
Italian Validation of the Short Version of the Failure to Mentalize Trauma Questionnaire in Adults at Risk Due to Childhood Trauma

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
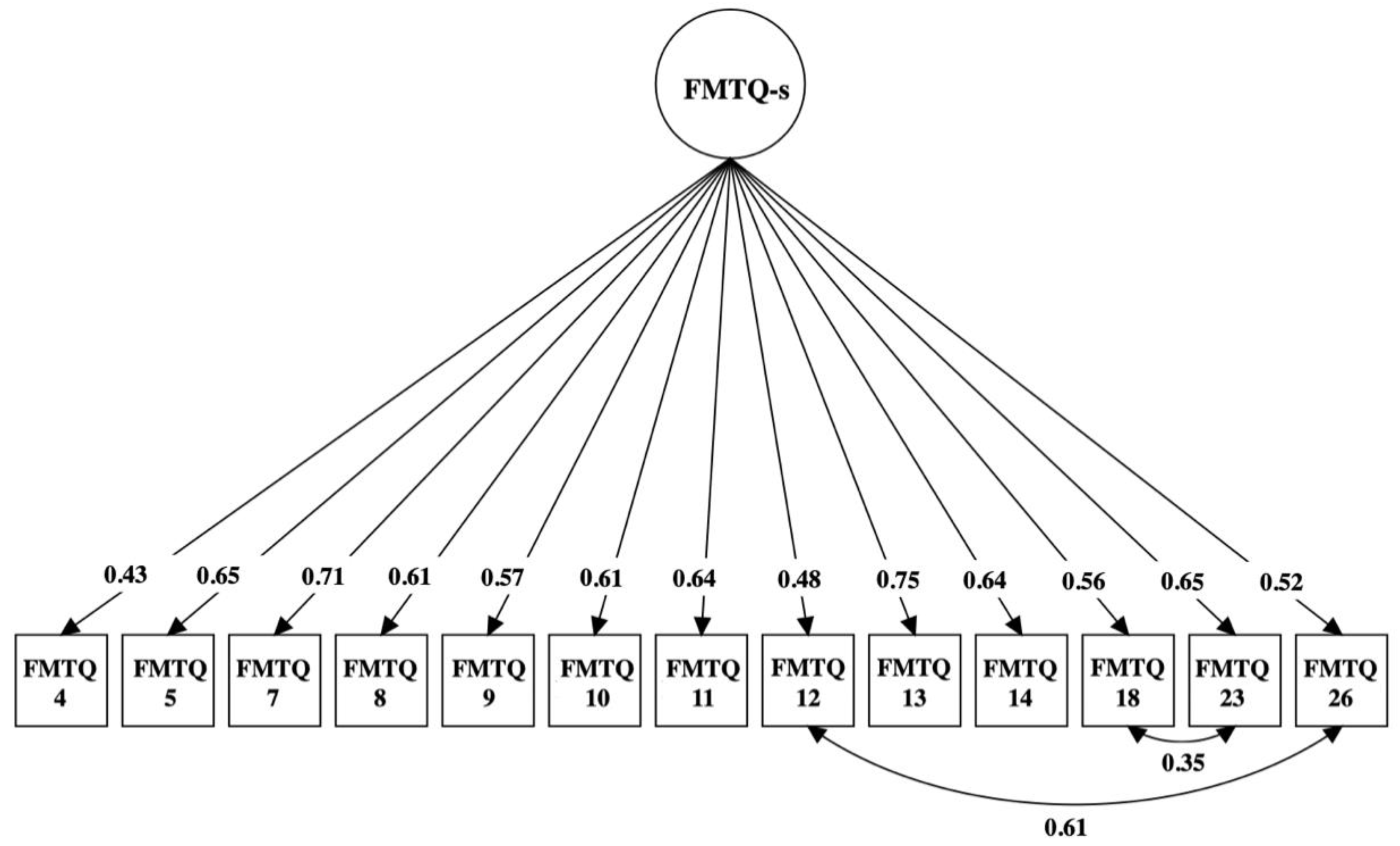
3.1. Factor Structure of the Italian FMTQ-s
3.2. Psychometric Properties of the Italian FMTQ-s
4. Discussion
Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gilgoff, R.; Singh, L.; Koita, K.; Gentile, B.; Silverio Marques, S. Adverse Childhood Experiences, Outcomes, and Interventions. Pediatr. Clin. 2020, 67, 259–273. [Google Scholar] [CrossRef] [PubMed]
- Spinazzola, J.; van der Kolk, B.; Ford, J.D. When Nowhere Is Safe: Interpersonal Trauma and Attachment Adversity as Antecedents of Posttraumatic Stress Disorder and Developmental Trauma Disorder. J. Trauma. Stress 2018, 31, 631–642. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.; Steele, K. Mentalising in complex trauma and dissociative disorders. Eur. J. Trauma Dissociation 2020, 5, 100168. [Google Scholar] [CrossRef]
- MacIntosh, H.B.; Godbout, N.; Dubash, N. Borderline personality disorder: Disorder of trauma or personality, a review of the empirical literature. Can. Psychol. Can. 2015, 56, 227–241. [Google Scholar] [CrossRef]
- Sansone, R.A.; Sansone, L.A. Childhood trauma, borderline personality, and eating disorders: A development cascade. Eat. Disord. 2007, 15, 333–346. [Google Scholar] [CrossRef] [PubMed]
- Annemiek van, D.; Julian, D.F.; Onno van der, H.; Van Son Maarten, J.M.; Van der Heijden, P.G.M.; Bühring, M. Childhood traumatization by primary caretaker and affect dysregulation in patients with borderline personality disorder and somatoform disorder. Eur. J. Psychotraumatol. 2011, 2, 5628. [Google Scholar] [CrossRef]
- Bowlby, J.; Ainsworth, M. The origins of attachment theory. Attach. Theory Soc. Dev. Clin. Perspect. 2013, 45, 759–775. [Google Scholar]
- Kuhar, M.; Zager Kocjan, G. Adverse childhood experiences and somatic symptoms in adulthood: A moderated mediation effects of disturbed self-organization and resilient coping. Psychol. Trauma-US 2022, 14, 1288. [Google Scholar] [CrossRef]
- Buimerr, E.E.; Brouwer, R.M.; Mandi, R.C.; Pas, P.; Schnack, H.G.; Hulshoff Pol, H.E. Adverse childhood experiences and fronto-subcortical structures in the developing brain. Front. Psychiatry 2022, 13, 955871. [Google Scholar] [CrossRef]
- Barral, C.; Meares, R. The holistic project of Pierre Janet: Part Two: Oscillations and becomings: From disintegration to integration. In Rediscovering Pierre Janet; Routledge: London, UK, 2019; pp. 116–128. [Google Scholar]
