MRI Assessment of Global and Regional Diaphragmatic Motion in Critically Ill Patients Following Prolonged Ventilator Weaning


Abstract
:1. Introduction
2. Methods
2.1. Study Cohort
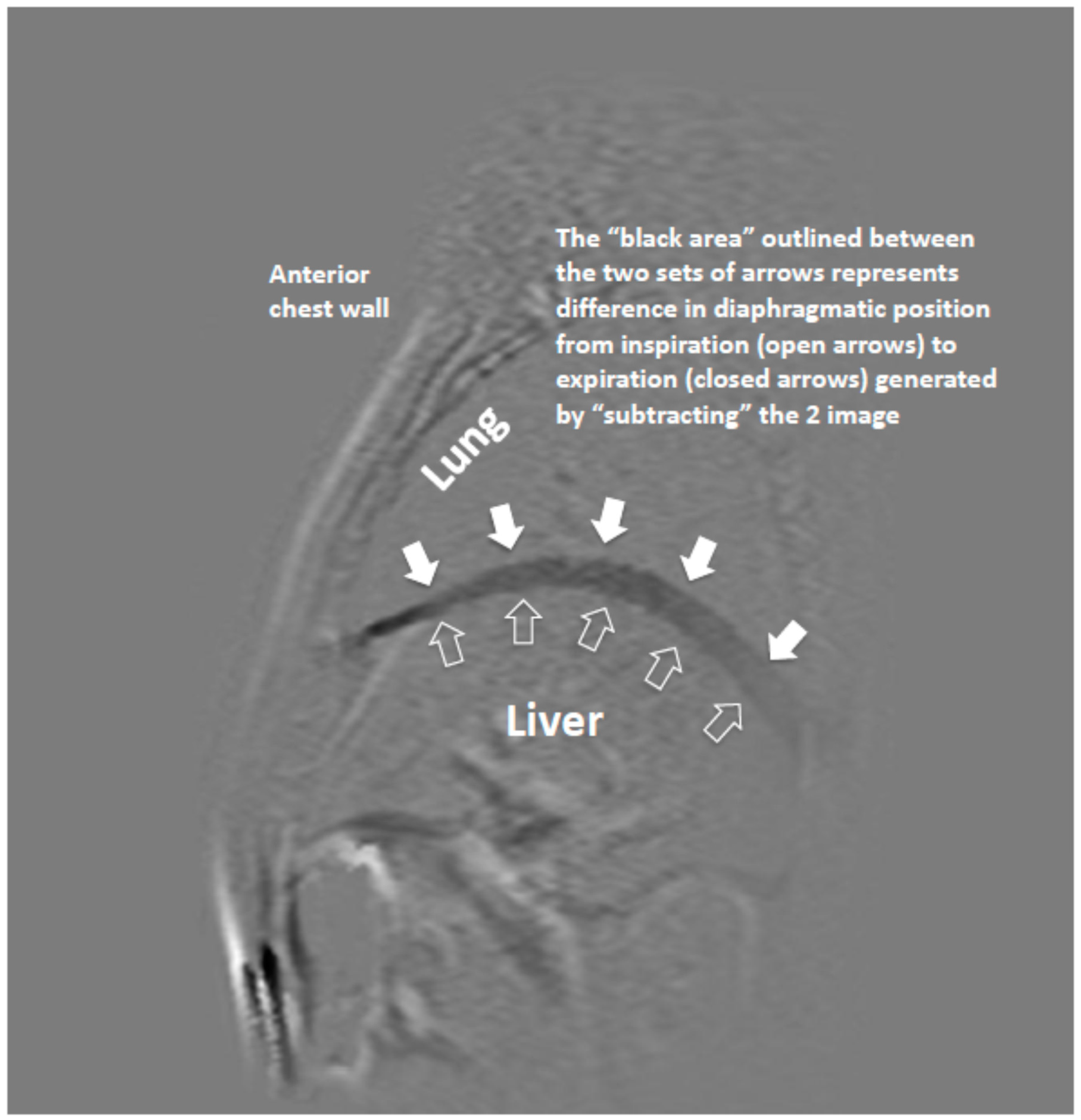
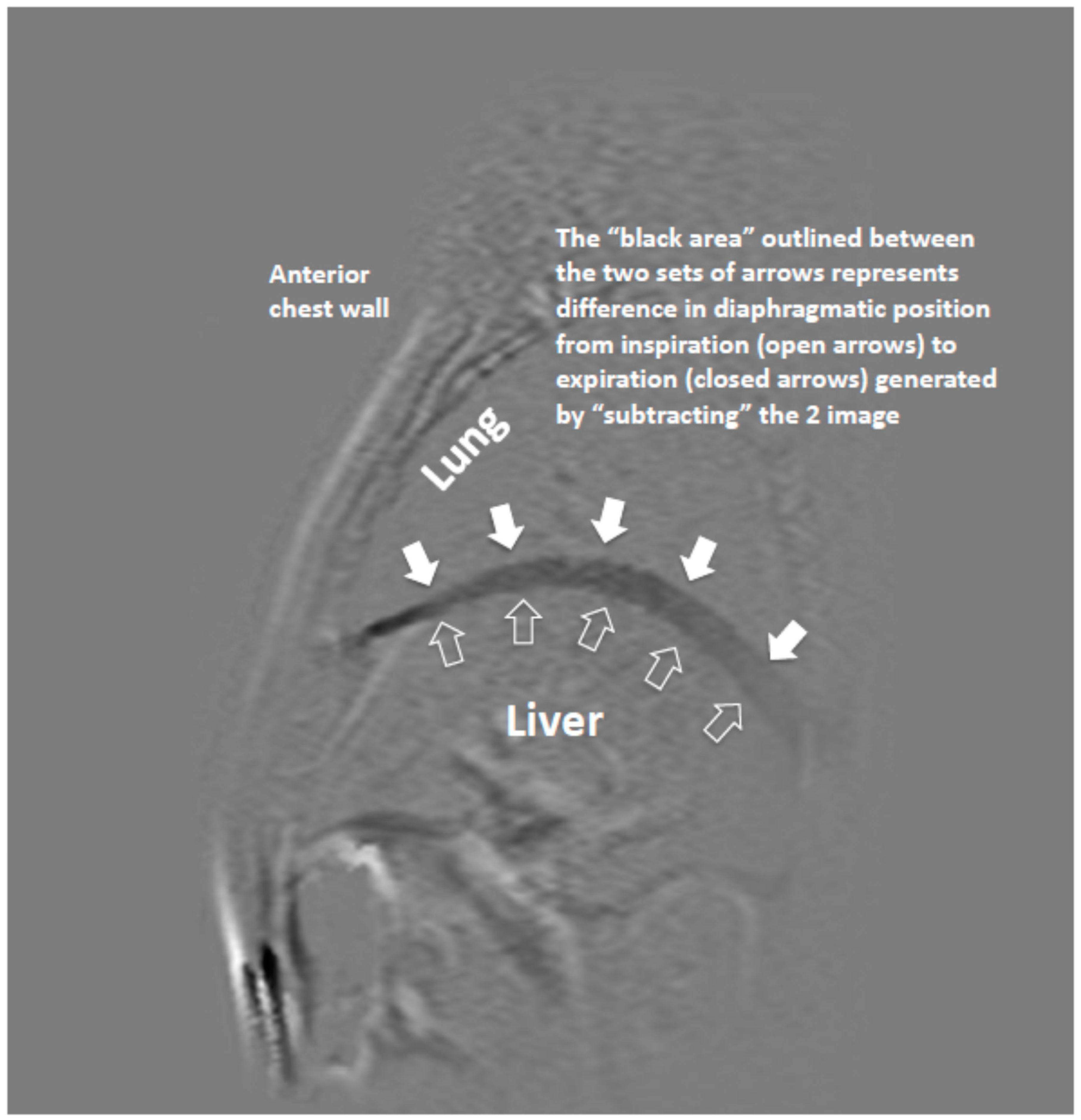
2.2. MR Imaging and Analysis of Diaphragm Motion
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. MRI Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations:
| VIDD | Ventilator Induced diaphragmatic dysfunction |
| MRI | Magnetic Resonance Imaging |
| CPAP | Continuous Positive Airway Pressure |
| COPD | Chronic Obstructive Pulmonary Disease |
| PRVC | Pressure Regulated Volume Control Ventilation |
| vs. | Volume Support ventilation |
| IQR | Interquartile range |
| MAP | Mean Arterial Pressure |
| FiO2 | Fractional Inspired Oxygen |
| BMI | Body Mass Index |
| HR | Heart Rate |
| SpO2 | Oxygen saturation by Pulse Oximetry |
| FFE | Fast Field Echo |
| RF | Radio Frequency |
| T | Tesla |
References
- Vassilakopoulos, T.; Zakynthinos, S.; Roussos, C. The tension-time index and the frequency/tidal volume ratio are the major pathophysiologic determinants of weaning failure and success. Am. J. Respir. Crit. Care Med. 1998, 158, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Purro, A.; Appendini, L.; De Gaetano, A.; Gudjonsdottir, M.; Donner, C.F.; Rossi, A. Physiologic determinants of ventilator dependence in long-term mechanically ventilated patients. Am. J. Respir. Crit. Care Med. 2000, 161, 1115–1123. [Google Scholar] [CrossRef] [PubMed]
- Vassilakopoulos, T.; Petrof, B.J. Ventilator-induced diaphragmatic dysfunction. Am. J. Respir. Crit. Care Med. 2004, 169, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Vassilakopoulos, T. Ventilator-induced diaphragm dysfunction, the clinical relevance of animal models. Intensive Care Med. 2008, 34, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Levine, S.; Nguyen, T.; Taylor, N.; Friscia, M.E.; Budak, M.T.; Rothenberg, P.; Zhu, J.; Sachdeva, R.; Sonnad, S.; Kaiser, L.R.; et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N. Engl. J. Med. 2008, 358, 1327–1335. