
The Novel Achievements in Oncological Metabolic Radio-Therapy: Isotope Technologies, Targeted Theranostics, Translational Oncology Research

 ,
, 
Abstract
1. Introduction
2. Methods
3. Results
3.1. Isotope Technology—Nucleus Stability/Instability
3.2. Targeted Theranostics
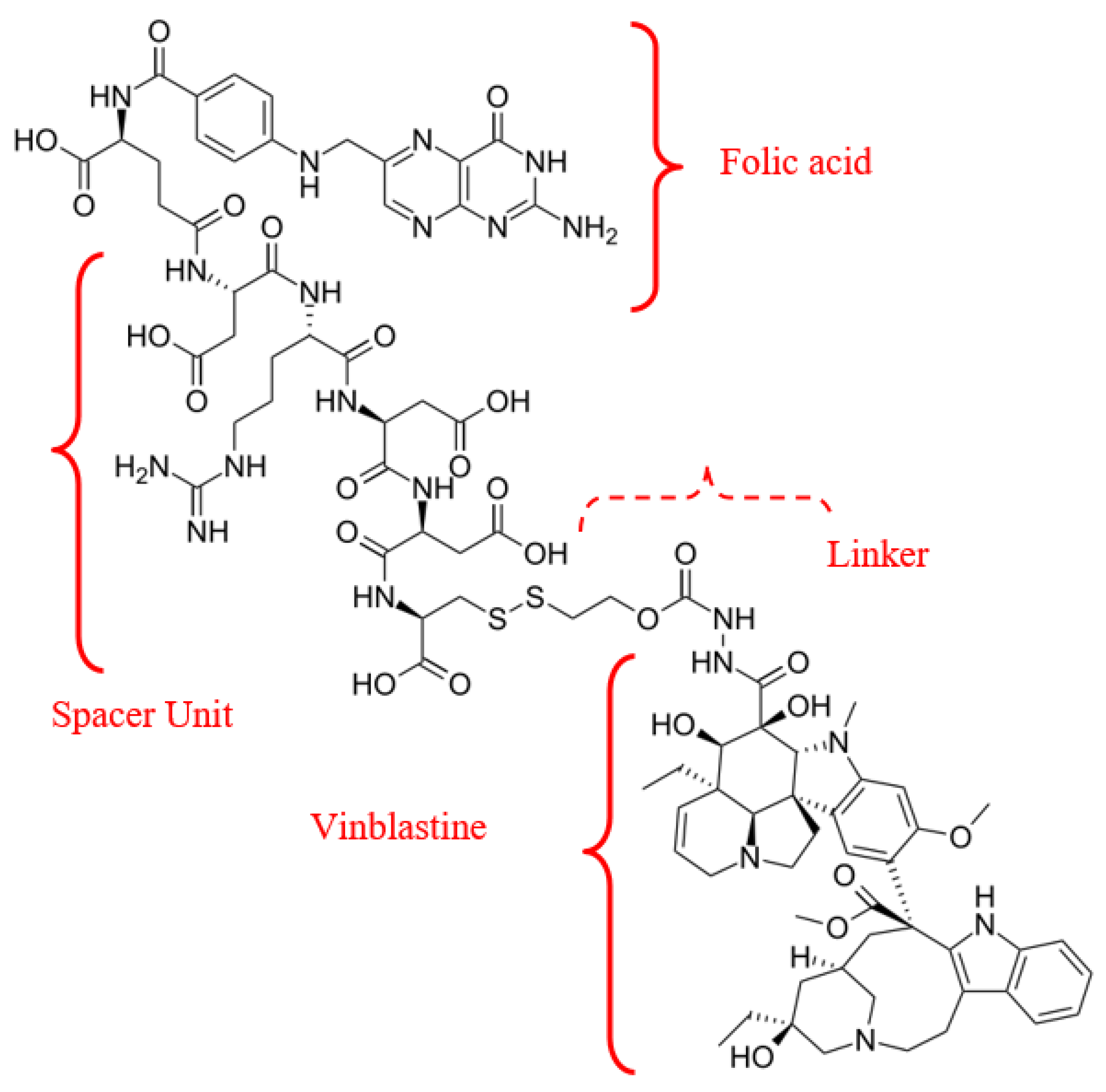
3.2.1. Radiopharmaceuticals—Antimetabolites
3.2.2. Radionuclide Therapy with Peptide Receptors
- 177Lu–Dotatate radioligand therapy (RLT)
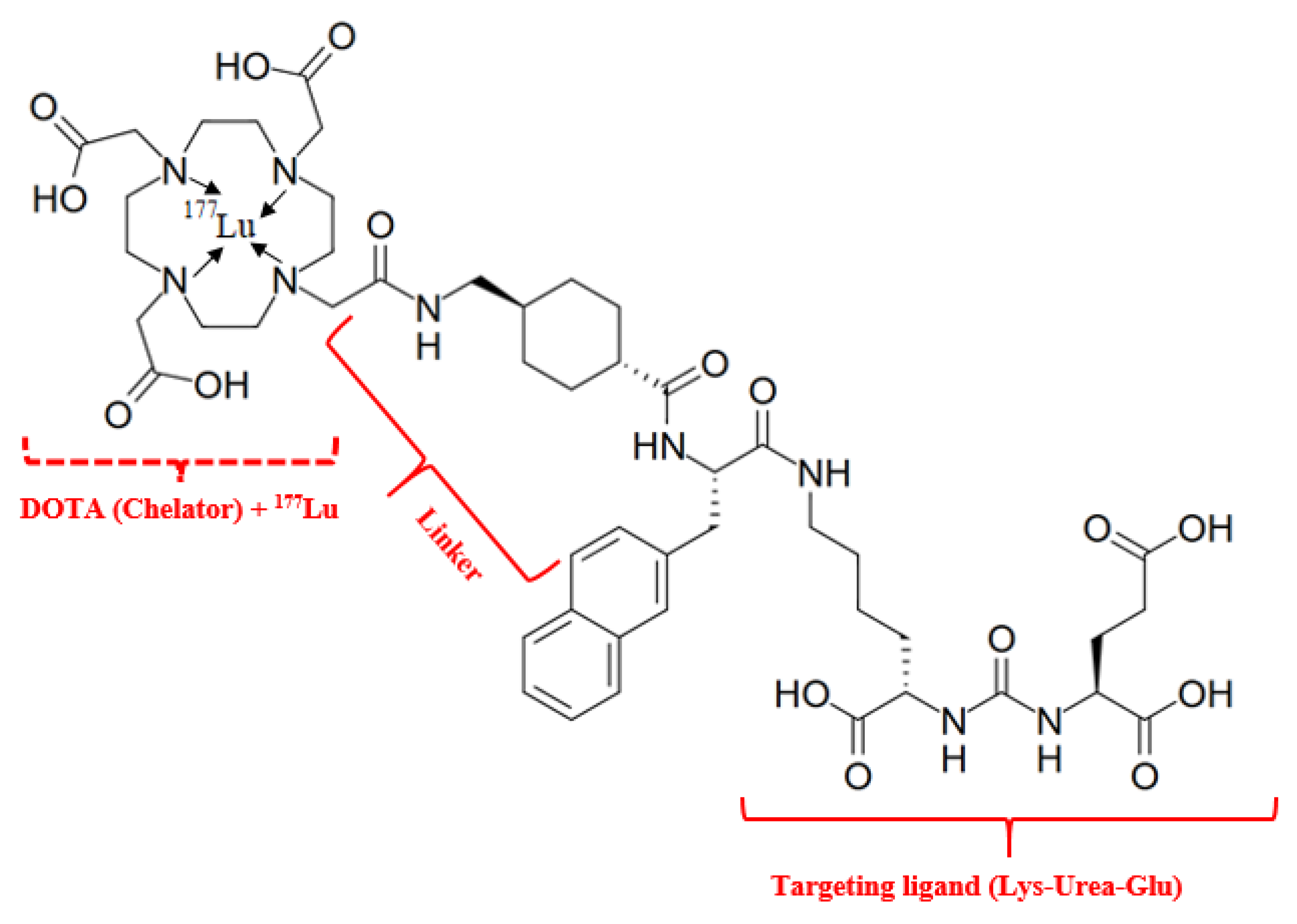
- 177Lu—vipivotide tetraxetan RLT
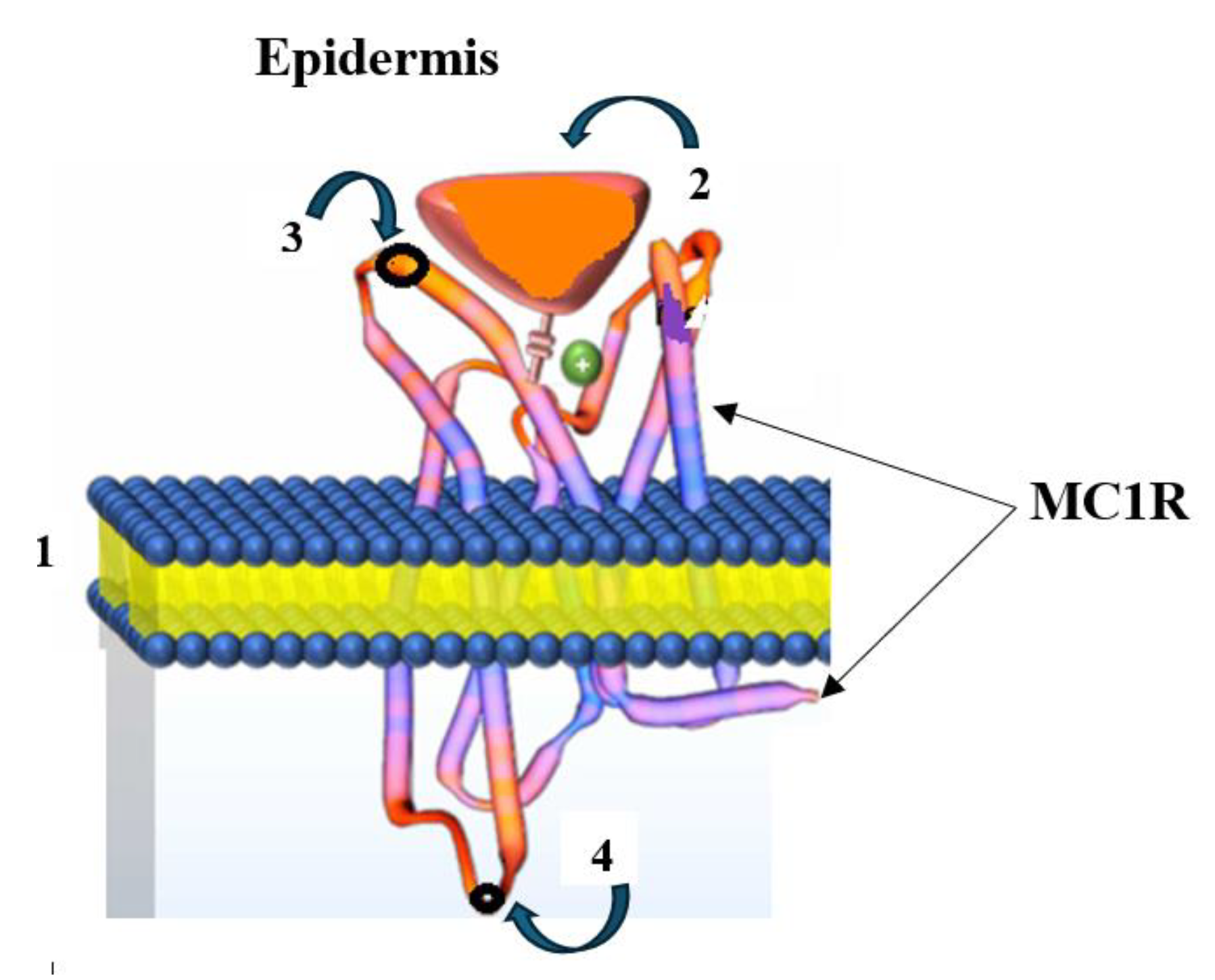
- MC1R targeting. Radioactive theranostics of melanoma
3.2.3. Radionuclide Therapy with Hormone Receptors
- 18F-Fluoroestradiol
3.2.4. Radiopharmaceuticals—Metabolites
3.3. Nanotheranostics—Prerequisites for Developments
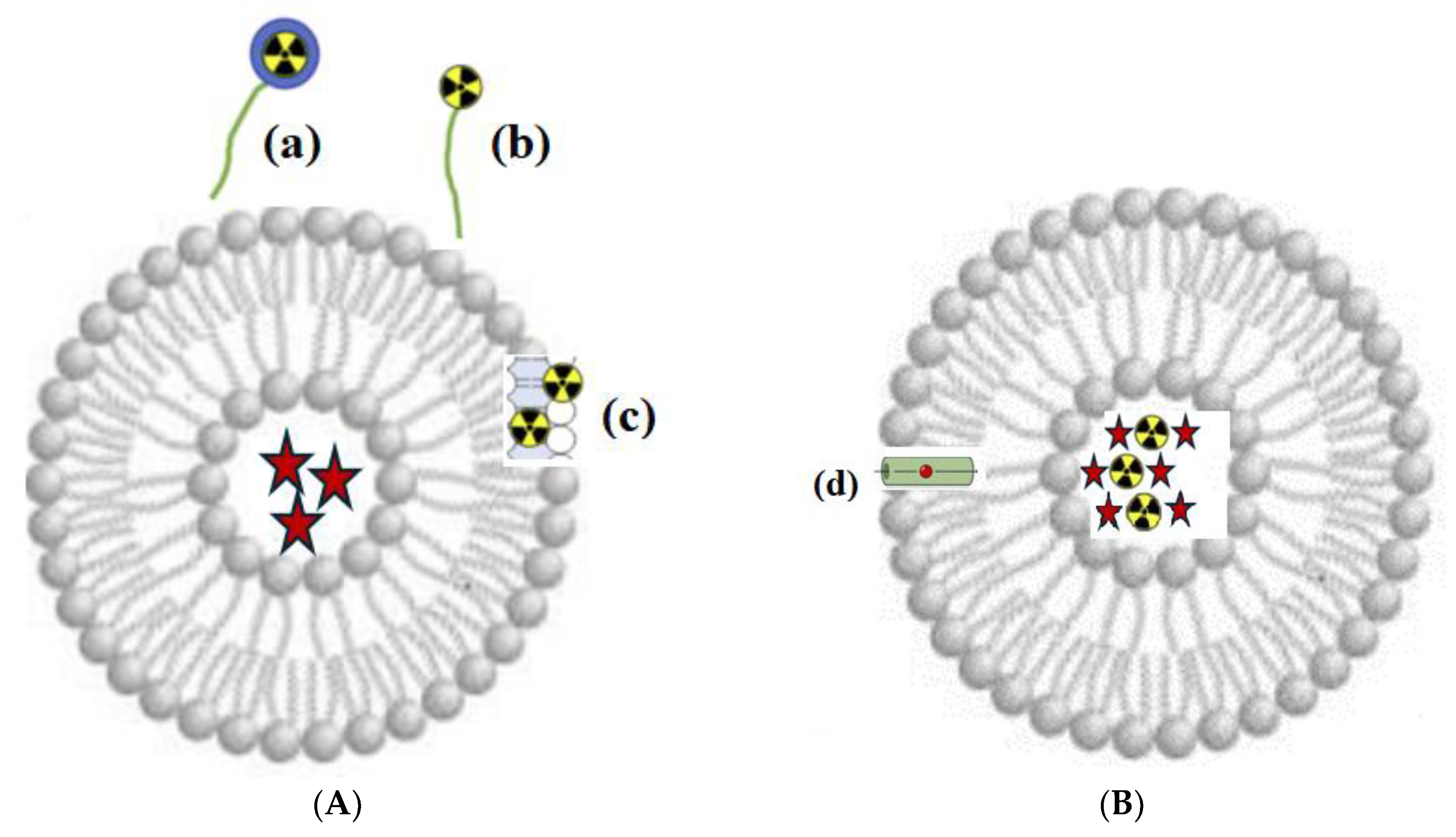
3.3.1. Radioactive Nanotheranostics
3.3.2. Nanoparticles
4. Future Directions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| IARC | International Agency for Research on Cancer |
| NCI | National Cancer Institute |
| NMSCs | Nonmelanoma skin cancers |
| SM | Sulfur mustard |
| NM | Nitrogen mustard |
| HDI | Human Development Index |
| siRNA | Small interfering RNA |
| mABs-drug | monoclonal AntiBody |
| MtRth | Metabolic RadioTherapy |
| DSB | DNA double-strand break |
| IT | Isomeric Transition |
| ISOLDE | Isotope Separator On-Line Detector |
| API | Active Pharmaceutical Ingredient |
| PET | Positron emission tomography |
| MRI | Magnetic resonance imaging |
| LET | Linear energy transfer |
| MIBG | Meta-iodobenzylguanidine |
| ARPI | Active radiopharmaceutical ingredients |
| RLT | Radioligand therapy |
| NCRT | Neoadjuvant chemoradiotherapy |
| ACRT | Adjuvant chemoradiotherapy |
| NETs | Neuroendocrine tumors |
| SST | Somatostatin |
| PRRT | Peptide receptor radionuclide therapy |
| PSMA | Prostate-specific membrane antigen |
| GEP | Gastroenteropancreatic |
| RTSR | Radioligand therapy of somatostatin receptor |
| MtMn | Metastatic melanoma |
| MC1R | Melanocortin- subtype 1 receptor |
| GPCRs | G protein-coupled receptors |
| α-MSH | α-Melanocyte-stimulating hormone |
| FES | 18F-fluoroestradiol |
| ER | Estrogen Receptor |
| PR | Progesterone Receptor |
| HR | Hormone Receptor |
| FDG | 8F-fluorodeoxyglucose |
| FR-α,β | Folate receptor alpha,beta |
| MSC | Mesenchymal stem cells |
| NNI | The National Nanotechnology Initiative |
| NCTCs | Nanocytostatic Therapeutic Complexes |
| PK | Pharmacokinetics |
| BD | Biodistribution |
| NOTA | 1,4,7-Triazacyclononane-1,4,7-Triacetic Acid |
| NODAG | Glutaric Acid Derivative of NOTA |
| DOTA | 1,4,7,10-Tetraazacyclododecane-1,4,7,10-Tetraacetic Acid |
| DODAGA | Derivative of DOTA |
| NCTCs | Nanocytostatics |
| AuNPs | Gold nanoparticles |
| AgNPs | Silver nanoparticles |
| TrAbl | Thermal ablation |
| SPIONs | SuperParamagnetic Iron Oxide Nanoparticles |
| MIH | Magnetic induction hyperthermia |
| ROS | Reactive oxygen species |
| DAC | Depletion of antioxidant capability |
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Filho, A.M.; Laversanne, M.; Ferlay, J.; Colombet, M.; Piñeros, M.; Znaor, A.; Parkin, D.M.; Soerjomataram, I.; Bray, F. The GLOBOCAN 2022 cancer estimates: Data sources, methods, and a snapshot of the cancer burden worldwide. Int. J. Cancer 2024, 156, 1336–1346. [Google Scholar] [CrossRef]
