Exercise-Induced Oxygen Desaturation during the 6-Minute Walk Test



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Measurements
Demographic and Anthrompometric Variables
2.3. Pulmonary Function Test Protocol
2.4. The 6-Minute Walk Test Protocol
2.5. Statistical Analysis
3. Results
3.1. Demographic, and BMI Characteristics of Patients Based on Category of SpO2 Change during the 6MWT
3.2. Pulmonary Function of Patients Based on Category of SpO2 Change during the 6MWT
3.3. The 6-Minute Walk Test Results of Patients Based on Category of SpO2 Change during the 6MWT
3.4. Demographic, and BMI Characteristics of ≥4% Oxygen Desaturators vs. Nondesaturators during the 6MWT
3.5. The 6-Minute Walk Test Results of ≥4% Oxygen Desaturators vs. Nondesaturators during the 6MWT
3.6. Regression Models to Predict Changes in SpO2 and a ≥4% Oxygen Desaturation during the 6MWT
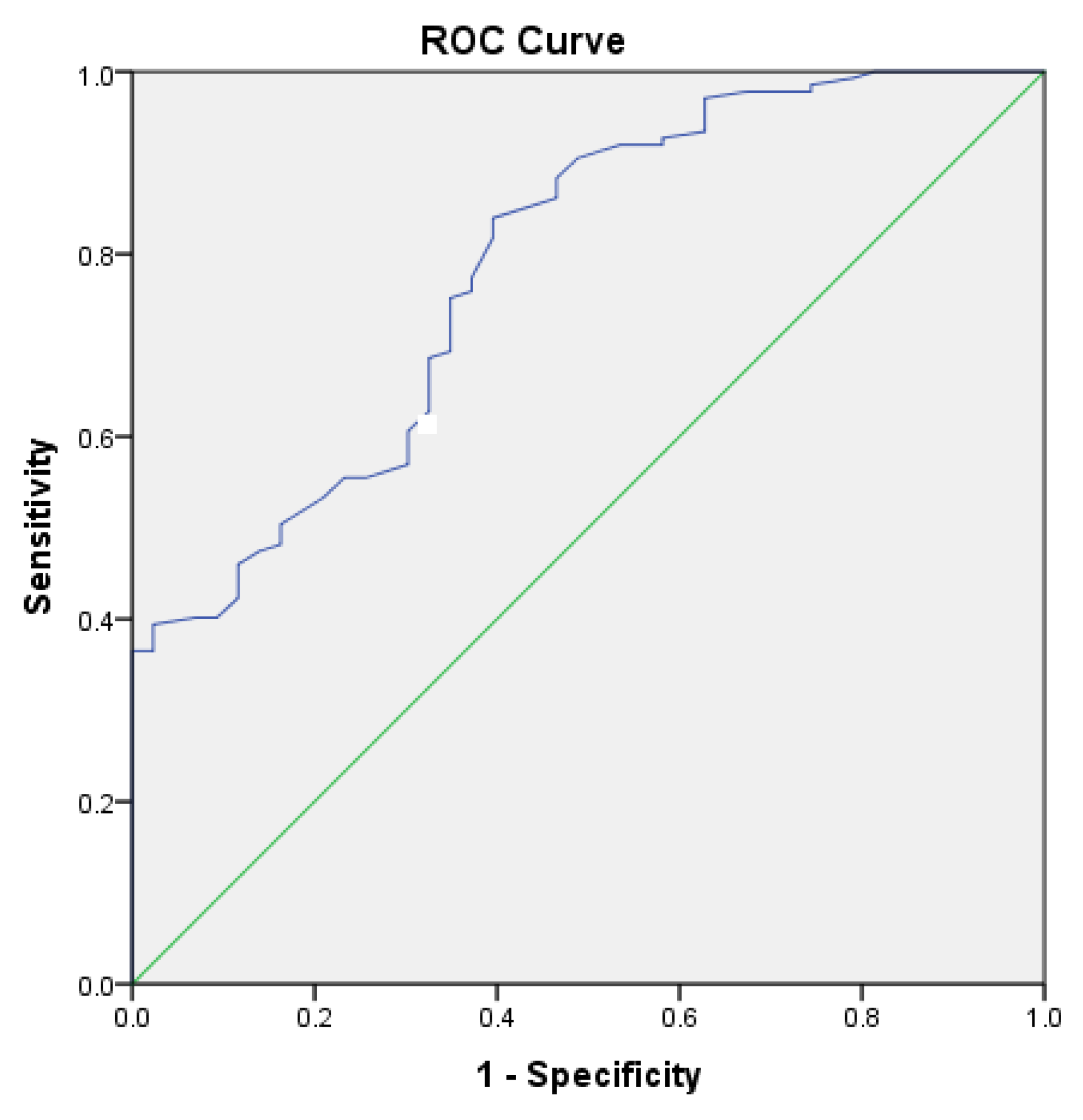
3.7. Receiver Operating Characteristics of DLCO% for Detection of ≥4% Oxygen Desaturation during the 6MWT
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Weisman, I.M.; Zeballos, R.J. An integrated approach to the interpretation of cardiopulmonary exercise testing. Clin. Chest Med. 1994, 15, 421–445. [Google Scholar] [PubMed]
- Solway, S.; Brooks, D.; Lacasse, Y.; Thomas, S. A qualitative systematic overview of the measurement properties of functional walk tests used in the cardiorespiratory domain. CHEST J. 2001, 119, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Thompson, P.J.; Berman, L.B.; Sullivan, M.J.; Townsend, M.; Jones, N.L.; Pugsley, S.O. How should we measure function in patients with chronic heart and lung disease? J. Chronic Dis. 1985, 38, 517–524. [Google Scholar] [CrossRef]
- Crapo, R.O. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar]
- Andrianopoulos, V.; Wouters, E.F.; Pinto-Plata, V.M.; Vanfleteren, L.E.; Bakke, P.S.; Franssen, F.M.; Agusti, A.; MacNee, W.; Rennard, S.I.; Singer, R.T.; et al. Prognostic value of variables derived from the six-minute walk test in patients with COPD: Results from the ECLIPSE study. Respir. Med. 2015, 109, 1138–1146. [Google Scholar] [CrossRef] [Green Version]
- Dajczman, E.; Wardini, R.; Kasymjanova, G.; Préfontaine, D.; Baltzan, M.A.; Wolkove, N. Six-minute walk distance is a predictor of survival in patients with chronic obstructive pulmonary disease undergoing pulmonary rehabilitation. Can. Respir. J. 2015, 22, 225–229. [Google Scholar] [CrossRef]
