The Use of Biochemical and Biophysical Markers in Early Screening for Preeclampsia in Mongolia

 ,
,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
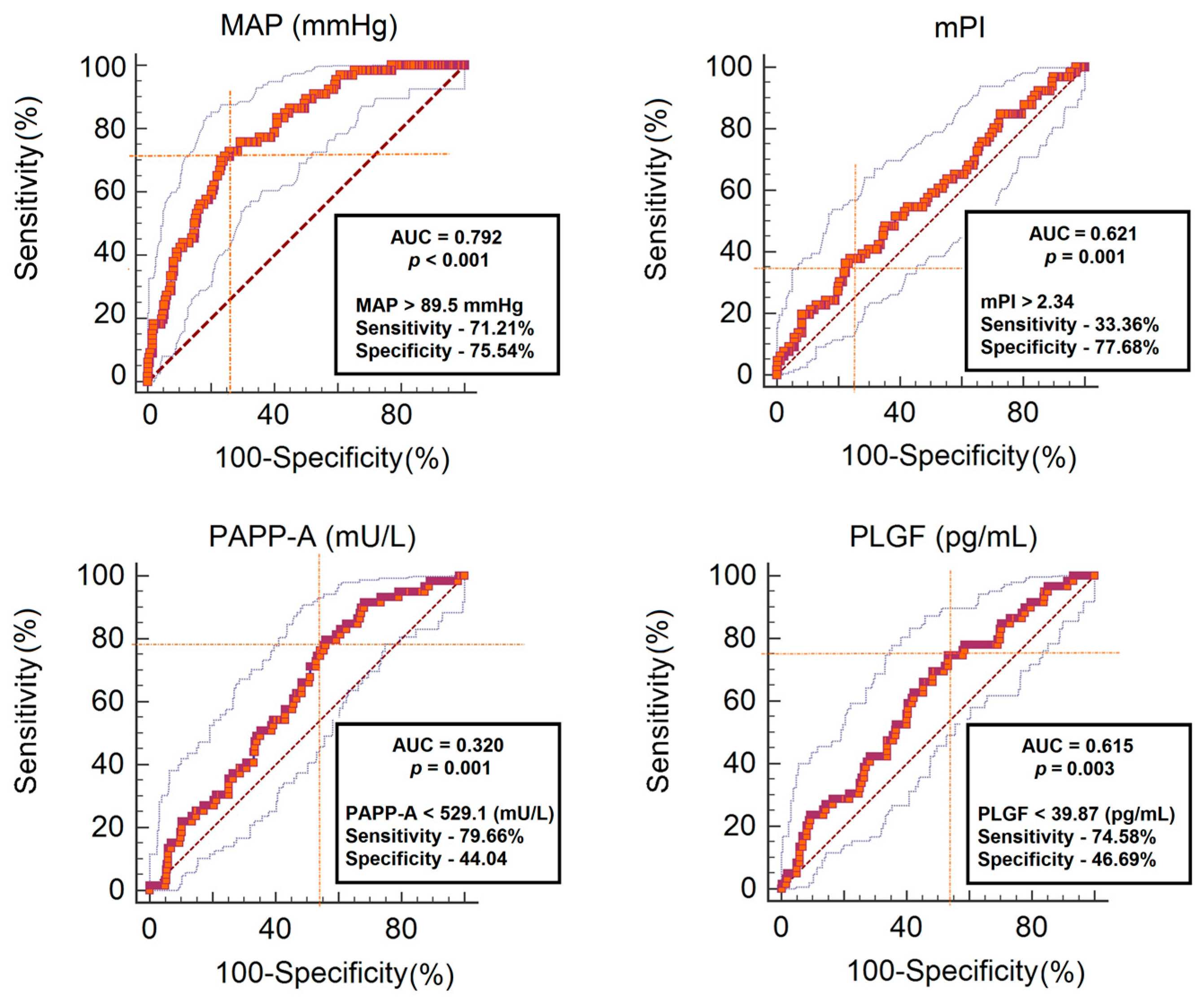
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Disclosure
References
- Khan, K.S.; Wojdyla, D.; Say, L.; Gulmezoglu, A.M.; Van Look, P.F. WHO analysis of causes of maternal death: A systematic review. Lancet 2006, 367, 1066–1074. [Google Scholar] [CrossRef]
- Huppertz, B. Placental origins of preeclampsia: Challenging the current hypothesis. Hypertension 2008, 51, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Center for Health Development. Health Indicators. 2016. Available online: http://hdc.gov.mn/2017/smta/2016%20Health%20indicator.pdf (accessed on 20 May 2018).
