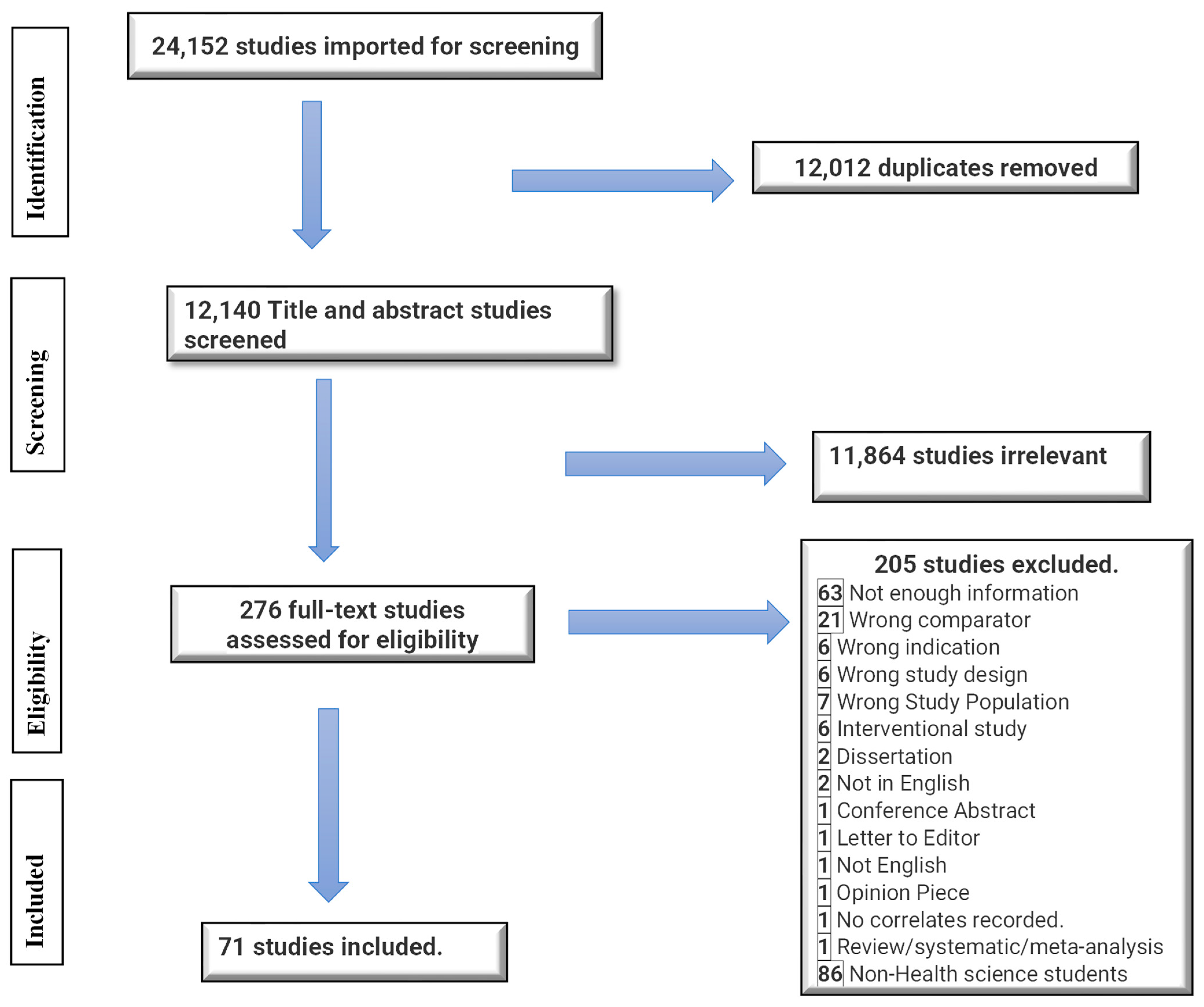
3. Results
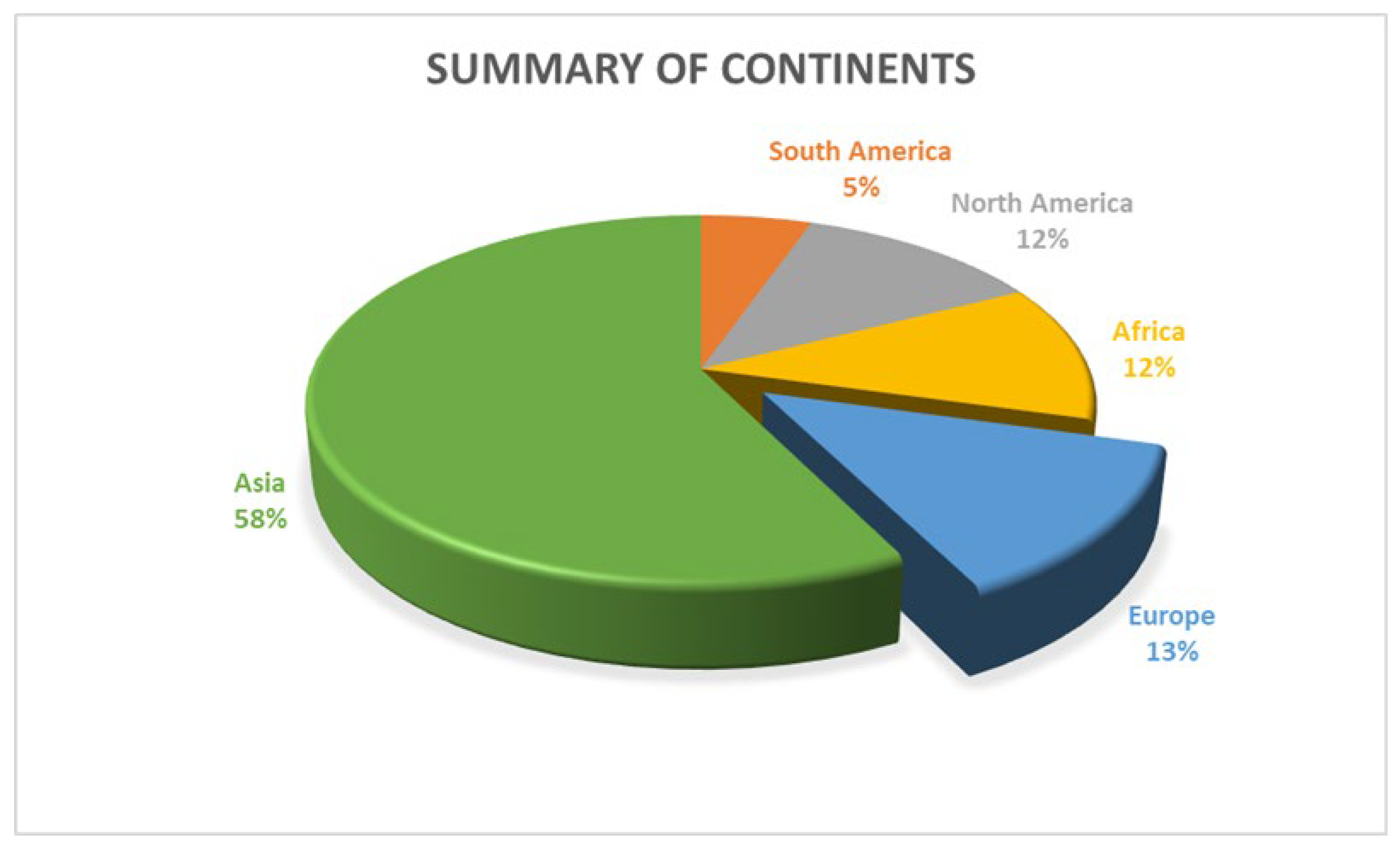
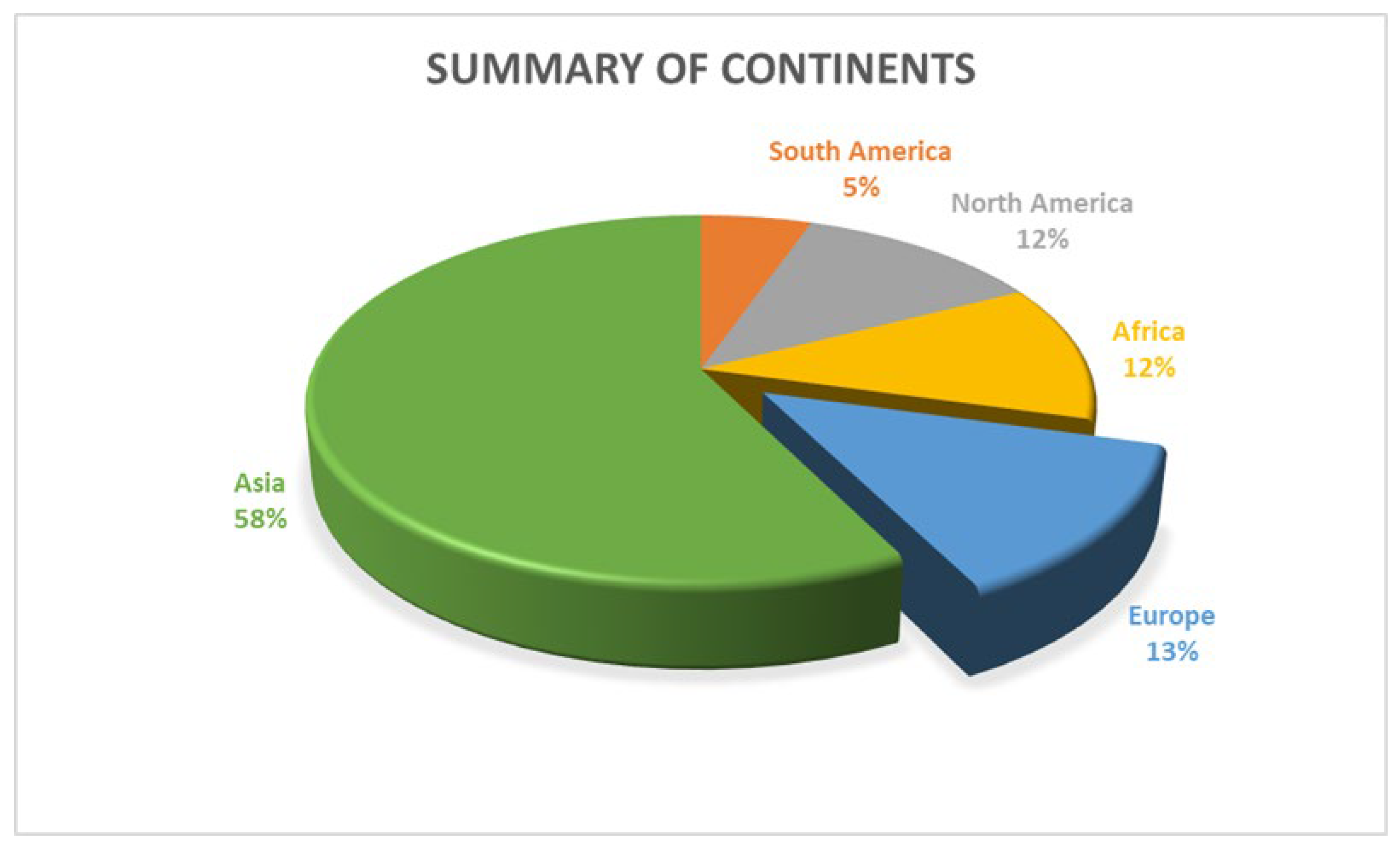
3.1. Study Characteristics
3.2. Number of Studies and Scales Used
3.3. Prevalence and Correlates of Anxiety and Depression
4. Discussion
4.1. Prevalence and Correlates of Anxiety and Depression among Health Science Students
4.2. Sociodemographic Correlates of Anxiety and Depression among Health Science Students
4.3. Personal and Health Conditions as Correlates of Anxiety and Depression
4.4. Academic-Related Issues as Predictors of Anxiety and Depression
4.5. Limitations of the Scoping Review
5. Conclusions and Implications for Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| depress*.mp.KL | |
| limit 1 to yr | 2017–2022 |
| anxiety*.mp. | |
| limit 3 to yr | 2017–2022 |
| 2 or 4 | |
| college student*.mp. | |
| limit 6 to yr | 2017–2022 |
| university student*.mp. | |
| limit 8 to yr | 2017–2022 |
| undergraduate student*.mp. | |
| limit 10 to yr | 2017–2022 |
| post-secondary student*.mp. | |
| limit 12 to yr | 2017–2022 |
| tertiary student*.mp. | |
| limit 14 to yr | 2017–2022 |
| 7 or 9 or 11 or 13 or 15 | |
| prevalence*.mp. | |
| limit 17 to yr | 2017–2022 |
| correlate*.mp. | |
| limit 19 to yr | 2017–2022 |
| determinant*.mp. | |
| limit 21 to yr | 2017–2022 |
| relat*.mp. | |
| limit 23 to yr | 2017–2022 |
| incidence*.mp. | |
| limit 25 to yr | 2017–2022 |
| 18 or 20 or 22 or 24 or 26 | |
| 5 and 16 and 2 |
References
- Richards, D.; Duffy, D.; Blackburn, B.; Earley, C.; Enrique, A.; Palacios, J.; Franklin, M.; Clarke, G.; Sollesse, S.; Connell, S.; et al. Digital IAPT: The effectiveness & cost-effectiveness of internet-delivered interventions for depression and anxiety disorders in the Improving Access to Psychological Therapies programme: Study protocol for a randomised control trial. BMC Psychiatry 2018, 18, 59. [Google Scholar]
- American Psychiatric Association. What Is Depression? APA: Washington, DC, USA, 2023. [Google Scholar]
- American Psychiatric Association. What Are Anxiety Disorders? APA: Washington, DC, USA, 2023. [Google Scholar]
- Langlois, S.; Morrison, P. Suicide deaths and suicide attempts. Health Rep. 2002, 13, 9–22. [Google Scholar]
- Agyapong, B.; Shalaby, R.; Eboreime, E.; Wei, Y.; Agyapong, V.I.O. Self-Reported Alcohol Abuse and the Desire to Receive Mental Health Counselling Predict Suicidal Thoughts/Thoughts of Self-Harm among Female Residents of Fort McMurray. Int. J. Env. Res. Public Health 2022, 19, 13620. [Google Scholar] [CrossRef]
- Abed, H.A.; Abd-Elraouf, M.S.E.D. Stress, Anxiety, Depression Among Medical Undergraduate Students at Benha University and Their Socio-Demographic Correlates. Egypt. J. Hosp. Med. 2022, 86, 27–32. [Google Scholar] [CrossRef]
- Shawahna, R.; Hattab, S.; Al-Shafei, R.; Tab’ouni, M. Prevalence and factors associated with depressive and anxiety symptoms among Palestinian medical students. BMC Psychiatry 2020, 20, 244. [Google Scholar] [CrossRef]
- Regehr, C.; Glancy, D.; Pitts, A. Interventions to reduce stress in university students: A review and meta-analysis. J. Affect. Disord. 2013, 148, 1–11. [Google Scholar] [CrossRef]
- Macaskill, A. The mental health of university students in the United Kingdom. Br. J. Guid. Couns. 2013, 41, 426–441. [Google Scholar] [CrossRef]
- Hakami, R.M. Prevalence of Psychological Distress among Undergraduate Students at Jazan University: A Cross-Sectional Study. Saudi J. Med. Med. Sci. 2018, 6, 82–88. [Google Scholar] [CrossRef]
- Yadav, R.; Gupta, S.; Malhotra, A.K. A cross sectional study on depression, anxiety and their associated factors among medical students in Jhansi, Uttar Pradesh, India. Int. J. Community Med. Public Health 2016, 3, 1209–1214. [Google Scholar] [CrossRef]
- Axelson, D.A.; Birmaher, B. Relation between anxiety and depressive disorders in childhood and adolescence. Depress. Anxiety 2001, 14, 67–78. [Google Scholar] [CrossRef]
- Ramón-Arbués, E.; Gea-Caballero, V.; Granada-López, J.M.; Juárez-Vela, R.; Pellicer-García, B.; Antón-Solanas, I. The prevalence of depression, anxiety and stress and their associated factors in college students. Int. J. Environ. Res. Public Health 2020, 17, 7001. [Google Scholar] [CrossRef]
- Gupta, P.B.K.A.; Ramakrishna, K. Prevalence of Depression and Anxiety Among Medical Students and House Staff During the COVID-19 Health-Care Crisis. Acad. Psychiatry 2021, 45, 575–580. [Google Scholar] [CrossRef]
- Ahad, A.; Chahar, P.; Haque, E.; Bey, A.; Jain, M.; Raja, W. Factors affecting the prevalence of stress, anxiety, and depression in undergraduate Indian dental students. J. Educ. Health Promot. 2021, 10, 266. [Google Scholar] [PubMed]
- Nebhinani, M.; Parihar, A.; Kumar, A.A.G.; Nebhinani, N.; Rani, R. COVID-19-induced anxiety and protective behaviour among nursing students: A survey from western India. J. Family Med. Prim. Care 2021, 10, 4483–4488. [Google Scholar] [CrossRef]
- Boolani, A.; Yager, C.; Reid, J.; Lackman, J.; Smith, M.L. Correlates of depressive mood among graduate-level allied health students: An exploratory study examining trait energy and fatigue. J. Am. Coll. Health 2021, 71, 1685–1695. [Google Scholar] [CrossRef]
- Adhikari, A.; Sujakhu, E.; GC, S.; Zoowa, S. Depression among Medical Students of a Medical College in Nepal during COVID-19 Pandemic: A Descriptive Cross-sectional Study. JNMA J. Nepal. Med. Assoc. 2021, 59, 645–648. [Google Scholar] [CrossRef]
- Adhikari, A.; Dutta, A.; Sapkota, S.; Chapagain, A.; Aryal, A.; Pradhan, A. Prevalence of poor mental health among medical students in Nepal: A cross-sectional study. BMC Med. Educ. 2017, 17, 232. [Google Scholar] [CrossRef]
- Shrestha, N.; Shrestha, N.; Khanal, S.; Dahal, S.; Lama, R.; Simkhada, P.; Pradhan, S.N. Prevalence of Depression among Medical Students of a Tertiary Care Teaching Hospital. JNMA J. Nepal. Med. Assoc. 2019, 57, 403–407. [Google Scholar] [CrossRef]
- Nezam, S.; Golwara, A.K.; Jha, P.C.; Khan, S.A.; Singh, S.; Tanwar, A.S. Comparison of prevalence of depression among medical, dental, and engineering students in Patna using Beck’s Depression Inventory II: A cross-sectional study. J. Fam. Med. Prim. Care 2020, 9, 3005–3009. [Google Scholar]
- Bresolin, J.Z.; Dalmolin, G.d.L.; Vasconcellos, S.J.L.; Barlem, E.L.D.; Andolhe, R.; Magnago, T.S.B.S. Depressive symptoms among healthcare undergraduate students. Rev. Lat. Am. Enferm. 2020, 28, e3239. [Google Scholar] [CrossRef]
- Ramakrishnan, D.; Raghunathan, D.; Valsan, K.I.; Ambika, S. Prevalence of Depression among Students of a Dental Tertiary Care Center in Kerala. Indian J. Community Med. 2019, 44 (Suppl. S1), S14–S18. [Google Scholar] [CrossRef]
