
Getting Good Sleep with Family Support: The Role of Fear of Crime and Loneliness

Abstract
:1. Introduction
1.1. Family Support and Sleep Quality
1.2. The Mediating Role of FOC between Family Support and Sleep Quality
1.3. The Mediating Role of Loneliness between Family Support and Sleep Quality
1.4. The Chain Mediating Effect of FOC and Loneliness
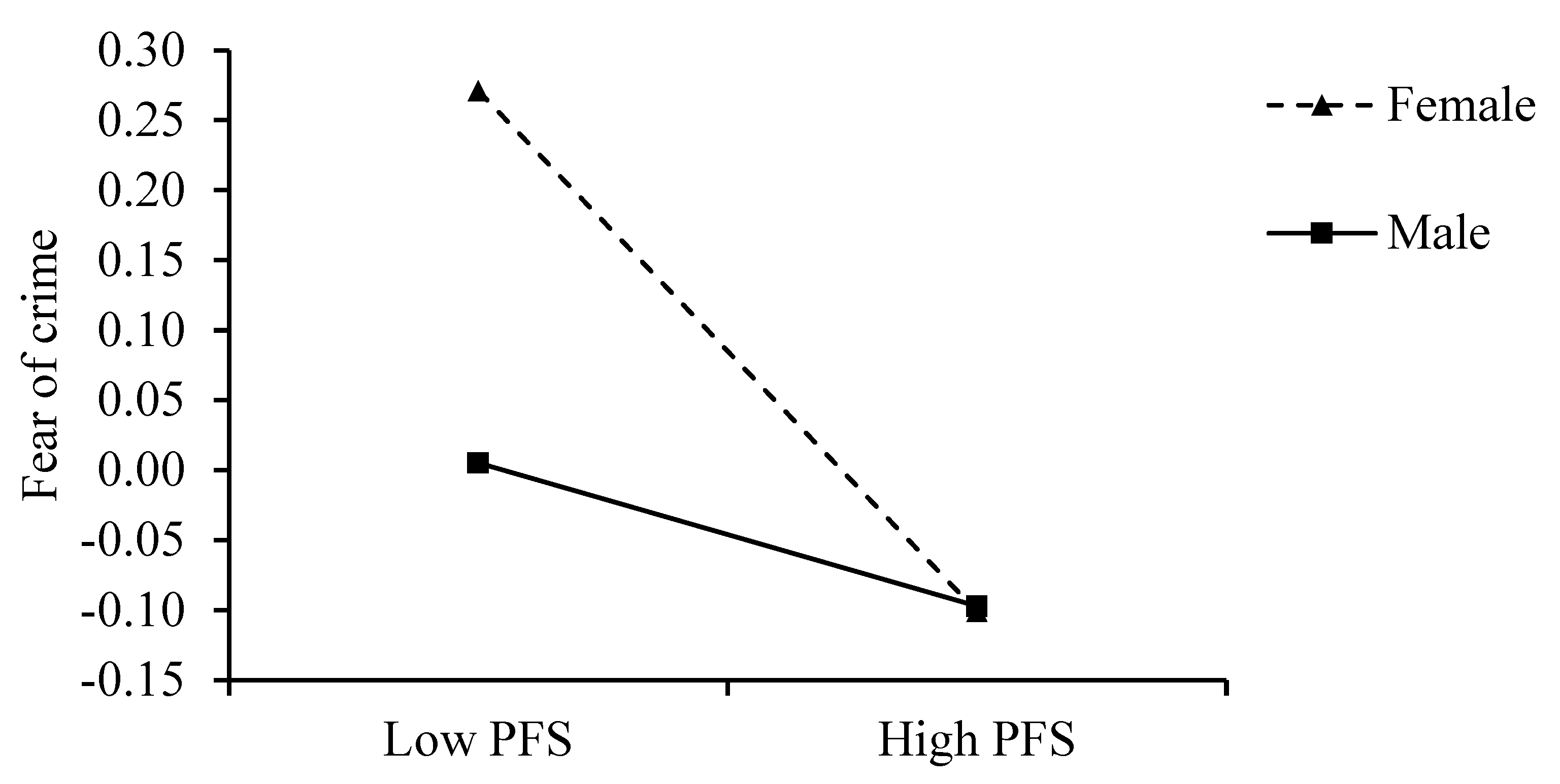
1.5. Regulatory Role of Gender
2. Materials and Methods
2.1. Sample and Procedure
2.2. Measures
2.2.1. Family Support
2.2.2. Fear of Crime (FOC)
2.2.3. Loneliness
2.2.4. Sleep Quality
2.2.5. Control Variables
2.3. Data Analysis
3. Results
3.1. Results of Descriptive Statistical Analysis
3.2. Common Method Bias Test
3.3. The Direct Impact of Family Support on Sleep Quality
3.4. Family Support Affects Sleep Quality through FOC and Loneliness
3.5. Moderating Effect of Gender
3.6. Outcomes without Control Variables
4. Discussion
4.1. Theoretical Implications
4.2. Practical Implications
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kent, R.G.; Uchino, B.N.; Cribbet, M.R.; Bowen, K.; Smith, T.W. Social relationships and sleep quality. Ann. Behav. Med. 2015, 49, 912–917. [Google Scholar] [CrossRef] [PubMed]
- Lewis, L.D. The interconnected causes and consequences of sleep in the brain. Science 2021, 374, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Kim, K.; Burr, J.A.; Wu, B. Longitudinal associations between parent–child relationship quality and insomnia for aging parents: The mediating role of depressive symptoms. Soc. Sci. Med. 2020, 253, 112972. [Google Scholar] [CrossRef] [PubMed]
- Ben Simon, E.; Walker, M.P. Sleep loss causes social withdrawal and loneliness. Nat. Commun. 2018, 9, 3146. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Sleep duration and all-cause mortality: A systematic review and meta-analysis of prospective studies. Sleep 2010, 33, 585–592. [Google Scholar] [CrossRef]
- Connolly, E.J.; Jackson, D.B.; Semenza, D.C. Quality over quantity? Using sibling comparisons to examine relations between sleep quality, sleep duration, and delinquency. Soc. Sci. Med. 2021, 280, 114053. [Google Scholar] [CrossRef]
- Park, G.-R.; Kim, J. Adolescent sleep duration and cardiometabolic risk in adulthood: Evidence from sibling comparison designs with biomarker data. Health Psychol. 2022, 41, 683–692. [Google Scholar] [CrossRef]
- Barber, L.K.; Taylor, S.G.; Burton, J.P.; Bailey, S.F. A self-regulatory perspective of work-to-home undermining spillover/crossover: Examining the roles of sleep and exercise. J. Appl. Psychol. 2017, 102, 753–763. [Google Scholar] [CrossRef]
- Gordon, A.M.; Carrillo, B.; Barnes, C.M. Sleep and social relationships in healthy populations: A systematic review. Sleep Med. Rev. 2021, 57, 101428. [Google Scholar] [CrossRef]
- Kane, H.S.; Krizan, Z. Sleep, emotional supportiveness, and socially straining behavior: A multidimensional approach. Sleep Health 2021, 7, 49–55. [Google Scholar] [CrossRef]
- Chung, J. Social support, social strain, sleep quality, and actigraphic sleep characteristics: Evidence from a national survey of US adults. Sleep Health 2017, 3, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Gorgol, J.; Stolarski, M.; Bullock, B. The mediating role of perceived social support in the relationship between morningness–eveningness and subjective well-being. J. Sleep Res. 2022, 31, e13520. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Ishikuro, M.; Obara, T.; Ueno, F.; Noda, A.; Onuma, T.; Matsuzaki, F.; Kikuchi, S.; Kobayashi, N.; Hamada, H.; et al. Social isolation and insomnia among pregnant women in Japan: The Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study. Sleep Health 2022, 8, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef] [PubMed]