- Farina, B.; Speranza, A.M.; Dittoni, S.; Gnoni, V.; Trentini, C.; Vergano, C.M.; Liotti, G.; Brunetti, R.; Testani, E.; Della mrca, G. Memories of attachment hamper EEG cortical connectivity in dissociative patients. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 449–458. [Google Scholar] [CrossRef]
- Fonagy, P.; Luyten, P.; Moulton-Perkins, A.; Lee, Y.W.; Warren, F.; Howard, S.; Ghinai, R.; Fearon, P.; Lowyck, B. Development and validation of a self-report measure of mentalizing: The reflective functioning questionnaire. PLoS ONE 2016, 11, e0158678. [Google Scholar] [CrossRef] [PubMed]
- Ensink, K.; Bégin, M.; Normandin, L.; Godbout, N.; Fonagy, P. Mentalization and dissociation in the context of trauma: Implications for child psychopathology. J. Trauma Dissociation 2017, 18, 11–30. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.L.; Fonagy, P.; Feigenbaum, J.; Montague, P.R.; Nolte, T. Multidirectional Pathways between Attachment, Mentalizing, and Posttraumatic Stress Symptomatology in the Context of Childhood Trauma. Psychopathology 2020, 53, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Santoro, G.; Midolo, L.R.; Costanzo, A.; Schimmenti, A. The vulnerability of insecure minds: The mediating role of mentalization in the relationship between attachment styles and psychopathology. Bull. Menninger. Clin. 2021, 85, 358–384. [Google Scholar] [CrossRef]
- Lyuten, P.; Campbell, C.; Allison, E.; Fonagy, P. The mentalizing approach to psychopathology: State of the art and future directions. Annu. Rev. Clin. Psychol. 2020, 26, 297–325. [Google Scholar] [CrossRef]
- Garon-Bissonnette, J.; Duguay, G.; Lemieux, R.; Dubois-Comtois, K.; Berthelot, N. Maternal childhood abuse and neglect predicts offspring development in early childhood: The roles of reflective functioning and child sex. Child. Abus. Negl. 2022, 128, 105030. [Google Scholar] [CrossRef]
- Berthelot, N.; Savard, C.; Lemieux, R.; Garon-Bissonnette, J.; Ensink, K.; Godbout, N. Development and validation of a self-report measure assessing failures in the mentalization of trauma and adverse relationships. Child. Abus. Negl. 2021, 128, 105017. [Google Scholar] [CrossRef]
- Hausberg, M.C.; Schulz, H.; Piegler, T.; Happach, C.G.; Klöpper, M.; Brütt, A.L.; Sammet, I.; Andreas, S. Is a self-rated instrument appropriate to assess mentalization in patients with mental disorders? Development and first validation of the Mentalization Questionnaire (MZQ). Psychother. Res. 2012, 22, 699–709. [Google Scholar] [CrossRef]
- Raimondi, G.; Samela, T.; Lester, D.; Imperatori, C.; Carlucci, L.; Contardi, A.; Balsamo, M.; Innamorati, M. Psychometric Properties of the Italian Mentalization Questionnaire: Assessing Structural Invariance and Construct Validity. J. Pers. Assess 2021, 104, 628–636. [Google Scholar] [CrossRef]
