
Clinical Use of a 180-Day Implantable Glucose Monitoring System in Dogs with Diabetes Mellitus: A Case Series

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Clinical Cases
2.1. Case Descriptions
2.1.1. Dog 1
2.1.2. Dog 2
2.1.3. Dog 3
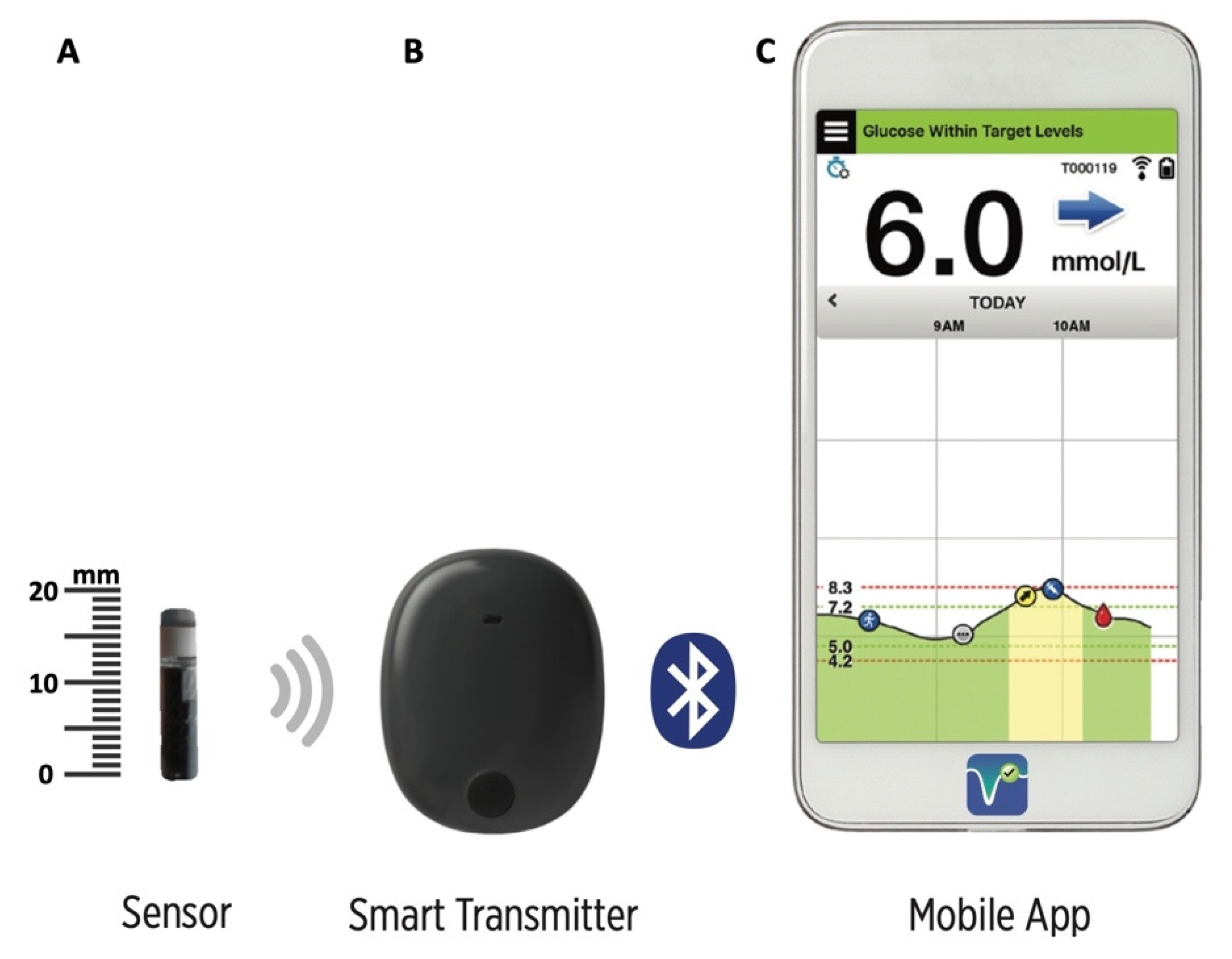
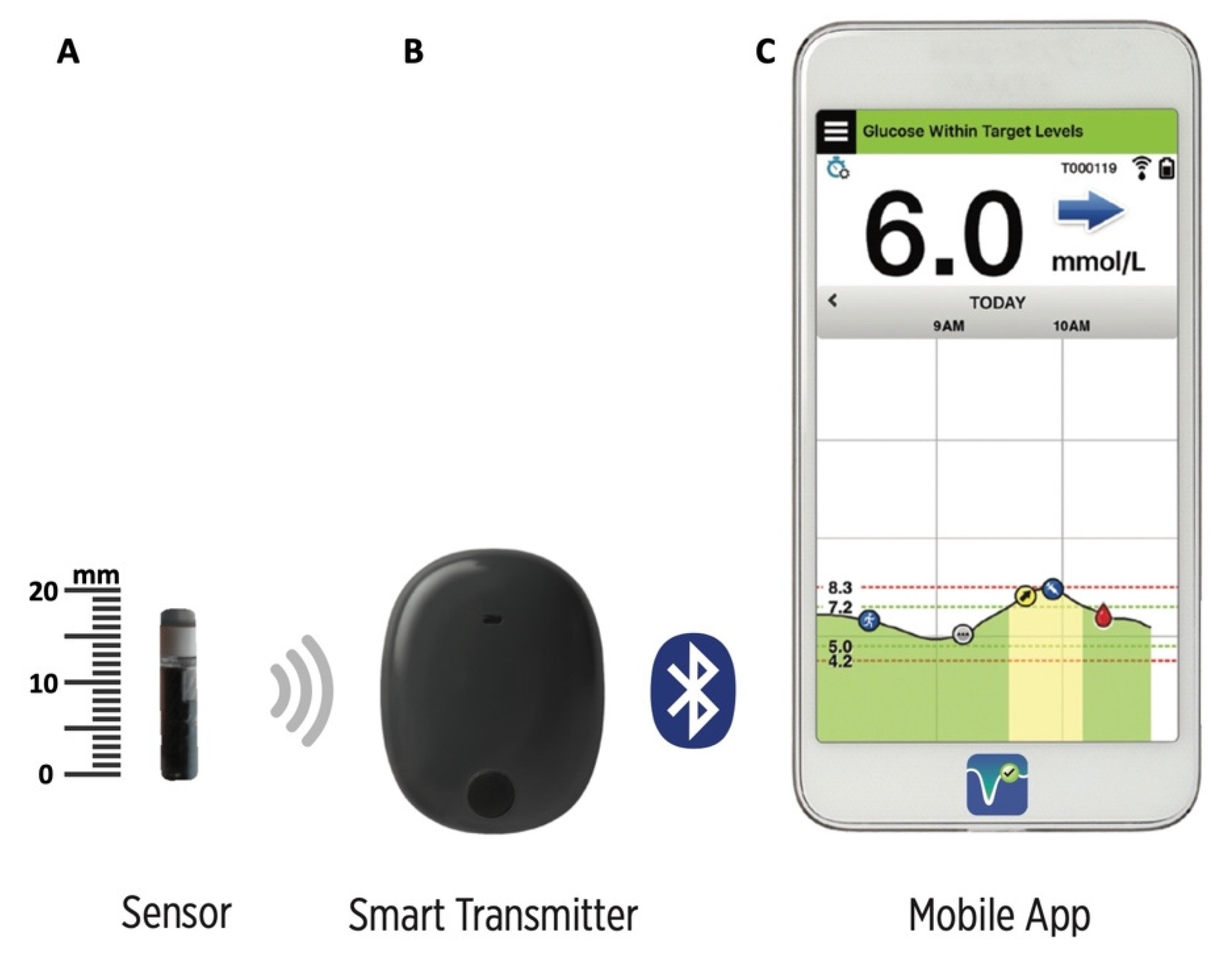
2.2. The Eversense Long-Term Implantable CGMS
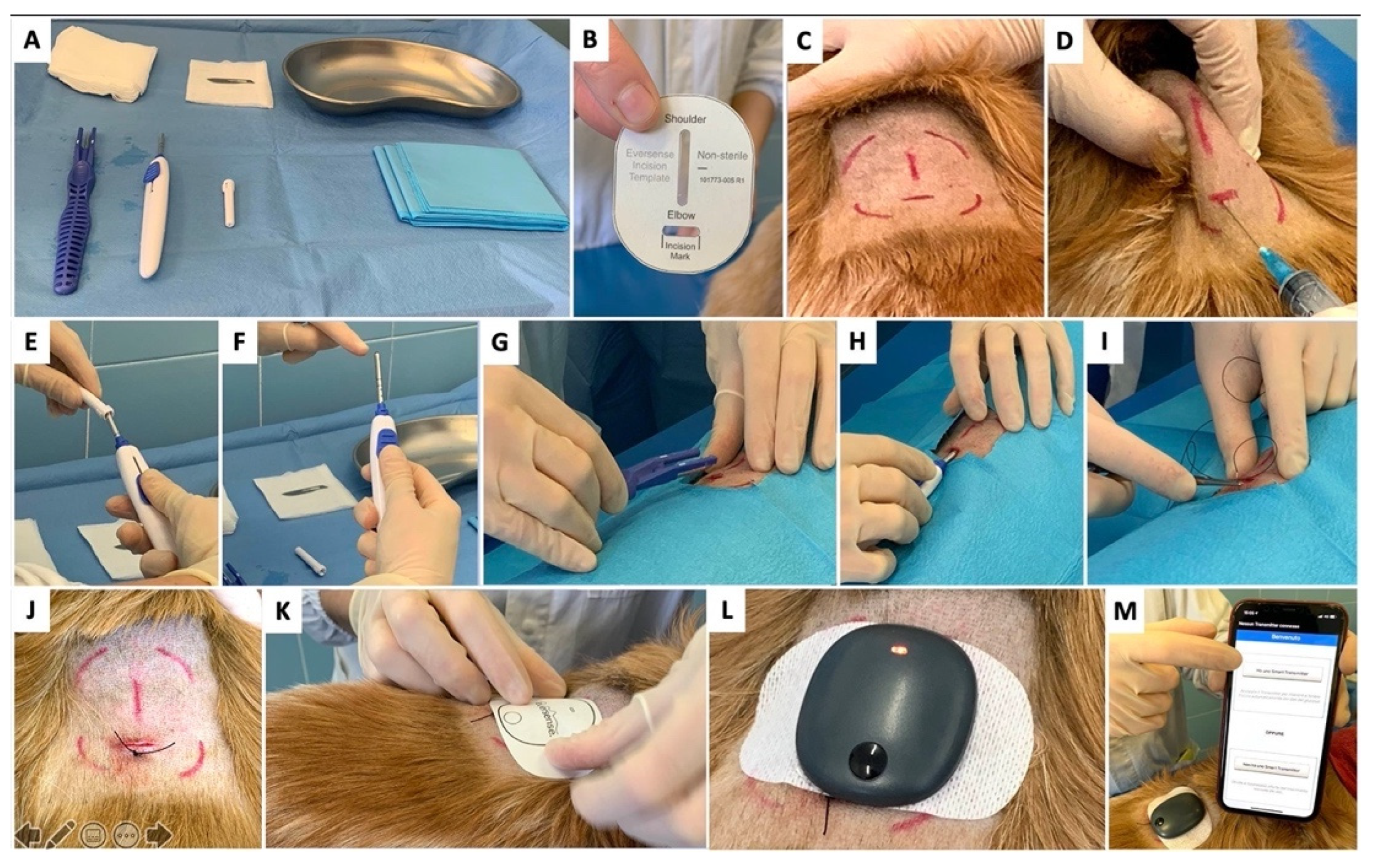
2.3. Sensor Insertion and Follow-Up Assessments
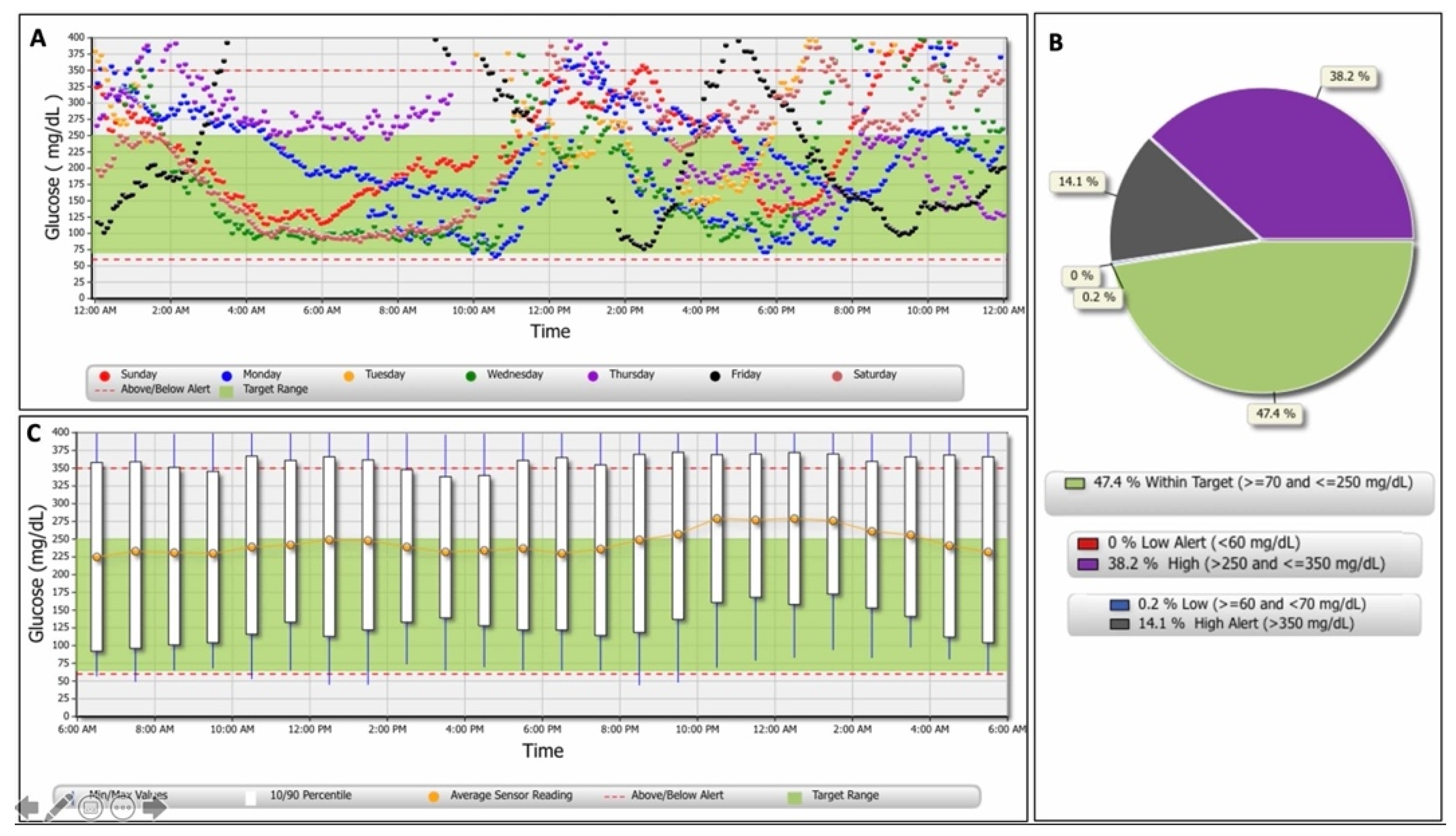
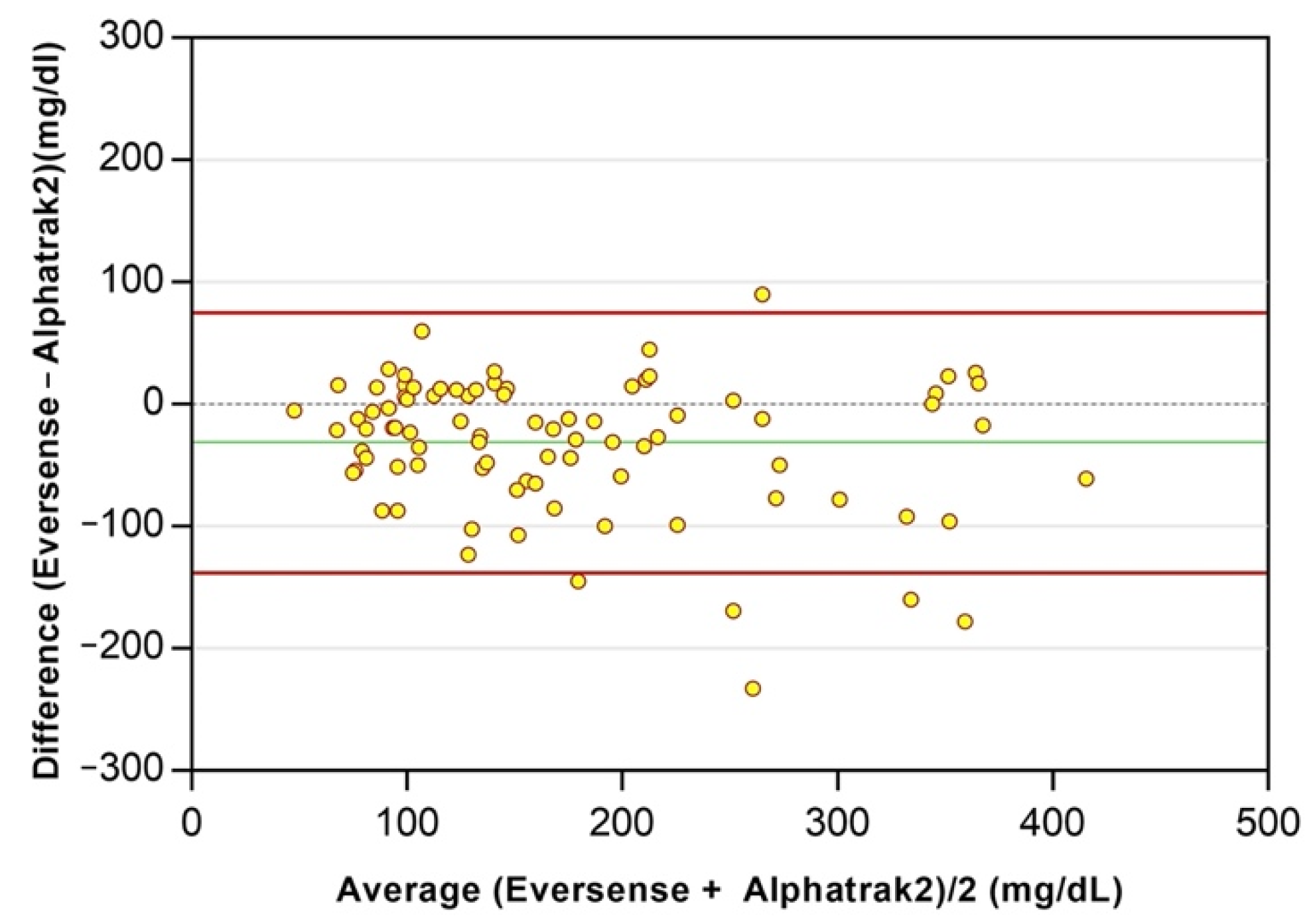
2.4. Glucose Data Analysis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pickup, J.C.; Freeman, S.C.; Sutton, A.J. Glycaemic control in type 1 diabetes during real time continuous glucose monitoring compared with self monitoring of blood glucose: Meta-analysis of randomised controlled trials using individual patient data. BMJ 2011, 343, d3805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolinder, J.; Antuna, R.; Geelhoed-Duijvestijn, P.; Kröger, J.; Weitgasser, R. Novel glucose sensing technology and hypoglycaemia in type 1 diabetes: A multi-centre, non-masked, randomised controlled trial. Lancet 2016, 388, 2254–2263. [Google Scholar] [CrossRef]
- Beck, R.W.; Riddlesworth, T.; Ruedy, K.; Ahmann, A.; Bergenstal, R.; Haller, S.; Kollman, C.; Kruger, D.; McGill, J.B.; Polonsky, W.; et al. Effect of continuous glucose monitoring on glycemic control in adults with type 1 diabetes using insulin injections: The DIAMOND randomized clinical trial. JAMA 2017, 317, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Carlson, A.L.; Mullen, D.M.; Bergenstal, R.M. Clinical use of continuous glucose monitoring in adults with type 2 diabetes. Diabetes Technol. Ther. 2017, 19, S4–S11. [Google Scholar] [CrossRef] [Green Version]