- Enkhtur, S.H.; Battulga, B.; Bayalag, M.; Khishgee, S. (Eds.) Why Mother Died, 3rd ed.; Munkhiin Useg Group: Ulaanbaatar, Mongolia, 2016; pp. 84–86. [Google Scholar]
- Nicolaides, K.H. Turning the pyramid of prenatal care. Fetal Diagn. Ther. 2011, 29, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Akolekar, R.; Syngelaki, A.; Sarquis, R.; Zvanca, M.; Nicolaides, K.H. Prediction of early, intermediate and late pre-eclampsia from maternal factors, biophysical and biochemical markers at 11–13 weeks. Prenat. Diagn. 2011, 31, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Poon, L.C.; Nicolaides, K.H. First-trimester maternal factors and biomarker screening for preeclampsia. Prenat. Diagn. 2014, 34, 618–627. [Google Scholar] [CrossRef] [PubMed]
- O’Gorman, N.; Wright, D.; Rolnik, D.L.; Nicolaides, K.H.; Poon, L.C. Study Protocol for the randomized controlled trial: Combined multimarker screening and randomized patient treatment with ASpirin for evidence based PREeclampsia prevention (ASPRE). BMJ Open 2016, 6, e011801. [Google Scholar] [CrossRef] [PubMed]
- Akolekar, R.; Zaragoza, E.; Poon, L.C.; Pepes, S.; Nicolaides, K.H. Maternal serum placental growth factor at 11 + 0 to 13 + 6 weeks of gestation in the prediction of pre-eclampsia. Ultrasound Obstet. Gynecol. 2008, 32, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Poon, L.C.; Akolekar, R.; Lachmann, R.; Beta, J.; Nicolaides, K.H. Hypertensive disorders in pregnancy: Screening by biophysical and biochemical markers at 11–13 weeks. Ultrasound Obstet. Gynecol. 2010, 35, 662–670. [Google Scholar] [CrossRef] [PubMed]
- Audibert, F.; Boucoiran, I.; An, N.; Aleksandrov, N.; Delvin, E.; Bujold, E.; Rey, E. Screening for preeclampsia using first-trimester serum markers and uterine artery Doppler in nulliparous women. Am. J. Obstet. Gynecol. 2010, 203, 383.e1–383.e8. [Google Scholar] [CrossRef] [PubMed]
- Poon, L.C.; Kametas, N.A.; Pandeva, I.; Valencia, C.; Nicolaides, K.H. Mean arterial pressure at 11 (+0) to 13 (+6) weeks in the prediction of preeclampsia. Hypertension 2008, 51, 1027–1033. [Google Scholar] [CrossRef] [PubMed]
- Villar, M.A.; Sibai, B.M. Clinical significance of elevated mean arterial blood pressure in second trimester and threshold increase and systolic or diastolic blood pressure during third trimester. Am. J. Obstet. Gynecol. 1989, 160, 419–423. [Google Scholar] [CrossRef]
- Oney, T.; Kaulhausen, H. The value of the mean arterial blood pressure in the second trimester (MAP-2 value) as a predictor of pregnancy induced-hypertension and preeclampsia. A. preliminary report. Clin. Exp. Hypertens. B 1983, 2, 211–216. [Google Scholar] [PubMed]
- The Fetal Medicine Foundation. Certificate of Competence in the Preeclampsia Screening and Fetal Doppler Ultrasound. Available online: http://www.fetalmedicine.org/ (accessed on 11 July 2018).
