
Gender Differences in Attachment Anxiety and Avoidance and Their Association with Psychotherapy Use—Examining Students from a German University




Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Procedure
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
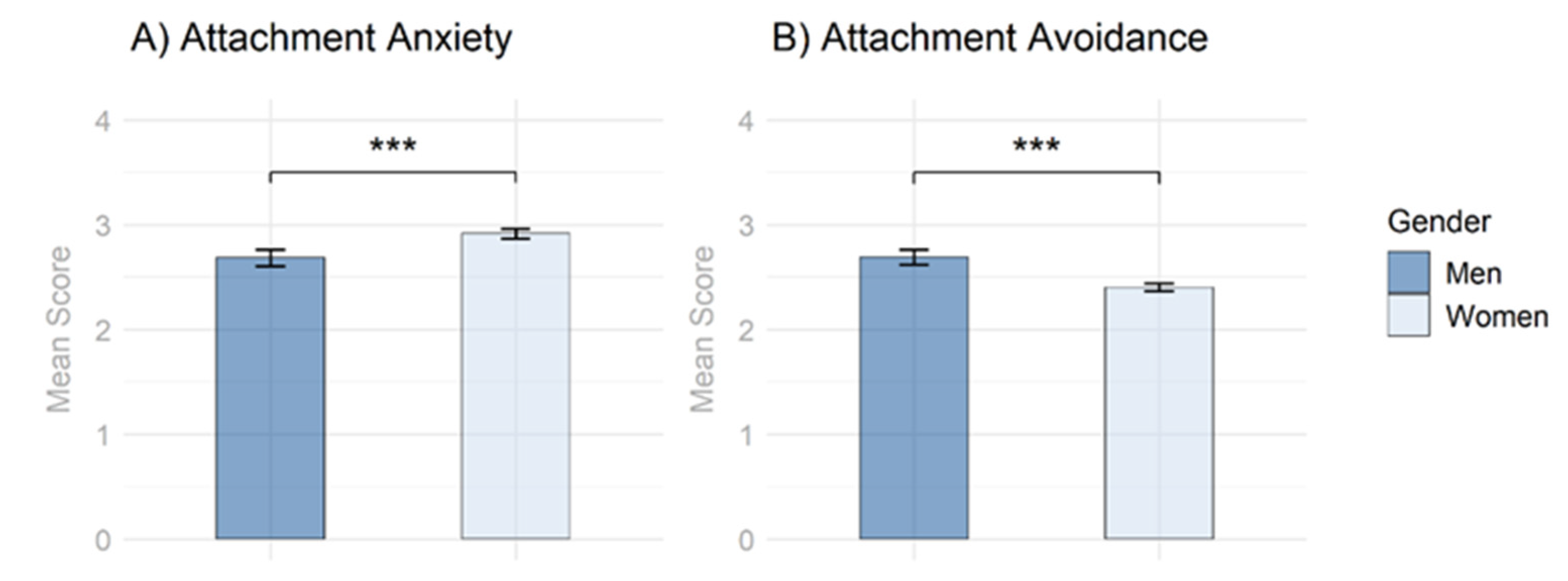
3.2. Group Comparisons
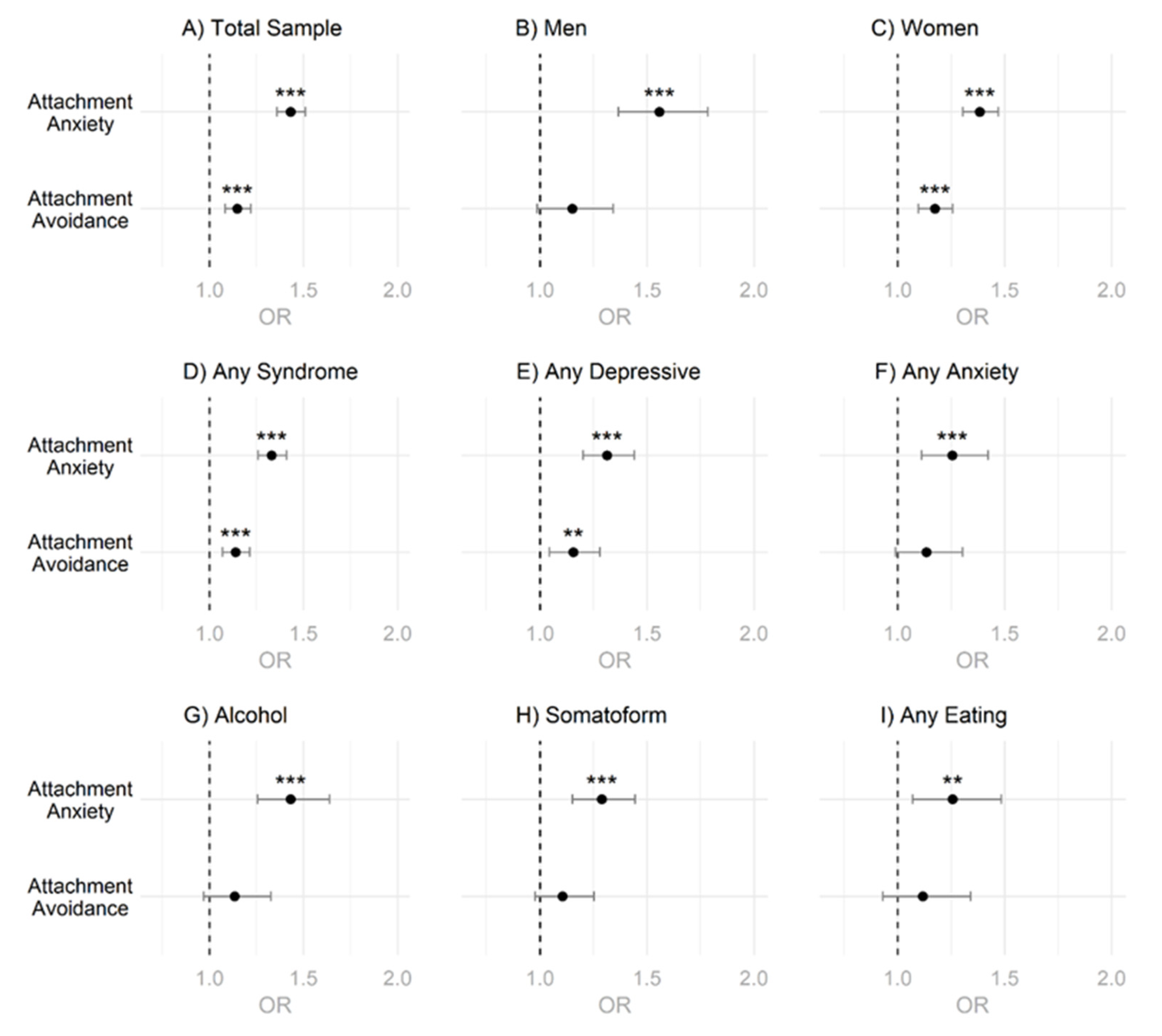
3.3. Logistic Regressions
4. Discussion
4.1. Summary of Results
4.2. Integration of Findings
4.3. Limitations
4.4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hasin, D.S.; Sarvet, A.L.; Meyers, J.L.; Saha, T.D.; Ruan, W.J.; Stohl, M.; Grant, B.F. Epidemiology of Adult DSM-5 Major Depressive Disorder and Its Specifiers in the United States. JAMA Psychiatry 2018, 75, 336–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salk, R.H.; Hyde, J.S.; Abramson, L.Y. Psychological Bulletin Gender Differences in Depression in Representative National Samples: Meta-Analyses of Diagnoses and Symptoms Gender Differences in Depression in Representative National Samples: Meta-Analyses of Diagnoses and Symptoms. Psychol. Bull. 2017, 143, 783–822. [Google Scholar] [CrossRef] [PubMed]
- Bandelow, B.; Michaelis, S. Epidemiology of Anxiety Disorders in the 21st Century. Dialogues Clin. Neurosci. 2015, 17, 327–335. [Google Scholar] [CrossRef]
- De Waal, M.W.M.; Arnold, I.A.; Eekhof, J.A.H.; Van Hemert, A.M. Somatoform Disorders in General Practice: Prevalence, Functional Impairment and Comorbidity with Anxiety and Depressive Disorders. Br. J. Psychiatry 2004, 184, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Galmiche, M.; Déchelotte, P.; Lambert, G.; Tavolacci, M.P. Prevalence of Eating Disorders over the 2000–2018 Period: A Systematic Literature Review. Am. J. Clin. Nutr. 2019, 109, 1402–1413. [Google Scholar] [CrossRef]
- Jacobi, F.; Höfler, M.; Strehle, J.; Mack, S.; Gerschler, A.; Scholl, L.; Busch, M.A.; Maske, U.; Hapke, U.; Gaebel, W.; et al. Mental Disorders in the General Population. Study on the Health of Adults in Germany and the Additional Module Mental Health (DEGS1-MH). Nervenarzt 2014, 85, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Grant, B.F.; Goldstein, R.B.; Saha, T.D.; Patricia Chou, S.; Jung, J.; Zhang, H.; Pickering, R.P.; June Ruan, W.; Smith, S.M.; Huang, B.; et al. Epidemiology of DSM-5 Alcohol Use Disorder Results from the National Epidemiologic Survey on Alcohol and Related Conditions III. JAMA Psychiatry 2015, 72, 757–766. [Google Scholar] [CrossRef] [Green Version]
- Grant, B.F.; Saha, T.D.; June Ruan, W.; Goldstein, R.B.; Patricia Chou, S.; Jung, J.; Zhang, H.; Smith, S.M.; Pickering, R.P.; Huang, B.; et al. Epidemiology of DSM-5 Drug Use Disorder Results from the National Epidemiologic Survey on Alcohol and Related Conditions-III. JAMA Psychiatry 2016, 73, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Hedegaard, H.; Curtin, S.C.; Warner, M. Increase in Suicide Mortality in The United States, 1999–2018. NCHS Data Brief 2020, 362, 1–8. [Google Scholar]