- Lind, M.; Polonsky, W.; Hirsch, I.B.; Heise, T.; Bolinder, J.; Dahlqvist, S.; Schwarz, E.; Ólafsdóttir, A.F.; Frid, A.; Wedel, H.; et al. Continuous glucose monitoring vs conventional therapy for glycemic control in adults with type 1 diabetes treated with multiple daily insulin injections: The GOLD randomized clinical trial. JAMA 2017, 417, 379–387. [Google Scholar] [CrossRef]
- Rodbard, D. Continuous glucose monitoring: A review of recent studies demonstrating improved glycemic outcomes. Diabetes Technol. Ther. 2017, 19, S25–S37. [Google Scholar] [CrossRef]
- Foster, N.C.; Beck, R.W.; Miller, K.M.; Clements, M.A.; Rickels, M.R.; DiMeglio, L.A.; Maahs, D.M.; Tamborlane, W.V.; Bergenstal, R.; Smith, E.; et al. State of type 1 diabetes management and outcomes from the T1D exchange in 2016–2018. Diabetes Technol. Ther. 2019, 21, 66–72. [Google Scholar] [CrossRef]
- Calhoun, P.; Price, D.; Beck, R.W. Glycemic Improvement Using Continuous Glucose Monitoring by Baseline Time in Range: Subgroup Analyses from the DIAMOND Type 1 Diabetes Study. Diabetes Technol. Ther. 2021, 23, 230–233. [Google Scholar] [CrossRef]
- Wiedmeyer, C.E.; Declue, A.E. Continuous glucose monitoring in dogs and cats. J. Vet. Intern. Med. 2008, 22, 2–8. [Google Scholar] [CrossRef]
- Moretti, S.; Tschuor, F.; Osto, M.; Franchini, M.; Wichert, B.; Ackermann, M.; Lutz, T.A.; Reusch, C.E.; Zini, E. Evaluation of a novel real-time continuous glucose-monitoring system for use in cats. J. Vet. Intern. Med. 2010, 24, 120–126. [Google Scholar] [CrossRef]
- Affenzeller, N.; Thalhammer, J.G.; Willmann, M. Home-Based Subcutaneous Continuous Glucose Monitoring in 10 Diabetic Dogs. Vet. Rec. 2011, 169, 206. [Google Scholar] [CrossRef] [PubMed]