- Kent de Grey, R.G.; Uchino, B.N.; Trettevik, R.; Cronan, S.; Hogan, J.N. Social support and sleep: A meta-analysis. Health Psychol. 2018, 38, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Stafford, M.; Bendayan, R.; Tymoszuk, U.; Kuh, D. Social support from the closest person and sleep quality in later life: Evidence from a British birth cohort study. J. Psychosom. Res. 2017, 98, 1–9. [Google Scholar] [CrossRef]
- Troxel, W.M.; Buysse, D.J.; Monk, T.H.; Begley, A.; Hall, M. Does social support differentially affect sleep in older adults with versus without insomnia? J. Psychosom. Res. 2010, 69, 459–466. [Google Scholar] [CrossRef]
- Mesas, A.E.; Peppard, P.E.; Hale, L.; Friedman, E.M.; Nieto, F.J.; Hagen, E.W. Individuals’ perceptions of social support from family and friends are associated with lower risk of sleep complaints and short sleep duration. Sleep Health 2020, 6, 110–116. [Google Scholar] [CrossRef]
- Selcuk, E.; Stanton, S.C.E.; Slatcher, R.B.; Ong, A.D. Perceived partner responsiveness predicts better sleep quality through lower anxiety. Soc. Psychol. Personal. Sci. 2016, 8, 83–92. [Google Scholar] [CrossRef]
- Jordan, L.; Hoang, A.P.; Chui, C.H.K.; Wang, W.; Mazzucato, V. Multiple precarity and intimate family life among African-Chinese families in Guangzhou. J. Ethn. Migr. Stud. 2021, 47, 2796–2814. [Google Scholar] [CrossRef]
- Miller, G.E.; Brody, G.H.; Yu, T.; Chen, E. A family-oriented psychosocial intervention reduces inflammation in low-SES African American youth. Proc. Natl. Acad. Sci. USA 2014, 111, 11287–11292. [Google Scholar] [CrossRef] [PubMed]
- Noble, K.G.; Houston, S.M.; Brito, N.H.; Bartsch, H.; Kan, E.; Kuperman, J.M.; Akshoomoff, N.; Amaral, D.G.; Bloss, C.S.; Libiger, O.; et al. Family income, parental education and brain structure in children and adolescents. Nat. Neurosci. 2015, 18, 773–778. [Google Scholar] [CrossRef] [PubMed]
- French, K.A.; Dumani, S.; Allen, T.D.; Shockley, K.M. A meta-analysis of work–family conflict and social support. Psychol. Bull. 2018, 144, 284–314. [Google Scholar] [CrossRef] [PubMed]
- García-Pérez, O.; Inda-Caro, M.; Fernández-García, C.-M.; Torío-López, S. The influence of perceived family supports and barriers on personal variables in a Spanish sample of secondary school science-technology students. Int. J. Sci. Educ. 2020, 42, 70–88. [Google Scholar] [CrossRef]
- Miller, J.G.; Kahle, S.; Hastings, P.D. Roots and benefits of costly giving: Children who are more altruistic have greater autonomic flexibility and less family wealth. Psychol. Sci. 2015, 26, 1038–1045. [Google Scholar] [CrossRef]
- Uchino, B.N.; Baucom, B.R.W.; Landvatter, J.; de Grey, R.G.K.; Tacana, T.; Flores, M.; Ruiz, J.M. Perceived social support and ambulatory blood pressure during daily life: A meta-analysis. J. Behav. Med. 2022, 45, 509–517. [Google Scholar] [CrossRef]
- Xian, X.; Zhang, Y.; Bai, A.; Zhai, X.; Hu, H.; Zhang, J.; Ye, M. Association between family support, stress, and sleep quality among college students during the COVID-19 online learning period. Int. J. Environ. Res. Public Health 2023, 20, 248. [Google Scholar] [CrossRef]
- Cullen, F.T. Social support as an organizing concept for criminology: Presidential address to the academy of criminal justice sciences. Justice Q. 1994, 11, 527–559. [Google Scholar] [CrossRef]