- Walther, A.; Grub, J.; Tsar, S.; Ehlert, U.; Heald, A.; Perrin, R.; Ogrodniczuk, J.; Seidler, Z.E.; Rice, S.; Kealy, D.; et al. Status Loss Due to COVID-19, Traditional Masculinity, and the Prediction of Suicidal Ideation and Recent Suicide Attempts. PsyArXiv 2021. [Google Scholar] [CrossRef]
- Bijl, R.V.; Ravelli, A.; van Zessen, G. Prevalence of Psychiatric Disorder in the General Population: Results of The Netherlands Mental Health Survey and Incidence Study (NEMESIS). Soc. Psychiatry Psychiatr. Epidemiol. 1998, 33, 587–595. [Google Scholar] [CrossRef]
- Walther, A.; Seidler, Z.E. Männliche Formen Der Depression Und Deren Behandlung. PiD-Psychother. Dialog 2020, 21, 40–45. [Google Scholar] [CrossRef]
- Walther, A.; Grub, J.; Ehlert, U.; Wehrli, S.; Rice, S.; Seidler, Z.E.; Debelak, R. Male Depression Risk, Psychological Distress, and Psychotherapy Uptake: Validation of the German Version of the Male Depression Risk Scale. J. Affect. Disord. Rep. 2021, 4, 100107. [Google Scholar] [CrossRef]
- Eggenberger, L.; Fordschmid, C.; Ludwig, C.; Weber, S.; Grub, J.; Komlenac, N.; Walther, A. Men’s Psychotherapy Use, Male Role Norms, and Male-Typical Depression Symptoms: Examining 716 Men and Women Experiencing Psychological Distress. Behav. Sci. 2021, 11, 83. [Google Scholar] [CrossRef]
- Brandstetter, S.; Dodoo-Schittko, F.; Speerforck, S.; Apfelbacher, C.; Grabe, H.J.; Jacobi, F.; Hapke, U.; Schomerus, G.; Baumeister, S.E. Trends in Non-Help-Seeking for Mental Disorders in Germany between 1997–1999 and 2009–2012: A Repeated Cross-Sectional Study. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Rommel, A.; Bretschneider, J.; Kroll, L.; Prütz, F.; Thom, J. Inanspruchnahme Psychiatrischer Und Psychotherapeutischer Leistungen. Individuelle Determinanten Und Regionale Unterschiede. PPmP-Psychother. Psychosom. Med. Psychol. 2018, 68, e31. [Google Scholar] [CrossRef] [Green Version]
- Dozier, M. Attachment Organization and Treatment Use for Adults with Serious Psychopathological Disorders. Dev. Psychopathol. 1990, 2, 47–60. [Google Scholar] [CrossRef]
- Seidler, Z.E.; Dawes, A.J.; Rice, S.M.; Oliffe, J.L.; Dhillon, H.M. The Role of Masculinity in Men’s Help-Seeking for Depression: A Systematic Review. Clin. Psychol. Rev. 2016, 49, 106–118. [Google Scholar] [CrossRef]
- Wong, Y.J.; Ho, M.H.R.; Wang, S.Y.; Miller, I.S.K. Meta-Analyses of the Relationship between Conformity to Masculine Norms and Mental Health-Related Outcomes. J. Couns. Psychol. 2017, 64, 80–93. [Google Scholar] [CrossRef]