- Mori, A.; Kurishima, M.; Oda, H.; Saeki, K.; Arai, T.; Sako, T. Comparison of glucose fluctuations between day- and night-time measured using a continuous glucose monitoring system in diabetic dogs. J. Vet. Med. Sci. 2013, 75, 113–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surman, S.; Fleeman, L. Continuos glucose monitoring in small animals. Vet. Clin. N. Am. Small Anim. Pract. 2013, 43, 381–406. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R.W. Canine Diabetes Mellitus. In Canine and Feline Endocrinology, 4th ed.; Feldman, E.C., Nelson, R.W., Reusch, C.E., Scott-Moncrieff, J.C., Behrend, E.N., Eds.; Elsevier Saunders: St Louis, MO, USA, 2015; pp. 213–257. [Google Scholar]
- Corradini, S.; Pilosio, B.; Dondi, F.; Linari, G.; Testa, S.; Brugnoli, F.; Gianella, P.; Pietra, M.; Fracassi, F. Accuracy of a flash glucose monitoring system in diabetic dogs. J. Vet. Intern. Med. 2016, 30, 983–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malerba, E.; Cattani, C.; Del Baldo, F.; Carotenuto, G.; Corradini, S.; Golinelli, S.; Drudi, I.; Fracassi, F. Accuracy of a flash glucose monitoring system in dogs with diabetic ketoacidosis. J. Vet. Intern. Med. 2020, 34, 83–91. [Google Scholar] [CrossRef] [Green Version]
- Deiting, V.; Mischke, R. Use of the “FreeStyle Libre” glucose monitoring system in diabetic cats. Res. Vet. Sci. 2021, 135, 253–259. [Google Scholar] [CrossRef]
- Del Baldo, F.; Fracassi, F.; Pires, J.; Tardo, A.M.; Malerba, E.; Manassero, E.; Gilor, C. Accuracy of a flash glucose monitoring system in cats and determination of the time lag between blood glucose and interstitial glucose concentrations. J. Vet. Intern. Med. 2021, 35, 1279–1287. [Google Scholar] [CrossRef]