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.N.; Mofarrahi, M.; Sigala, I.; Kim, H.C.; Vassilakopoulos, T.; Maltais, F.; Bellenis, I.; Chaturvedi, R.; Gottfried, S.B.; Metrakos, P.; et al. Mechanical ventilation-induced diaphragm disuse in humans’ triggers autophagy. Am. J. Respir. Crit. Care Med. 2010, 182, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Gierada, D.S.; Curtin, J.J.; Erickson, S.J.; Prost, R.W.; Standt, J.A.; Goodman, L.R. Diaphragm motion: Fast gradient-recalled-echo MR imaging in healthy subjects. Radiology 1995, 194, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.Y.; Suh, H.J.; Hong, S.B.; Koh, Y.; Lim, C.M. Diaphragm dysfunction assessed by ultrasonography, influence on weaning from mechanical ventilation. Crit. Care Med. 2011, 39, 2627–2630. [Google Scholar] [CrossRef] [PubMed]
- Grosu, H.B.; Lee, Y.I.; Lee, J.; Eden, E.; Eikermann, M.; Rose, K.M. Diaphragm muscle thinning in patients who are mechanically ventilated. Chest 2012, 142, 1455–1460. [Google Scholar] [CrossRef] [PubMed]
- Umbrello, M.; Formenti, P.; Longhi, D.; Galimberti, A.; Piva, I.; Pezzi, A.; Mistraletti, G.; Marini, J.J.; Iapichino, G. Diaphragm ultrasound as indicator of respiratory effort in critically ill patients undergoing assisted mechanical ventilation, a pilot clinical study. Crit. Care 2015, 19, 161. [Google Scholar] [CrossRef] [PubMed]
- Kotani, T.; Minami, S.; Takahashi, K.; Isobe, K.; Nakata, Y.; Takaso, M.; Inoue, M.; Maruta, T.; Akazawa, T.; Ueda, T.; et al. An analysis of chest wall and diaphragm motions in patients with idiopathic scoliosis using dynamic breathing. Spine 2004, 1, 298–302. [Google Scholar] [CrossRef]
- MacIntyre, N.R.; Epstein, S.K.; Carson, S.; Scheinhorn, D.; Christopher, K.; Muldoon, S. Management of patients requiring prolonged mechanical ventilation, report of a NAMDRC consensus conference. Chest 2005, 128, 3937–3954. [Google Scholar] [CrossRef] [PubMed]