- Levant, R.F.; Hall, R.J.; Weigold, I.K.; Mccurdy, E.R. Construct Validity Evidence for the Male Role Norms Inventory-Short Form: A Structural Equation Modeling Approach Using the Bifactor Model. J. Couns. Psychol. 2016, 63, 534–542. [Google Scholar] [CrossRef]
- Fitzpatrick, B. Men in Groups: Attachment and Masculinity; Pacifica Graduate Institute: Carpinteria, CA, USA, 2016; ISBN 1369633394. [Google Scholar]
- Calzo, J.P. Determinants of Variability in College Men’s Sociosexuality: A Focus on Avoidance, Bros, and Masculinity Ideologies; University of Michigan: Ann Arbor, MI, USA, 2010; ISBN 112443819X. [Google Scholar]
- Saldubehere, A. The Relationships between Traditional Masculinity Ideology, Alexithymia, and Attachment among Male Millennials in The United States. Ph.D. Thesis, Alliant International University, Alhambra, CA, USA, 2019. [Google Scholar]
- Smiler, A.P.; Heasley, R. Boys’ and Men’s Intimate Relationships: Friendships and Romantic Relationships. In APA Handbook of Men and Masculinities; American Psychological Association: Washington, DC, USA, 2016; pp. 569–589. ISBN 1433818558. [Google Scholar]
- Mikulincer, M.; Shaver, P.R. Attachment Theory and Emotions in Close Relationships: Exploring the Attachment-related Dynamics of Emotional Reactions to Relational Events. Pers. Relatsh. 2005, 12, 149–168. [Google Scholar] [CrossRef]
- Bartholomew, K.; Kwong, M.J.; Hart, S.D. Attachment. In Handbook of Personality Disorders: Theory, Research, and Treatment; The Guilford Press: New York, NY, USA, 2001; pp. 196–230. [Google Scholar]
- Gillath, O.; Bunge, S.A.; Shaver, P.R.; Wendelken, C.; Mikulincer, M. Attachment-Style Differences in the Ability to Suppress Negative Thoughts: Exploring the Neural Correlates. Neuroimage 2005, 28, 835–847. [Google Scholar] [CrossRef] [PubMed]
- Fraley, C.R.; Niedenthal, P.M.; Marks, M.; Brumbaugh, C.; Vicary, A. Adult Attachment and the Perception of Emotional Expressions: Probing the Hyperactivating Strategies Underlying Anxious Attachment. J. Pers. 2006, 74, 1163–1190. [Google Scholar] [CrossRef] [PubMed]
- Richards, D.A.; Schat, A.C.H. Attachment at (Not to) Work: Applying Attachment Theory to Explain Individual Behavior in Organizations. J. Appl. Psychol. 2011, 96, 169–182. [Google Scholar] [CrossRef] [PubMed]
- Mikulincer, M.; Shaver, P.R.; Pereg, D. Attachment Theory and Affect Regulation: The Dynamics, Development, and Cognitive Consequences of Attachment-Related Strategies. Motiv. Emot. 2003, 27, 77–102. [Google Scholar] [CrossRef]
- Slade, A.; Holmes, J. Attachment and Psychotherapy. Curr. Opin. Psychol. 2019, 25, 152–156. [Google Scholar] [CrossRef]
- Diener, M.J.; Monroe, J.M. The Relationship between Adult Attachment Style and Therapeutic Alliance in Individual Psychotherapy: A Meta-Analytic Review. Psychotherapy 2011, 48, 237–248. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R.; Berant, E. An Attachment Perspective on Therapeutic Processes and Outcomes. J. Pers. 2013, 81, 606–616. [Google Scholar] [CrossRef]