- Bernstein, D.P.; Stein, J.A.; Newcomb, M.D.; Walker, E.; Pogge, D.; Ahluvalia, T.; Stokes, J.; Handelsman, L.; Medrano, M.; Desmond, D.; et al. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child. Abus. Negl. 2003, 27, 169–190. [Google Scholar] [CrossRef]
- Innamorati, M.; Erbuto, D.; Venturini, P.; Fagioli, F.; Ricci, F.; Lester, D.; Amore, M.; Girardi, P.; Pompili, M. Factorial validity of the Childhood Trauma Questionnaire in Italian psychiatric patients. Psychiatry Res. 2016, 245, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Klaghofer, R.; Brähler, E. Konstruktion und teststatistische prüfung einer kurzform der scl-90–r [construction and test statistical evaluation of a short version of the scl-90–r]. Z. Klin. Psychol. Psychiatr. Psychother. 2001, 49, 115–124. [Google Scholar]
- Imperatori, C.; Bianciardi, E.; Niolu, C.; Fabbricatore, M.; Gentileschi, P.; Di Lorenzo, G.; Siracusano, A.; Innamorati, M. The symptom-checklist-K-9 (SCL-K-9) discriminates between overweight/obese patients with and without significant binge eating pathology: Psychometric properties of an Italian version. Nutrients 2020, 12, 674. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R.; Cleary, P.A. Confirmation of the dimensional structure of the SCL-90-R: A study in construct validation. J. Clin. Psychol. 1977, 33, 981–989. [Google Scholar] [CrossRef]
- Kyriazos, T.A. Applied Psychometrics: Sample Size and Sample Power Considerations in Factor Analysis (EFA, CFA) and SEM in General. Psychology 2018, 9, 2207–2230. [Google Scholar] [CrossRef]
- Wolf, E.J.; Harrington, K.M.; Clark, S.L.; Miller, M.W. Sample Size Requirements for Structural Equation Models: An Evaluation of Power, Bias and Solution Propriety. Educ. Psychol. Meas. 2013, 73, 913–934. [Google Scholar] [CrossRef] [PubMed]
- Wheathon, B.; Muthén, B.; Alwin, D.F.; Summers, G.F. Assessing reliability and stability in panel models. Sociol. Methodol. 1977, 8, 84–136. [Google Scholar] [CrossRef]
- Yu, C.Y. Evaluating Cutoff Criteria of Model Fit Indices for Latent Variable Models with Binary and Continuous Outcomes; University of California, Los Angeles: Los Angeles, CA, USA, 2002. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Jöreskog, K.G. Statistical analysis of sets of congeneric tests. Psychometrika 1971, 36, 109–133. [Google Scholar] [CrossRef]
- Meredith, W. Measurement invariance, factor analysis and factorial invariance. Psychometrika 1993, 58, 525–543. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; IEA: Paris, France, 2013. [Google Scholar] [CrossRef]