- World Health Organization. WHO Recommendations for Prevention and Treatment of Pre-Eclampsia and Eclampsia; World Health Organization: Geneva, Switzerland, 2011; Available online: http://apps.who.int/iris/bitstream/handle/10665/44703/9789241548335_eng.pdf?sequence=1 (accessed on 8 July 2018).
- Von Dadelszen, P.; Magee, L.A. Pre-eclampsia: An update. Curr. Hypertens. Rep. 2014, 16, 454. [Google Scholar] [CrossRef] [PubMed]
- Redman, C.W. Current topic: Pre-eclampsia and the placenta. Placenta 1991, 12, 301–308. [Google Scholar] [CrossRef]
- Anderson, U.D.; Olsson, M.G.; Kristensen, K.H.; Akerstrom, B.; Hansson, S.R. Review: Biochemical markers to predict preeclampsia. Placenta 2012, 33, S42–S47. [Google Scholar] [CrossRef] [PubMed]
- Levine, R.J.; Maynard, S.E.; Qian, C.; Lim, K.H.; England, L.J.; Yu, K.F.; Schisterman, E.F.; Thadhani, R.; Sachs, B.P.; Epstein, F.H.; et al. Circulating angiogenic factors and the risk of preeclampsia. N. Engl. J. Med. 2004, 350, 672–683. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.C.; Stenhouse, E.J.; Crossley, J.A.; Aitken, D.A.; Cameron, A.D.; Connor, J.M. Early pregnancy levels of pregnancy-associated plasma protein a and the risk of intrauterine growth restriction, premature birth, preeclampsia, and stillbirth. J. Clin. Endocrinol. Metab. 2002, 87, 1762–1767. [Google Scholar] [CrossRef] [PubMed]
- Yaron, Y.; Heifetz, S.; Ochshorn, Y.; Lehavi, O.; Orr-Urtreger, A. Decreased first trimester PAPP-A is a predictor of adverse pregnancy outcome. Prenat. Diagn. 2002, 22, 778–782. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.; Syngelaki, A.; Akolekar, R.; Poon, L.C.; Nicolaides, K.H. Competing risks model in screening for preeclampsia by maternal characteristics and medical history. Am. J. Obstet. Gynecol. 2015, 213, 62.e1–62.e10. [Google Scholar] [CrossRef] [PubMed]
- Spencer, K.; Yu, C.K.; Cowans, N.J.; Otigbah, C.; Nicolaides, K.H. Prediction of pregnancy complications by first-trimester maternal serum PAPP-A and free β-hCG and with second-trimester uterine artery Doppler. Prenat. Diagn. 2005, 25, 949–953. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.M.; Bindra, R.; Curcio, P.; Cicero, S.; Nicolaides, K.H. Screening for pre-eclampsia and fetal growth restriction by uterine artery Doppler at 11–14 weeks of gestation. Ultrasound Obstet. Gynecol. 2001, 18, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Parra, M.; Rodrigo, R.; Barja, P.; Bosco, C.; Fernandez, V.; Munoz, H.; Soto-Chacon, E. Screening test for preeclampsia through assessment of uteroplacental blood flow and biochemical markers of oxidative stress and endothelial dysfunction. Am. J. Obstet. Gynecol. 2005, 193, 1486–1491. [Google Scholar] [CrossRef] [PubMed]
