A Reproductive Management Program for an Urban Population of Eastern Grey Kangaroos (Macropus giganteus)



Abstract
:Simple Summary
Abstract

1. Introduction
2. Methods
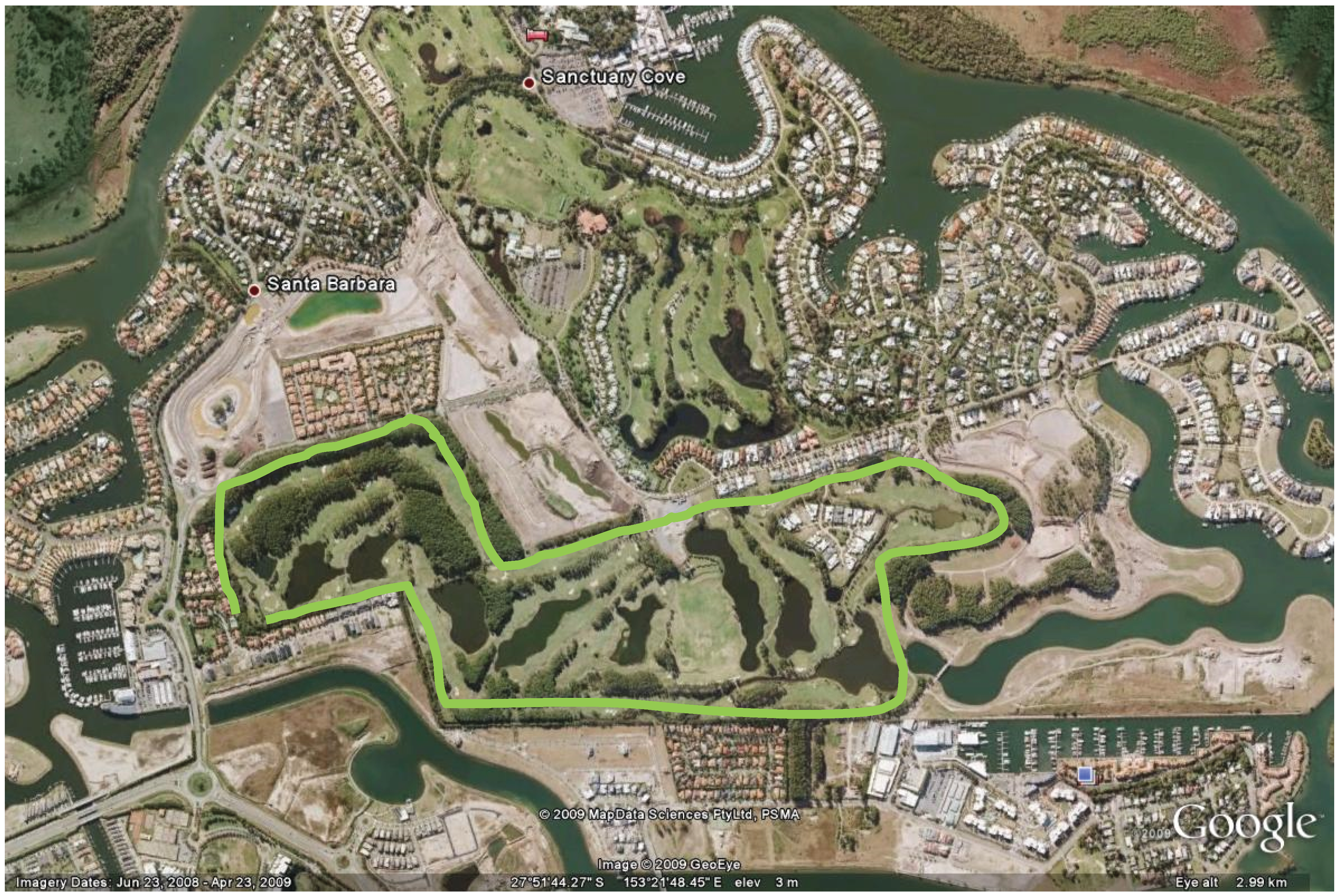
2.1. Study Site
2.2. The Eastern Grey Kangaroo Population
2.3. Census
2.4. Capture Restraint and Reproductive Control

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | Activity |
|---|---|
| March 2003 | Initial population estimate |
| August–September 2003 | Capture and tag all kangaroos. Suprelorin implantation of females more than 5 kg only |
| November 2005 | Population census |
| May–July 2007 | Capture and tag all kangaroos. Surgical sterilisation of all males more than 5 kg. Suprelorin implantation of all females above 5 kg |
| March–September 2007 | Behavioural observations |
| November 2008 | Population census |
| November 2009 | Population census |
2.5. Kangaroo Capture and Veterinary Procedures
2.5.1. Capture and Anaesthesia
- checked for pouch young (PY) and if found, the joeys were then sexed and weighed,
- patch of hair shaved and cleaned above the shoulders at the site for the hormonal implant,
- numbered red ear tag placed in the right ear and a red arm band on the right arm.
- intravenous injection of Alfaxan® to provide a deeper and more stable level of anaesthesia during surgery. Alfaxan® was also useful because of its shorter period of action than Zoletil® particularly when given intravenously,
- scrotum was shaved, cleaned and prepared for surgery,
- castrated males were also given an injection of lignocaine directly into the testes as a local anaesthetic,
- one numbered red ear tag was placed in their left ear,
- one numbered blue ear tag was placed in the right ear and blue arm band was placed on the right arm if the animal was being castrated,
- alternatively, one numbered green ear tag was placed in the right ear and a blue arm band on the left arm if the animal was being vasectomised,
- injection of engemycin, benacillin antibiotics to help prevent post-operative infection and an injection of metacam for additional for pain relief and a consequently less stressful recovery.
| Demographic | Procedure | Number of Kangaroos | |
| 2003 Program | 2007 Program | ||
| All kangaroos (incl. pouch young) | Estimated number present at time of management intervention 1 | 194 | 286 |
| All kangaroos | Kangaroos darted | 124 | 187 |
| Females > 5 kg | Deslorelin implant | 80 | 107 |
| Males > 50 kg | Vasectomy | 0 | 19 |
| Males < 50 kg | Vasectomy | 0 | 7 |
| Males > 50 kg | Orchidectomy | 0 | 5 |
| Males > 5 and < 50 kg | Orchidectomy | 0 | 52 |
2.5.2. Processing
2.6. Behavioural Observations
- (a)
- Focal animal sampling: one adult and one sub-adult male kangaroo were chosen at random during each observation session. While it would have been preferable to observe the same target kangaroos over the whole period of the study, this was not possible due to the difficulty in locating and identifying particular individuals across the 100 hectare site.