- Casanova, C.; Cote, C.; Marin, J.M.; Pinto-Plata, V.; de Torres, J.P.; Aguirre-Jaíme, A.; Vassaux, C.; Celli, B.R. Distance and oxygen desaturation during the 6-min walk test as predictors of long-term mortality in patients with COPD. CHEST J. 2008, 134, 746–752. [Google Scholar] [CrossRef]
- Singh, S.J.; Puhan, M.A.; Andrianopoulos, V.; Hernandes, N.A.; Mitchell, K.E.; Hill, C.J.; Lee, A.L.; Camillo, C.A.; Troosters, T.; Spruit, M.A.; et al. An official systematic review of the European Respiratory Society/American Thoracic Society: Measurement properties of field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1447–1478. [Google Scholar] [CrossRef]
- Chen, H.; Liang, B.M.; Tang, Y.J.; Wang, K.; Yi, Q.; Ou, X.M.; Feng, Y.L. Relationship between 6-minute walk test and pulmonary function test in stable chronic obstructive pulmonary disease with different severities. Chin. Med. J. 2012, 125, 3053–3058. [Google Scholar]
- Garin, M.C.; Highland, K.B.; Silver, R.M.; Strange, C. Limitations to the 6-minute walk test in interstitial lung disease and pulmonary hypertension in scleroderma. J. Rheumatol. 2009, 36, 330–336. [Google Scholar] [CrossRef]
- Deuschle, K.; Weinert, K.; Becker, M.O.; Backhaus, M.; Huscher, D.; Riemekasten, G. Six-minute walk distance as a marker for disability and complaints in patients with systemic sclerosis. Clin. Exp. Rheumatol. Incl Suppl. 2011, 29, S53. [Google Scholar]
- Nishiyama, O.; Yamazaki, R.; Sano, H.; Iwanaga, T.; Higashimoto, Y.; Kume, H.; Tohda, Y. Pulmonary Hemodynamics and Six-Minute Walk Test Outcomes in Patients with Interstitial Lung Disease. Can. Respir. J. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulain, M.; Durand, F.; Palomba, B.; Desplan, J.; Varray, A. 6-minute walk testing is more sensitive than maximal incremental cycle testing for detecting oxygen desaturation in patients with COPD. CHEST J. 2003, 123, 1401–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyatt, G.H.; Townsend, M.; Keller, J.; Slnger, J.; Nogradi, S. Measuring functional status in chronic lung disease: Conclusions from a randomized control trial. Respir. Med. 1991, 85, 17–21. [Google Scholar] [CrossRef]
- Barthelemy, J.C.; Geyssant, A.; Riffat, J.; Antoniadis, A.; Berruyer, J.; LaCour, J.R. Accuracy of pulse oximetry during moderate exercise: A comparative study. Scand. J. Clin. Lab. Investig. 1990, 50, 533–539. [Google Scholar] [CrossRef]