- Shea, E.K.; Hess, R.S. Validation of a flash glucose monitoring system in outpatient diabetic cats. J. Vet. Intern. Med. 2021, 35, 1703–1712. [Google Scholar] [CrossRef]
- Davison, L.J.; Slater, L.A.; Herrtage, M.E.; Church, D.B.; Judge, S.; Ristic, J.M.E.; Catchpole, B. Evaluation of a continuous glucose monitoring system in diabetic dogs. J. Small Anim. Pract. 2003, 44, 435–442. [Google Scholar] [CrossRef]
- Wiedmeyer, C.E.; Johnson, P.J.; Cohn, L.A.; Meadows, R.L.; Kerl, M.E.; Tessman, R.K.; Perlis, J.; Declue, A.E. Evaluation of a continuous glucose monitoring system for use in veterinary medicine. Diabetes Technol. Ther. 2005, 7, 885–895. [Google Scholar] [CrossRef]
- Del Baldo, F.; Canton, C.; Testa, S.; Swales, H.; Drudi, I.; Golinelli, S.; Fracassi, F. Comparison between a flash glucose monitoring system and a portable blood glucose meter for monitoring dogs with diabetes mellitus. J. Vet. Intern. Med. 2020, 34, 2296–2305. [Google Scholar] [CrossRef]
- Deiss, D.; Szadkowska, A.; Gordon, D.; Mallipedhi, A.; Schütz-Fuhrmann, I.; Aguilera, E.; Ringsell, C.; De Block, C.; Irace, C. Clinical practice recommendations on the routine use of Eversense, the first long-term implantable continuous glucose monitoring system. Diabetes Technol. Ther. 2019, 21, 254–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irace, C.; Cutruzzolà, A.; Nuzzi, A.; Assaloni, R.; Brunato, B.; Pitocco, D.; Tartaglione, L.; Di Molfetta, S.; Cignarelli, A.; Laviola, L.; et al. Clinical Use of a 180-Day Implantable Glucose Sensor Improves Glycated Hemoglobin and Time in Range in Patients with Type 1 Diabetes. Diabetes Obes. Metab. 