- (b)
- Continuous sampling: the mean frequencies of agonistic and sexual behaviours for all visible sub-adult and adult male and all mature female kangaroos in a mob were recorded. Mobs of at least 15 kangaroos were chosen for behavioural observations to increase the detection of interactive behaviours.
2.7. Statistical Analysis of Behavioural Observations
3. Results
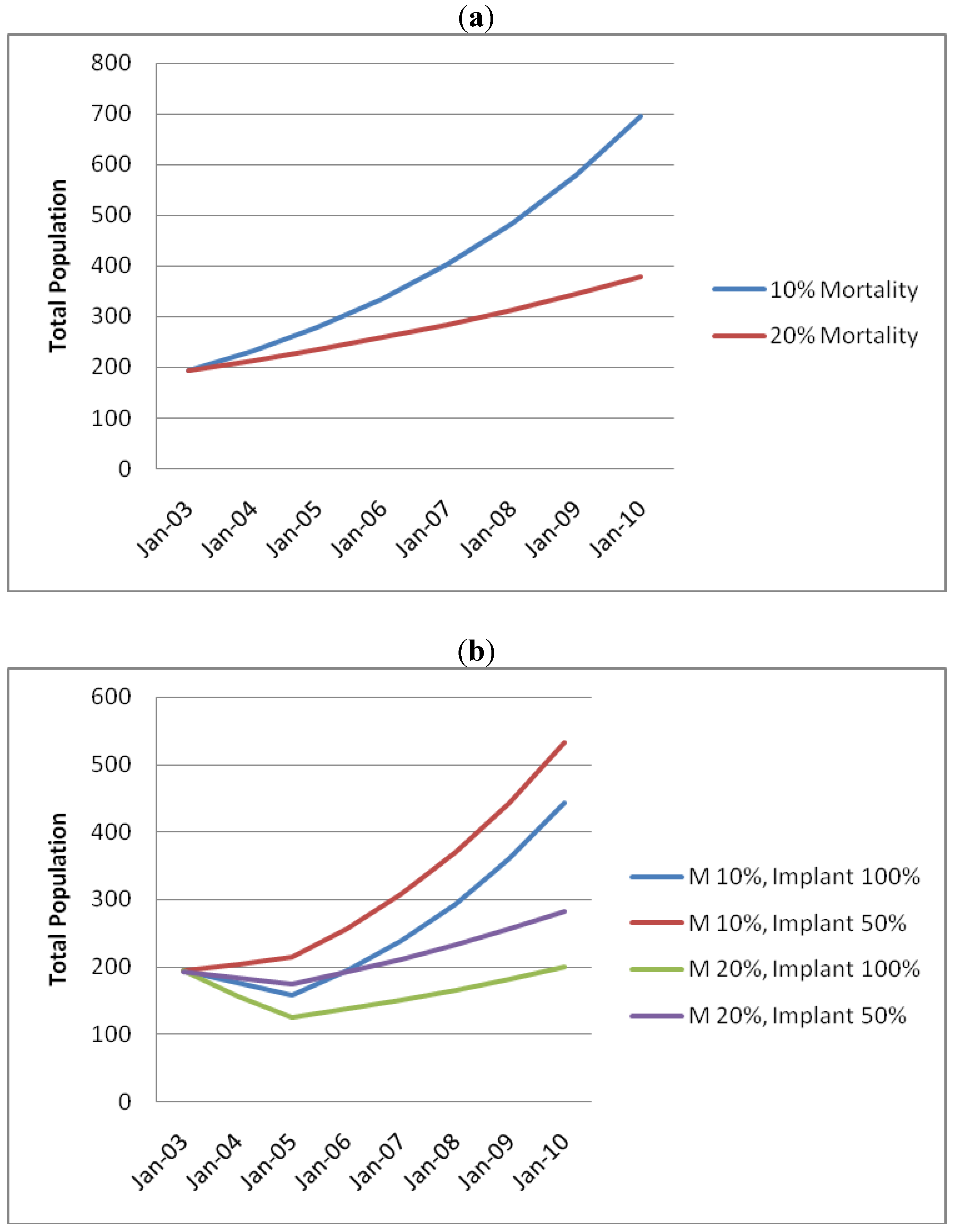
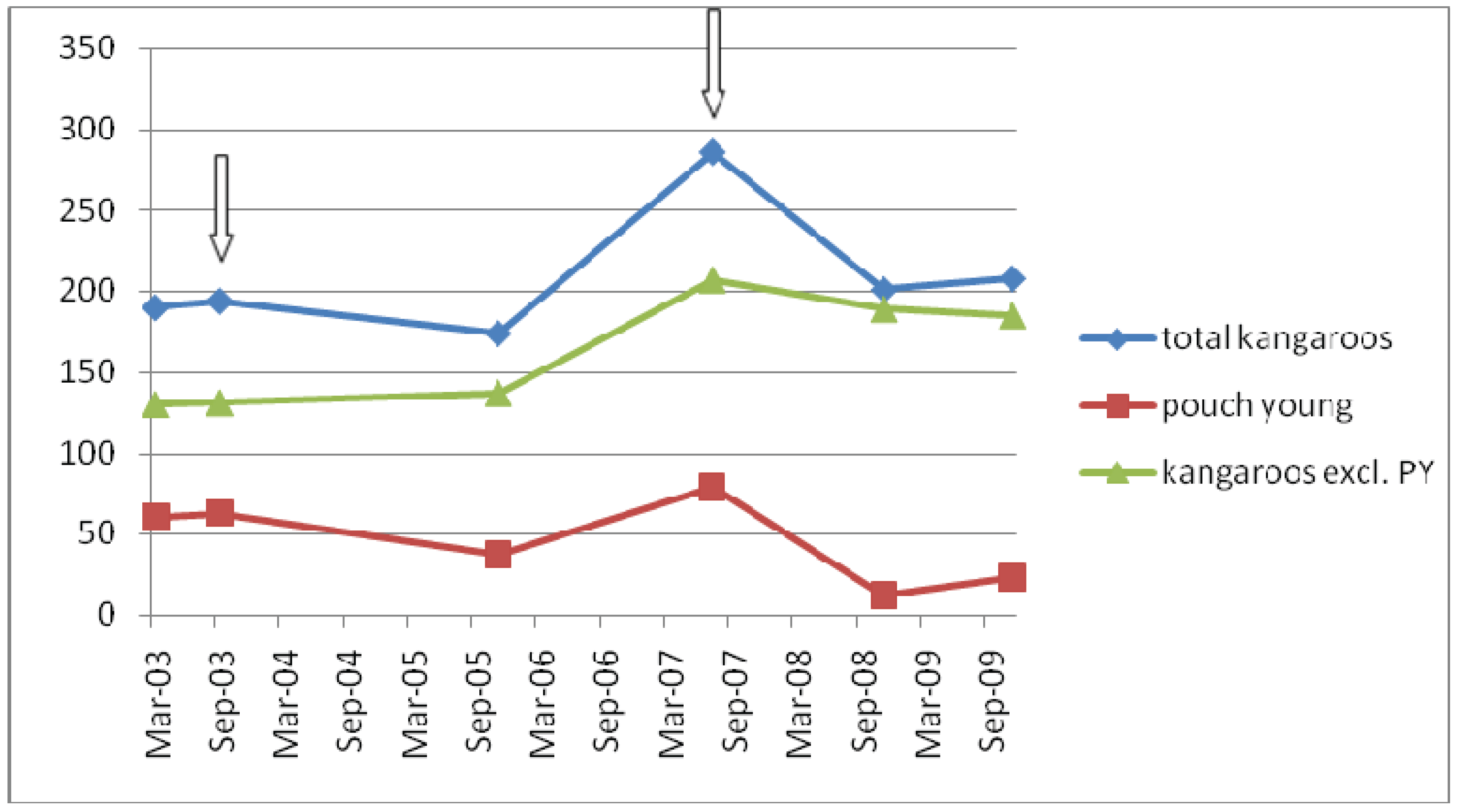
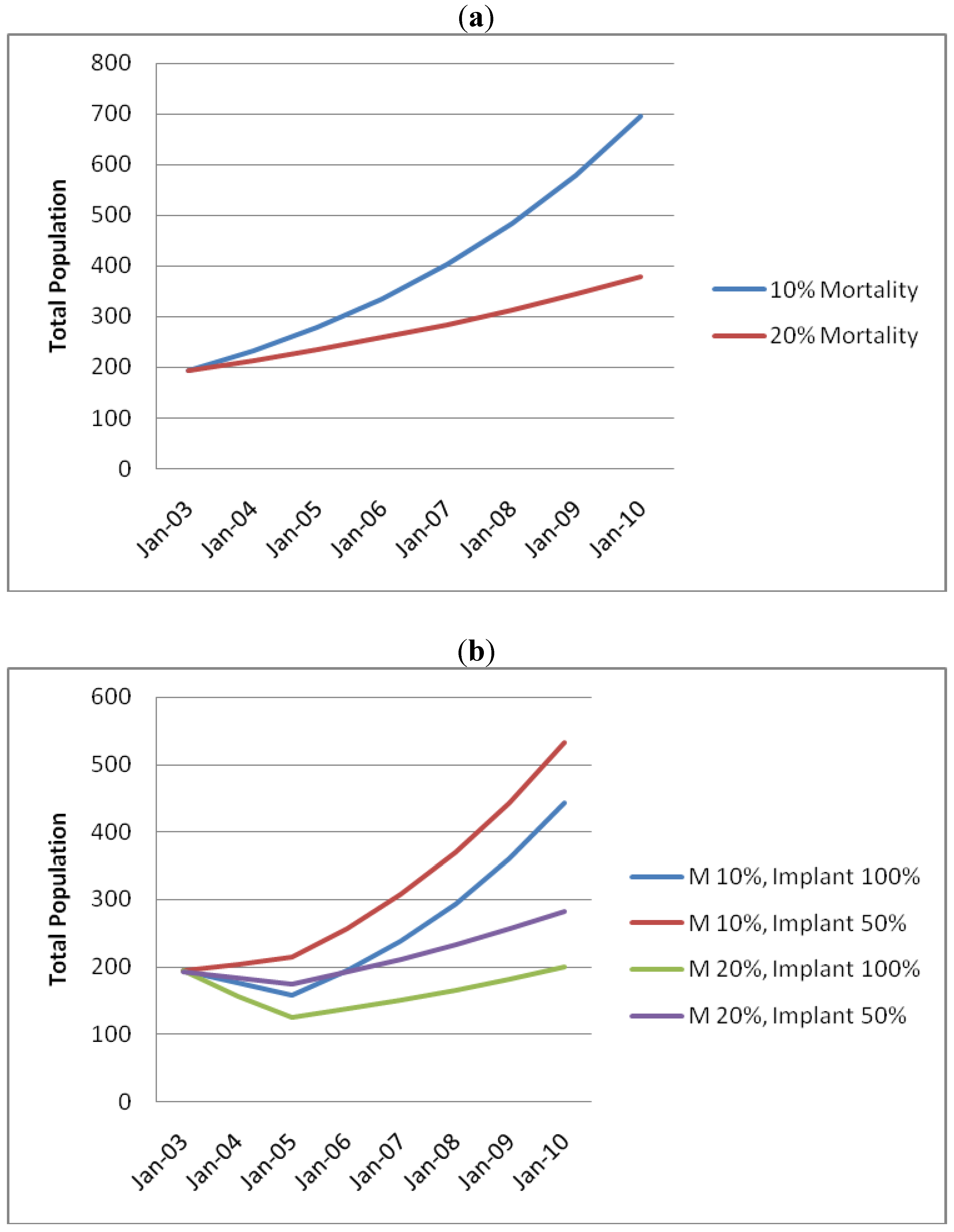
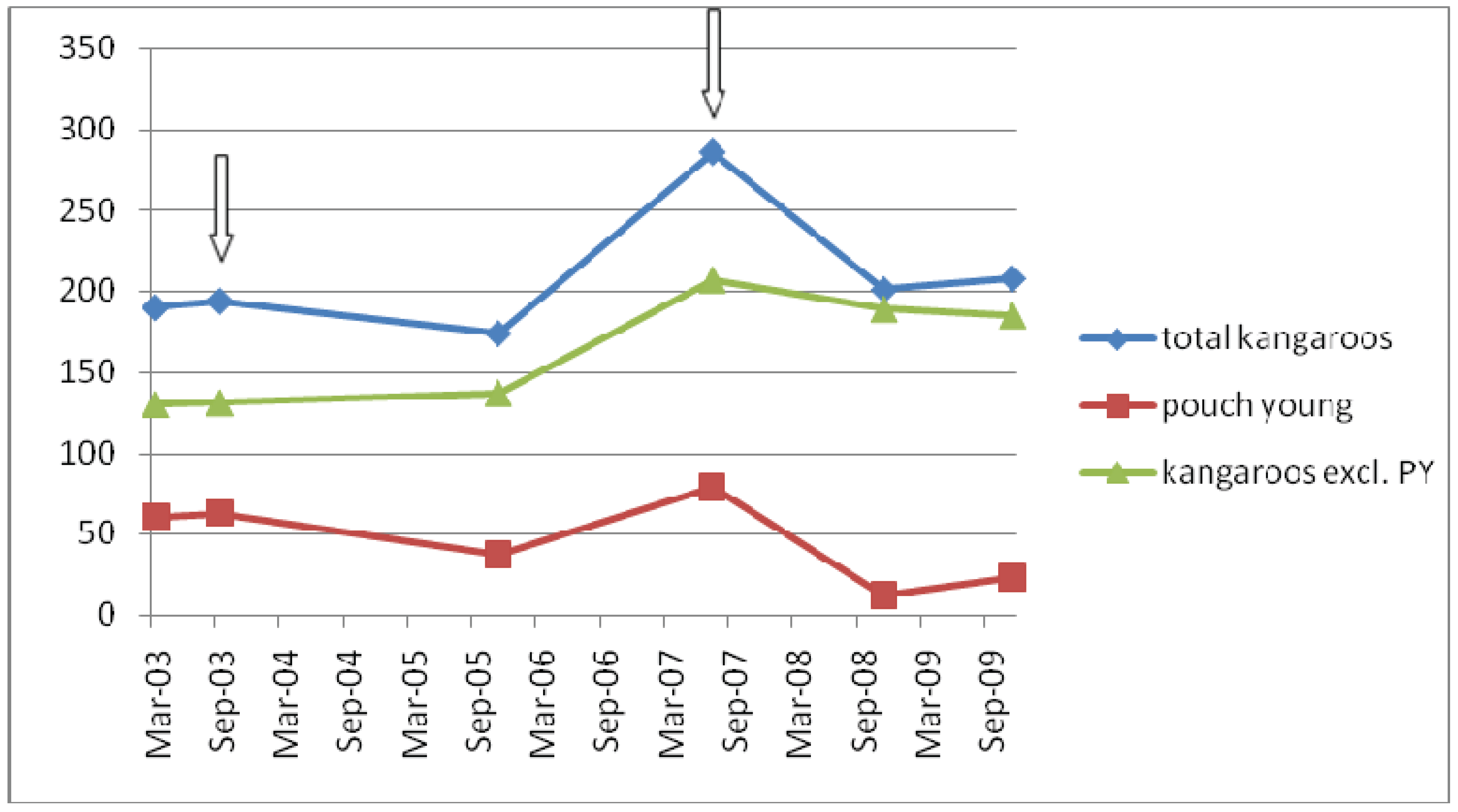
3.1. Reproduction and Demographic Effects
| Above 5 kg | Pouch young | TOTAL | ||
| Males | Females | Unspecified | ||
| Estimated animals present | 47 | 87 | 60 | 194 (100%) |
| Total captured | 44 | 80 | 57 | 181 (93%) |
| Estimated not captured | 3 | 7 | 3 | 13 (7%) |
| Females implanted with deslorelin | - | 80 | - | 80 (92% of all females) |
| Females with pouch young | - | 60 | - | 60 |
| Above 5 kg | Pouch Young | Total | ||
| Males | Females | Unspecified | ||
| Estimated animal present | 82 | 125 | 79 | 286 (100%) |
| Total captured | 72 | 115 | 79 | 266 (93%) |
| Estimated not captured | 10 | 10 | 0 | 20 (7%) |
| Male orchidectomy | 53 | - | - | 53 |
| Males vasectomy | 19 | - | - | 19 |
| Females implanted with deslorelin | - | 107 | - | 107 |
| Females with pouch young | - | 79 | - | 79 |
| Mortality | 11 | 2 | 13 | |
| Number with 2003 tags | 40 | 40 | ||
3.2. Behaviour
3.2.1. Agonistic Behaviours in Males
| Age Group | Behaviour | Treatment | P Value | |||||
|---|---|---|---|---|---|---|---|---|
| U* | V* | O* | U* vs. O* | U* vs. V* | O* vs. V* | |||
| Sub-adults | Fighting | Present | 10 | 0 | 3 | 0.08 | 0.001 | 0.20 |
| Absent | 18 | 29 | 25 | |||||