- Kantarci, F.; Mihmanli, I.; Demirel, M.K.; Harmanci, K.; Akman, C.; Aydogan, F.; Mihmanli, A.; Uysal, O. Normal Diaphragmatic Motion and the Effects of Body Composition, Determination with M-Mode Sonography. J. Ultrasound Med. 2004, 23, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Boussuges, A.; Gole, Y.; Blanc, P. Diaphragm motion studied by M-Mode ultrasonongraphy. Methods, reproducibility and normal values. Chest 2009, 135, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Gerscovich, E.O.; Cronan, M.; McGahan, J.P.; Jain, K.; Jones, C.D.; McDonald, C. Ultrasonography evaluation of diaphragmatic motion. J. Ultrasound Med. 2001, 20, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Goligher, E.C.; Fan, E.; Herridge, M.S.; Murray, A.; Vorona, S.; Brace, D.; Rittayamai, N.; Lanys, A.; Tomlinson, G.; Singh, J.M. Evolution of Diaphragm Thickness during Mechanical Ventilation. Impact of Inspiratory Effort. Am. J. Respir. Crit. Care Med. 2015, 192. [Google Scholar] [CrossRef] [PubMed]
- Goligher, E.C.; Laghi, F.; Detsky, M.E.; Farias, P.; Murray, A.; Brace, D.; Brochard, L.J.; Bolz, S.S.; Rubenfeld, G.D.; Kavanagh, B.P.; et al. Measuring diaphragm thickness with ultrasound in mechanically ventilated patients, feasibility, reproducibility and validity. Intensive Care Med. 2015, 41, 642–649. [Google Scholar] [CrossRef] [PubMed]
- DiNino, E.; Gartman, E.J.; Sethi, J.M.; McCool, F.D. Diaphragm ultrasound as a predictor of successful extubation from mechanical ventilation. Thorax 2014, 69, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Giovanni, F.; Giovanna, D.F.; Fabrizio, E. Diaphragm Ultrasound as a new index of discontinuation from mechanical ventilation. Crit. Ultrasound J. 2014, 6, 8. [Google Scholar]

{kind=link}
| Features | Patient Group (Median) | Control Group (Median) |
|---|---|---|
| Age | 65 (50–78) | 36 (32–43) |
| BMI | 25.5 (24.4–26.6) | 24.9 (24.3–25.5) |
| Sex | ||
| Male | 7 | 8 |
| Females | 1 | |
| Ventilation (days) | ||
| VS | 14 (6–18) | |
| PRVC | 9 (7–20) | |
| Total | 25 (22–27) | |
| Length of ICU Stay (days) | 29 (27–37) | |
| FiO2 | 0.32 (0.26–0.4) | |
| MAP | 77 (70–88) | |
| HR | 76 (62–80) | |
| Temperature | 36.6 (36–36.9) | |
| SpO2 | 95 (94–96) |
| Patients | Admission Diagnosis | Comorbidities | Steroid Use |
|---|---|---|---|
| 1 | Pneumonia | COPD | Yes |
| 2 | Pneumonia | CCF | No |