- Feeney, B.C.; Collins, N.L. A new look at social support: A theoretical perspective on thriving through relationships. Personal. Soc. Psychol. Rev. 2015, 19, 113–147. [Google Scholar] [CrossRef] [PubMed]
- Kent de Grey, R.G.; Uchino, B.N.; Pietromonaco, P.R.; Hogan, J.N.; Smith, T.W.; Cronan, S.; Trettevik, R. Strained bedfellows: An actor–partner analysis of spousal attachment insecurity and sleep quality. Ann. Behav. Med. 2019, 53, 115–125. [Google Scholar] [CrossRef]
- Leschak, C.J.; Eisenberger, N.I. Two distinct immune pathways linking social relationships with health: Inflammatory and antiviral processes. Psychosom. Med. 2019, 81, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Uchino, B.N.; Bowen, K.; Kent de Grey, R.; Mikel, J.; Fisher, E.B. Social support physical health: Models mechanisms opportunities. In Principles and Concepts of Behavioral Medicine: A Global Handbook; Fisher, E.B., Cameron, L.D., Christensen, A.J., Ehlert, U., Guo, Y., Oldenburg, B., Snoek, F.J., Eds.; Springer: New York, NY, USA, 2018; pp. 341–372. [Google Scholar] [CrossRef]
- Zambrano, D.N.; Mindell, J.A.; Reyes, N.R.; Hart, C.N.; Herring, S.J. “It’s not all about my baby’s sleep”: A qualitative study of factors influencing low-income African American mothers’ sleep quality. Behav. Sleep Med. 2016, 14, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Chopik, W.J.; Schiamberg, L.B. Longitudinal associations between marital quality and sleep quality in older adulthood. J. Behav. Med. 2017, 40, 821–831. [Google Scholar] [CrossRef] [PubMed]
- Troxel, W.M. It’s more than sex: Exploring the dyadic nature of sleep and implications for health. Psychosom. Med. 2010, 72, 578–586. [Google Scholar] [CrossRef]
- Hardyns, W.; Pauwels, L.J.R.; Heylen, B. Within-individual change in social support, perceived collective efficacy, perceived disorder and fear of crime: Results from a two-wave panel study. Br. J. Criminol. 2018, 58, 1254–1270. [Google Scholar] [CrossRef]
- Zee, K.S.; Bolger, N.; Higgins, E.T. Regulatory effectiveness of social support. J. Personal. Soc. Psychol. 2020, 119, 1316–1358. [Google Scholar] [CrossRef]
- Uchino, B.N. Understanding the links between social support and physical health: A life-span perspective with emphasis on the separability of perceived and received support. Perspect. Psychol. Sci. 2009, 4, 236–255. [Google Scholar] [CrossRef]
- Goh, Z.; Ilies, R.; Wilson, K.S. Supportive supervisors improve employees’ daily lives: The role supervisors play in the impact of daily workload on life satisfaction via work–family conflict. J. Vocat. Behav. 2015, 89, 65–73. [Google Scholar] [CrossRef]
- Wang, D.; Uzzi, B. Weak ties, failed tries, and success. Science 2022, 377, 1256–1258. [Google Scholar] [CrossRef]
- Moran, K.; McDonald, J.; Jackson, A.; Turnbull, S.; Minnis, H. A study of Attachment Disorders in young offenders attending specialist services. Child Abus. Negl. 2017, 65, 77–87. [Google Scholar] [CrossRef]
- Haushofer, J.; Fehr, E. On the psychology of poverty. Science 2014, 344, 862–867. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.; Farrington, D.P.; Sekol, I. Children’s antisocial behavior, mental health, drug use, and educational performance after parental incarceration: A systematic review and meta-analysis. Psychol. Bull. 2012, 138, 175–210. [Google Scholar] [CrossRef]
- Kincade, L.L.; Fox, C.A. “Runs in the family”: Fear of police violence and separation among Black families in central Alabama. Psychol. Violence 2022, 12, 221–230. [Google Scholar] [CrossRef]