- Pucci, C.; Martinelli, C.; Ciofani, G. Innovative approaches for cancer treatment: Current perspectives and new challenges. Ecancermedicalscience 2019, 13, 961. [Google Scholar] [CrossRef]
- Abergel, R.; Aris, J.; Bolch, W.E.; Dewji, S.A.; Golden, A.; Hooper, D.A.; Margot, D.; Menker, C.G.; Paunesku, T.; Schaue, D.; et al. The enduring legacy of Marie Curie: Impacts of radium in 21st century radiological and medical sciences. Int. J. Radiat. Biol. 2022, 98, 267–275. [Google Scholar] [CrossRef]
- Elliott, R.L. Combination cancer immunotherapy “Expanding Paul Ehrlich’s Magic Bullet Concept”. Surg. Oncol. 2012, 21, 53–55. [Google Scholar] [CrossRef]
- Lewis, W.D.; Lilly, S.; Jones, K.L. Lymphoma: Diagnosis and Treatment. Am. Fam. Physician 2020, 101, 34–41. [Google Scholar] [CrossRef]
- Liner, K.; Brown, C.; McGirt, L.Y. Clinical potential of mechlorethamine gel for the topical treatment of mycosis fungoides-type cutaneous T-cell lymphoma: A review on current efficacy and safety data. Drug Des. Devel. Ther. 2018, 12, 241–254. [Google Scholar] [CrossRef] [PubMed]
- Goodman, L.S.; Wintrobe, M.M.; Dameshek, W.; Goodman, M.J.; Gilman, A.; McLennan, M.T. Nitrogen mustard therapy. Use of methyl-bis(beta-chloroethyl) amine hydrochloride and tris(beta-chloroethyl) amine hydrochloride for Hodgkin’s disease, lymphosarcoma, leukemia and certain allied and miscellaneous disorders. JAMA 1984, 251, 2255–2261. [Google Scholar] [CrossRef]
- Ravichandran, R. Radioactive Cobalt-60 Teletherapy Machine—Estimates of Personnel Dose in Mock Emergency in Patient Release during “Source Stuck Situation”. J. Med. Phys. 2017, 42, 96–98. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.; Kudchodkar, S.B.; Chung, C.N.; Park, Y.K.; Xu, Z.; Pardi, N.; Abdel-Mohsen, M.; Muthumani, K. Expanding the Reach of Monoclonal Antibodies: A Review of Synthetic Nucleic Acid Delivery in Immunotherapy. Antibodies 2023, 12, 46. [Google Scholar] [CrossRef] [PubMed]
- Palamà, I.E.; Leporatti, S. Nanomedicine in Cancer Targeting and Therapy. J. Pers. Med. 2022, 12, 1312. [Google Scholar] [CrossRef]
- Henderson, M.L.; Zieba, J.K.; Li, X.; Campbell, D.B.; Williams, M.R.; Vogt, D.L.; Bupp, C.P.; Edgerly, Y.M.; Rajasekaran, S.; Hartog, N.L. Gene Therapy for Genetic Syndromes: Understanding the Current State to Guide Future Care. BioTech 2024, 13, 1. [Google Scholar] [CrossRef]
- Song, Y.; Zou, J.; Castellanos, E.A.; Matsuura, N.; Ronald, J.A.; Shuhendler, A.; Weber, W.A.; Gilad, A.A.; Müller, C.; Witney, T.H.; et al. Theranostics—A sure cure for cancer after 100 years? Theranostics 2024, 14, 2464–2488. [Google Scholar] [CrossRef]
- Moazzam, M.; Zhang, M.; Hussain, A.; Yu, X.; Huang, J.; Huang, Y. The landscape of nanoparticle-based siRNA delivery and therapeutic development. Mol. Ther. 2024, 32, 284–312. [Google Scholar] [CrossRef]
- Bonnet, B.; Tournier, L.; Deschamps, F.; Yevich, S.; Marabelle, A.; Robert, C.; Albiges, L.; Besse, B.; Bonnet, V.; De Baère, T. Thermal Ablation Combined with Immune Checkpoint Blockers: A 10-Year Monocentric Experience. Cancers 2024, 16, 855. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.S.; Salari, E.; Chen, X.; Switchenko, J.; Eaton, B.R.; Zhong, J.; Yang, X.; Shu, H.-K.G.; Sudmeier, L.J. Radiomic Analysis of Treatment Effect for Patients with Radiation Necrosis Treated with Pentoxifylline and Vitamin E. Tomography 2024, 10, 1501–1512. [Google Scholar] [CrossRef]