- Alves, J.V.d.S.; Paula, W.d.; Netto, P.R.R.; Godman, B.; Nascimento, R.C.R.M.d.; Coura-Vital, W. Prevalence and factors associated with anxiety among university students of health sciences in Brazil: Findings and implications. J. Bras. De Psiquiatr. 2021, 70, 99–107. [Google Scholar] [CrossRef]
- Yusof, N.S.M.; Zainal, Z.A.; Huri, H.Z.; Jacob, S.A.; Alwi, M.N.M.; Hassan, Y.; Ghazali, L.N. Prevalence of depression among undergraduate pharmacy students in Malaysia. Int. J. Pharm. Res. 2020, 12, 09752366. [Google Scholar]
- Basheti, I.A.; Mhaidat, Q.N.; Mhaidat, H.N. Prevalence of anxiety and depression during COVID-19 pandemic among healthcare students in Jordan and its effect on their learning process: A national survey. PLoS ONE 2021, 16, e0249716. [Google Scholar] [CrossRef]
- Meng, J.; Gao, C.; Tang, C.; Wang, H.; Tao, Z. Prevalence of hypochondriac symptoms among health science students in China: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0222663. [Google Scholar] [CrossRef]
- Shaffique, S.; Farooq, S.S.; Anwar, H.; Asif, H.M.; Akram, M.; Jung, S.K. Meta-analysis of prevalence of depression, anxiety and stress among University Students. RADS J. Biol. Res. Appl. Sci. 2020, 11, 27–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Straus, S.E. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Covidence. Covidence: Better Systematic Review Management. 2020. Available online: https://www.covidence.org/ (accessed on 8 March 2022).
- Al-Maashani, M.; Al-Balushi, N.; Al-Alawi, M.; Mirza, H.; Al-Huseini, S.; Al-Balushi, M.; Obeid, Y.; Jose, S.; Al-Sibani, N.; Al-Adawi, S. Prevalence and Correlates of Depressive Symptoms among Medical Students: A Cross-sectional Single-centre Study. East Asian Arch. Psychiatry 2020, 30, 28–31. [Google Scholar] [CrossRef]
- Albajjar, M.A.; Bakarman, M.A. Prevalence and correlates of depression among male medical students and interns in Albaha University, Saudi Arabia. J. Fam. Med. Prim. Care 2019, 8, 1889–1894. [Google Scholar]
- AlShamlan, N.A.; AlShamlan, R.A.; AlShamlan, A.A.; AlOmar, R.S.; AlAmer, N.A.; Darwish, M.A.; Sebiany, A.M. Prevalence of depression and its associated factors among clinical-year medical students in Eastern Province, Saudi Arabia. Postgrad Med. J. 2020, 96, 343–348. [Google Scholar] [CrossRef]
- Alkhamees, A.A.; Alaqil, N.S.; Alsoghayer, A.S.; Alharbi, B.A. Prevalence and determinants of burnout syndrome and depression among medical students at Qassim University, Saudi Arabia. Saudi Med. J. 2020, 41, 1375–1380. [Google Scholar] [CrossRef]
- Azad, N.; Shahid, A.; Abbas, N.; Shaheen, A.; Munir, N. Anxiety and Depression in Medical Students of a Private Medical College. J. Ayub Med. Coll. Abbottabad 2017, 29, 123–127. [Google Scholar] [PubMed]
- Azim, S.R.; Baig, M. Frequency and perceived causes of depression, anxiety and stress among medical students of a private medical institute in Karachi: A mixed method study. J. Pak. Med. Assoc. 2019, 69, 840–845. [Google Scholar] [PubMed]
- Aluh, D.O.; Abba, A.; Afosi, A.B. Prevalence and correlates of depression, anxiety and stress among undergraduate pharmacy students in Nigeria. Pharm. Educ. 2020, 20, 236–248. [Google Scholar] [CrossRef]
- Bertani, D.E.; Mattei, G.; Ferrari, S.; Pingani, L.; Galeazzi, G.M. Anxiety, depression and personality traits in Italian medical students. Riv. Psichiatr. 2020, 55, 342–348. [Google Scholar] [PubMed]
- Basudan, S.; Binanzan, N.; Alhassan, A. Depression, anxiety and stress in dental students. Int. J. Med. Educ. 2017, 8, 179–186. [Google Scholar] [CrossRef]
- Bert, F.; Moro, G.L.; Corradi, A.; Acampora, A.; Agodi, A.; Brunelli, L.; Chironna, M.; Cocchio, S.; Cofini, V.; D’errico, M.M.; et al. Prevalence of depressive symptoms among Italian medical students: The multicentre cross-sectional “PRIMES” study. PLoS ONE 2020, 15, e0231845. [Google Scholar] [CrossRef]
- Biswas, M.; Al Jubayer, A.; Hasan, M.T.; Samir, N.; Alin, S.I.; Homaira, N.; Khatun, M.R.; Anjum, A. The Prevalence and Associated Factors of Depressive Symptoms Among Medical Students in Bangladesh During the COVID-19 Pandemic: A Cross-Sectional Pilot Study. Front. Public Health 2022, 9, 811345. [Google Scholar] [CrossRef]
- Coelho, L.D.S.; Tony, A.C.C.; Laguardia, G.C.A.; Santos, K.B.D.; Friedrich, D.B.C.; Cavalcante, R.B. Are symptoms of depression and anxiety in nursing students associated with their sociodemographic characteristics? Rev. Bras. Enferm. 2021, 74 (Suppl. S3), e20200503. [Google Scholar] [CrossRef]
- Çelik, N.; Ceylan, B.; Ünsal, A.; Çağan, Ö. Depression in health college students: Relationship factors and sleep quality. Psychol. Health Med. 2019, 24, 625–630. [Google Scholar] [CrossRef]
- Elsawy, W.I.H.; Sherif, A.A.R.; Attia, M.S.E.D.; El-Nimr, N.A. Depression among medical students in Alexandria, Egypt. Afr. Health Sci. 2020, 20, 1416–1425. [Google Scholar] [CrossRef]
- Falade, J.; Oyebanji, A.H.; Babatola, A.O.; Falade, O.O.; Olumuyiwa, T.O. Prevalence and correlates of psychiatric morbidity, comorbid anxiety and depression among medical students in public and private tertiary institutions in a Nigerian state: A cross-sectional analytical study. Pan. Afr. Med. J. 2020, 37, 53. [Google Scholar] [CrossRef]
- Fitzpatrick, O.; Biesma, R.; Conroy, R.M.; McGarvey, A. Prevalence and relationship between burnout and depression in our future doctors: A cross-sectional study in a cohort of preclinical and clinical medical students in Ireland. BMJ Open 2019, 9, e023297. [Google Scholar] [CrossRef]
- Fawzy, M.; Hamed, S.A. Prevalence of psychological stress, depression and anxiety among medical students in Egypt. Psychiatry Res. 2017, 255, 186–194. [Google Scholar] [CrossRef]
- Gan, G.G.; Yuen Ling, H. Anxiety, depression and quality of life of medical students in Malaysia. Med. J. Malays. 2019, 74, 57–61. [Google Scholar]
- Hoying, J.; Melnyk, B.M.; Hutson, E.; Tan, A. Prevalence and correlates of depression, anxiety, stress, healthy beliefs, and lifestyle behaviors in first-year graduate health sciences students. Worldviews Evid. Based Nurs. 2020, 17, 49–59. [Google Scholar] [CrossRef]
- Hanoon, Y.; Habib, H. Assessment of depressive symptoms among students at Al-Kindy College of Medicine in Baghdad. Fam. Med. Prim. Care Rev. 2021, 23, 307–312. [Google Scholar] [CrossRef]
- Junaid, M.A.L.; Auf, A.I.; Shaikh, K.; Khan, N.; Abdelrahim, S.A. Correlation between Academic Performance and Anxiety in Medical Students of Majmaah University–KSA. JPMA 2020, 2020, 865–868. [Google Scholar] [CrossRef]
- Khoshhal, K.I.; Khairy, G.A.; Guraya, S.Y.; Guraya, S.S. Exam anxiety in the undergraduate medical students of Taibah University. Med. Teach. 2017, 39 (Suppl. S1), S22–S26. [Google Scholar] [CrossRef]
- Kathem, S.H.; Al-Jumail, A.A.; Noor-Aldeen, M.; Najah, N.; Khalid, D.A. Measuring depression and anxiety prevalence among Iraqi healthcare college students using hospital anxiety and depression scale. Pharm. Pract. 2021, 19, 2303. [Google Scholar] [CrossRef]