- Lorenc, T.; Clayton, S.; Neary, D.; Whitehead, M.; Petticrew, M.; Thomson, H.; Cummins, S.; Sowden, A.; Renton, A. Crime, fear of crime, environment, and mental health and wellbeing: Mapping review of theories and causal pathways. Health Place 2012, 18, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Qin, N.; Yan, E.C.W.; Lai, D.W.L. Perceived victimization risk, avoidance behavior, and health of community-dwelling older adults in urban China. Aging Ment. Health 2020, 24, 171–177. [Google Scholar] [CrossRef]
- Ross, C.E. Fear of victimization and health. J. Quant. Criminol. 1993, 9, 159–175. [Google Scholar] [CrossRef]
- Stafford, M.; Chandola, T.; Marmot, M. Association between fear of crime and mental health and physical functioning. Am. J. Public Health 2007, 97, 2076–2081. [Google Scholar] [CrossRef]
- Domènech-Abella, J.; Switsers, L.; Mundó, J.; Dierckx, E.; Dury, S.; De Donder, L. The association between perceived social and physical environment and mental health among older adults: Mediating effects of loneliness. Aging Ment. Health 2021, 25, 962–968. [Google Scholar] [CrossRef]
- Estrella, M.L.; Durazo-Arvizu, R.A.; Gallo, L.C.; Isasi, C.R.; Perreira, K.M.; Vu, T.H.T.; Vasquez, E.; Sachdeva, S.; Zeng, D.; Llabre, M.M.; et al. Associations between perceived neighborhood environment and cognitive function among middle-aged and older women and men: Hispanic Community Health Study/Study of Latinos Sociocultural Ancillary Study. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 55, 685–696. [Google Scholar] [CrossRef]
- Rader, N.E.; Rogers, S.A.; Cossman, J.S. Physical health, mental health, and fear of crime among college students: A consideration of sex differences. Violence Against Women 2019, 26, 3–23. [Google Scholar] [CrossRef]
- Hale, L.; Hill, T.D.; Friedman, E.; Nieto, F.J.; Galvao, L.W.; Engelman, C.D.; Malecki, K.M.; Peppard, P.E. Perceived neighborhood quality, sleep quality, and health status: Evidence from the Survey of the Health of Wisconsin. Soc. Sci. Med. 2013, 79, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Simonelli, G.; Patel, S.R.; Rodríguez-Espínola, S.; Pérez-Chada, D.; Salvia, A.; Cardinali, D.P.; Vigo, D.E. The impact of home safety on sleep in a Latin American country. Sleep Health 2015, 1, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Hill, T.D.; Trinh, H.N.; Wen, M.; Hale, L. Perceived neighborhood safety and sleep quality: A global analysis of six countries. Sleep Med. 2016, 18, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, J.T.; Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Thisted, R.A. Loneliness as a specific risk factor for depressive symptoms: Cross-sectional and longitudinal analyses. Psychol. Aging 2006, 21, 140–151. [Google Scholar] [CrossRef]
- Ernst, M.; Klein, E.M.; Beutel, M.E.; Brähler, E. Gender-specific associations of loneliness and suicidal ideation in a representative population sample: Young, lonely men are particularly at risk. J. Affect. Disord. 2021, 294, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Pieters, R. Bidirectional dynamics of materialism and loneliness: Not just a vicious cycle. J. Consum. Res. 2013, 40, 615–631. [Google Scholar] [CrossRef]
- Stewart, C.C.; Yu, L.; Glover, C.M.; Mottola, G.; Bennett, D.A.; Wilson, R.S.; Boyle, P.A. Loneliness interacts with cognition in relation to healthcare and financial decision making among community-dwelling older adults. Gerontologist 2020, 60, 1476–1484. [Google Scholar] [CrossRef]
- Lou, V.W.Q.; Ng, J.W. Chinese older adults’ resilience to the loneliness of living alone: A qualitative study. Aging Ment. Health 2012, 16, 1039–1046. [Google Scholar] [CrossRef]