| Grunting | Present | 8 | 0 | 0 | 0.007 | 0.006 | N/A | |
| Absent | 20 | 29 | 28 | |||||
| Adults | Fighting | Present | 5 | 8 | 2 | 0.68 | 0.76 | 0.21 |
| Absent | 23 | 21 | 22 | |||||
| High walking | Present | 5 | 4 | 1 | 0.33 | 0.97 | 0.55 | |
| Absent | 23 | 25 | 23 | |||||
| Chest beating | Present | 3 | 6 | 1 | 0.76 | 0.66 | 0.21 | |
| Absent | 25 | 23 | 23 | |||||
| Grunting | Present | 8 | 7 | 1 | 0.06 | 0.97 | 0.12 | |
| Absent | 20 | 22 | 23 | |||||
| Age Group | Treatment | P Value | |||||
|---|---|---|---|---|---|---|---|
| U* | V* | O* | U* vs. O* | U* vs. V* | O* vs. V* | ||
| Sub-adults | Present | 6 | 0 | 0 | 0.01 | 0.01 | 0.99 |
| Absent | 4 | 10 | 10 | ||||
| Adults | Present | 4 | 2 | 1 | 0.32 | 0.69 | 0,90 |
| Absent | 6 | 8 | 9 | ||||
| Age Group | Behaviour | Treatment | P Value | |||||
|---|---|---|---|---|---|---|---|---|
| U* | V* | O* | U* vs. O* | U* vs. V* | O* vs. V* | |||
| Sub-adults | Following & sniffing | Present | 8 | 0 | 1 | 0.03 | 0.006 | 0.664 |
| Absent | 20 | 29 | 27 | |||||
| Erection | Present | 10 | 0 | 1 | 0.007 | 0.001 | 0.68 | |
| Absent | 18 | 28 | 27 | |||||
| Adults | Following & sniffing | Present | 26 | 21 | 6 | <0.001 | 0.122 | 0.002 |
| Absent | 2 | 8 | 18 | |||||
| Erection | Present | 18 | 19 | 4 | 0.002 | 0.99 | 0.001 | |
| Absent | 10 | 10 | 20 | |||||
3.2.2. Sexual Behaviours in Males
3.2.3. Female Behaviour
3.2.4. Animal Welfare Impact of Management Interventions
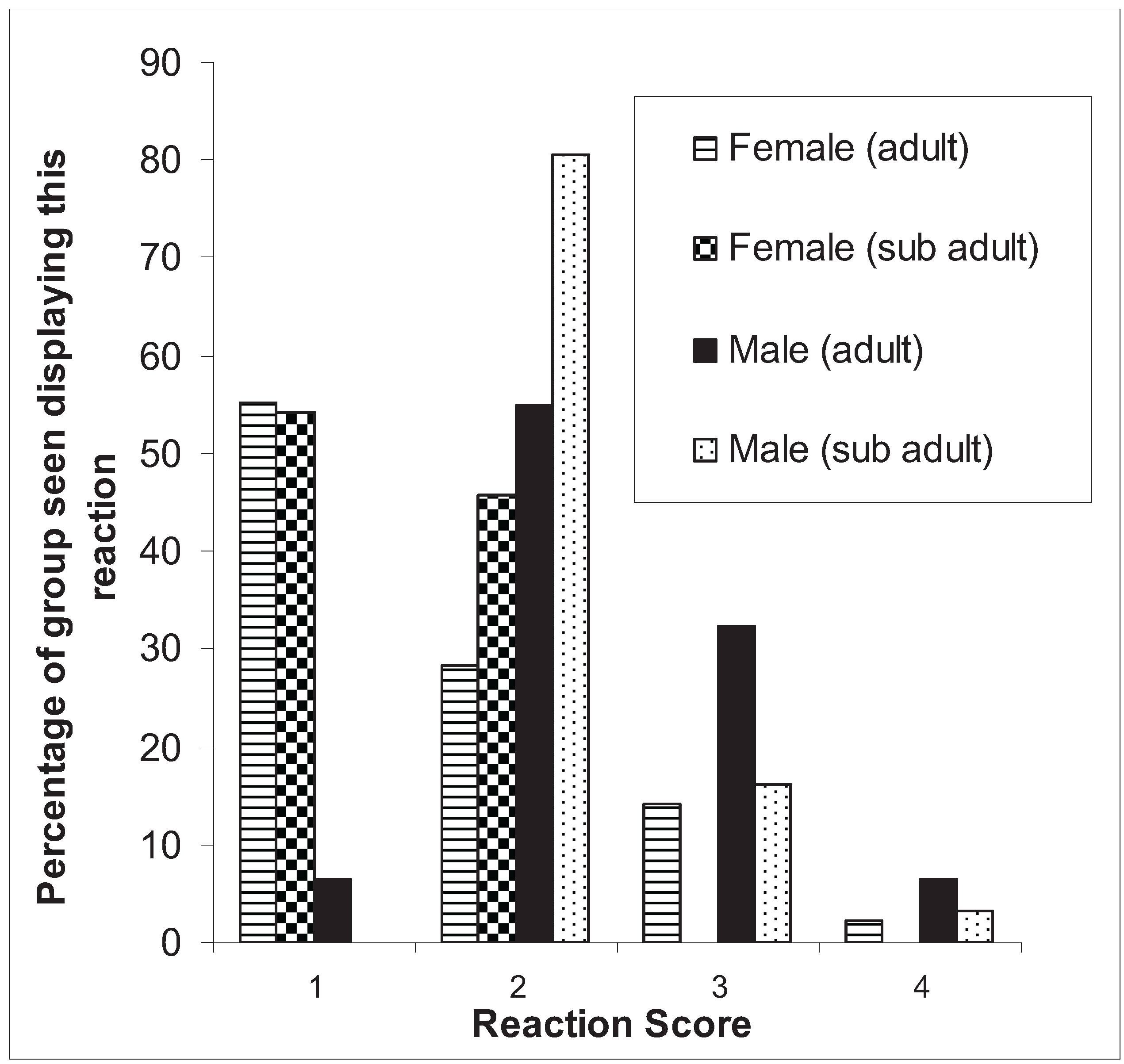
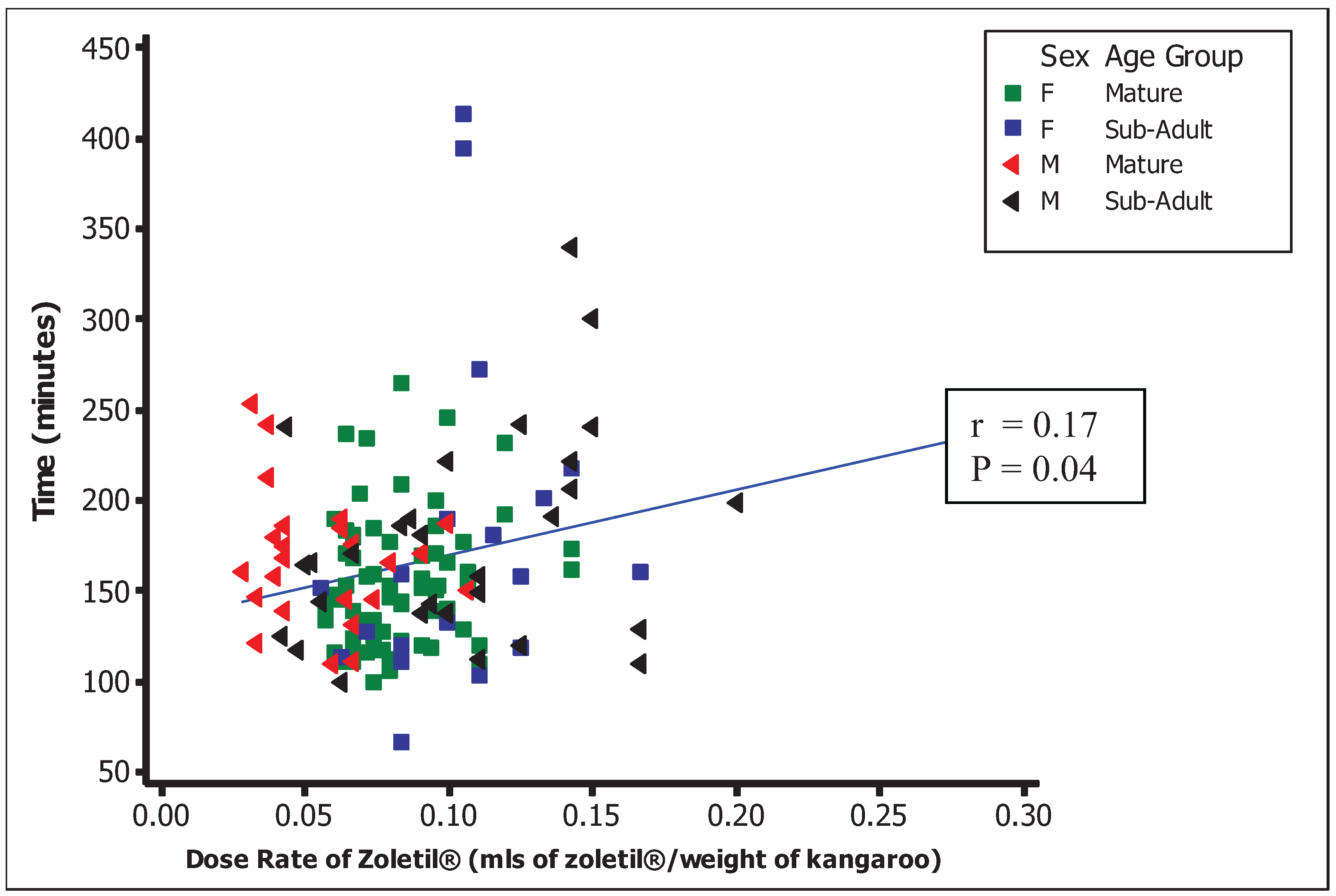
3.2.4.1. Response to Darting

3.2.4.2. Mortality
| Cause of death/reason for euthanasia | 2003 (19 mortalities) | 2007 (13 mortalities) | % of all deaths | ||
|---|---|---|---|---|---|