- Scott, E.C.; Baines, A.C.; Gong, Y. Trends in the approval of cancer therapies by the FDA in the twenty-first century. Nat. Rev. Drug Discov. 2023, 22, 625–640. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Häggström, I.; Szczypiński, P.; Gibbs, P.; Cook, G. Introduction to Radiomics. J. Nucl. Med. 2020, 61, 488–495. [Google Scholar] [CrossRef] [PubMed]
- National Research Council (US); Institute of Medicine (US); Committee on State of the Science of Nuclear Medicine. Advancing Nuclear Medicine Through Innovation; National Academies Press: Washington, DC, USA, 2007. [Google Scholar]
- Goetz, L.H.; Schork, N.J. Personalized medicine: Motivation, challenges, and progress. Fertil. Steril. 2018, 109, 952–963. [Google Scholar] [CrossRef]
- Otto, T. Personal dose-equivalent conversion coefficients for 1252 radionuclides. Radiat. Prot. Dosim. 2016, 168, 1–10. [Google Scholar] [CrossRef]
- Stokke, C.; Kvassheim, M.; Blakkisrud, J. Radionuclides for Targeted Therapy: Physical Properties. Molecules 2022, 27, 5429. [Google Scholar] [CrossRef] [PubMed]
- Alpha Emitter Radiation Therapy National Cancer Institute (NCI). Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/alpha-emitter-radiation-therapy (accessed on 17 May 2025).
- Selected Beta Particle Emitting Radionuclides for Therapeutic Nuclear Medicine by Open Medscience. Available online: https://openmedscience.com (accessed on 7 January 2025).
- Ku, A.; Facca, V.J.; Cai, Z.; Reilly, R.M. Auger electrons for cancer therapy—A review. EJNMMI Radiopharm. Chem. 2019, 4, 27. [Google Scholar] [CrossRef] [PubMed]
- Anuradha, A.; Undavalli, S.B.; Kumar, A.J. DNA mutilation: A telltale sign of cancer inception. J. Oral Maxillofac. Pathol. 2023, 27, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Syroeshkin, A.V.; Uspenskaya, E.V.; Levitskaya, O.V.; Kuzmina, E.S.; Kazimova, I.V.; Quynh, H.T.N.; Pleteneva, T.V. New Approaches to Determining the D/H Ratio in Aqueous Media Based on Diffuse Laser Light Scattering for Promising Application in Deuterium-Depleted Water Analysis in Antitumor Therapy. Sci. Pharm. 2024, 92, 63. [Google Scholar] [CrossRef]
- Yang, S.N. Two-Boson Exchange Physics: A Brief Review. Few-Body Syst. 2013, 54, 45–51. [Google Scholar] [CrossRef]
- Adamian, G.G.; Antonenko, N.V.; Diaz-Torres, A. How to extend the chart of nuclides? Eur. Phys. J. 2020, 56, 47. [Google Scholar] [CrossRef]
- Arsenyev, N.N.; Severyukhin, A.P. Electric Dipole Polarizability of Magic Nuclei. Mosc. Univ. Phys. 2024, 79, 200–207. [Google Scholar] [CrossRef]
- Burkhardt, C.; Bühler, L.; Viertl, D.; Stora, T. New Isotopes for the Treatment of Pancreatic Cancer in Collaboration with CERN: A Mini Review. Front. Med. 2021, 8, 674656. [Google Scholar] [CrossRef]
- Bara, S.; Jajčišinová, E.; Cocolios, T.E.; Andel, B.; Antalic, S.; Camaiani, A.; Costache, C.; Dockx, K.; Farooq-Smith, G.J.; Kellerbauer, A.; et al. Half-life determination of 215At and 221Ra with high-purity radioactive ion beams. Appl. Radiat. Isot. 2024, 208, 111289. [Google Scholar] [CrossRef]