| 3 | Pneumonia | NIDDM | No |
| 4 | Acute Pancreatitis | NIDDM, AF | No |
| 5 | Pneumonia | Hypertension CABG | No |
| 6 | Acute Pancreatitis | COPD | Yes |
| 7 | Aspiration Pneumonia | None | No |
| 8 | Pneumonia | Ischemic heart Disease | No |
| Measurement Sites | Patient Median/IQR (mm) | Control Median/IQR (mm) | P Value |
|---|---|---|---|
| Right hemidiaphragm | |||
| R1 | 6.2 (4.1–9.4) | 8.0 (5.9–12.2) | 0.18 |
| R2 | 8.9 (4.8–10.7) | 9.4 (7–17.9) | 0.14 |
| R3 | 11.1 (5.4–12.8) | 11.5 (9–20.9) | 0.15 |
| R4 | 11.6 (5.6–14.5) | 11.7 (9.1–21.6) | 0.21 |
| R5 | 10.3 (5.5–12.8) | 11.9 (10.4–18.9) | 0.06 |
| R (Mean) | 9.8 (5.0–12.3) | 10.1 (8.3–18.5) | 0.12 |
| Left hemidiaphragm | |||
| L1 | 5.0 (3.3–7.1) | 7.8 (7.1–10.5) | 0.01 |
| L2 | 5.1 (3.8–9.1) | 10.7 (6.4–12.6) | 0.02 |
| L3 | 6.7 (5.0–11.4) | 13.5 (11.5–18) | 0.005 |
| L4 | 8.6 (4.3–12.9) | 14.3 (11.5–18.8) | 0.03 |
| L5 | 8.1 (3.8–14.7) | 12.7 (10.9–17.3) | 0.05 |
| L (Mean) | 6.4 (4.6–12.2) | 11.6 (9.1–14.5) | 0.02 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saleem Khan, K.; Meaney, J.; Martin-Loeches, I.; Collins, D.V. MRI Assessment of Global and Regional Diaphragmatic Motion in Critically Ill Patients Following Prolonged Ventilator Weaning. Med. Sci. 2019, 7, 66. https://doi.org/10.3390/medsci7050066
Saleem Khan K, Meaney J, Martin-Loeches I, Collins DV. MRI Assessment of Global and Regional Diaphragmatic Motion in Critically Ill Patients Following Prolonged Ventilator Weaning. Medical Sciences. 2019; 7(5):66. https://doi.org/10.3390/medsci7050066
Chicago/Turabian StyleSaleem Khan, Khurram, James Meaney, Ignacio Martin-Loeches, and Daniel V. Collins. 2019. "MRI Assessment of Global and Regional Diaphragmatic Motion in Critically Ill Patients Following Prolonged Ventilator Weaning" Medical Sciences 7, no. 5: 66. https://doi.org/10.3390/medsci7050066
APA StyleSaleem Khan, K., Meaney, J., Martin-Loeches, I., & Collins, D. V. (2019). MRI Assessment of Global and Regional Diaphragmatic Motion in Critically Ill Patients Following Prolonged Ventilator Weaning. Medical Sciences, 7(5), 66. https://doi.org/10.3390/medsci7050066