| Died | Euthanased | Died | Euthanased | ||
| Dart-related injury/fracture | 0 | 5 | 0 | 1 | 19% |
| Trauma occurring during anaesthetic induction | 0 | 0 | 0 | 2 | 6% |
| Hyperthermia/myopathy | 5 | 0 | 1 | 0 | 19% |
| Death after anaesthetic recovery (unspecified cause) | 4 | 0 | 3 | 0 | 22% |
| Anaesthetic death | 0 | 0 | 1 | 0 | 3% |
| Drowning/near drowning | 0 | 0 | 1 | 2 | 9% |
| Predation | 2 | 0 | 0 | 0 | 6% |
| Untreatable disease | 0 | 1 | 0 | 0 | 3% |
| Joey death (unviable orphan) | 2 | 0 | 1 | 1 | 13% |
| Totals | 13 | 6 | 7 | 6 | 100% |
3.2.4.3. Non-Lethal Injuries
3.2.4.4. Financial Costs and Resource Effort
4. Discussion
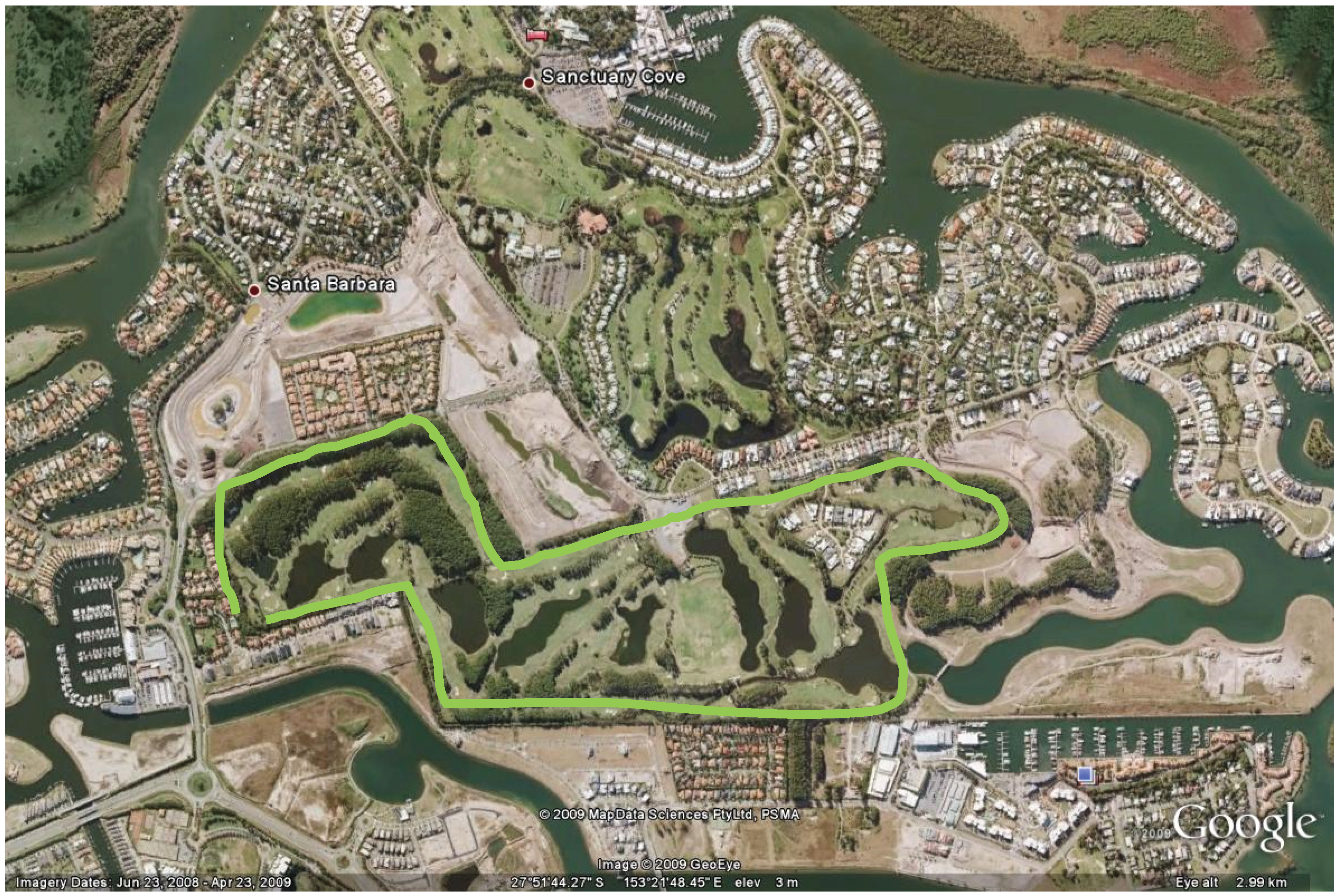
4.1. Efficacy of Population Management Program
4.2. Animal Welfare Considerations
- (1)
- Injury caused by the dart
- (2)
- Injury or misadventure that occurs during induction or recovery from anaesthesia
- (3)
- Anaesthesia and other veterinary procedures
- (4)
- Predation as a result of impairment of appropriate flight or defence responses [18]

4.2.1. Animal Reaction to Darting
4.2.2. Short Term Behavioural Responses of Kangaroos to Reproductive Procedures
5. Conclusions
Acknowledgements and Approvals
References
- Archer, M.; Grigg, G.; Flannery, T. The Kangaroo; Kevin Weldon: McMahons Points, NSW, Australia, 1985. [Google Scholar]
- Dawson, T.J. Kangaroos, Biology of the Largest Marsupials; University of New South Wales Press Ltd.: Sydney, Australia, 1995. [Google Scholar]
- Tribe, A. Managing Kangaroos as a Sustainable Resource. In Proceedings of Annual Conference of the Australian Veterinary Association, Sydney, Australia, 12–17 May 1991; p. 66.