- Kumar, S.G.; Kattimani, S.; Sarkar, S.; Kar, S.S. Prevalence of depression and its relation to stress level among medical students in Puducherry, India. Ind. Psychiatry J. 2017, 26, 86–90. [Google Scholar] [CrossRef]
- Killinger, S.L.; Flanagan, S.; Castine, E.; Howard, K.A. Stress and Depression among Veterinary Medical Students. J. Vet. Med. Educ. 2017, 44, 3–8. [Google Scholar] [CrossRef]
- Kupcewicz, E.; Mikla, M.; Kadučáková, H.; Grochans, E.; Valcarcel, M.D.R.; Cybulska, A.M. Correlation between Positive Orientation and Control of Anger, Anxiety and Depression in Nursing Students in Poland, Spain and Slovakia during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 2482. [Google Scholar] [CrossRef]
- Kebede, M.A.; Anbessie, B.; Ayano, G. Prevalence and predictors of depression and anxiety among medical students in Addis Ababa, Ethiopia. Int. J. Ment. Health Syst. 2019, 13, 30. [Google Scholar] [CrossRef]
- Kumar, B.; Shah, M.A.A.; Kumari, R.; Kumar, A.; Kumar, J.; Tahir, A. Depression, Anxiety, and Stress Among Final-year Medical Students. Cureus 2019, 11, e4257. [Google Scholar] [CrossRef]
- Lee, C.M.; Juarez, M.; Rae, G.; Jones, L.; Rodriguez, R.M.; Davis, J.A.; Boysen-Osborn, M.; Kashima, K.J.; Krane, N.K.; Kman, N.; et al. Anxiety, PTSD, and stressors in medical students during the initial peak of the COVID-19 pandemic. PLoS ONE 2021, 16, e0255013. [Google Scholar] [CrossRef]
- López, R.B.; Navarro, N.M.; Astorga, A.C. Relationship between personality organization and the prevalence of symptoms of depression, anxiety and stress among university students in health careers in the Region of Coquimbo, Chile. Rev. Colomb. Psiquiatr. 2017, 46, 203–208. [Google Scholar] [CrossRef]
- Lu, L.; Wang, X.; Wang, X.; Guo, X.; Pan, B. Association of Covid-19 pandemic-related stress and depressive symptoms among international medical students. BMC Psychiatry 2022, 22, 20. [Google Scholar] [CrossRef]
- Milić, J.; Škrlec, I.; Milić Vranješ, I.; Podgornjak, M.; Heffer, M. High levels of depression and anxiety among Croatian medical and nursing students and the correlation between subjective happiness and personality traits. Int. Rev. Psychiatry 2019, 31, 653–660. [Google Scholar] [CrossRef]
- Melaku, L.; Bulcha, G.; Worku, D. The prevalence and severity of depression, anxiety, and stress among medical undergraduate students of Arsi University and their association with substance use, Southeast Ethiopia. Educ. Res. Int. 2021, 2021, 1–12. [Google Scholar] [CrossRef]
- Mirza, A.A.; Milaat, W.A.; Ramadan, I.K.; Baig, M.; Elmorsy, S.A.; Beyari, G.M.; Halawani, M.A.; Azab, R.A.; Zahrani, M.T.; Khayat, N.K. Depression, anxiety and stress among medical and non-medical students in Saudi Arabia: An epidemiological comparative cross-sectional study. Neurosciences 2021, 26, 141–151. [Google Scholar] [CrossRef]
- Mahroon, Z.A.; Borgan, S.M.; Kamel, C.; Maddison, W.; Royston, M.; Donnellan, C. Factors Associated with Depression and Anxiety Symptoms Among Medical Students in Bahrain. Acad. Psychiatry 2018, 42, 31–40. [Google Scholar] [CrossRef]
- Nakhostin-Ansari, A.; Sherafati, A.; Aghajani, F.; Khonji, M.S.; Aghajani, R.; Shahmansouri, N. Depression and Anxiety among Iranian Medical Students during COVID-19 Pandemic. Iran. J. Psychiatry 2020, 15, 228–235. [Google Scholar] [CrossRef]
- Fata Nahas, A.R.M.; Elkalmi, R.M.; Al-Shami, A.M.; Elsayed, T.M. Prevalence of Depression Among Health Sciences Students: Findings From a Public University in Malaysia. J. Pharm. Bioallied Sci. 2019, 11, 170–175. [Google Scholar] [CrossRef]
- Nahar, V.K.; Davis, R.E.; Dunn, C.; Layman, B.; Johnson, E.C.; Dascanio, J.J.; Johnson, J.W.; Sharma, M. The prevalence and demographic correlates of stress, anxiety, and depression among veterinary students in the Southeastern United States. Res. Vet. Sci. 2019, 125, 370–373. [Google Scholar] [CrossRef]
- Otim, M.; Al Marzouqi, A.M.; Subu, M.; Damaj, N.; Al-Harbawi, S. Prevalence of Generalised Anxiety Disorders Among Clinical Training Students at the University of Sharjah. J. Multidiscip. Healthc. 2021, 14, 1863–1872. [Google Scholar] [CrossRef]
- Pokhrel, N.B.; Khadayat, R.; Tulachan, P. Depression, anxiety, and burnout among medical students and residents of a medical school in Nepal: A cross-sectional study. BMC Psychiatry 2020, 20, 298. [Google Scholar] [CrossRef]
- Pukas, L.; Rabkow, N.; Keuch, L.; Ehring, E.; Fuchs, S.; Stoevesandt, D.; Sapalidis, A.; Pelzer, A.; Rehnisch, C.; Watzke, S. Prevalence and predictive factors for depressive symptoms among medical students in Germany—A cross-sectional study. GMS J. Med. Educ. 2022, 39, Doc13. [Google Scholar]
- Pham, T.; Bui, L.; Nguyen, A.; Nguyen, B.; Tran, P.; Vu, P.; Dang, L. The prevalence of depression and associated risk factors among medical students: An untold story in Vietnam. PLoS ONE 2019, 14, e0221432. [Google Scholar] [CrossRef]
- Patelarou, A.; Mechili, E.A.; Galanis, P.; Zografakis-Sfakianakis, M.; Konstantinidis, T.; Saliaj, A.; Bucaj, J.; Alushi, E.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I.; et al. Nursing students, mental health status during COVID-19 quarantine: Evidence from three European countries. J. Ment. Health 2021, 30, 164–169. [Google Scholar] [CrossRef]
- Patten, E.V.; Vaterlaus, J.M. Prevalence of Depression, Anxiety, and Stress in Undergraduate Dietetics Students. J. Nutr. Educ. Behav. 2021, 53, 67–74. [Google Scholar] [CrossRef]
- Risal, A.; Shikhrakar, S.; Mishra, S.; Kunwar, D.; Karki, E.; Shrestha, B.; Holen, A. Anxiety and Depression during COVID-19 Pandemic among Medical Students in Nepal. Kathmandu Univ. Med. J. (KUMJ) 2020, 18, 333–339. [Google Scholar] [CrossRef]
- Santangelo, O.E.; Provenzano, S.; Armetta, F.; Pesco, G.; Allegro, A.; Lampasona, M.; Pantaleo, L.; Terranova, A. Prevalence of depressive symptomatology among nursing students during the COVID-19 pandemic. Ann. Ig. 2022, 34, 227–235. [Google Scholar] [PubMed]
- Silva, V.; Costa, P.; Pereira, I.; Faria, R.; Salgueira, A.P.; Costa, M.J.; Sousa, N.; Cerqueira, J.J.; Morgado, P. Depression in medical students: Insights from a longitudinal study. BMC Med. Educ. 2017, 17, 184. [Google Scholar] [CrossRef]
- Umar, M.U.; Suraj, S.S.; Umar, B.I.; Gajida, A.U. Prevalence and factors associated with depression among medical students in Nigeria. Niger Postgrad Med. J. 2021, 28, 198–203. [Google Scholar] [CrossRef]
- Solanki, H.K.; Awasthi, S.; Kaur, A.; Pamei, G. Depression, its correlates and quality of life of undergraduate medical students in the Kumaon region of Uttarakhand state, India. Indian J. Community Health 2021, 33, 357–363. [Google Scholar] [CrossRef]
- Tayefi, B.; Eftekhar, M.; Tayefi, M.; Darroudi, S.; Khalili, N.; Mottaghi, A.; Shanjani, Z.H.; Nojomi, M. Prevalence and Socio-Demographic Correlates of Mental Health Problems Among Iranian Health Sciences Students. Acad. Psychiatry 2020, 44, 73–77. [Google Scholar] [CrossRef]