- El-Azony, K.M.; Mohamed, N.M.A.; Aloraini, D.A. Advantages and disadvantages of nuclear reactions used in reactors or cyclotrons, in addition to a theoretical study based on photodisintegration on natural indium for 111Ag production. Nucl. Sci. Tech. 2022, 33, 14. [Google Scholar] [CrossRef]
- Moya, E.; Cerrato, C.; Bedoya, L.M. Radiopharmaceutical small-scale preparation in Europe: Will we be able to harmonize the situation? EJNMMI Radiopharm. Chem. 2024, 9, 64. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.J.; Foy, K.C.; Kaumaya, P.T. Cancer immunotherapy: Present status, future perspective, and a new paradigm of peptide immunotherapeutics. Discov. Med. 2013, 15, 166–176. [Google Scholar]
- Idée, J.M.; Louguet, S.; Ballet, S.; Corot, C. Theranostics and contrast-agents for medical imaging: A pharmaceutical company viewpoint. Quant. Imaging Med. Surg. 2013, 3, 292–297. [Google Scholar] [PubMed]
- Okamoto, S.; Shiga, T.; Tamaki, N. Clinical Perspectives of Theranostics. Molecules 2021, 26, 2232. [Google Scholar] [CrossRef]
- Kelkar, S.S.; Reineke, T.M. Theranostics: Combining imaging and therapy. Bioconjug. Chem. 2011, 22, 1879–1903. [Google Scholar] [CrossRef]
- Siegel, E. The beginnings of radioiodine therapy of metastatic thyroid carcinoma: A memoir of Samuel M. Seidlin, M. D. (1895–1955) and his celebrated patient. Cancer Biother. Radiopharm. 1999, 14, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Lișcu, H.D.; Verga, N.; Atasiei, D.I.; Ilie, A.-T.; Vrabie, M.; Roșu, L.; Poștaru, A.; Glăvan, S.; Lucaș, A.; Dinulescu, M.; et al. Therapeutic Management of Locally Advanced Rectal Cancer: Existing and Prospective Approaches. J. Clin. Med. 2025, 14, 912. [Google Scholar] [CrossRef]
- Hennrich, U.; Eder, M. [177Lu] Lu-PSMA-617 (PluvictoTM): The First FDA-Approved Radiotherapeutical for Treatment of Prostate Cancer. Pharmaceuticals 2022, 15, 1292. [Google Scholar] [CrossRef]
- Burki, T.K. 177Lu-Dotatate for midgut neuroendocrine tumours. Lancet Oncol. 2017, 18, e74. [Google Scholar] [CrossRef]
- Imhof, A.; Brunner, P.; Marincek, N. Response, survival, and long-term toxicity after therapy with the radiolabeled somatostatin analogue [90Y-DOTA]-TOC in metastasized neuroendocrine cancers. J. Clin. Oncol. 2011, 29, 2416–2423. [Google Scholar] [CrossRef]
- Bodei, L.; Kidd, M.; Paganelli, G. Long-term tolerability of PRRT in 807 patients with neuroendocrine tumours: The value and limitations of clinical factors. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Reilly, R.M.B. The radiopharmaceutical science of monoclonal antibodies and peptides for imaging and targeted in situ radiotherapy of malignancies. In Handbook of Pharmaceutical Biotechnology; Gad, S.C., Ed.; John Wiley & Sons: Toronto, ON, Canada, 2007; pp. 987–1053. [Google Scholar]
- Chambers, C.G.; Wang, J.; Sakr, T.M.; Miao, Y.; Smith, C.J. NOTA and NODAGA Radionuclide Complexing Agents: Versatile Approaches for Advancements in Radiochemistry. Molecules 2025, 30, 2095. [Google Scholar] [CrossRef]