- Adderton Herbert, C. Long acting contraceptives: A new tool to manage overabundant kangaroo populations in nature reserves and urban areas. Aust. Mammal. 2004, 26, 67–74. [Google Scholar]
- Herbert, C.A.; Trigg, T.E.; Cooper, D.W. Fertility control in female eastern grey kangaroos using the GnRH agonist deslorelin. 1. Effects on reproduction. Wildl. Res. 2006, 33, 41–46. [Google Scholar]
- Coulson, G.; Nave, C.D.; Shaw, D.; Renfree, M.B. Long-term efficacy of levonorgestrel implants for fertility control of eastern grey kangaroos (Macropus giganteus). Wildl. Res. 2008, 35, 520–524. [Google Scholar]
- Kitchener, A.L.; Harman, A.; Kay, D.J.; McCartney, C.A.; Mate, K.E.; Rodger, J.C. Immunocontraception of eastern grey kangaroos (Macropus giganteus) with recombinant brushtail possum (Trichosurus vulpecula) ZP3 protein. J. Rep. Immunol. 2009, 79, 156–162. [Google Scholar]
- Nave, C.D.; Coulson, G.; Poiani, A.; Shaw, G.; Renfree, M.B. Fertility control in the eastern grey kangaroo using levonorgestrel implants. J. Wildl. Manag. 2002, 66, 470–477. [Google Scholar]
- Brooks, R.P.; Fleming, M.W.; Kennelly, J.J. Beaver. Colony response to fertility control: evaluating a concept. J. Wildl. Manag. 1980, 44, 568–575. [Google Scholar] [CrossRef]
- Davidson, J.M. Characteristics of sex behaviour in male rats following castration. Anim. Behav. 1966, 14, 266–272. [Google Scholar]
- Ramsey, D. Effects of fertility control on behavior and disease transmission in brushtail Possums. J. Wildl. Manag. 2007, 71, 109–116. [Google Scholar] [CrossRef]
- Zamaratskaia, G.; Rydhmer, L.; Andersson, H.K.; Chen, G.; Lowagie, S.; Andersson, K.; Lundstrom, K. Long-term effect of vaccination against gonadotropin-releasing hormone, using Improvac (TM), on hormonal profile and behaviour of male pigs. Anim. Rep. Sci. 2008, 108, 37–48. [Google Scholar] [CrossRef]