- Bahçecioğlu Turan, G.; Özer, Z.; Çiftçi, B. Analysis of anxiety levels and attitudes of nursing students toward the nursing profession during the COVID-19 pandemic. Perspect. Psychiatr. Care 2021, 57, 1913–1921. [Google Scholar] [CrossRef]
- Van Venrooij, L.T.; Barnhoorn, P.C.; Giltay, E.J.; van Noorden, M.S. Burnout, depression and anxiety in preclinical medical students: A cross-sectional survey. Int. J. Adolesc. Med. Health 2017, 29, 20170077. [Google Scholar] [CrossRef]
- Van der Walt, S.; Mabaso, W.S.; Davids, E.L.; De Vries, P.J. The burden of depression and anxiety among medical students in South Africa: A cross-sectional survey at the University of Cape Town. South Afr. Med. J. 2020, 110, 69–79. [Google Scholar] [CrossRef]
- Yuan, L.L.; Lu, L.; Wang, X.H.; Guo, X.X.; Ren, H.; Gao, Y.Q.; Pan, B.-C. Prevalence and Predictors of Anxiety and Depressive Symptoms Among International Medical Students in China During COVID-19 Pandemic. Front. Psychiatry 2021, 12, 761964. [Google Scholar] [CrossRef]
- Zakeri, M.; De La Cruz, A.; Wallace, D.; Sansgiry, S.S. General Anxiety, Academic Distress, and Family Distress Among Doctor of Pharmacy Students. Am. J. Pharm. Educ. 2021, 85, 8522. [Google Scholar] [CrossRef]
- Zeng, Y.; Wang, G.; Xie, C.; Hu, X.; Reinhardt, J.D. Prevalence and correlates of depression, anxiety and symptoms of stress in vocational college nursing students from Sichuan, China: A cross-sectional study. Psychol. Health Med. 2019, 24, 798–811. [Google Scholar] [CrossRef]
- Iqbal, S.; Gupta, S.; Venkatarao, E. Stress, anxiety and depression among medical undergraduate students and their socio-demographic correlates. Indian J. Med. Res. 2015, 141, 354–357. [Google Scholar] [PubMed]
- Tian-Ci Quek, T.; Wai-San Tam, W.X.; Tran, B.; Zhang, M.; Zhang, Z.; Su-Hui Ho, C.; Chun-Man Ho, R. The global prevalence of anxiety among medical students: A meta-analysis. Int. J. Environ. Res. Public Health 2019, 16, 2735. [Google Scholar] [CrossRef]
- Gradus, J.L. Epidemiology of PTSD; National Center for PTSD (United States Department of Veterans Affairs): White River Junction, VT, USA, 2007. [Google Scholar]
- Agyapong, B.; Obuobi-Donkor, G.; Burback, L.; Wei, Y. Stress, Burnout, Anxiety and Depression among Teachers: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 10706. [Google Scholar] [CrossRef]
- Catuzzi, J.E.; Beck, K.D. Anxiety vulnerability in women: A two-hit hypothesis. Exp. Neurol. 2014, 259, 75–80. [Google Scholar] [CrossRef]
- Parker, G.; Brotchie, H. Gender differences in depression. Int. Rev. Psychiatry 2010, 22, 429–436. [Google Scholar] [CrossRef]
- Chang, J.J.; Ji, Y.; Li, Y.H.; Pan, H.F.; Su, P.Y. Prevalence of anxiety symptom and depressive symptom among college students during COVID-19 pandemic: A meta-analysis. J. Affect. Disord. 2021, 292, 242–254. [Google Scholar] [CrossRef]
- Gorman, J.M. Gender differences in depression and response to psychotropic medication. Gend. Med. 2006, 3, 93–109. [Google Scholar] [CrossRef]
- Serpytis, P.; Navickas, P.; Lukaviciute, L.; Navickas, A.; Aranauskas, R.; Serpytis, R.; Deksnyte, A.; Glaveckaite, S.; Petrulioniene, Z.; Samalavicius, R. Gender-Based Differences in Anxiety and Depression Following Acute Myocardial Infarction. Arq. Bras. Cardiol. 2018, 111, 676–683. [Google Scholar] [CrossRef]
- Moustafa, A.A.; Tindle, R.; Frydecka, D.; Misiak, B. Impulsivity and its relationship with anxiety, depression and stress. Compr. Psychiatry 2017, 74, 173–179. [Google Scholar] [CrossRef]
- Bertolote, J.M. Preventing Suicide a Resource for General Physicians; Health DoM, Ed.; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Liu, C.H.; Stevens, C.; Wong, S.H.M.; Yasui, M.; Chen, J.A. The prevalence and predictors of mental health diagnoses and suicide among U.S. college students: Implications for addressing disparities in service use. Depress. Anxiety 2019, 36, 8–17. [Google Scholar] [CrossRef]
- Pires, G.N.; Bezerra, A.G.; Tufik, S.; Andersen, M.L. Effects of acute sleep deprivation on state anxiety levels: A systematic review and meta-analysis. Sleep Med. 2016, 24, 109–118. [Google Scholar] [CrossRef]
- Mathew, A.R.; Hogarth, L.; Leventhal, A.M.; Cook, J.W.; Hitsman, B. Cigarette smoking and depression comorbidity: Systematic review and proposed theoretical model. Addiction 2017, 112, 401–412. [Google Scholar] [CrossRef]
- Shaukat, N.; Ali, D.M.; Razzak, J. Physical and mental health impacts of COVID-19 on healthcare workers: A scoping review. Int. J. Emerg. Med. 2020, 13, 40. [Google Scholar] [CrossRef]
- Agyapong, B.; Shalaby, R.; Wei, Y.; Agyapong, V.I. Can ResilienceNhope, an evidence-based text and email messaging innovative suite of program help to close the psychological treatment and mental health literacy gaps in college students? Front. Public Health 2022, 10, 890131. [Google Scholar] [CrossRef]
- Agyapong, B.; Brett-MacLean, P.; Burback, L.; Agyapong, V.I.O.; Wei, Y. Interventions to Reduce Stress and Burnout among Teachers: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 5625. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Authors/Year | Country | Study Design | Population Sample/Sample Size (Response Rate) | Students’ Age Range/Mean | Scales Used | Key Findings | |
|---|---|---|---|---|---|---|---|
| Correlates of Anxiety/Depression | Prevalence of Anxiety/Depression | ||||||
| Alves et al., 2021 [24] | Brazil | Cross-sectional | Health 493 RR = 22.5% | Mean age of 23.1 years | The Beck Anxiety Inventory | Live with parents Dissatisfied with the course and being in the exam period | Severe anxiety 28.0%, Moderate anxiety 29.8% |
| Al-Maashani et al., 2020 [33] | Oman | Cross-sectional | 197/1041 medical students RR = 18.9% | NR | Patient Health Questionnaire-9 (PHQ-9) | Female gender Family history of depression | The prevalence of depressive symptoms was 41.3% |
| Adhikari et al., 2021 [18] | Nepal | Cross-sectional | 223 medical students | NR | Patient Health Questionnaire | Preclinical years (first and second year) compared to third, fourth and final year. Age less than 24 | The prevalence of depression among medical students was 23.3%. (17.7–28.9 at 95% interval) |
| Albajjar et al., 2019 [34] | Saudi Arabia | Cross-sectional | 161/306 medical students RR = 52.6% | AR = 19–26 Mean of 22.03 ± 1.94 years | Becks Depression Inventory | History of domestic abuse or violence History of major trauma or psychiatric event | The prevalence of depression was 53.8% Depression was mild in 25.8% and severe or extreme in 4.4% of the participants |
| AlShamlan et al., 2020 [35] | Saudi Arabia | Cross-sectional | 527 medical students | NR | Patient Health Questionnaire (PHQ-9) | Female gender Students who perceived that they were not yet ready for their future specialities. | The prevalence of depression was found to be 39.27% |