- Vasileiou, K.; Barnett, J.; Barreto, M.; Vines, J.; Atkinson, M.; Long, K.; Bakewell, L.; Lawson, S.; Wilson, M. Coping with loneliness at University: A qualitative interview study with students in the UK. Ment. Health Prev. 2019, 13, 21–30. [Google Scholar] [CrossRef]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Ann. Behav. Med. 2010, 40, 218–227. [Google Scholar] [CrossRef]
- Masi, C.M.; Chen, H.H.-Y.; Hawkley, L.; Cacioppo, J.T. A meta-analysis of interventions to reduce loneliness. Personal. Soc. Psychol. Rev. 2011, 15, 219–266. [Google Scholar] [CrossRef] [PubMed]
- Gerst-Emerson, K.; Jayawardhana, J. Loneliness as a public health issue: The impact of loneliness on health care utilization among older adults. Am. J. Public Health 2015, 105, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhu, R.; Shiv, B. The lonely consumer: Loner or conformer? J. Consum. Res. 2011, 38, 1116–1128. [Google Scholar] [CrossRef]
- Cacioppo, S.; Capitanio, J.P.; Cacioppo, J.T. Toward a neurology of loneliness. Psychol. Bull. 2014, 140, 1464–1504. [Google Scholar] [CrossRef]
- Williams, N.J.; Grandner, M.A.; Wallace, D.M.; Cuffee, Y.; Airhihenbuwa, C.; Okuyemi, K.; Ogedegbe, G.; Jean-Louis, G. Social and behavioral predictors of insufficient sleep among African Americans and Caucasians. Sleep Med. 2016, 18, 103–107. [Google Scholar] [CrossRef]
- Aanes, M.M.; Hetland, J.; Pallesen, S.; Mittelmark, M.B. Does loneliness mediate the stress-sleep quality relation? The Hordaland Health Study. Int. Psychogeriatr. 2011, 23, 994–1002. [Google Scholar] [CrossRef]
- Salmi, V.; Smolej, M.; Kivivuori, J. Crime victimization, exposure to crime news and social trust among adolescents. Young 2007, 15, 255–272. [Google Scholar] [CrossRef]
- Singer, A.J.; Chouhy, C.; Lehmann, P.S.; Walzak, J.N.; Gertz, M.; Biglin, S. Victimization, fear of Crime, and trust in criminal justice institutions: A cross-national analysis. Crime Delinq. 2019, 65, 822–844. [Google Scholar] [CrossRef]
- McNeeley, S.; Stutzenberger, A. Victimization, risk perception, and the desire to move. Vict. Offenders 2013, 8, 446–464. [Google Scholar] [CrossRef]
- Näsi, M.; Tanskanen, M.; Kivivuori, J.; Haara, P.; Reunanen, E. Crime news consumption and fear of violence: The role of traditional media, social media, and alternative information sources. Crime Delinq. 2020, 67, 574–600. [Google Scholar] [CrossRef]
- Yuan, Y.; McNeeley, S. Reactions to crime: A multilevel analysis of fear of crime and defensive and participatory behavior. J. Crime Justice 2016, 39, 455–472. [Google Scholar] [CrossRef]
- Maruthaveeran, S.; van den Bosh, C.K. Fear of crime in urban parks—What the residents of Kuala Lumpur have to say? Urban For. Urban Green. 2015, 14, 702–713. [Google Scholar] [CrossRef]
- Lee, J.M.-L.; Ang, S.; Chan, A. Fear of crime is associated with loneliness among older adults in Singapore: Gender and ethnic differences. Health Soc. Care Community 2021, 29, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- van Eijk, G. Between risk and resistance: Gender socialization, equality, and ambiguous norms in fear of crime and safekeeping. Fem. Criminol. 2015, 12, 103–124. [Google Scholar] [CrossRef]
- Silva, C.; Guedes, I. The role of the media in the fear of crime: A qualitative study in the Portuguese context. Crim. Justice Rev. 2022, 48, 300–317. [Google Scholar] [CrossRef]
- Finkel, E.J.; Simpson, J.A.; Eastwick, P.W. The psychology of close relationships: Fourteen core principles. Annu. Rev. Psychol. 2017, 68, 383–411. [Google Scholar] [CrossRef]