- Seidler, Z.E.; Wilson, M.J.; Kealy, D.; Oliffe, J.L.; Ogrodniczuk, J.S.; Rice, S.M. Men’s Dropout from Mental Health Services: Results from a Survey of Australian Men Across the Life Span. Am. J. Men’s Health 2021, 15, 15579883211014776. [Google Scholar] [CrossRef]
- Kirchmann, H.; Strauß, B. Methoden Zur Erfassung von Bindungsmerkmalen. Klin. Diagn. Eval. 2008, 1, 293–327. [Google Scholar]
- Crowell, J.A.; Fraley, R.C.; Roisman, G.I. Measurement of Individual Differences in Adult Attachment. In Handbook of Attachment: Theory, Research, and Clinical Applications; Cassidy, J., Shaver, P.R., Eds.; Guilford Press: New York, NY, USA, 2016; pp. 598–639. [Google Scholar]
- Bakermans-Kranenburg, M.; van IJzendoorn, M.H. The First 10,000 Adult Attachment Interviews: Distributions of Adult Attachment Representations in Clinical and Non-Clinical Groups. Attach. Hum. Dev. 2009, 11, 223–263. [Google Scholar] [CrossRef]
- Petrowski, K.; Brähler, E.; Suslow, T.; Zenger, M. Revised Short Screening Version of the Attachment Questionnaire for Couples from the German General Population. PLoS ONE 2020, 15, e0230864. [Google Scholar] [CrossRef]
- Del Giudice, M. Sex, Attachment, and the Development of Reproductive Strategies. Behav. Brain Sci. 2009, 32, 1–67. [Google Scholar] [CrossRef] [PubMed]
- Del Giudice, M.; Belsky, J. Sex Differences in Attachment Emerge in Middle Childhood: An Evolutionary Hypothesis. Child Dev. Perspect. 2010, 4, 97–105. [Google Scholar] [CrossRef]
- Del Giudice, M. Sex Differences in Romantic Attachment: A Meta-Analysis. Personal. Soc. Psychol. Bull. 2011, 37, 193–214. [Google Scholar] [CrossRef]
- Del Giudice, M. Sex Differences in Attachment Styles. Curr. Opin. Psychol. 2019, 25, 1–5. [Google Scholar] [CrossRef]
- Duschinsky, R.; Bakkum, L.; Mannes, J.M.M.; Skinner, G.C.M.; Turner, M.; Mann, A.; Coughlan, B.; Reijman, S.; Foster, S.; Beckwith, H. Six Attachment Discourses: Convergence, Divergence and Relay. Attach. Hum. Dev. 2021, 23, 355–374. [Google Scholar] [CrossRef]
- Weber, R.; Ehrenthal, J.C.; Pförtner, T.K.; Albus, C.; Stosch, C. Die Schönste Zeit Des Lebens? Z. Klin. Psychol. Psychother. 2020, 49, 43–51. [Google Scholar] [CrossRef]
- Leiner, D.J. SoSci Survey, Version 3.1.06. Available online: https://www.soscisurvey.de (accessed on 22 June 2021).
- Eggenberger, L.; Komlenac, N.; Ehlert, U.; Grub, J.; Walther, A. Association between Psychotherapy Use, Sexual Orientation, and Traditional Masculinity among Psychologically Distressed Men. Psychol. Men Masc. 2022. [Google Scholar] [CrossRef]