- Meng, X.L.; Rosenthal, R.; Rubin, D.B. Comparing correlated correlation coefficients. Psychol. Bull. 1992, 111, 172. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthen & Muthen: Los Angeles, CA, USA, 2017; 893p. [Google Scholar]
- Van der Ark, L.A. New Developments in Mokken Scale Analysis in R. J. Stat. Softw. 2012, 48, 1–27. [Google Scholar]
- IBM SPSS Statistics for Windows 25.0. IBM Corp. (n.d.). IBM SPSS Statistics for Windows (25.0). [Internet]. 2007. p. 335. Available online: https://www.ibm.com/support/pages/downloading-ibm-spss-statistics-25 (accessed on 1 June 2022).
- Doba, K.; Saloppé, X.; Choukri, F.; Nandrino, J.L. Childhood trauma and posttraumatic stress symptoms in adolescents and young adults: The mediating role of mentalizing and emotion regulation strategies. Child. Abus. Negl. 2022, 132, 105815. [Google Scholar] [CrossRef] [PubMed]
- Katzman, W.; Papouchis, N. Effects of childhood trauma on mentalization capacities and dissociative experiences. J. Trauma Dissociation 2023, 24, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Becker, R. Gender and survey participation: An event history analysis of the gender effects of survey participation in a probability-based multi-wave panel study with a sequential mixed-mode design. Methods Data Anal. 2022, 16, 30. [Google Scholar]
- Li, A.; Wang, S.; Paetzold, R.L.; Rholes, W.S.; Liu, X. Childhood trauma and its link to adult dissociation: The role of mentalizing and disorganized attachment in a Chinese adult sample. J. Trauma Dissociation 2023, 24, 559–574. [Google Scholar] [CrossRef]
- Kim, H.S.; Pyo, H.J.; Fava, M.; Mischoulon, D.; Park, M.J.; Jeon, H.J. Bullying, Psychological, and Physical Trauma During Early Life Increase Risk of Major Depressive Disorder in Adulthood: A Nationwide Community Sample of Korean Adults. Front. Psychiatry 2022, 13, 792734. [Google Scholar] [CrossRef]
- McLaughlin, K.A.; Green, J.G.; Gruber, M.J.; Sampson, N.A.; Zaslavsky, A.M.; Kessier, R.C. Childhood adversities and first onset of psychiatric disorders in a national sample of US adolescents. Arch. Gen. Psychiatry 2012, 69, 1151–1160. [Google Scholar] [CrossRef]
- Tessier, V.P.; Normadin, L.; Ensink, K.; Fonagy, P. Fact or fiction? A longitudinal study of play and the development of reflective functioning. Bull. Menn. Clin. 2016, 80, 60–79. [Google Scholar] [CrossRef]
- Van de Mortel, T.F. Faking it: Social desirability response bias in self-report research. Aust. J. Adv. Nurs. 2008, 25, 40–48. [Google Scholar]

{kind=link}
| Variables | N|M | %|(SD) |
|---|---|---|
| Age M(SD) | 27.24 | (8.00) |
| Sex N/% | ||
| Men | 72 | 10.2% |
| Women | 637 | 89.8% |
| Job status N/% | ||
| Employed | 304 | 42.9% |