| Alkhamees et al., 2020 [36] | Saudi Arabia | Cross-sectional | 153 medical students | NR | Maslach Burnout Inventory Patient Health Questionnaire (PHQ-9) | Older Age Female Gender Student academic year High emotional exhaustion High cynicism Burnout | The current study assessed the prevalence of burnout and depression among medical students at UCM using the MBI and the PHQ-9. The estimated prevalence was 5.6% and 50.2%, respectively |
| Azad et al., 2017 [37] | Pakistan | Cross-sectional | 150/415 medical students RR = 36.1% | AR = 17–26 Mean = 20.6 ± 0.88 | Beck Anxiety Scale | Time of assessment Female gender | About 19% of the students had moderate to severe anxiety |
| Ahad et al., 2021 [15] | India | Cross-sectional | 507 dental students RR = 65.3% | AR = 17–32 Mean age of 22.04 ± 2.20 years | Depression, Anxiety, and Stress Scale (DASS)-42 | Depression: age is a strong positive predictor for anxiety and depression Anxiety: staying in the hostel was a positive predictor of anxiety | Anxiety was 66.86% (n = 339) Depression (57.39%) |
| Azim et al., 2019 [38] | Pakistan | Mixed-method qualitative-quantitative study | 188/270 (70%) medical students | AR = 18–25 Mean = 21.4 ± 2.2 years | Depression, Anxiety, and Stress Scale-21 | Third-year student Moderate or poor socioeconomic status | The prevalence of anxiety was 72%. |
| Abed et al., 2022 [6] | Egypt | Cross-sectional | 597 medical students | NR | Depression, Anxiety, and Stress Scale (DASS-21) | Depression/Anxiety: Smoking Female gender In the third year Student average achievement score Social activity Transportation | Anxiety: Out of the included students, 82.6% experienced anxiety Depression: Out of the included students, 88.8% experienced depression |
| Aluh et al., 2020 [39] | Nigeria | cross-sectional | 408 pharmacy students RR = 13.32% | Mean age = 22.57 ± 3.39 | Depression, Anxiety and Stress Scale (DASS) | Anxiety/depression: Students in lower years of study perceived poor academic performance | The overall prevalence of depression, anxiety and stress was 44.6%, 63.5%, and 35%, respectively |
| Adhikari et al., 2017 [19] | Nepal | Cross-sectional | 343 medical students | AR = 18–25 | Hospital Anxiety Scale Patient Health Questionnaire | Anxiety: Female Gender Preclinical students Depression: Preclinical years (first and second year) compared to third, fourth and final year) Age less than 24 | Anxiety: There was a 5.8% prevalence rate for anxiety. Depression: The prevalence of depression among medical students was 23.3%. (17.7–28.9 at 95% interval) |
| Bertani et al., 2020 [40] | Italy | Cross-sectional | 459/944 (48%) medical students | AR = 19–50 Mean = 23 plus or minus 3 | Hospital Anxiety and Depression Scale (HADS) Personality Inventory for DSM-5 | Anxiety/depression: Personality traits Namely detachment negative effect Cognitive enhancers | The prevalence of anxiety was 20% The prevalence of depression was 7% |
| Basheti et al., 2021 [26] | Jordan | Cross-sectional | 450 healthcare students (medicine, dentistry, Pharm.D., pharmacy, nursing, and other) | Mean = 21.62 | Hospital Anxiety and Depression Scale (HADS) | Smoking Lower family income Use of medications | 22.4% of students were classified as having anxiety 33.8% of students were classified to have depression |
| Basudan et al., 2017 [41] | Saudi Arabia | Cross-sectional | 247 dental students | Anxiety scale (DASS-21) Depression scale (DASS-21) | Anxiety/Depression: Male Gender-Low anxiety Satisfaction with faculty relationships Satisfaction with peer relationships Dentistry is the first choice for the field of study | Prevalence of anxiety was 66.8%. The prevalence of depression was 55.9%. | |
| Bert et al., (2020) [42] | Italy | Multicenter cross-sectional | 2396 medical students RR = 95% | Median age was 22 | Beck Depression Inventory-II (BDI-II) | Age being female bisexual/asexual orientation, living with partner/housemates poor economic status less than 90 min of weekly exercise relatives with psychiatric disorders personal chronic disease judging medical school choice negatively unsatisfying friendships with classmates competitive and hostile climate among classmates thinking that medical school hinders specific activities and being worried about not measuring up to the profession | Depression—29.5% |
| Bresolin et al., 2020 [22] | Brazil | Cross-sectional | 792 healthcare students (Nursing, Pharmacy, Physiotherapy, Speech Therapy, Medicine, Dentistry and Occupational Therapy) | NR | Beck Depression Inventory | Non-performance of physical and leisure activities Speech therapy Nursing courses | Depression was moderate to severe in 23.6% of students |
| Boolani et al., 2021 [17] | United States | Cross-sectional | 77 health students | AR = 18–45 Mean = 25.83 | 30-item Profile of Mood States Short Form (POMS-SF) | Worse sleep quality Increased sitting time Trait physical fatigue | 65/77 (84.4%) of participants reported feelings of depression |
| Biswas et al., 2022 [43] | Bangladesh | Cross-sectional | 425 medical students RR- = 93.2%. | Age = 22 years | Patient Health Questionnaire-9 | Female students Those who struggled to stay away from social media Those who tried to be optimistic to maintain better psychology those who always had sleeping difficulty in the last four weeks | Prevalence of depression was 80.2% |
| Coelho LDS et al., 2021 [44] | Brazil | Cross-sectional | 192 | Mean age = 21.44 (±3.56) | Beck Depression and Anxiety Inventories | Anxiety/depression: Female gender Student from 6th–10th semester Psychotropic drug use | On the anxiety scale, a minimal classification was predominant (30.21%) On the depression scale, severe symptoms were the most frequent (30.73%) |
| Çelik et al., 2019 [45] | Turkey | Cross-sectional | 445 health students (nursing, midwifery and health management) | Mean age = 21.0 ± 2.0 | Beck Depression Inventory | Sleep quality: As sleep quality deteriorates, the level of depression also increases Academic failure Level of income Smokers or alcohol drinkers | The risk of depressive symptoms in students with poor sleep quality was 3.28 times. |
| Elsawy et al., 2020 [46] | Egypt | Cross-sectional | 390 medical students | NR | Beck Depression Inventory Scale—2 (BDI-2) | Female gender The presence of mental illness Not having someone to talk to when under stress Experiencing stressful life event(s) during the previous six months Not being satisfied with the socioeconomic level Reporting that the surrounding environment is not suitable for studying Not specifying a grade to achieve Extreme dissatisfaction with students results | The prevalence of moderate and severe depression was 27.9% and 17.2, respectively The prevalence of depression was high among medical students |