- Ziegler, B.; Rovedder, P.M.; Oliveira, C.L.; e Silva, F.D.; Dalcin, P.D. Repeatability of the 6-minute walk test in adolescents and adults with cystic fibrosis. Respir. Care 2010, 55, 1020–1025. [Google Scholar]
- Wilsher, M.; Good, N.; Hopkins, R.; Young, P.; Milne, D.; Gibson, A.; Suppiah, R.; Ly, J.; Doughty, R.; Dalbeth, N. The six-minute walk test using forehead oximetry is reliable in the assessment of scleroderma lung disease. Respirology 2012, 17, 647–652. [Google Scholar] [CrossRef]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Paciocco, G.; Martinez, F.J.; Bossone, E.; Pielsticker, E.; Gillespie, B.; Rubenfire, M. Oxygen desaturation on the six-minute walk test and mortality in untreated primary pulmonary hypertension. Eur. Respir. J. 2001, 17, 647–652. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, S.; Čečins, N. Six-minute walk test: Observed adverse events and oxygen desaturation in a large cohort of patients with chronic lung disease. Intern. Med. J. 2011, 41, 416–422. [Google Scholar] [CrossRef]
- Chetta, A.; Pisi, G.; Zanini, A.; Foresi, A.; Grzincich, G.L.; Aiello, M.; Battistini, A.; Olivieri, D. Six-minute walking test in cystic fibrosis adults with mild to moderate lung disease: Comparison to healthy subjects. Respir. Med. 2001, 95, 986–991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitzan, M.; Romem, A.; Koppel, R. Pulse oximetry: Fundamentals and technology update. Med. Devices 2014, 7, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Chetta, A.; Aiello, M.; Foresi, A.; Marangio, E.; D’Ippolito, R.; Castagnaro, A.; Olivieri, D. Relationship between outcome measures of six-minute walk test and baseline lung function in patients with interstitial lung disease. Sarcoidosis Vasc. Diffus. lung Dis. Off. J. WASOG 2001, 18, 170–175. [Google Scholar]
- Hadeli, K.O.; Siegel, E.M.; Sherrill, D.L.; Beck, K.C.; Enright, P.L. Predictors of oxygen desaturation during submaximal exercise in 8000 patients. CHEST J. 2001, 120, 88–92. [Google Scholar] [CrossRef] [Green Version]
- Kaminsky, D.A.; Whitman, T.; Callas, P.W. DLCO versus DLCO/VA as predictors of pulmonary gas exchange. Respir. Med. 2007, 101, 989–994. [Google Scholar] [CrossRef] [Green Version]