- D’Onofrio, A.; Engelbrecht, S.; Läppchen, T.; Rominger, A.; Gourni, E. GRPR-targeting radiotheranostics for breast cancer management. Front. Med. 2023, 10, 1250799. [Google Scholar] [CrossRef]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. NETTER-1 Trial Investigators. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Keam, S.J. Lutetium Lu 177 Vipivotide Tetraxetan: First Approval. Mol. Diagn. Ther. 2022, 26, 467–475. [Google Scholar] [CrossRef]
- Li, A.A.; Geliashvili, T.M.; Rumyantsev, A.A.; Pronin, A.I.; Krylov, A.S.; Baranova, O.D.; Parnas, A.V.; Ilyakov, V.S.; Vorobyeva, D.A. Impressive response to 177Lu-PSMA-617 therapy in a patient with metastatic castration-resistant prostate cancer refractory to apalutamide, docetaxel and metastasis-directed therapy. Onkourologiya Cancer Urol. 2024, 20, 98–103. (In Russian) [Google Scholar] [CrossRef]
- Heyder, N.A.; Kleinau, G.; Speck, D. Structures of active melanocortin-4 receptor–Gs-protein complexes with NDP-α-MSH and setmelanotide. Cell Res. 2021, 31, 1176–1189. [Google Scholar] [CrossRef]
- Suominen, A.; Suni, A.; Ruohonen, S.; Szabó, Z.; Pohjolainen, L.; Cai, M.; Savontaus, E.; Talman, V.; Kerkelä, R.; Petteri, R. Melanocortin 1 Receptor Regulates Pathological and Physiological Cardiac Remodeling. J. Am. Heart Assoc. 2025, 14, 037961. [Google Scholar] [CrossRef] [PubMed]
- Mun, Y.; Kim, W.; Shin, D. Melanocortin 1 Receptor (MC1R): Pharmacological and Therapeutic Aspects. Int. J. Mol. Sci. 2023, 24, 12152. [Google Scholar] [CrossRef] [PubMed]
- Baidoo, K.E.; Milenic, D.E.; Brechbiel, M.W. Methodology for labeling proteins and peptides with lead-212. Nucl. Med. Biol. 2013, 40, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Azzam, A.; Said, S.A.; Al-abyad, M. Evaluation of different production routes for the radio medical isotope 203Pb using TALYS 1.4 and EMPIRE 3.1 code calculations. Appl. Radiate Isot. 2014, 91, 109–113. [Google Scholar] [CrossRef]
- McNeil, B.L.; Robertson, A.K.H.; Fu, W. Production, purification, and radiolabeling of the 203Pb/212Pb theranostic pair. EJNMMI Radiopharm. Chem. 2021, 6, 6. [Google Scholar] [CrossRef]
- Kosenko, V.V.; Trapkova, A.A.; Kalmykov, S.N. Regulation of radiopharmaceutical products. Bulletin of the Scientific Centre for Expert Evaluation of Medicinal Products. Regul. Res. Med. Eval. 2022, 12, 379–388. [Google Scholar]
- Venema, C.M.; Apollonio, G.; Hospers, G.A.; Schröder, C.P.; Dierckx, R.A.; Vries, E.F.; Glaudemans, A.W. Recommendations and Technical Aspects of 16α-[18F]Fluoro-17β-Estradiol PET to Image the Estrogen Receptor In Vivo: The Groningen Experience. Clin. Nucl. Med. 2016, 41, 844–851. [Google Scholar] [CrossRef]
- Parnas, A.V.; Pronin, A.I.; Ilyakov, V.S.; Meshcheryakova, N.A.; Kamolova, Z.K.; Mikhaylov, A.I. [18F]-Fluoroestradiol PET/CT: A modern look at nuclear medicine applications. Tumors Female Reprod. Syst. 2021, 17, 20–26. [Google Scholar] [CrossRef]
- Talbot, J.N.; Gligorov, J.; Nataf, V.; Montravers, F.; Huchet, V.; Michaud, L.; Ohnona, J.; Balogova, S.; Cussenot, O.; Daraï, E.; et al. Current applications of PET imaging of sex hormone receptors with a fluorinated analogue of estradiol or of testosterone. Q. J. Nucl. Med. Mol. Imaging 2015, 59, 4–17. [Google Scholar]
- O’Brien, S.R.; Edmonds, C.E.; Lanzo, S.M.; Weeks, J.K.; Mankoff, D.A.; Pantel, A.R. 18F-Fluoroestradiol: Current Applications and Future Directions. Radiographics 2023, 43, e220143. [Google Scholar] [CrossRef] [PubMed]