2020, 22, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Kropff, J.; Choudhary, P.; Neupane, S.; Barnard, K.; Bain, S.C.; Kapitza, C.; Forst, T.; Link, M.; Dehennis, A.; DeVries, J.H. Accuracy and longevity of an implantable continuous glucose sensor in the PRECISE study: A 180-day, prospective, multicenter, pivotal trial. Diabetes Care 2017, 40, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christiansen, M.P.; Klaff, L.J.; Brazg, R.; Chang, A.R.; Levy, C.J.; Lam, D.; Denham, D.S.; Atiee, G.; Bode, B.W.; Walters, S.J.; et al. A prospective multicenter evaluation of the accuracy of a novel implanted continuous glucose sensor: PRECISE II. Diabetes Technol. Ther. 2018, 20, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Aronson, R.; Abitbol, A.; Tweden, K.S. First assessment of the performance of an implantable continuous glucose monitoring system through 180 days in a primarily adolescent population with type 1 diabetes. Diabetes Obes. Metab. 2019, 21, 1689–1694. [Google Scholar] [CrossRef]
- Christiansen, M.P.; Klaff, L.J.; Bailey, T.S.; Brazg, R.; Carlson, G.; Tweden, K.S. A prospective multicenter evaluation of the accuracy and safety of an implanted continuous glucose sensor: The PRECISION study. Diabetes Technol. Ther. 2019, 21, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Deiss, D.; Irace, C.; Carlson, G.; Tweden, K.S.; Kaufman, F.R. Real-world safety of an implantable continuous glucose sensor over multiple cycles of use: A post-market registry study. Diabetes Technol. Ther. 2020, 22, 48–52. [Google Scholar] [CrossRef]