| Falade et al., 2020 [47] | Nigeria | Cross-sectional | 944 medical students RR = 97.8% | 16 and 32 years, the overall mean was 21 ± 3.0 years | Hospital Anxiety and Depression Scale | Being a student receiving less than one dollar equivalent per day as an allowance A student from the Igbo ethnic group | Prevalence of anxiety was 25% Depression—14.3% |
| Fitzpatrick et al., 2019 [48] | Ireland | Cross-sectional | 269 medical students | NR | Beck Depression Inventory—Fast Screen | Increase burnout increases depression | There was a 39% prevalence of depression caseness Low burnout had 13% depression Intermediate burnout had 38% depression The high burnout category had 66% depression. |
| Fawzy et al. (2017) [49] | Egypt | Cross-sectional | 700 medical students RR = 100% | Mean age of 21.22 ± 1.632 years | Depression, Anxiety, and Stress Scale-21 (DASS-21) | Anxiety/Depression: Females Gender Those living in the University campus/students’ residence facility In the preclinical years lower academic achievement had higher scores in DASS | Prevalence of anxiety was 73% Prevalence of depression was 65% |
| Gupta et al., 2021 [14] | United States | Cross-sectional | 438 (33.4%) medical students | NR | PHQ-9 and GAD-7 | Anxiety/depression: Medical students Female gender | The prevalence of anxiety was 48.1%. Moderate to severe anxiety was 20.3% The prevalence of depression was 45.3%. Moderate to severe depression was 17.2% |
| Gan et al., 2019 [50] | Malaysia | Cross-sectional | 149 medical students RR = 96.7% | AR = 22–24 | Hospital Anxiety and Depression Scale (HADS) | Anxiety and depression were associated with significantly poorer QOL. Students with depression symptoms were associated with lower physical, psychological and environmental domain scores, whereas those with anxiety had lower psychological, social and environmental scores. | The prevalence rates of anxiety and depression were 33% and 11%, respectively |
| Hoying et al., 2020 [51] | United States | Cross-sectional | 197 Health sciences students (Dentistry, Medicine, Nursing, Optometry, Pharmacy, Social Work, and Veterinary Medicine) | Mean age = 24.5 years | General Anxiety Disorder Scale Patient Health Questionnaire-9 | Less than seven hr. of sleep per night Worse general health Lower healthy lifestyle beliefs Lower healthy lifestyle behaviours Higher stress Perceived lack of control | Anxiety—14% Depression—17% |
| Hanoon et al., 2021 [52] | Baghdad | Cross-sectional | 301 medical students | Center for Epidemiological Studies Depression Scale (CESD-R) | Stage of the study Female gender Social relationship | The overall prevalence of depressive symptoms is 55.48%. | |
| Junaid et al., 2020 [53] | Saudi Arabia | cross-sectional | 247 medical students RR-90% | NR | Beck Anxiety Inventory (BAI) | Females Low academic grades Those in the final year | Anxiety—40% |
| Khoshhal et al., 2017 [54] | Saudi Arabia | Cross-sectional | 111 Medical students RR = 89% | NR | Visual Analog Scale (VAS) | Studying all night before the exam Extensive course load Female gender | 65% of students experienced exam anxiety |
| Kathem et al., 2021 [55] | Iraq | Cross-sectional | 750 healthcare students (Pharmacy and medicine) | AR = 19–23 | Hospital Anxiety Scale Hospital Depression Scale | Lower sleep hours at night Academic achievement Colleagues and family social support during exams | More than one-half (52.1%) of the participants had scores that indicated anxiety symptoms In comparison, 20.1% had scores that indicated borderline anxiety symptoms Approximately forty-six per cent (45.9%) of the participants had scores that indicated depression symptoms, and one-quarter (24.8%) had scores that indicated depression borderline symptoms |
| Kumar et al., 2017 [56] | India | Cross-sectional | 444 medical students RR = 88.8% | NR | Beck Depression Inventory Scale | Severe stress level Those without interpersonal problems Low levels of perceived interpersonal support Age, study year, satisfaction with the major, parental relationship, and mother’s education among medical student Smoking, alcohol use, family history of depression, academic achievement, and interpersonal problems in the family | Depression—48.4% |
| Killinger et al., 2017 [57] | North America | Cross-sectional | 1245 veterinary medical students | AR = 18–54 | Centre for Epidemiological Studies Depression Scale (CES-D) | Female gender Year in the program—Rates of depression were highest in year two and year three and lowest in year one and year 4 | 66% of the population had symptoms ofdepression |
| Kupcewicz et al., 2022 [58] | Poland Spain Slovakia | Cross-sectional | 756 nursing students | Mean age = 21.20 years | Positive Orientation Scale Courtauld Emotional Scale | Age-Anxiety control increases with age. More time working on computer Family crisis | Depression was diagnosed in 35.8% of study participants |
| Kebede et al., 2019 [59] | Ethiopia | Cross-sectional | 273 medical students | AR = 18–21 | Hospital Anxiety and Depression Scale | Female gender First-year educational level Second-year educational level Poor/low social support | The prevalence of anxiety and depression was 51.30% |
| Kumar et al. (2019) [60] | Karachi | Observational study | 312 Medical students RR = 69.3% | Mean age = 22.74 ± 1.52 years | Depression Anxiety Stress Scale-21 (DASS-21) | The pressure of passing exams The pressure of living up to family’s expectations Fear of stepping into the real world of medicine Dissatisfaction with the administration | Anxiety—74% Depression—57.6% |
| Lee et al., 2021 [61] | United States | Cross-sectional | 741 medical students | NR | General Anxiety Disorder Scale (GAD-7) | Female gender Being Asian | During the initial peak phase of COVID-19, over 60% of US medical students screened positive for pandemic-related anxiety |
| Lopez et al., 2017 [62] | Chile | Cross-sectional | 235 health students (medical, nursing, and kinesiology) | AR = 18–34 Mean = 20.7 ± 3.41 | Depression, Anxiety, and Stress Scale (DASS-21) | Personality organization dimensions | The prevalence of anxiety was 39% The prevalence of depression was 23% |
| Lu et al., (2022) [63] | China | Cross-sectional | 519 Medical students RR = 50.39% | Mean = 22.76 ± 3.60 | Patient Health Quesionnaire-9 | Negative coping positive correlation with depression Perceived social support negative correlation with depression. | 9.83%, 3.08%, and 2.12% of students had mild, moderate and severe depressive symptoms, respectively |
| Authors/Year | Country | Study Design | Population Sample/Sample Size (Response Rate) | Students’ Age Range/Mean | Scales Used | Key Findings | |
|---|---|---|---|---|---|---|---|
| Correlates of Anxiety/Depression | Prevalence of Anxiety/Depression | ||||||