- Asquith, K.L.; Kitchener, A.L.; Kaya, D.J. Immunisation of the male tammar wallaby (Macropus eugenii) with spermatozoa elicits epididymal antigen-specific antibody secretion and compromised fertilisation rate. J. Rep. Immunol. 2006, 69, 127–147. [Google Scholar]
- Kitchener, A.L.; Edds, L.M.; Molinia, F.C.; Kay, D.J. Porcine Zonae Pellucidae Immunization of Tammar Wallabies (Macropus eugenii): Fertility and Immune Responses. Reprod. Fertil. Dev. 2002, 14, 215–223. [Google Scholar] [CrossRef]
- Coulson, G. Management of overabundant macropods—Are there conservation benefits? In Managing Marsupial Abundance for Conservation Benefits; Austin, A., Ed.; Cooperative Research Centre for the Conservation and Management of Marsupials: Sydney, Australia, 1998. [Google Scholar]
- Vogelnest, L.; Portas, T. Macropods. In Medicine of Australian Mammals; Vogelnest, L., Woods, R., Eds.; CSIRO Publishing: Collingwood, Australia, 2008; pp. 133–225. [Google Scholar]
- Coulson, G. Repertoires of social behaviour in captive and free-ranging grey kangaroos, Macropus giganteus and Macropus fuliginosus (Marsupialia: Macropodidae). J. Zool. 1997, 242, 119–130. [Google Scholar]
- Coulson, G. Repertoires of social behaviour in the Macropodoidea. In Kangaroos, Wallabies and Rat-Kangaroos; Grigg, G.C., Jarman, P.J., Hume, I.D., Eds.; Surrey Beatty & Sons: Sydney, Australia, 1989; pp. 457–473. [Google Scholar]
- Mcdonald, I.; University of Queensland, Gatton, Australia. Personal observation, 2008.