- Löwe, B.; Spitzer, R.L.; Zipfel, S.; Herzog, W. Manual: Komplettversion und Kurzform Autorisierte Deutsche Version Des “Prime MD Patient Health Questionnaire (PHQ)”. Nervenarzt 2002, 6, 2–11. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Patient Health Questionnaire Primary Care Study Group; Patient Health Questionnaire Primary Care Study Group. Validation and Utility of a Self-Report Version of PRIME-MD: The PHQ Primary Care Study. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [Green Version]
- Löwe, B.; Spitzer, R.L.; Gräfe, K.; Kroenke, K.; Quenter, A.; Zipfel, S.; Buchholz, C.; Witte, S.; Herzog, W. Comparative Validity of Three Screening Questionnaires for DSM-IV Depressive Disorders and Physicians’ Diagnoses. J. Affect. Disord. 2004, 78, 131–140. [Google Scholar] [CrossRef]
- Ehrenthal, J.C.; Dinger, U.; Lamla, A.; Funken, B.; Schauenburg, H. Evaluation Der Deutschsprachigen Version des Bindungsfragebogens “Experiences in Close Relationships—Revised” (ECR-RD) (Evaluation of the German Version of the Attachment Questionnaire “Experiences in Close Relationships—Revised”[ECR-RD]). PPmP-Psychother. Psychosom. Med. Psychol. 2008, 59, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Fraley, R.C.; Heffernan, M.E.; Vicary, A.M.; Brumbaugh, C.C. The Experiences in Close Relationships—Relationship Structures Questionnaire: A Method for Assessing Attachment Orientations across Relationships. Psychol. Assess. 2011, 23, 615–625. [Google Scholar] [CrossRef] [Green Version]
- R Core Team, R. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Revelle, W. Psych: Procedures for Personality and Psychological Research; Northwestern University: Evanston, IL, USA, 2020. [Google Scholar]
- Fox, J.; Sanford, W. An {R} Companion to Applied Regression, 3rd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2019. [Google Scholar]
- Mangiafico, S. Rcompanion: Functions to Support Extension Education Program Evaluation; The Comprehensive R Archive Network: Vienna, Austria, 2021. [Google Scholar]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Brown, M.B.; Forsythe, A.B. Robust Tests for the Equality of Variances. J. Am. Stat. Assoc. 1974, 69, 364–367. [Google Scholar] [CrossRef]
- Cook, R.D. Detection of Influential Observation in Linear Regression. Technometrics 1977, 19, 15–18. [Google Scholar] [CrossRef]
- Fox, J.; Monette, G. Generalized Collinearity Diagnostics. J. Am. Stat. Assoc. 1992, 87, 178–183. [Google Scholar] [CrossRef]
- Rosenfield, S.; Smith, D. Gender and Mental Health: Do Men and Women Have Different Amounts or Types of Problems. In A Handbook for The Study of Mental Health: Social Contexts, Theories, and Systems; Cambridge University Press: Cambridge, UK, 2010; Volume 13, pp. 256–267. [Google Scholar]
- Rosenfield, S. Gender and Mental Health: Do Women Have More Psychopathology, Men More, or Both the Same (and Why)? In A Handbook for The Study of Mental Health: Social Contexts, Theories, and Systems; Cambridge University Press: Cambridge, UK, 1999. [Google Scholar]