- Banyal, A.; Tiwari, S.; Sharma, A.; Chanana, I.; Patel, S.K.S.; Kulshrestha, S.; Kumar, P. Vinca alkaloids as a potential cancer therapeutics: Recent update and future challenges. 3 Biotech 2023, 13, 211. [Google Scholar] [CrossRef]
- Zhou, Y.; Unno, K.; Hyjek, E.; Liu, H.; Zimmerman, T.; Karmakar, S.; Putt, K.S.; Shen, J.; Low, P.S.; Wickrema, A. Expression of functional folate receptors in multiple myeloma. Leuk. Lymphoma 2018, 59, 2982–2989. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Chen, Y.; Wang, C.; Xia, Y.; Yu, T.; Tang, M.; Meng, K.; Yin, L.; Yang, Y.; Shen, L.; et al. The role of mesenchymal stem cells in cancer and prospects for their use in cancer therapeutics. MedComm 2024, 5, e663. [Google Scholar] [CrossRef]
- Vergote, I.; Leamon, C.P. Vintafolide: A novel targeted therapy for the treatment of folate receptor expressing tumors. Ther. Adv. Med. Oncol. 2015, 7, 206–218. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 13342, Vinblastine. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Vinblastine (accessed on 23 May 2025).
- Surh, Y.J. The 50-Year War on Cancer Revisited: Should We Continue to Fight the Enemy Within? J. Cancer Prev. 2021, 26, 219–223. [Google Scholar] [CrossRef]
- DeVita, V.T.; Rosenberg, S.A., Jr. Two hundred years of cancer research. N. Engl. J. Med. 2012, 366, 2207–2214. [Google Scholar] [CrossRef]
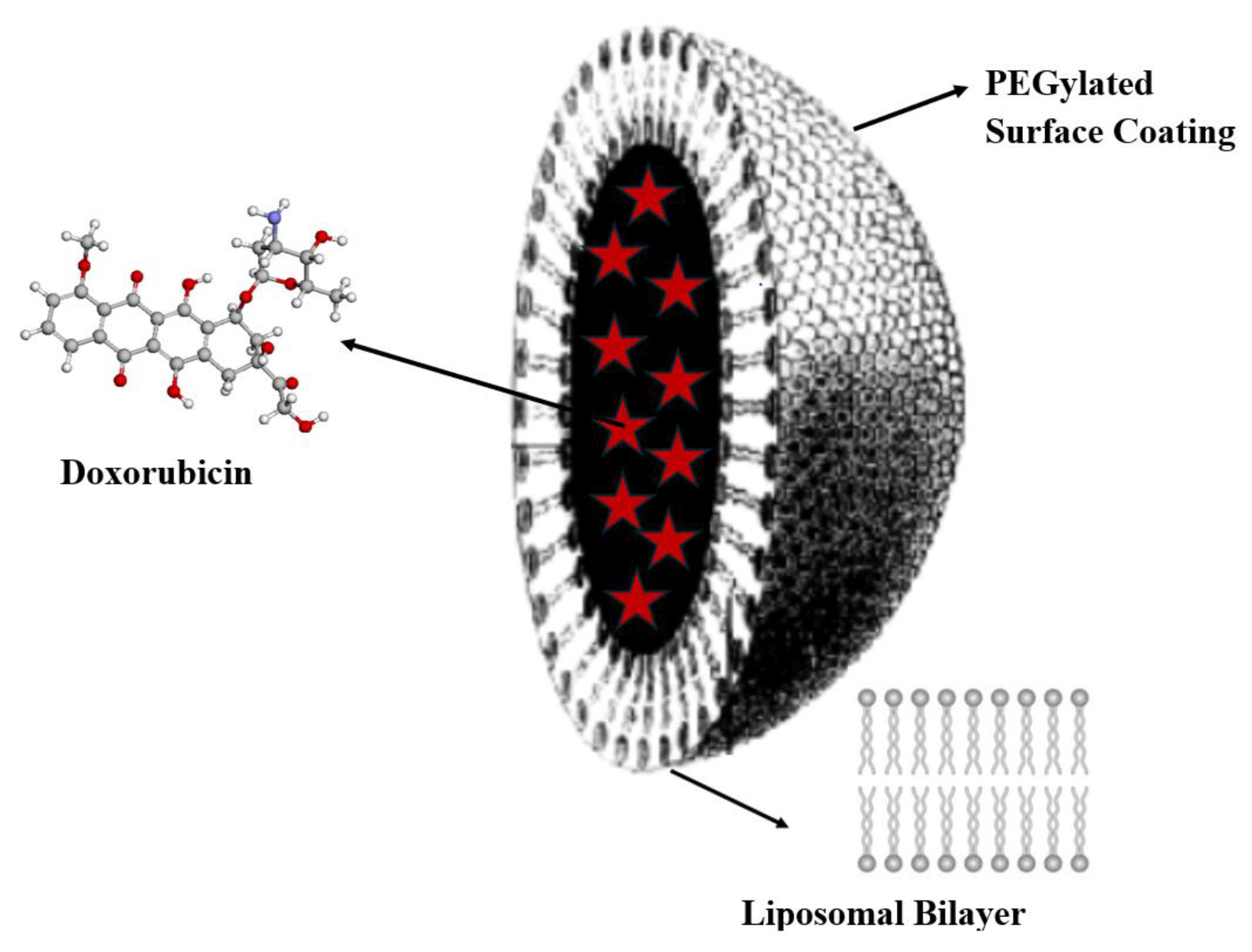
- Gabizon, A.; Shmeeda, H.; Barenholz, Y. Pharmacokinetics of pegylated liposomal doxorubicin: Review of animal and humanstudies. Clin. Pharmacokinet. 2003, 42, 419–436. [Google Scholar] [CrossRef]
- Barenholz, Y. Doxil®—The first FDA-approved nano-drug: Lessons learned. J. Control. Release 2012, 160, 117–134. [Google Scholar] [CrossRef]
- Vysikaylo, P.I.; Samsonenko, N.V.; Semin, M.V. De Broglie wave in vacuum, matter and nanostructures. J. Phys. Conf. Ser. 2020, 1560, 012006. [Google Scholar] [CrossRef]
- Daniel, M.C.; Didier, A. Gold Nanoparticles: Assembly, Supramolecular Chemistry, Quantum-Size-Related Properties, and Applications toward Biology, Catalysis, and Nanotechnology. Chem. Rev. 2004, 104, 293–346. [Google Scholar] [CrossRef] [PubMed]
- Feynman, R.P. There’s plenty of room at the bottom. Eng. Sci. 1960, 23, 22–36. [Google Scholar]
- Yeo, J.; Jung, G.S.; Martín-Martínez, F.J.; Ling, S.; Gu, G.X.; Qin, Z.; Buehler, M.J. Materials-by-Design: Computation, Synthesis, and Characterization from Atoms to Structures. Phys. Scr. 2018, 93, 053003. [Google Scholar] [CrossRef]
- Ghaffar, K.A.; Giddam, A.K.; Zaman, M.; Skwarczynski, M.; Toth, I. Liposomes as nanovaccine delivery systems. Curr. Top. Med. Chem. 2014, 14, 1194–1208. [Google Scholar] [CrossRef] [PubMed]
- De Leo, V.; Maurelli, A.M.; Giotta, L.; Catucci, L. Liposomes containing nanoparticles: Preparation and applications. Colloids Surf. B Biointerfaces 2022, 218, 112737. [Google Scholar] [CrossRef]
- Bayda, S.; Adeel, M.; Tuccinardi, T.; Cordani, M.; Rizzolio, F. The History of Nanoscience and Nanotechnology: From Chemical-Physical Applications to Nanomedicine. Molecules 2019, 25, 112. [Google Scholar] [CrossRef] [PubMed]
- National Nanotechnology Initiative (NNI). Available online: www.nano.gov (accessed on 1 June 2025).