- Vogelnest, L. Chemical Restraint of Australian Native Fauna. In Wildlife in Australia: Healthcare and Management; Proceedings 327; Post Graduate Foundation in Veterinary Science, University of Sydney: Sydney, Australia, 1999; pp. 149–187. [Google Scholar]
- Arnold, G.W.; Steven, D.; Weeldenburg, J.; Brown, O.E. The use of alpha-chloralose for the repeated capture of western grey kangaroos, Macropus-fuliginosus. Austr. Wildl. Res. 1986, 13, 527–533. [Google Scholar]
- Mauthe von Degerfeld, M. Personal experiences in the use of Zoletil for anaesthesia of the red necked wallaby (Macropus rufogriseus). Vet. Res. Comm. 2005, 29, 297–300. [Google Scholar]
- Pitt, J.; Lariviere, S.; Messier, F. Efficacy of Zoletil for field immobilization of raccoons. Wildl. Soc. Bull. 2006, 34, 1045–1048. [Google Scholar]
- Manharth, A.; Harris-Gerber, L. Surgical castration and the effect on aggression in rock hyrax (Procavia capensis). J. Zoo Wildl. Med. 2002, 33, 80–82. [Google Scholar]
- Ganslosser, U. Agonistic behavior in Macropodoids—A Review. In Kangaroos, Wallabies and Rat Kangaroos; Grigg, G., Jarman, P., Hume, I., Eds.; Surrey, Beatty and Sons: Sydney, Australia, 1989; Volume 2. [Google Scholar]
- Hohn, M.; Kronschnabel, M.; Gansloßer, U. Similarities and differences in activites and agonistic behavior of male eastern grey kangaroos (Macropus giganteus) in captivity and the wild. Zoo Biol. 2000, 19, 529–539. [Google Scholar]
- Catling, P.C.; Sutherland, R.L. Effect of gonadectomy, season and the presence of female tammar wallabies (Macropus Eugenii) on concentration of testosterone, luteinizing hormone and follicle stimulating hormone in the plasma of male tammar wallabies. J. Endocrinol. 1980, 86, 25–33. [Google Scholar]