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 328 Diseases and Injuries for 195 Countries, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Walther, A.; Rice, T.; Kufert, Y.; Ehlert, U. Neuroendocrinology of a Male-Specific Pattern for Depression Linked to Alcohol Use Disorder and Suicidal Behavior. Front. Psychiatry 2017, 7, 206. [Google Scholar] [CrossRef] [Green Version]
- Fiacco, S.; Walther, A.; Ehlert, U. Steroid Secretion in Healthy Aging. Psychoneuroendocrinology 2019, 105, 64–78. [Google Scholar] [CrossRef]
- Schneider, L.; Walther, A. Geschlechtsunterschiede in Glucocorticoidkonzentrationen und Entzündungsparametern im Zusammenhang Mit Depression. Nervenheilkunde 2020, 39, 222–237. [Google Scholar] [CrossRef]
- Walther, A.; Breidenstein, J.; Miller, R. Association of Testosterone Treatment with Alleviation of Depressive Symptoms in Men: A Systematic Review and Meta-Analysis. JAMA Psychiatry 2019, 76, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Deligiannidis, K.M.; Freeman, M.P. Complementary and Alternative Medicine for the Treatment of Depressive Disorders in Women. Psychiatr. Clin. 2010, 33, 441–463. [Google Scholar] [CrossRef] [PubMed]
- Mirowsky, J.; Ross, C.E. Sex Differences in Distress: Real or Artifact? Am. Sociol. Rev. 1995, 60, 449–468. [Google Scholar] [CrossRef]
- Martin, L.A.; Neighbors, H.W.; Griffith, D.M. The Experience of Symptoms of Depression in Men vs. Women: Analysis of the National Comorbidity Survey Replication. JAMA Psychiatry 2013, 70, 1100–1106. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation (WHO). Depression and Other Common Mental Disorders Global Health Estimates; WHO Reference Number: WHO/MSD/MER/2017.2; The WHO Document Production Services: Geneva, Switzerland, 2017. [Google Scholar]
- Li, N.; He, J.; Li, T. Gender Difference of Insecure Attachment: Universal or Culture-Specific? Behav. Brain Sci. 2009, 32, 36–37. [Google Scholar] [CrossRef]
- Kirchmann, H.; Steyer, R.; Mayer, A.; Joraschky, P.; Schreiber-Willnow, K.; Strauss, B. Effects of Adult Inpatient Group Psychotherapy on Attachment Characteristics: An Observational Study Comparing Routine Care to an Untreated Comparison Group. Psychother. Res. 2012, 22, 95–114. [Google Scholar] [CrossRef]
- Bosquet, M.; Egeland, B. The Development and Maintenance of Anxiety Symptoms from Infancy through Adolescence in a Longitudinal Sample. Dev. Psychopathol. 2006, 18, 517–550. [Google Scholar] [CrossRef] [Green Version]
- Belsky, J.; Fearon, R.M.P. Early Attachment Security, Subsequent Maternal Sensitivity, and Later Child Development: Does Continuity in Development Depend upon Continuity of Caregiving? Attach. Hum. Dev. 2002, 4, 361–387. [Google Scholar] [CrossRef]