- Gomez, O.; Martinez, J.M.; Figueras, F.; Del Rio, M.; Borobio, V.; Puerto, B.; Coll, O.; Cararach, V.; Vanrell, J.A. Uterine artery Doppler at 11–14 weeks of gestation to screen for hypertensive disorders and associated complications in an unselected population. Ultrasound Obstet. Gynecol. 2005, 26, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Pilalis, A.; Souka, A.P.; Antsaklis, P.; Daskalakis, G.; Papantoniou, N.; Mesogitis, S.; Antsaklis, A. Screening for pre-eclampsia and fetal growth restriction by uterine artery Doppler and PAPP-A at 11–14 weeks’ gestation. Ultrasound Obstet. Gynecol. 2007, 29, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Cnossen, J.S.; Vollebregt, K.C.; de Vrieze, N.; ter Riet, G.; Mol, B.W.; Franx, A.; Khan, K.S.; van der Post, J.A. Accuracy of mean arterial pressure and blood pressure measurements in predicting pre-eclampsia: Systematic review and meta-analysis. BMJ 2008, 336, 1117–1120. [Google Scholar] [CrossRef] [PubMed]
- Poon, L.C.; Kametas, N.A.; Chelemen, T.; Leal, A.; Nicolaides, K.H. Maternal risk factors for hypertensive disorders in pregnancy: A multivariate approach. J. Hum. Hypertens. 2010, 24, 104–110. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total | Preeclampsia | Unaffected PE |
|---|---|---|---|
| Maternal age (years) | 33.4 ± 6.0 | 36.1 ± 5.6 | 32.8 ± 5.9 |
| Gestational age (weeks) | 12.3 ± 0.6 | - | - |
| Maternal weight (kg) | 63.2 ± 10.8 | 69.2 ± 10.7 | 62.12 ± 10.6 |
| Fetal crown-rump length (mm) | 60.4 ± 8.6 | - | - |
| BMI (kg/m2) | 24.3 ± 3.9 | 26.8 ± 4.1 | 23.8 ± 3.7 |
| <18.5 | 14 (3.6) | 1 (1.5) | 13 (3.9) |
| 18.5–24.99 | 232 (59.0) | 21 (31.8) | 211 (64.5) |
| 25.00–29.9 | 107 (27.2) | 29 (43.9) | 78 (23.8) |
| >30 | 40 (10.2) | 15 (22.7) | 25 (7.6) |
| Medical history | |||
| Chronic hypertension | 20 (5.1) | 11 (16.7) | 9 (2.8) |
| Renal disease | 40 (10.2) | 10 (15.2) | 30 (9.2) |
| Diabetes II type | 3 (0.8) | 2 (3.0) | 1 (0.3) |
| Normal | 294 (74.8) | 35 (53.0) | 259 (79.2) |
| Other | 34 (8.7) | 8 (12.1) | 28 (8.5) |
| Previous preeclampsia | |||
| Yes | 71 (25.9) | 29 (58.0) | 42 (19.1) |
| No | 203 (74.1) | 21 (42.0) | 182 (80.9) |
| Family history of PE | |||
| Yes | 33 (8.4) | 5 (7.6) | 28 (8.5) |
| No | 299 (76.1) | 47 (71.2) | 252 (77.1) |
| Unknown | 61 (15.5) | 14 (21.2) | 47 (14.4) |
| Parity (N %) | |||
| Nulliparous | 119 (30.3) | 16 (24.2) | 103 (31.5) |
| Multiparous | 274 (69.7) | 50 (75.8) | 224 (68.5) |
| Birth weight (grams) | 3441.1 ± 503.5 | 3283.6 ± 633.2 | 3472.9 ± 467.8 |
| GA at delivery (weeks) | 39.0 ± 1.5 | 38.0 ± 1.8 | 39.2 ± 1.4 |
| Weeks | PAPP-A (mU/L) | PlGF (pg/mL) | MAP (mmHg) | mPI |
|---|---|---|---|---|
| 11–11+6 | 494.5 ± 443.4 | 37.8 ± 22.0 | 86.4 ± 9.9 | 2.1 ± 0.4 |