| Milić et al., 2019 [64] | Croatia | Cross-sectional | 562 medical and nursing students | AR = 20–24 Mean = 22 | Patient health questionnaire (PHQ-9) General Anxiety Disorder Scale (GAD-7) Subjective Happiness Scale (SHS) | Emotional stability negatively correlated with anxiety and depression. | The prevalence of anxiety was 54.5% among Croatian medical students The prevalence of depression was 60.2% among Croatian medical students |
| Melaku et al., (2021) [65] | Ethiopia | cross-sectional | 265 medical students RR = 98% | Mean = 22.03 | Depression, Anxiety, Stress Scale-21 (DASS-21) | Anxiety: Gender-Males less likely to be depressed. Marital status-less likely to be depressed. Cigarette smoking-Increases depression. Depression: Low Monthly income-More depressed. Residency- Non-dormitory living respondents more likely to be depressed. Alcohol drinking-More likely to be depressed. | Anxiety—60.8% Depression—52.3% |
| Mirza et al., 2021 [66] | Saudi Arabia | Cross-sectional | 231 medical students | Mean = 21.67 ± 1.56 | Depression, anxiety and stress scale-21 items (DASS-21) | Anxiety: Female gender High consumption of energy drinks Spending more time on leisure activities and hobbies Long travel time from home to university Family conflicts Depression: Female gender History of psychiatric disorder Senior academic year Travel time from home to university Family conflicts at home | Approximately 54%, 53%, and 38% of participants were found to be suffering from anxiety, depression and stress. |
| Mahroon et al., 2018 [67] | Bahrain | cross-sectional | Medical 350 RR-87.6% | AR = 18 to 25 | The Beck Anxiety Inventory The Beck Depression Inventory | Anxiety: Female gender Year of Study Academic performance Depression: Arab ethnicity Female gender relationship with peers Year of Study Academic performance | Prevalence of anxiety is 51% Prevalence of depression is 40% |
| Nakhostin-Ansari et al., 2020 [68] | Iran | Cross-sectional | 323/500 (64.6%) medical students | Mean = 23.73. | Beck Anxiety Inventory (BAI) Beck Depression Inventory (BDI) | Female gender Lower grade point average Experience of COVID-19 symptoms. | The prevalence of anxiety was 38.1% The prevalence of depression was 27.6% |
| Nahas et al., 2019 [69] | Malaysia | Cross-sectional | 365/425 (85.9%) health students (Medicine, Pharmacy, Dentistry, Nursing, and Allied Health Sciences students) | NR | Patient Health Questionnaire (PHQ-9) | Student’s origin- urban areas more likely to report depression. | The prevalence of depression was 36.4% |
| Nezam et al., 2020 [21] | Patna | Cross-sectional | 2798/3100 (90.25%) medical, dental and students) | NR | Beck’s Depression Inventory 2 | Dental students-higher prevalence than medical students. | The overall prevalence of depressive symptoms was found to be 47.78% Of the three streams, students belonging to the engineering stream (40.28%) showed a maximum prevalence of depressive symptoms, followed by dental (38.50%) and medical students (34.74%) |
| Nahar et al., 2019 [70] | Southeastern United States | Cross-sectional | 264 veterinary students | Mean = 25.3 ± 3.21 years | Patient health questionnaire (PHQ-4) | Female Gender Grade point: Low Average Non-white | The prevalence of anxiety was 52.3% among veterinary students The prevalence of depression was 22.6% among veterinary students |
| Nebhinani et al., 2021 [16] | Western India | Cross-sectional survey | 229 nursing students | AR = 21–25 Mean = 21.6 ± 2.8 | COVID-induced anxiety scale Likert scale | Age- Positive association with the age of the students only (p = 0.001) Negative linear correlation between anxiety score and protective behavior score. | The prevalence of anxiety was 75.5% |
| Otim et al., 2021 [71] | United Arab Emirates | Cross-sectional | 219 clinical training students | NR | State-Trait Anxiety Inventory for Adults (STAI) | Female gender Students living off-campus Students who slept for 5 h or less Students that reported no physical activity Current smoker | 63% of the sample had high state anxiety, and 62% had high trait anxiety |
| Pokhrel et al., (2020) [72] | Nepal | cross-sectional | 651 Medical students | Mean = 25 years | Nepali version of the Hospital Anxiety and Depression Scale | Anxiety: Female gender Depression Personal burnout Teaching and learning-related stressors History of mental illness Depression: Anxiety Personal burnout Work-related burnout | Anxiety—45.3% Depression—31% |
| Pukas et al., (2022) [73] | Germany | Cross-sectional | 1103 medical students RR = 90.2% | Mean = 23.1 | BDI-II | Neuroticism Insufficient emotional support Eating irregular meals Use of medication or drugs to calm down mental overload | Prevalence of depressive symptoms was 11% for mild, 5.6% for moderate and 2.4% for severe symptoms |
| Pham et al., 2019 [74] | Vietnam | cross-sectional | 494 medical students RR = 78.8% | AR = 21 and above | Patient Health Questionnaire 9 (PHQ-9) | non-self-determined motivation perceived financial burden vigorous level of physical activity | The prevalence of self-reported depression was 15.2% |
| Patelarou et al., 2021 [75] | Greece, Spain, and Albania | Cross-sectional | 787 nursing students | Mean = 22.7 | Patient Health Questionnaire 9 (PHQ-9) | Decreased age Identifying as Spanish Living with people in high-risk groups Working status during the pandemic | 1/3 of the nursing student population experienced depression |
| Patten 2021 [76] | US | Cross-sectional | 611 Dietetics students | NR | Depression, Anxiety, and Stress Scale (DASS-21) | Significant sources of stress were postgraduation plans (including internships), managing time, dietetics courses, finances, and self-imposed expectations. | Depression (30%), anxiety (40%), and stress (27%) |
| Raghunathan et al., 2019 [23] | India | Cross-sectional | 364 dental students | NR | Patient Health Questionnaire-9 (PHQ-9) | Being married Having a low and average level of course satisfaction Having close friends Female gender Breakups in relationships | The prevalence of depression was estimated at 26.9%. |
| Risal et al., 2020 [77] | Nepal | Cross-sectional | 416 medical students | Mean age = 22.2 | Hospital Anxiety and Depression Scale | History of a mental problem Concurrent physical illness possible COVID-19 exposure | The prevalence of anxiety was 11.8% The prevalence of depression was 5.5% |
| Santangelo et al., 2022 [78] | Italy | Cross-sectional | Nursing students 525 | Mean age = 21.8 | Quick Inventory of Depressive Symptomatology Self-Report Questionnaire (QIDS-SR16) | Female gender Low perceived economic status Low perceived health status To be a smoker | Per the scores obtained from the QIDSSR16 test, we can say that just over half of the sample (51.3%) does not exhibit depressive symptomatology |