- Satterlee, A.B.; Yuan, H.; Huang, L. A radio-theranostic nanoparticle with high specific drug loading for cancer therapy and imaging. J. Control. Release 2015, 217, 170–182. [Google Scholar] [CrossRef]
- Phillips, W.T.; Goins, B.A.; Bao, A. Wiley Interdisciplinary Reviews: Nanomedicine and Nanobiotechnology. Radioact. Liposomes 2008, 1, 69–83. [Google Scholar]
- Man, F.; Gawne, P.J.; de Rosales, R.T.M. Nuclear imaging of liposomal drug delivery systems: A critical review of radiolabelling methods and applications in nanomedicine. Adv. Drug Deliv. Rev. 2019, 143, 134–160. [Google Scholar] [CrossRef]
- Kane, S.M.; Padda, I.S.; Patel, P.; Davis, D.D. Technetium-99m. In StatPearls [Internet]; StatPearls: Treasure Island, FL, USA, 2025. [Google Scholar]
- Munir, M.; Setiawan, H.; Awaludin, R.; Kett, V.L. Aerosolised micro and nanoparticle: Formulation and delivery method for lung imaging. Clin. Transl. Imaging 2023, 11, 33–50. [Google Scholar] [CrossRef]
- Silva, M.C.; Silva, A.S.; Fernandez-Lodeiro, J. Supercritical CO2-assisted spray drying of strawberry-like gold-coated magnetite nanocomposites in chitosan powders for inhalation. Materials 2017, 10, 74. [Google Scholar] [CrossRef]
- Huynh, M.; Kempson, I.; Bezak, E.; Phillips, W. Predictive modeling of hypoxic head and neck cancers during fractionated radiotherapy with gold nanoparticle radiosensitization. Med. Phys. 2021, 48, 3120–3133. [Google Scholar] [CrossRef]
- Patchin, E.S.; Anderson, D.S.; Silva, R.M. Size-dependent deposition, translocation, and microglial activation of inhaled silver nanoparticles in the rodent nose and brain. Environ. Health Perspect. 2016, 124, 1870–1875. [Google Scholar] [CrossRef]
- Gomes, M.; Ramalho, M.J.; Loureiro, J.A.; Pereira, M.C. Advancing Brain Targeting: Cost-Effective Surface-Modified Nanoparticles for Faster Market Entry. Pharmaceutics 2025, 17, 661. [Google Scholar] [CrossRef]
- Kiwumulo, H.; Muwonge, H.; Lubwama, M. Iron oxide nanoparticles in leukemia: Design, diagnostic applications, and therapeutic strategies. J. Egypt. Natl. Canc. Inst. 2025, 37, 44. [Google Scholar]
- Lian, Y.; Wang, L.; Cao, J. Recent advances on the magnetic nanoparticle–based nanocomposites for magnetic induction hyperthermia of tumor: A short review. Adv. Compos. Hybrid Mater. 2021, 4, 925–937. [Google Scholar] [CrossRef]
- Burlec, A.F.; Corciova, A.; Boev, M.; Batir-Marin, D.; Mircea, C.; Cioanca, O.; Danila, G.; Danila, M.; Bucur, A.F.; Hancianu, M. Current Overview of Metal Nanoparticles’ Synthesis, Characterization, and Biomedical Applications, with a Focus on Silver and Gold Nanoparticles. Pharmaceuticals 2023, 16, 1410. [Google Scholar] [CrossRef]
- Grosges, T.; Barchiesi, D. Gold Nanoparticles as Photothermal Agent in Cancer Therapy: Theoretical Study of Concentration and Agglomeration Effects on Temperature. Appl. Sci. 2022, 12, 3315. [Google Scholar] [CrossRef]
- Takáč, P.; Michalková, R.; Čižmáriková, M.; Bedlovičová, Z.; Balážová, Ľ.; Takáčová, G. The Role of Silver Nanoparticles in the Diagnosis and Treatment of Cancer: Are There Any Perspectives for the Future? Life 2023, 13, 466. [Google Scholar] [CrossRef]
- Lee, K.; Lee, H.; Lee, K.W.; Park, T.G. Optical Imaging of Intracellular Reactive Oxygen Species for the Assessment of the Cytotoxicity of Nanoparticles. Biomaterials 2011, 32, 2556–2565. [Google Scholar] [CrossRef]
- Niwase, T.; Watanabe, Y.X.; Hirayama, Y.; Mukai, M.; Schury, P.; Andreyev, A.N.; Hashimoto, T.; Iimura, S.; Ishiyama, H.; Ito, Y.; et al. Discovery of New Isotope 241U and Systematic High-Precision Atomic Mass Measurements of Neutron-Rich Pa-Pu Nuclei Produced via Multinucleon Transfer Reactions. Phys. Rev. Lett. 2023, 130, 132502. [Google Scholar] [PubMed]
- Tarasov, O.B.; Gade, A.A.; Fukushima, K.; Hausmann, M.; Kwan, E.; Portillo, M.; Smith, M.; Ahn, D.S.; Bazin, D.; Chyzh, R.; et al. Observation of New Isotopes in the Fragmentation of Pt198 at FRIB. Phys. Rev. Lett. 2024, 132, 072501. [Google Scholar]
- Liu, X. Development and application of oncolytic viruses as the nemesis of tumor cells. Front. Microbiol. 2023, 14, 1188526. [Google Scholar] [CrossRef]
- Science-Based Medicine. Tag: Oncolytic Viruses. Available online: https://sciencebasedmedicine.org/tag/oncolytic-viruses/ (accessed on 30 May 2025).