| 12–12+6 | 579.9 ± 497.1 | 45.8 ± 50.2 | 85.4 ± 8.2 | 2.0 ± 0.5 |
| 13–13+6 | 629.4 ± 519.8 | 63.2 ± 67.3 | 87.4 ± 9.6 | 1.9 ± 0.5 |
| Characteristics and Markers | Preeclampsia | Unaffected PE | p-Value |
|---|---|---|---|
| Maternal age (year) | 36.1 ± 5.6 | 32.8 ± 5.9 | <0.001 |
| BMI (Kg/m2) | 26.7 ± 4.1 | 23.8 ± 3.7 | <0.001 |
| Parity (nulliparous/multiparous) | 16/50 | 103/224 | <0.001 |
| Smoking (n) (yes/no) | 11/55 | 39/288 | <0.001 |
| PAPP-A (mU/L) | 366.1 ± 195.3 | 633.6 ± 496.9 | 0.003 |
| PlGF (pg/mL) | 38.6 ± 19.6 | 45.1 ± 24.0 | 0.01 |
| MAP (mm Hg) | 94.05 ± 9.05 | 84.55 ± 8.15 | <0.001 |
| mPI | 2.16 ± 0.55 | 2.0 ± 0.50 | 0.019 |
| Delivery age (weeks) | 38.0 ± 1.8 | 39.0 ± 1.4 | <0.001 |
| Birth weight (grams) | 3283.63 ± 633.19 | 3472 ± 467.86 | 0.005 |
| Risk Factors | Frequency n (%) | RR (95% CI) | p | |
|---|---|---|---|---|
| PE | Unaffected PE | |||
| Previous PE | 29 (58.0) | 42 (19.1) | 5.81 (3.27–11.16) | <0.001 |
| Chronic hypertension | 11 (16.7) | 9 (2.9) | 7.06 (2.79–17.84) | <0.001 |
| Obesity | 15 (22.7) | 25 (7.3) | 3.87 (1.89–7.92) | <0.001 |
| Birth interval > 10 years | 5 (7.8) | 28 (8.6) | 2.08 (1.03–4.19) | 0.033 |
| Kidney diseases (non glomerulonephritis) | 10 (15.2) | 30 (9.2) | 1.76 (0.81–3.82) | 0.143 |
| Smoking | 11 (16.9) | 39 (11.9) | 1.05 (0.72–3.12) | 0.270 |
| Detection Rate * (Sensitivity) | ||
|---|---|---|
| FPR (5%) | FPR (10%) | |
| With History | ||
| MAP | 62.7 (40.0–80.8) | 68.3 (46.3–86.5) |
| MAP + mPI | 69.5 (48.7–83.1) | 73.7 (54,7–89.6) |
| MAP + PAPP-A | 79.3 (56.6–89.2) | 81.1 (60.4–91.5) |
| MAP + PlGF | 86.5 (73.4–90.2) | 90.9 (78.5–92.3) |
| MAP + PlGF + PAPP-A + mPI | 91.4 (78.0–96.0) | 95.3 (80.1–96.5) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tserensambuu, U.; Chuluun-Erdene, A.; Janlav, M.; Tudevdorj, E. The Use of Biochemical and Biophysical Markers in Early Screening for Preeclampsia in Mongolia. Med. Sci. 2018, 6, 57. https://doi.org/10.3390/medsci6030057
Tserensambuu U, Chuluun-Erdene A, Janlav M, Tudevdorj E. The Use of Biochemical and Biophysical Markers in Early Screening for Preeclampsia in Mongolia. Medical Sciences. 2018; 6(3):57. https://doi.org/10.3390/medsci6030057
Chicago/Turabian StyleTserensambuu, Urjindelger, Ariunbold Chuluun-Erdene, Munkhtsetseg Janlav, and Erkhembaatar Tudevdorj. 2018. "The Use of Biochemical and Biophysical Markers in Early Screening for Preeclampsia in Mongolia" Medical Sciences 6, no. 3: 57. https://doi.org/10.3390/medsci6030057
APA StyleTserensambuu, U., Chuluun-Erdene, A., Janlav, M., & Tudevdorj, E. (2018). The Use of Biochemical and Biophysical Markers in Early Screening for Preeclampsia in Mongolia. Medical Sciences, 6(3), 57. https://doi.org/10.3390/medsci6030057