- Ann Easterbrooks, M.; Abeles, R. Windows to the Self in 8-Year-Olds: Bridges to Attachment Representation and Behavioral Adjustment. Attach. Hum. Dev. 2000, 2, 85–106. [Google Scholar] [CrossRef]
- Schieche, M.; Spangler, G. Individual Differences in Biobehavioral Organization during Problem-solving in Toddlers: The Influence of Maternal Behavior, Infant–Mother Attachment, and Behavioral Inhibition on the Attachment-exploration Balance. Dev. Psychobiol. J. Int. Soc. Dev. Psychobiol. 2005, 46, 293–306. [Google Scholar] [CrossRef]
- Meredith, P.J.; Strong, J.; Feeney, J.A. Adult Attachment Variables Predict Depression before and after Treatment for Chronic Pain. Eur. J. Pain 2007, 11, 164–170. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 4894) | Men (N = 1207) | Women (N = 3687) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N (%) | M (SD) | N (%) | M (SD) | N (%) | M (SD) | Test Statistic (df) | p | p (corr.) | |
| Age | 24.3 (4.9) | 25.1 (5.2) | 24.1 (4.8) | 6.43 (4890) | <0.001 *** | <0.001 *** | |||
| Nationality | |||||||||
| German | 4637 (94.7) | 1150 (95.3) | 3487 (94.6) | 1.55 (4890) | 0.122 | 0.224 | |||
| Non-German | 339 (6.9) | 82 (6.8) | 257 (7.0) | 1.22 (4890) | 0.222 | 0.224 | |||
| Study situation | |||||||||
| Previous degree | 950 (19.4) | 226 (18.7) | 724 (19.6) | −2.69 (4889) | 0.007 ** | 0.021 * | |||
| Previous dropout | 1182 (24.2) | 324 (26.8) | 858 (23.3) | 1.44 (4889) | 0.149 | 0.149 | |||
| Thinking about dropout | 2233 (45.6) | 583 (48.3) | 1650 (44.8) | 1.87 (4889) | 0.062 | 0.124 | |||
| Financed by | |||||||||
| Relatives | 3450 (70.5) | 845 (70.0) | 2605 (70.7) | 1.25 (4889) | 0.211 | 0.422 | |||
| Job | 3319 (67.8) | 814 (67.4) | 2505 (67.9) | −1.49 (4889) | 0.137 | 0.411 | |||
| BAföG | 1185 (24.2) | 244 (20.2) | 941 (25.5) | −3.37 (4889) | <0.001 *** | 0.004 ** | |||
| Scholarship | 217 (4.4) | 68 (5.6) | 149 (4.0) | 2.58 (4889) | 0.001 ** | 0.039 * | |||
| Other means | 456 (9.3) | 123 (10.2) | 333 (9.0) | 0.15 (4889) | 0.882 | 0.882 | |||
| Counseling/Therapy | |||||||||
| Contact with counseling service | 3485 (71.2) | 895 (74.2) | 2590 (70.2) | 3.41 (4889) | <0.001 *** | 0.001 ** | |||
| Previous psychotherapy | 1273 (26.0) | 272 (22.5) | 1001 (27.1) | −4.50 (4889) | <0.001 *** | <0.001 *** | |||
| Current psychotherapy | 425 (8.7) | 83 (6.9) | 342 (9.3) | 3.06 (4889) | 0.002 ** | 0.002 ** | |||
| Intention psychotherapy | 1388 (28.4) | 278 (23.0) | 1110 (30.1) | 4.79 (4889) | <0.001 *** | <0.001 *** | |||
| Medical Conditions | |||||||||
| Previous medical care | 1049 (21.4) | 218 (18.1) | 831 (22.5) | 4.09 (4889) | <0.001 *** | <0.001 *** | |||
| Current medical care | 337 (6.9) | 64 (5.3) | 273 (7.4) | 2.91 (4889) | 0.004 ** | 0.016 * | |||
| Physical impairment | 459 (9.4) | 103 (8.5) | 356 (9.7) | 1.67 (4881) | 0.095 | 0.117 | |||