| Shawahna et al., 2020 [7] | Palestine | Cross-sectional | 286 medical students RR = 67.3% | Median age was 20, with an IQR of 3 years | Beck Anxiety Inventory (BAI) Beck Depression Inventory-II (BDI-II) | Anxiety: academic stage academic year 4 to 6 low BDI scores. mental health status Depression: Higher Grade Point Average–Low BDI score Low mental health status, Attempted suicide, Low religious commitment- higher BDI-II scores | 21.3% had severe anxiety 9.1% had severe depression |
| Shrestha et al., (2019) [20] | Nepal | cross-sectional | 217 medical students | NR = 18–29 years. | Beck’s Depression Index II | Academically incompetent Medical students progressed to their clinical years | Depression—27.2% |
| Silva et al., 2017 [79] | Portugal | Longitudinal study | 2234/238 (74%) medical students | Beck Depression Inventory (BDI) | Academic burnout Anxiety traits Medicine choice Relationship patterns | The prevalence of depression ranged between 12.7% to 21.5%. | |
| Suraj et al., 2021 [80] | Nigeria | Cross-sectional | 279/285 (98%) medical students | AR = 21.75 ± 3.25 years Mean = 21.75 | 3-item Oslo Social Support Rating Scale | Female gender Age < 22 years Those at the lower level of study Poor social support Family history of depression History of depression | The prevalence of depression among medical students was 15.1% |
| Solanki et al., 2021 [81] | North India | Cross-sectional | 414/500 (82.8%) medical students | AR = 17–29 Mean = 20.9 | Centre for Epidemiologic Studies Depression Scale (CES-D) WHO Quality of Life—BREF questionnaire Smartphone Addiction Scale | Smartphone addiction Living with chronic disease They feel like their siblings or friends are more accomplished than themselves. Hospitalization of any family member for over 24 h in the last year Divorce or separation of parents Parental pressure for academic excellence Financial crisis in the family Romantic breakup | The prevalence of depression was 36.7%. |
| Tayefi et al., 2020 [82] | Iran | Cross-sectional | 560 health students (medical and other health sciences) | Mean = 21.1 ± 5.3 years | Beck Depression Inventory Beck Anxiety Inventory General Health Questionnaire WHO wellbeing index | Ethnicity- Kurdish students more likely to have mild to severe depression symptoms compared to Persian students. Birthplace- Being born in the capital city lower anxiety. Maternal education level-Higher maternal education less likely anxiety. General psychiatric morbidity | About 29% (n = 161) of the students had mild to severe anxiety symptoms (20.7% mild, 7.1% moderate, and 0.9% severe) Overall, out of 560 health sciences students, 56 (10%) students had mild to severe depressive symptoms; of those, 37 (6.6%) were mild, 10 (1.8%) were moderate, and 9 (1.6%) were severe |
| Turan et al., 2021 [83] | Turkey | Cross-sectional | Nursing students 456 | Mean = 21.09 ± 2.41 | Anxiety scale Attitude Scale for Nursing Profession | Female gender, Third-year students, People who chose the profession willingly, Students who did not think about changing the profession of nursing and those who did not have anxieties about the profession | Anxiety was prevalent in 43.2% of the participants |
| van Venrooij et al., (2017) [84] | Netherlands | Cross-sectional | 433 medical students RR = 33.0% | Mean = 21.2 years | Depression and anxiety-related symptoms and vitality using the Symptom Questionnaire-48 (SQ-48) | Low optimism Low happiness High need for recovery | Depression and anxiety related symptoms—46.0% Depression—27.0% Anxiety—29.1% |
| Van der Walt et al., 2020 [85] | South Africa | cross-sectional | 473 medical students RR = 97.3% | Age = 22 years | Patient Health Questionnaire-9 Hospital Anxiety and Depression Scale | Students who undertook the 2017 mini-semester Female sex | 36.4% were above the cut-off for major depressive disorder and 45.9% for anxiety disorder Reported rates of disorders diagnosed by a health professional were 25.0% for depressive disorder and 20.5% for anxiety disorder |
| Yusof et al., 2020 [25] | Malaysia | Cross-sectional | 610 Pharmacy students RR = 20.3% | AR = 18–29 years | Depression Anxiety Stress Scale-42 (DASS-42) | Students who did not have depression, students who smoke, have separated parents, with a family history of mental illness, had a recent loss of someone close, and with lower GPAs were statistically significantly associated with depression | 47.4% were having depression of different severity |
| Yuan et al., 2021 [86] | China | Cross-sectional | 519/5550 medical students RR = 9.4% | AR = 16–42 | Generalized Anxiety Disorder-7 (GAD-7) Patient Health Questionnaire-9 (PHQ-9) Simplified Coping Style Questionnaire (SCSQ) Perceived Stress Scale (PSS-10) Multidimensional Scale of Perceived Social Support (MSPSS) Revised Life Orientation Test (LOT-R) Resilience Scale- 14 (RS-14) | Stressors in school- Increase anxiety and depression. Negative coping style perceived stress | The prevalence of anxiety symptoms in the sample population was 28.5% The prevalence of depressive symptoms in the sample population was 31.6% |
| Zakeri et al., (2021) [87] | United States | Cross-sectional | 238 pharmacy students RR = 63% | NR | Counselling Center Assessment of Psychological Symptoms instrument (CCAPS-62) | High academic distress and high family distress were associated with a greater probability of a student having high general anxiety. | Anxiety—50% |
| Zeng et al., 2019 [88] | China | Cross-sectional | 544 nursing students RR = 89.9% | AR = 17–24 years | Depression, Anxiety and Stress Scale 21 (DASS 21) | Reduced engagement in physical and other leisure activities Poor sleep quality, experience of negative life events, poor self-perceived mental health | Depression—28.7% Anxiety—41.7% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agyapong-Opoku, G.; Agyapong, B.; Obuobi-Donkor, G.; Eboreime, E. Depression and Anxiety among Undergraduate Health Science Students: A Scoping Review of the Literature. Behav. Sci. 2023, 13, 1002. https://doi.org/10.3390/bs13121002
Agyapong-Opoku G, Agyapong B, Obuobi-Donkor G, Eboreime E. Depression and Anxiety among Undergraduate Health Science Students: A Scoping Review of the Literature. Behavioral Sciences. 2023; 13(12):1002. https://doi.org/10.3390/bs13121002
Chicago/Turabian StyleAgyapong-Opoku, Gerald, Belinda Agyapong, Gloria Obuobi-Donkor, and Ejemai Eboreime. 2023. "Depression and Anxiety among Undergraduate Health Science Students: A Scoping Review of the Literature" Behavioral Sciences 13, no. 12: 1002. https://doi.org/10.3390/bs13121002
APA StyleAgyapong-Opoku, G., Agyapong, B., Obuobi-Donkor, G., & Eboreime, E. (2023). Depression and Anxiety among Undergraduate Health Science Students: A Scoping Review of the Literature. Behavioral Sciences, 13(12), 1002. https://doi.org/10.3390/bs13121002