- Staker, L. The Complete Guide to the Care of Macropods: A Comprehensive Guide to the Handrearing, Rehabilitation and Captive Management of Kangaroo Species; Matilda Publishing: Townsville, Australia, 2006. [Google Scholar]
- Bolitho, E.; Coulson, G.; Bricknell, S. Body Size, Dominance and Mating Success in Grey Kangaroos. In Proceedings of the 6th International Behaviour Ecology Congress, Canberra, Australia, 29 September–4 October 1996.
- Woodward, R.; Herbertstein, M.E.; Herbert, C.A. Fertility control in female eastern grey kangaroos using the GnRH agonist deslorelin. 2. Effects on behaviour. Wildlife Res. 2006, 33, 47–55. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Tribe, A.; Hanger, J.; McDonald, I.J.; Loader, J.; Nottidge, B.J.; McKee, J.J.; Phillips, C.J.C. A Reproductive Management Program for an Urban Population of Eastern Grey Kangaroos (Macropus giganteus). Animals 2014, 4, 562-582. https://doi.org/10.3390/ani4030562
Tribe A, Hanger J, McDonald IJ, Loader J, Nottidge BJ, McKee JJ, Phillips CJC. A Reproductive Management Program for an Urban Population of Eastern Grey Kangaroos (Macropus giganteus). Animals. 2014; 4(3):562-582. https://doi.org/10.3390/ani4030562
Chicago/Turabian StyleTribe, Andrew, Jon Hanger, Ian J. McDonald, Jo Loader, Ben J. Nottidge, Jeff J. McKee, and Clive J. C. Phillips. 2014. "A Reproductive Management Program for an Urban Population of Eastern Grey Kangaroos (Macropus giganteus)" Animals 4, no. 3: 562-582. https://doi.org/10.3390/ani4030562
APA StyleTribe, A., Hanger, J., McDonald, I. J., Loader, J., Nottidge, B. J., McKee, J. J., & Phillips, C. J. C. (2014). A Reproductive Management Program for an Urban Population of Eastern Grey Kangaroos (Macropus giganteus). Animals, 4(3), 562-582. https://doi.org/10.3390/ani4030562