- Bhardwaj, N.; Apel, R. Societal gender inequality and the gender gap in safety perceptions: Comparative evidence from the International Crime Victims Survey. Eur. J. Criminol. 2022, 19, 746–766. [Google Scholar] [CrossRef]
- Macassa, G.; Winersjö, R.; Wijik, K.; Magrath, C.; Ahmadi, N.; Soares, J. Fear of crime and its relationship with self-reported health and stress among men. J. Public Health Res. 2017, 6, 1010. [Google Scholar] [CrossRef]
- Reid, L.W.; Konrad, M. The gender gap in fear: Assessing the interactive effects of gender and perceived risk on fear of crime. Sociol. Spectr. 2004, 24, 399–425. [Google Scholar] [CrossRef]
- Chataway, M.; Bourke, A. Fear of crime disorder quality of life. In Geographies of Behavioural Health, Crime, and Disorder; Lersch, K.M., Chakraborty, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2020; Volume 126, pp. 137–163. [Google Scholar] [CrossRef]
- Cossman, J.S.; Rader, N.E. Fear of crime and personal vulnerability: Examining self-reported health. Sociol. Spectr. 2011, 31, 141–162. [Google Scholar] [CrossRef]
- Jackson, J. A psychological perspective on vulnerability in the fear of crime. Psychol. Crime Law 2009, 15, 365–390. [Google Scholar] [CrossRef]
- Snedker, K.A. Explaining the gender gap in fear of crime: Assessments of risk and vulnerability among New York City residents. Fem. Criminol. 2011, 7, 75–111. [Google Scholar] [CrossRef]
- Rader, N.E.; Cossman, J.S.; Porter, J.R. Fear of crime and vulnerability: Using a national sample of Americans to examine two competing paradigms. J. Crim. Justice 2012, 40, 134–141. [Google Scholar] [CrossRef]
- Callanan, V.; Rosenberger, J.S. Media, gender, and fear of crime. Crim. Justice Rev. 2015, 40, 322–339. [Google Scholar] [CrossRef]
- Lemaster, P.; Strough, J. Beyond Mars and Venus: Understanding gender differences in financial risk tolerance. J. Econ. Psychol. 2014, 42, 148–160. [Google Scholar] [CrossRef]
- Fetchenhauer, D.; Buunk, B.P. How to explain gender differences in fear of crime: Towards an evolutionary approach. Sex. Evol. Gend. 2005, 7, 95–113. [Google Scholar] [CrossRef]
- Fox, K.A.; Nobles, M.R.; Fisher, B.S. A multi-theoretical framework to assess gendered stalking victimization: The utility of self-control, social learning, and control balance theories. Justice Q. 2016, 33, 319–347. [Google Scholar] [CrossRef]
- Cops, D.; Pleysier, S. ‘Doing gender’ in fear of crime: The impact of gender identity on reported levels of fear of crime in adolescents and young adults. Br. J. Criminol. 2011, 51, 58–74. [Google Scholar] [CrossRef]
- Martin, A.E. The divergent effects of diversity ideologies for race and gender relations. Organ. Behav. Hum. Decis. Process. 2023, 175, 104226. [Google Scholar] [CrossRef]
- Logan, T.K.; Walker, R. The gender safety gap: Examining the impact of victimization history, perceived risk, and personal control. J. Interpers. Violence 2017, 36, 603–631. [Google Scholar] [CrossRef]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef]
- Grinshteyn, E.; Muennig, P.; Pabayo, R. Using the General Social Survey-National Death Index cohort to study the relationship between neighbourhood fear and mortality in the USA. BMJ Open 2019, 9, e030330. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.W. UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. J. Personal. Assess. 1996, 66, 20–40. [Google Scholar] [CrossRef]