- Ahmadi, Z.; Sundh, J.; Bornefalk-Hermansson, A.; Ekström, M. Long-Term Oxygen Therapy 24 vs 15 h/day and Mortality in Chronic Obstructive Pulmonary Disease. PLoS ONE 2016, 11, e0163293. [Google Scholar] [CrossRef] [Green Version]
- Fiore, C.B.; Lee, A.L.; McDonald, C.F.; Hill, C.J.; Holland, A.E. Should oxyhaemoglobin saturation be monitored continuously during the 6-minute walk test? Chronic Respir. Dis. 2011, 8, 181–184. [Google Scholar] [CrossRef]


{kind=link}
| Change in SpO2 (Δ = SpO2 at End of Study–SpO2 at Start of Study) | ||||
|---|---|---|---|---|
| Variable | Increased (Δ ≥ +1%) N = 60 (19%) | Unchanged (−2 ≤ Δ ≤ 0%) N = 146 (46%) | Decreased (Δ ≤ −3%) N = 113 (35%) | p-Value |
| Age, years | 48.30 ± 13.96 | 54.41 ± 13.35 | 57.68 ± 13.91 | <0.001 |
| Sex, no. (%) | 0.236 | |||
| Male | 22 (18) | 51 (42) | 47 (39) | |
| Female | 37 (19) | 95 (48) | 67 (33) | |
| Race, no. (%) | 0.364 | |||
| White | 35 (19) | 84 (45) | 66 (36) | |
| Black | 25 (19) | 59 (46) | 47 (36) | |
| Hispanic | 0 (0) | 1 (100) | 0 (0) | |
| Asian | 1 (100) | 0 (0) | 0 (0) | |
| Other | 0 (0) | 0 (0) | 1 (100) | |
| BMI (kg/m2) | 27.82 ± 7.68 | 30.06 ± 8.28 | 30.06 ± 8.06 | 0.157 |
| Obstruction (FEV1/FVC < 70%), no. (%) | 12 (20) | 35 (24) | 46 (41) | <0.001 |
| Restriction (TLC < 80%), no. (%) | 20 (33) | 37 (25) | 39 (35) | 0.114 |
| Combined obstruction and restriction, no. (%) | 0 (0) | 2 (1) | 3 (3) | 0.387 |
| FVC, L | 2.92 ± 1.06 | 2.88 ± 0.97 | 2.46 ± 1.02 | 0.003 |
| FVC, %predicted | 76.33 ± 16.71 | 79.85 ± 16.53 | 68.56 ± 23.24 | <0.001 |
| FEV1 L | 2.16 ± 0.93 | 2.10 ± 0.76 | 1.63 ± 0.77 | <0.001 |
| FEV1, %predicted | 70.91 ± 23.49 | 74.85 ± 20.23 | 58.12 ± 21.89 | <0.001 |
| FEV1/FVC ratio | 73.15 ± 16.99 | 73.86 ± 14.56 | 67.31 ± 21.21 | 0.014 |
| TLC, L | 4.91 ± 1.41 | 4.92 ± 1.47 | 4.67 ± 1.55 | 0.418 |
| TLC, %predicted | 89.12 ± 18.31 | 91.67 ± 21.52 | 85.92 ± 26.71 | 0.174 |
| RV, L | 2.01 ± 0.94 | 2.08 ± 1.01 | 2.23 ± 1.10 | 0.363 |
| RV, %predicted | 114.82 ± 53.17 | 113.01 ± 49.08 | 117.41 ± 58.12 | 0.825 |
| DLCO, mL/min/mmHg | 14.85 ± 5.36 | 15.58 ± 6.15 | 10.59 ± 0.94 | <0.001 |
| DLCO, %predicted | 64.57 ± 21.55 | 71.40 ± 26.28 | 45.07 ± 19.25 | <0.001 |
| Airway resistance, cmH2O/L/sec | 1.93 ± 1.35 | 1.88 ± 1.20 | 2.27 ± 1.48 | 0.075 |
| Change in SpO2 (Δ = SpO2 at End of Study–SpO2 at Baseline) | ||||
|---|---|---|---|---|
| 6MWT Variable | Increased (Δ ≥ +1) N = 60 (19%) | Unchanged (−2 ≤ Δ ≤ 0%) N = 146 (46%) | Decreased (Δ ≤ −3%) N = 113 (35%) | p-Value |