| Physical / sexual abuse | 173 (3.5) | 53 (4.4) | 120 (3.3) | 1.93 (4770) | 0.053 | 0.117 | |||
| Medication | 295 (6.0) | 60 (5.0) | 235 (6.4) | −2.07 (4770) | 0.039 * | 0.117 | |||
| Psychological Syndromes | |||||||||
| Any syndrome | 2856 (58.4) | 678 (56.2) | 2178 (59.1) | −1.72 (4889) | 0.085 | 0.399 | |||
| Any depressive | 1710 (34.9) | 392 (32.5) | 1318 (35.7) | −2.05 (4887) | 0.040 * | 0.322 | |||
| Minor depression | 703 (14.4) | 156 (12.9) | 547 (14.8) | −1.51 (4887) | 0.130 | 0.399 | |||
| Major depression | 1007 (20.6) | 236 (19.6) | 771 (20.9) | −1.10 (4887) | 0.271 | 0.542 | |||
| Any anxiety | 614 (12.5) | 109 (9.0) | 505 (13.7) | −4.51 (4889) | <0.001 *** | <0.001 *** | |||
| Anxiety–panic | 114 (2.3) | 21 (1.7) | 93 (2.5) | −1.75 (4889) | 0.080 | 0.3985 | |||
| Anxiety–generalized | 549 (11.2) | 101 (8.4) | 448 (12.2) | −3.82 (4889) | <0.001 *** | 0.001 ** | |||
| Alcohol use syndrome | 934 (19.1) | 340 (28.2) | 594 (16.1) | −9.52 (4889) | <0.001 *** | <0.001 *** | |||
| Somatoform syndrome | 1157 (23.6) | 128 (10.6) | 1029 (27.9) | −11.71 (4889) | <0.001 *** | <0.001 *** | |||
| Any eating disorder | 576 (11.8) | 123 (10.2) | 453 (12.3) | −2.01 (4889) | 0.044 * | 0.322 | |||
| Eating–bulimia | 136 (2.8) | 29 (2.4) | 107 (2.9) | −0.85 (4541) | 0.398 | 0.542 | |||
| Eating–binge | 441 (9.0) | 94 (7.8) | 347 (9.4) | −1.84 (4889) | 0.065 | 0.391 | |||
| ECR-RD12 a | |||||||||
| Attachment anxiety | 2.86 (1.41) | 2.69 (1.39) | 2.92 (1.41) | −4.80 (4700) | <0.001 *** | <0.001 *** | |||
| Attachment avoidance | 2.47 (1.23) | 2.69 (1.25) | 2.40 (1.22) | 6.88 (4700) | <0.001 *** | <0.001 *** | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weber, R.; Eggenberger, L.; Stosch, C.; Walther, A. Gender Differences in Attachment Anxiety and Avoidance and Their Association with Psychotherapy Use—Examining Students from a German University. Behav. Sci. 2022, 12, 204. https://doi.org/10.3390/bs12070204
Weber R, Eggenberger L, Stosch C, Walther A. Gender Differences in Attachment Anxiety and Avoidance and Their Association with Psychotherapy Use—Examining Students from a German University. Behavioral Sciences. 2022; 12(7):204. https://doi.org/10.3390/bs12070204
Chicago/Turabian StyleWeber, Rainer, Lukas Eggenberger, Christoph Stosch, and Andreas Walther. 2022. "Gender Differences in Attachment Anxiety and Avoidance and Their Association with Psychotherapy Use—Examining Students from a German University" Behavioral Sciences 12, no. 7: 204. https://doi.org/10.3390/bs12070204
APA StyleWeber, R., Eggenberger, L., Stosch, C., & Walther, A. (2022). Gender Differences in Attachment Anxiety and Avoidance and Their Association with Psychotherapy Use—Examining Students from a German University. Behavioral Sciences, 12(7), 204. https://doi.org/10.3390/bs12070204