- Allen, D.G.; Peltokorpi, V.; Rubenstein, A.L. When “embedded” means “stuck”: Moderating effects of job embeddedness in adverse work environments. J. Appl. Psychol. 2016, 101, 1670–1686. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, C.; Oswald, A.J. The scientific value of numerical measures of human feelings. Proc. Natl. Acad. Sci. USA 2022, 119, e2210412119. [Google Scholar] [CrossRef]
- Bernerth, J.B.; Aguinis, H. A critical review and best-practice recommendations for control variable usage. Pers. Psychol. 2016, 69, 229–283. [Google Scholar] [CrossRef]
- Griskevicius, V.; Tybur, J.M.; Delton, A.W.; Robertson, T.E. The influence of mortality and socioeconomic status on risk and delayed rewards: A life history theory approach. J. Personal. Soc. Psychol. 2011, 100, 1015–1026. [Google Scholar] [CrossRef]
- Durante, K.M.; Griskevicius, V.; Redden, J.P.; White, A.E. Spending on daughters versus sons in economic recessions. J. Consum. Res. 2015, 42, 435–457. [Google Scholar] [CrossRef]
- Edwards, J.R.; Lambert, L.S. Methods for integrating moderation and mediation: A general analytical framework using moderated path analysis. Psychol. Methods 2007, 12, 1–22. [Google Scholar] [CrossRef]
- Aiken, L.S.; West, S.G. Multiple Regression: Testing and Interpreting Interactions; Sage: Thousand Oaks, CA, USA, 1991. [Google Scholar]
- Lindell, M.K.; Whitney, D.J. Accounting for common method variance in cross-sectional research designs. J. Appl. Psychol. 2001, 86, 114–121. [Google Scholar] [CrossRef]
- Malhotra, N.K.; Kim, S.S.; Patil, A. Common method variance in IS research: A comparison of alternative approaches and a reanalysis of past research. Manag. Sci. 2006, 52, 1865–1883. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; Organ, D.W. Self-reports in organizational research: Problems and prospects. J. Manag. 1986, 12, 531–544. [Google Scholar] [CrossRef]
- Muller, D.; Judd, C.M.; Yzerbyt, V.Y. When moderation is mediated and mediation is moderated. J. Personal. Soc. Psychol. 2005, 89, 852–863. [Google Scholar] [CrossRef] [PubMed]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation analysis. Annu. Rev. Psychol. 2007, 58, 593–614. [Google Scholar] [CrossRef] [PubMed]
- Becker, T.E. Potential problems in the statistical control of variables in organizational research: A qualitative analysis with recommendations. Organ. Res. Methods 2005, 8, 274–289. [Google Scholar] [CrossRef]
- York, R. Control variables and causal inference: A question of balance. Int. J. Soc. Res. Methodol. 2018, 21, 675–684. [Google Scholar] [CrossRef]
- Semenza, D.C.; Gentina, E. Sleep and delinquency: The context of self-control, social support, and sex differences among French adolescents. Eur. J. Criminol. 2023, 20, 878–904. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. PFS | 5.35 | 1.26 | |||||||||
| 2. FOC | 1.60 | 0.66 | −0.16 *** | ||||||||
| 3. LLN | 1.71 | 0.76 | −0.24 *** | 0.17 *** | |||||||
| 4. SQ | 5.03 | 1.44 | 0.11 *** | −0.18 *** | −0.15 *** | ||||||
| 5. Gender | 0.56 | 0.50 | −0.01 | −0.10 ** | −0.02 | 0.02 | |||||
| 6. Age | 64.87 | 11.52 | 0.02 | −0.15 *** | 0.04 | 0.01 | 0.07 * | ||||
| 7. Edu | 0.51 | 0.50 | 0.10 ** | 0.02 | −0.10 ** | −0.00 | 0.16 *** | −0.29 *** | |||
| 8. MS | 0.91 | 0.29 | 0.16 *** | 0.05 | −0.10 ** | 0.05 | −0.00 | −0.18 *** | 0.15 *** | ||
| 9. LA | 0.13 | 0.34 | −0.15 *** | −0.01 | 0.16 *** | −0.06 | 0.01 | 0.18 *** | −0.20 *** | −0.59 *** | |
| 10. SES | 3.08 | 1.18 | 0.15 *** | −0.01 | −0.08 ** | 0.07* | −0.03 | −0.03 | 0.28 *** | 0.07 * | −0.08 ** |
| Variables | B | SE | p | Bootstrapped 95% CI | |
|---|---|---|---|---|---|
| LL | UL | ||||