- Cohen, T.A.; Nelson, R.W.; Kass, P.H.; Christopher, M.M.; Feldman, E.C. Evaluation of six portable blood glucose meters for measuring blood glucose concentration in dogs. J. Am. Vet. Med. Assoc. 2009, 235, 276–280. [Google Scholar] [CrossRef]
- Shea, E.K.; Hess, R.S. Assessment of postprandial hyperglycemia and circadian fluctuation of glucose concentrations in diabetic dogs using a flash glucose monitoring system. J. Vet. Intern. Med. 2021, 35, 843–852. [Google Scholar] [CrossRef]
- Kirchsteiger, H.; Heinemann, L.; Freckmann, G.; Lodwig, V.; Schmelzeisen-Redeker, G.; Schoemaker, M.; Del Re, L. Performance comparison of CGM systems: MARD values are not always a reliable indicator of CGM system accuracy. J. Diabetes Sci. Technol. 2015, 9, 1030–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obermaier, K.; Schmelzeisen-Redeker, G.; Schoemaker, M.; Klötzer, H.M.; Kirchsteiger, H.; Eikmeier, H.; del Re, L. Performance evaluations of continuous glucose monitoring systems: Precision absolute relative deviation is part of the assessment. J. Diabetes Sci. Technol. 2013, 7, 824–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
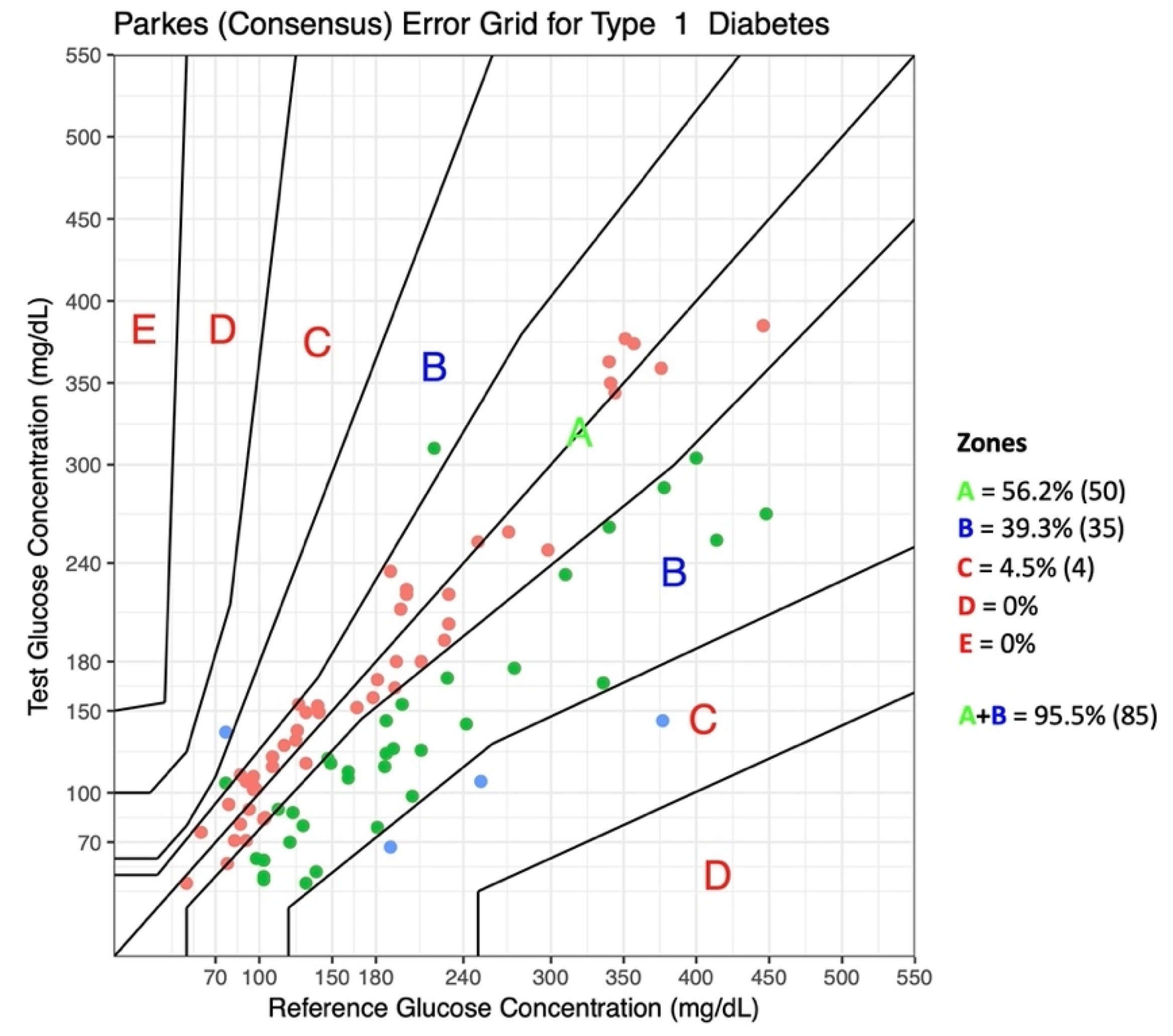
- Parkes, J.L.; Slatin, S.L.; Pardo, S.; Ginsberg, B.H. A new Consensus Error grid to evaluate the clinical significance of inaccuracies in the measurement of blood glucose. Diabetes Care 2000, 23, 1143–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanenbaum, M.L.; Hanes, S.J.; Miller, K.M.; Naranjo, D.; Bensen, R.; Hood, K.K. Diabetes device use in adults with type 1 diabetes: Barriers to uptake and potential intervention targets. Diabetes Care 2017, 40, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Engler, R.; Routh, T.L.; Lucisano, J.Y. Adoption barriers for continuous glucose monitoring and their potential reduction with