
Patient and Caregiver Perceptions of Animal Assisted Activity in Orthodontics


 ,
,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. AAA Concerns and Benefits
3.2. Dental Anxiety and AAA
3.3. Impact of the COVID-19 Pandemic
4. Discussion
5. Conclusions
- -
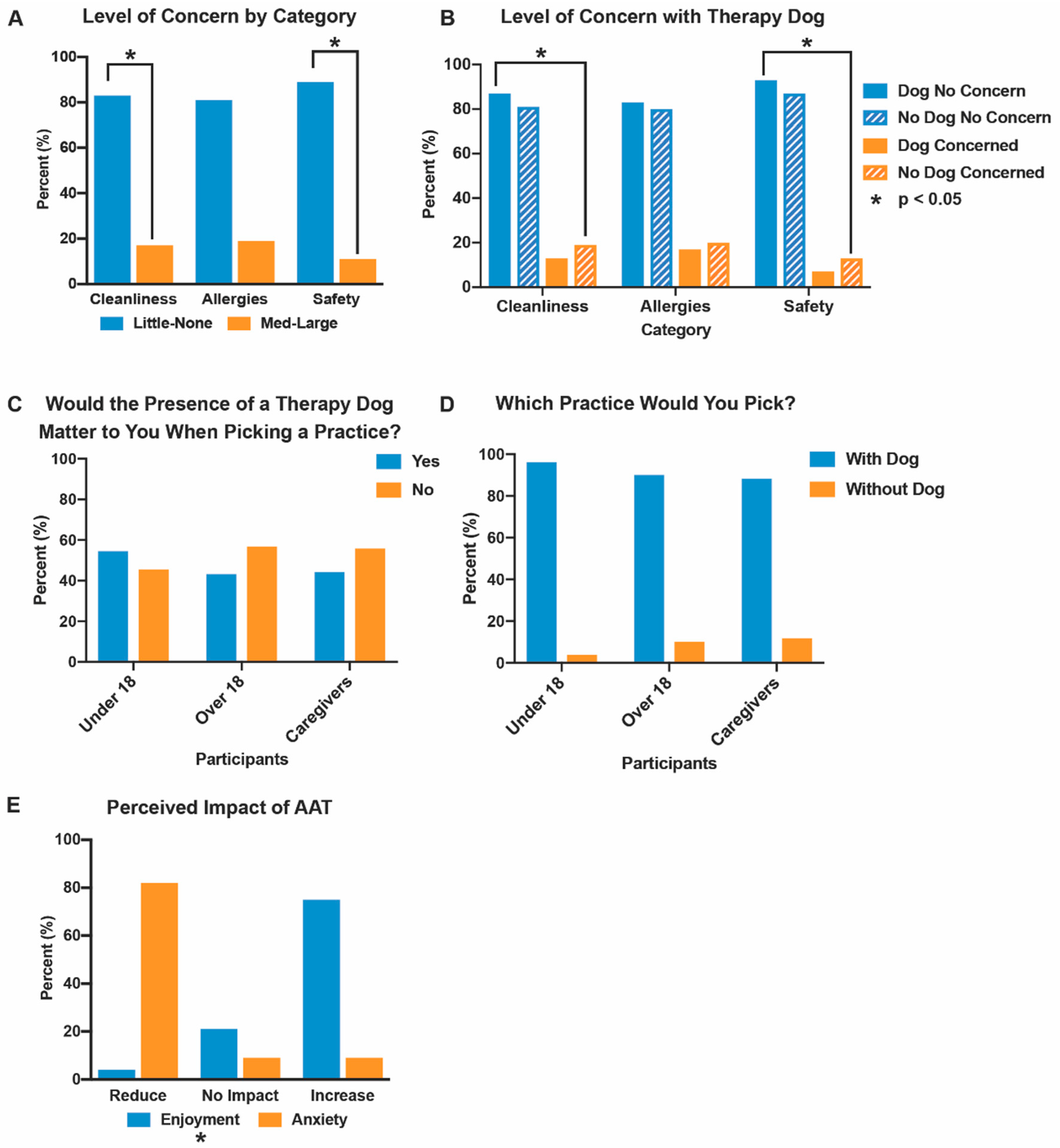
- Over a third of patients under 18 have a level of orthodontic anxiety that could benefit from interventions such as AAA.