| SpO2, % | ||||
| Start of test | 96.57 ± 2.04 | 97.99 ± 1.89 | 97.20 ± 2.43 | <0.001 1 |
| End of test | 98.45 ± 1.63 | 97.10 ± 2.10 | 90.42 ± 5.11 | <0.001 1 |
| Change | +1.88 | −0.89 | −6.78 | <0.001 2 |
| Borg Dyspnea | ||||
| Start of test | 1.52 ± 1.64 | 1.20 ± 1.38 | 1.00 ± 1.34 | 0.076 |
| End of test | 3.51 ± 1.93 | 3.16 ± 2.23 | 3.86 ± 6.97 | 0.465 |
| Change | +1.99 | +1.96 | +2.86 | 0.611 |
| Borg Fatigue | ||||
| Start of test | 1.43 ± 1.90 | 1.48 ± 1.78 | 1.28 ± 1.65 | 0.660 |
| End of test | 3.51 ± 3.07 | 3.59 ± 2.69 | 2.82 ± 2.31 | 0.054 |
| Change | +2.08 | +2.11 | +1.54 | 0.132 |
| Pulse rate, 1/min | ||||
| Start of test | 79.13 ± 15.26 | 79.31 ± 15.96 | 80.73 ± 14.53 | 0.714 |
| End of test | 103.88 ± 24.07 | 105.66 ± 20.71 | 113.77 ± 78.72 | 0.331 |
| Change | +24.75 | +26.35 | +33.04 | 0.312 |
| 6-minute walk distance, m | 397.88 ± 147.42 | 392.99 ± 119.17 | 353.98 ± 138.27 | 0.033 1 |
| Variable | Nondesaturators (Δ SpO2 > −3%) N = 224 (70%) | Desaturators (Δ SpO2 ≤ −4%) N = 95 (30%) | p-Value |
|---|---|---|---|
| Age, years | 52.92 ± 14.11 | 57.96 ± 13.20 | 0.003 |
| Sex, no. (%) | 0.697 | ||
| Male | 82 (68) | 38 (32) | |
| Female | 142 (72) | 57 (28) | |
| Race, no. (%) | 0.364 | ||
| White | 53 (29) | 130 (71) | |
| Black | 41 (32) | 88 (68) | |
| Hispanic | 1 (100) | 0 (0) | |
| Asian | 1 (100) | 0 (0) | |
| Other | 0 (0) | 1 (100) | |
| BMI (kg/m2) | 29.42 ± 8.10 | 30.14 ± 8.19 | 0.472 |
| Obstruction (FEV1/FVC<70%), no. (%) | 39 (40) | 59 (60) | 0.01 |
| Restriction (TLC < 80%), no. (%) | 33 (34.4) | 63 (65.6) | 0.238 |
| Combined obstruction and restriction, no. (%) | 3 (3.2) | 2 (1.8) | 0.444 |
| FVC, L | 2.88 ± 0.9 | 92.43 ± 1.05 | 0.001 |
| FVC, %predicted | 78.05 ± 16.51 | 68.55 ± 24.84 | 0.002 |
| FEV1, L | 2.10 ± 0.82 | 1.59 ± 0.74 | <0.001 |
| FEV1, %predicted | 72.72 ± 21.55 | 57.64 ± 21.85 | <0.001 |
| FEV1/FVC ratio | 73.14 ± 15.80 | 67.39 ± 21.38 | 0.027 |
| TLC, L | 4.94 ± 1.45 | 4.55 ± 1.55 | 0.05 |
| TLC, % predicted | 90.89 ± 20.44 | 85.08 ± 28.09 | 0.094 |
| RV, L | 2.10 ± 1.00 | 2.16 ± 1.10 | 0.636 |
| RV, %predicted | 114.85 ± 50.58 | 114.89 ± 58.69 | 0.996 |
| DLCO, mL/min/mmHg | 15.28 ± 5.92 | 9.77 ± 4.35 | <0.001 |
| DLCO, %predicted | 68.54 ± 24.81 | 42.51 ± 19.25 | <0.001 |
| Airway resistance, cmH2O/L/sec | 1.95 ± 1.33 | 2.20 ± 1.33 | 0.144 |
| 6MWT Variables | Nondesaturators (Δ SpO2 > −3%) N = 224 (70%) | Desaturators (Δ SpO2 ≤ −4%) N = 95 (30%) | p-Value |