a fully implanted system: Results from patient preference surveys. Clin. Diabetes 2018, 36, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Zeugswetter, F.K.; Sellner, A. Flash glucose monitoring in diabetic dogs: A feasible method for evaluating glycemic control. Tierarztl. Prax. Ausg. K Kleintiere/Heimtiere 2020, 48, 330–338. [Google Scholar] [CrossRef]
- Shoelson, A.; Mahony, O.M.; Pavlick, M. Complications associated with a flash glucose monitoring system in diabetic cats. J. Feline Med. Surg. 2021, 23, 557–562. [Google Scholar] [CrossRef]
- Pyl, J.; Dendooven, E.; Van Eekelen, I.; den Brinker, M.; Dotremont, H.; France, A.; Foubert, K.; Pieters, L.; Lambert, J.; De Block, C.; et al. Prevalence and prevention of contact dermatitis caused by FreeStyle Libre: A monocentric experience. Diabetes Care 2020, 43, 918–920. [Google Scholar] [CrossRef]
- Pavletic, M.M. Anatomy and circulation of the canine skin. Microsurgery 1991, 12, 103–112. [Google Scholar] [CrossRef]
- Joseph, J.I. Review of the Long-Term Implantable Senseonics Continuous Glucose Monitoring System and Other Continuous Glucose Monitoring Systems. J. Diabetes Sci. Technol. 2021, 15, 167–173. [Google Scholar] [CrossRef]
- Eversense, X.L. User Guide; Senseonics Inc.: Germantown, MD, USA, 2018; Rev B 06/2019; Available online: https://global.eversensediabetes.com/sites/default/files/2019-09/LBL-1402-28-001_Rev_B_Eversense_User_Guide_mgdL_UAE_Web.pdf (accessed on 10 December 2021).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Glucose (mg/dL) | DOG 1 | DOG 3 |
|---|---|---|
| Mean glucose (±SD 1) | 119 ± 49.8 | 249 ± 87.4 |
| Lowest sensor glucose | 40 | 44 |
| Highest sensor glucose | 350 | 399 |