| Mediator = FOC | |||||
| PFS | −0.090 | 0.018 | <0.001 | −0.126 | −0.055 |
| Age | −0.008 | 0.002 | <0.001 | −0.012 | −0.005 |
| Edu | −0.054 | 0.046 | 0.236 | −0.144 | 0.037 |
| MS | 0.188 | 0.085 | 0.027 | 0.018 | 0.353 |
| LA | 0.075 | 0.080 | 0.346 | −0.079 | 0.235 |
| SES | 0.008 | 0.019 | 0.698 | −0.031 | 0.046 |
| Mediator = Loneliness | |||||
| PFS | −0.124 | 0.023 | <0.001 | −0.168 | −0.081 |
| FOC | 0.175 | 0.039 | <0.001 | 0.098 | 0.251 |
| Age | 0.003 | 0.002 | 0.182 | −0.001 | 0.007 |
| Edu | −0.020 | 0.050 | 0.694 | −0.115 | 0.078 |
| MS | −0.028 | 0.113 | 0.805 | −0.249 | 0.193 |
| LA | 0.233 | 0.099 | 0.018 | 0.046 | 0.434 |
| SES | −0.021 | 0.021 | 0.308 | −0.061 | 0.021 |
| Outcome variable = SQ | |||||
| PFS | 0.068 | 0.039 | 0.087 | −0.010 | 0.144 |
| FOC | −0.294 | 0.071 | <0.001 | −0.439 | −0.159 |
| LLN | −0.229 | 0.064 | <0.001 | −0.359 | −0.105 |
| Age | −0.001 | 0.004 | 0.773 | −0.009 | 0.007 |
| Edu | −0.140 | 0.098 | 0.152 | −0.333 | 0.048 |
| MS | 0.120 | 0.208 | 0.563 | −0.297 | 0.518 |
| LA | −0.074 | 0.176 | 0.676 | −0.429 | 0.265 |
| SES | 0.075 | 0.043 | 0.080 | −0.010 | 0.158 |
| PFS → FOC → SQ | 0.026 | 0.008 | 0.002 | 0.013 | 0.047 |
| PFS → LL → SQ | 0.028 | 0.009 | 0.003 | 0.013 | 0.051 |
| PFS → FOC → LL → SQ | 0.004 | 0.002 | 0.022 | 0.001 | 0.008 |
| Variables | B | SE | p | Bootstrapped 95% CI | |
|---|---|---|---|---|---|
| LL | UL | ||||
| Mediator = FOC | |||||
| PFS | −0.154 | 0.028 | <0.001 | −0.210 | −0.100 |
| Gender | −0.131 | 0.045 | 0.003 | −0.220 | −0.043 |
| PFS × Gender | 0.107 | 0.035 | 0.002 | 0.040 | 0.176 |
| Age | −0.008 | 0.002 | <0.001 | −0.012 | −0.005 |
| Edu | −0.027 | 0.046 | 0.554 | −0.118 | 0.064 |
| MS | 0.202 | 0.084 | 0.016 | 0.036 | 0.364 |
| LA | 0.099 | 0.080 | 0.212 | −0.054 | 0.256 |
| SES | 0.006 | 0.020 | 0.753 | −0.033 | 0.045 |
| Mediator = Loneliness | |||||
| PFS | −0.124 | 0.023 | <0.001 | −0.168 | −0.081 |
| FOC | 0.173 | 0.039 | <0.001 | 0.097 | 0.249 |
| Gender | −0.033 | 0.048 | 0.492 | −0.125 | 0.061 |
| Age | 0.003 | 0.002 | 0.159 | −0.001 | 0.007 |
| Edu | −0.013 | 0.050 | 0.798 | −0.108 | 0.085 |
| MS | −0.026 | 0.113 | 0.821 | −0.246 | 0.194 |
| LA | 0.235 | 0.099 | 0.017 | 0.049 | 0.435 |
| SES | −0.022 | 0.021 | 0.285 | −0.063 | 0.020 |
| Outcome variable = SQ | |||||
| PFS | 0.068 | 0.040 | 0.085 | −0.011 | 0.145 |
| FOC | −0.292 | 0.071 | <0.001 | −0.437 | −0.156 |
| LLN | −0.229 | 0.065 | <0.001 | −0.358 | −0.104 |
| Gender | 0.040 | 0.095 | 0.675 | −0.151 | 0.221 |
| Age | −0.001 | 0.004 | 0.739 | −0.009 | 0.007 |
| Edu | −0.148 | 0.099 | 0.137 | −0.341 | 0.045 |
| MS | 0.118 | 0.208 | 0.572 | −0.299 | 0.515 |
| LA | −0.075 | 0.176 | 0.669 | −0.429 | 0.264 |
| SES | 0.076 | 0.043 | 0.075 | −0.009 | 0.159 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xia, C.; Xu, J.; Wang, Y. Getting Good Sleep with Family Support: The Role of Fear of Crime and Loneliness. Behav. Sci. 2023, 13, 909. https://doi.org/10.3390/bs13110909
Xia C, Xu J, Wang Y. Getting Good Sleep with Family Support: The Role of Fear of Crime and Loneliness. Behavioral Sciences. 2023; 13(11):909. https://doi.org/10.3390/bs13110909
Chicago/Turabian StyleXia, Chun, Jia Xu, and Yaya Wang. 2023. "Getting Good Sleep with Family Support: The Role of Fear of Crime and Loneliness" Behavioral Sciences 13, no. 11: 909. https://doi.org/10.3390/bs13110909
APA StyleXia, C., Xu, J., & Wang, Y. (2023). Getting Good Sleep with Family Support: The Role of Fear of Crime and Loneliness. Behavioral Sciences, 13(11), 909. https://doi.org/10.3390/bs13110909