- Milestones in Cancer Research and Discovery. National Cancer Institute (NIH). Available online: https://www.cancer.gov/research/progress/250-years-milestones (accessed on 18 June 2025).
- Downar, J. Cancer: It’s time to change the sign. CMAJ 2010, 182, 1588. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Radiation Type | Subatomic Particles | Mass × 10−27 kg | Energy | Tissue Penetration Range | Linear Energy Transfer, keV/µm | Relative Biological Effectiveness |
|---|---|---|---|---|---|---|
| Alpha, α * | 2 protons and 2 neutrons | 6.6 | Discrete; ~4–10 MeV | ~20–70 µm | ~50–300 | ~5 |
| Beta minus, β− ** | Electron | 0.00091 | Continuous; maximum of some hundred keV to some MeV | <1 mm | ~0.1–2 | ~1 |
| Auger *** | Electron | 0.00091 | <10 keV | <1 µm | ~4–26 | ~1 or higher |
| Radionuclide | ||||
|---|---|---|---|---|
| Isotope Type | T1/2 | Radioactive Decay (Electron Emission) * | Reactor (Therapy, Diagnosis) | Cyclotron (Diagnosis) |
| Medical Application | ||||
| Mo-99 | 65.94 h | β− | diagnosing diseases—e.g., heart failure, cancer—with Tc-99m ** | |
| Tc-99m | 6 h | 99mTc → 99 Tc + γ (88%) IT (Isomeric Transition): 99mTc → 99Tc+ + e− (12%) | - | diagnoses of peptide, small molecule, and cell labeling, perfusion imaging |
| In-111 | 2.8047 days | eA | - | diagnoses of brain and colon |
| Xe-133 | 5.243 days | eA | lung ventilation studies | - |
| I-123 | 13.27 h | eA | - | diagnoses of thyroid function |
| Ho-166 | 26.8 h | β− | therapy of liver tumors | - |
| Tl-201 | 72.912 h | ce | - | detecting cardiac conditions |
| Lu-177 | 6.65 days | β− | therapy of neuroendocrine tumors | - |
| Ru-82 | 1.3 min | β− | - | detecting cardiac conditions |
| Ra-223 | 11.4 days | α | - | treatments for prostate cancer spread to bones |
| F-18 | 109.77 min | β+ | - | visualization of tumors various localizations differential diagnostics |
| I-125 I-131 | 59.402 and 8.02070 days | eA + ce and ce | therapy of prostate cancer and thyroid conditions | - |
| Co-57 | 271.79 days | eA + ce | ||
| At-211 | 7.214 h | α | high degree of selectivity of therapeutic effect on thyroid tumor tissue (Isotope Separator On-Line Detector, ISOLDE) [32,33] | |
| Ga-67 | 3.2612 days | eA | - | diagnoses of infections and inflammation |
| Ga-68 | 67.71 min | β+ | - | one of the first radiopharmaceutical markers (1963); visualization of prostate cancer, neuroendocrine tumors and other diseases |
| Cu-62 | 9.67 min | β− + eA | ||
| Cu-64 | 12.70 h | β+; β− + eA | ||
| Sr-89 | 50.53 days | β− | pain management in bone cancer | - |
| Y-90 | 64.10 h | β− | therapy of liver cancer and rheumatic conditions | - |
| Ir-192 | 73.827 days | β− | therapy of cervical, prostate, lung, breast and skin cancer | - |
| Pb-212 | 10.64 h | β− and α | treatment of ovarian cancer and neuroendocrine tumors | - |
| Pb-203 | 51.873 h | eA | - | cancer marker |
| Radioactive Nanoparticles | Radioactive Decay | Standard Method of Diagnosis | Advantages | Disadvantages |
|---|---|---|---|---|
| Tracing agents | ||||
| Tc-99m | γ (140 keV) | single-photon emission computed tomography | Trace amount is required | Radiations, limited spatial resolution (~15 mm), no lung morphology image |
| Ga-67 | β+ (1899 keV) | positron emission tomography | Radiations, limited spatial resolution (~6 mm), no lung morphology image | |
| AuNPs | X-ray absorption | comprising computed tomography | Therapeutic effect (photothermal and radiosensitiser) | higher concentration is required compared to other CAs |
| AgNPs | Antimicrobial activity | Easy to be deposited in other tissues after pulmonary delivery | ||
| Contrast agents | ||||
| FeNPs | Shortening the T1 relaxation time of nearby water | magnetic resonance imaging (MRI) | Magnetic hyperthermia therapy | Inflammatory response and extrapulmonary toxicity were observed upon inhalation |
| GdNPs | Shortening the T1 and T2 relaxation time of nearby water | Radiosensitiser | Toxicity of free ions | |
| MnNPs | Shortening the T1 relaxation time of nearby water | Enhancement of photo- and chemotherapy | Neurotoxicity upon inhalation | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uspenskaya, E.V.; Safdari, A.; Antonov, D.V.; Valko, I.A.; Kazimova, I.V.; Timofeev, A.A.; Zubarev, R.A. The Novel Achievements in Oncological Metabolic Radio-Therapy: Isotope Technologies, Targeted Theranostics, Translational Oncology Research. Med. Sci. 2025, 13, 107. https://doi.org/10.3390/medsci13030107
Uspenskaya EV, Safdari A, Antonov DV, Valko IA, Kazimova IV, Timofeev AA, Zubarev RA. The Novel Achievements in Oncological Metabolic Radio-Therapy: Isotope Technologies, Targeted Theranostics, Translational Oncology Research. Medical Sciences. 2025; 13(3):107. https://doi.org/10.3390/medsci13030107
Chicago/Turabian StyleUspenskaya, Elena V., Ainaz Safdari, Denis V. Antonov, Iuliia A. Valko, Ilaha V. Kazimova, Aleksey A. Timofeev, and Roman A. Zubarev. 2025. "The Novel Achievements in Oncological Metabolic Radio-Therapy: Isotope Technologies, Targeted Theranostics, Translational Oncology Research" Medical Sciences 13, no. 3: 107. https://doi.org/10.3390/medsci13030107
APA StyleUspenskaya, E. V., Safdari, A., Antonov, D. V., Valko, I. A., Kazimova, I. V., Timofeev, A. A., & Zubarev, R. A. (2025). The Novel Achievements in Oncological Metabolic Radio-Therapy: Isotope Technologies, Targeted Theranostics, Translational Oncology Research. Medical Sciences, 13(3), 107. https://doi.org/10.3390/medsci13030107