| Total number of glucose values | 22.022 | 9.151 |
| % within glucose target (70–250) | 86.1 | 47.4 |
| % below glucose target (<70) | 11.9 | 0.2 |
| % above glucose target (>250) | 2.1 | 52.3 |
| % below low-glucose alert (<60) | 8.8 | - |
| % above high-glucose alert (>350) | - | 14.1 |
| Low Glucose Range (BG < 100 mg/dL) | |
|---|---|
| Number of glucose values | 17 |
| MAD (mg/dL) | 17.4 |
| Percent of values within ±15 mg/dL of the BG value | 52.9% (9/17) |
| High Glucose Range (BG > 100 mg/dL) | |
| Number of glucose values | 72 |
| MARD (%) mARD (%) MRD (%) Percent of values within ±15% of the BG value | 24.5 |
| 20.5 | |
| −18.7 | |
| 41.7% (30/72) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tardo, A.M.; Irace, C.; Del Baldo, F.; Foglia, A.; Fracassi, F. Clinical Use of a 180-Day Implantable Glucose Monitoring System in Dogs with Diabetes Mellitus: A Case Series. Animals 2022, 12, 860. https://doi.org/10.3390/ani12070860
Tardo AM, Irace C, Del Baldo F, Foglia A, Fracassi F. Clinical Use of a 180-Day Implantable Glucose Monitoring System in Dogs with Diabetes Mellitus: A Case Series. Animals. 2022; 12(7):860. https://doi.org/10.3390/ani12070860
Chicago/Turabian StyleTardo, Antonio Maria, Concetta Irace, Francesca Del Baldo, Armando Foglia, and Federico Fracassi. 2022. "Clinical Use of a 180-Day Implantable Glucose Monitoring System in Dogs with Diabetes Mellitus: A Case Series" Animals 12, no. 7: 860. https://doi.org/10.3390/ani12070860
APA StyleTardo, A. M., Irace, C., Del Baldo, F., Foglia, A., & Fracassi, F. (2022). Clinical Use of a 180-Day Implantable Glucose Monitoring System in Dogs with Diabetes Mellitus: A Case Series. Animals, 12(7), 860. https://doi.org/10.3390/ani12070860