|---|---|---|---|
| SpO2, % | |||
| Start of test | 97.56 ± 2.07 | 97.18 ± 2.43 | 0.157 1 |
| End of test | 97.24 ± 2.26 | 89.67 ± 5.15 | <0.001 1 |
| Change | −0.32 | −7.51 | <0.001 2 |
| Borg Dyspnea | |||
| Start of test | 1.26 ± 1.48 | 1.02 ± 1.29 | 0.163 |
| End of test | 3.26 ± 2.13 | 3.97 ± 7.55 | 0.196 |
| Change | +2.00 | +2.95 | 0.465 |
| Borg Fatigue | |||
| Start of test | 1.46 ± 1.83 | 1.26 ± 1.57 | 0.354 |
| End of test | 3.52 ± 2.77 | 2.77 ± 2.28 | 0.012 |
| Change | +2.06 | +1.51 | 0.053 |
| Pulse rate, 1/min | |||
| Start of test | 79.29 ± 15.30 | 80.93 ± 15.34 | 0.383 |
| End of test | 108.96 ± 57.87 | 106.33 ± 21.38 | 0.669 |
| Change | +29.67 | +25.40 | 0.848 |
| 6-minute walk distance, m | 391.69 ± 128.83 | 352.67 ± 138.19 | 0.017 1 |
| Variable | Parameter Estimate (β) ± Standard Error | p-Value |
|---|---|---|
| (Constant) | 4.886 ± 1.783 | 0.007 |
| Age, years | 0.002 ± 0.024 | 0.933 |
| FVC, L | 0.254 ± 0.79 | 0.748 |
| FEV1, L | 0.197 ± 1.022 | 0.847 |
| DLCO, mL/min/mmHg | −0.291 ± 0.071 | <0.001 |
| Variable | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Age, years | 0.951 | 0.892, 1.014 | 0.125 |
| FVC, L | 0.883 | 0.070, 11.203 | 0.923 |
| FEV1, L | 2.816 | 0.081, 98.292 | 0.568 |
| DLCO, mL/min/mmHg | 0.909 | 0.742, 1.115 | 0.360 |
| Variable | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Age, years | 1.003 | 0.973, 1.034 | 0.859 |
| FVC, L | 0.581 | 0.174, 1.933 | 0.376 |
| FEV1, L | 3.574 | 0.751, 17.014 | 0.110 |
| DLCO, mL/min/mmHg | 0.749 | 0.655, 0.856 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gupta, R.; Ruppel, G.L.; Espiritu, J.R.D. Exercise-Induced Oxygen Desaturation during the 6-Minute Walk Test. Med. Sci. 2020, 8, 8. https://doi.org/10.3390/medsci8010008
Gupta R, Ruppel GL, Espiritu JRD. Exercise-Induced Oxygen Desaturation during the 6-Minute Walk Test. Medical Sciences. 2020; 8(1):8. https://doi.org/10.3390/medsci8010008
Chicago/Turabian StyleGupta, Raghav, Gregg L. Ruppel, and Joseph Roland D. Espiritu. 2020. "Exercise-Induced Oxygen Desaturation during the 6-Minute Walk Test" Medical Sciences 8, no. 1: 8. https://doi.org/10.3390/medsci8010008
APA StyleGupta, R., Ruppel, G. L., & Espiritu, J. R. D. (2020). Exercise-Induced Oxygen Desaturation during the 6-Minute Walk Test. Medical Sciences, 8(1), 8. https://doi.org/10.3390/medsci8010008