| Unemployed or retired | 98 | 13.8% |
| Student | 307 | 43.3% |
| Marital status N/% | ||
| Single | 489 | 69% |
| Married/stable relationship | 202 | 28.5% |
| Divorced/widowed | 18 | 2.5% |
| Use of tobacco N/% | 314 | 44.3% |
| Alcohol N/% | 456 | 64.3% |
| Use of illegal drugs N/% | 67 | 9.4% |
| Model | χ2 (df) | RMSEA (90% CI) | CFI | TLI | SRMR | Model Comparison | χ2 (Δdf) | p | Results |
|---|---|---|---|---|---|---|---|---|---|
| Configural | 463.06 (126) | 0.088 (0.079–0.096) | 0.94 | 0.92 | 0.05 | - | - | - | Accepted |
| Metric | 453.63 (138) | 0.081 (0.073–0.089) | 0.95 | 0.94 | 0.05 | Configural | 6.92 (12) | 0.86 | Accepted |
| Scalar | 420.93 (176) | 0.063 (0.056–0.071) | 0.96 | 0.96 | 0.05 | Metric | 35.08 (38) | 0.60 | Accepted |
| FMTQ-s | MZQ | GSI-K-9 | CTQ_PA | CTQ_SA | CTQ_EA | CTQ_PN | |
|---|---|---|---|---|---|---|---|
| MZQ | −0.68 ** | ||||||
| GSI-K-9 | 0.61 ** | −0.65 ** | |||||
| CTQ_PA | 0.26 ** | −0.22 ** | 0.23 ** | ||||
| CTQ_SA | 0.10 ** | −0.11 ** | 0.16 ** | 0.22 ** | |||
| CTQ_EA | 0.42 ** | −0.38 ** | 0.44 ** | 0.61 ** | 0.23 ** | ||
| CTQ_PN | 0.26 ** | −0.20 ** | 0.26 ** | 0.57 ** | 0.26 ** | 0.57 ** | |
| CTQ_EN | 0.37 ** | −0.35 ** | 0.37 ** | 0.51 ** | 0.18 ** | 0.74 ** | 0.65 ** |
| r_diff | 95% CI | p | |
|---|---|---|---|
| CTQ_PA | 0.48 | 0.34–0.55 | <0.001 |
| CTQ_SA | −0.01 | −0.14–0.12 | 0.88 |
| CTQ_EA | 0.8 | 0.61–0.75 | <0.001 |
| CTQ_PN | 0.46 | 0.32–0.54 | <0.001 |
| CTQ_EN | 0.72 | 0.54–0.71 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raimondi, G.; Imperatori, C.; Gostoli, S.; Gremigni, P.; Innamorati, M. Italian Validation of the Short Version of the Failure to Mentalize Trauma Questionnaire in Adults at Risk Due to Childhood Trauma. Behav. Sci. 2023, 13, 843. https://doi.org/10.3390/bs13100843
Raimondi G, Imperatori C, Gostoli S, Gremigni P, Innamorati M. Italian Validation of the Short Version of the Failure to Mentalize Trauma Questionnaire in Adults at Risk Due to Childhood Trauma. Behavioral Sciences. 2023; 13(10):843. https://doi.org/10.3390/bs13100843
Chicago/Turabian StyleRaimondi, Giulia, Claudio Imperatori, Sara Gostoli, Paola Gremigni, and Marco Innamorati. 2023. "Italian Validation of the Short Version of the Failure to Mentalize Trauma Questionnaire in Adults at Risk Due to Childhood Trauma" Behavioral Sciences 13, no. 10: 843. https://doi.org/10.3390/bs13100843
APA StyleRaimondi, G., Imperatori, C., Gostoli, S., Gremigni, P., & Innamorati, M. (2023). Italian Validation of the Short Version of the Failure to Mentalize Trauma Questionnaire in Adults at Risk Due to Childhood Trauma. Behavioral Sciences, 13(10), 843. https://doi.org/10.3390/bs13100843