- -
- The majority of patients and caregivers believe dental AAA will reduce anxiety and boost enjoyment.
- -
- For nearly half of the participants, an office with a therapy dog would influence their choice of provider, with most (92%) choosing the dog.
- -
- The majority of participants were unconcerned with the potential allergies (81%), safety risks (89%), and cleanliness (83%) of the therapy dogs.
- -
- AAA could be a valuable practice builder and promising anxiety-management tool welcomed by most families.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- White, A.M.; Giblin, L.; Boyd, L.D. The Prevalence of Dental Anxiety in Dental Practice Settings. J. Dent. Hyg. 2017, 91, 30–34. [Google Scholar] [PubMed]
- Grisolia, B.M.; dos Santos, A.P.P.; Dhyppolito, I.M.; Buchanan, H.; Hill, K.; Oliveira, B.H. Prevalence of Dental Anxiety in Children and Adolescents Globally: A Systematic Review with Meta-Analyses. Int. J. Paediatr. Dent. 2021, 31, 168–183. [Google Scholar] [CrossRef] [PubMed]
- Locker, D.; Liddell, A.; Dempster, L.; Shapiro, D. Age of Onset of Dental Anxiety. J. Dent. Res. 1999, 78, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Klingberg, G.; Broberg, A.G. Dental Fear/Anxiety and Dental Behaviour Management Problems in Children and Adolescents: A Review of Prevalence and Concomitant Psychological Factors. Int. J. Paediatr. Dent. 2007, 17, 391–406. [Google Scholar] [CrossRef] [PubMed]
- McGrath, C.; Bedi, R. The Association between Dental Anxiety and Oral Health-Related Quality of Life in Britain. Community Dent. Oral. Epidemiol. 2004, 32, 67–72. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentistry Behavior Guidance for the Pediatric Dental Patient. Pediatr. Dent. 2018, 40, 254–267.
- Coté, C.J.; Wilson, S.; American Academy of Pediatrics; American Academy of Pediatric Dentistry. Guidelines for Monitoring and Management of Pediatric Patients Before, During, and After Sedation for Diagnostic and Therapeutic Procedures. Pediatrics 2019, 143, e20191000. [Google Scholar] [CrossRef] [Green Version]
- Fleming, P.S. Timing Orthodontic Treatment: Early or Late? Aust. Dent. J. 2017, 62 (Suppl. 1), 11–19. [Google Scholar] [CrossRef] [Green Version]
- American Veterinary Medical Association. Animal-Assisted Interventions: Definitions. Available online: https://www.avma.org/resources-tools/avma-policies/animal-assisted-interventions-definitions (accessed on 7 July 2022).
- Marcus, D.A. The Science behind Animal-Assisted Therapy. Curr. Pain Headache Rep. 2013, 17, 322. [Google Scholar] [CrossRef]
- Braun, C.; Stangler, T.; Narveson, J.; Pettingell, S. Animal-Assisted Therapy as a Pain Relief Intervention for Children. Complement. Ther. Clin. Pract. 2009, 15, 105–109. [Google Scholar] [CrossRef]
- Marcus, D.A.; Bernstein, C.D.; Constantin, J.M.; Kunkel, F.A.; Breuer, P.; Hanlon, R.B. Animal-Assisted Therapy at an Outpatient Pain Management Clinic. Pain Med. 2012, 13, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Kamioka, H.; Okada, S.; Tsutani, K.; Park, H.; Okuizumi, H.; Handa, S.; Oshio, T.; Park, S.-J.; Kitayuguchi, J.; Abe, T.; et al. Effectiveness of Animal-Assisted Therapy: A Systematic Review of Randomized Controlled Trials. Complement. Ther. Med. 2014, 22, 371–390. [Google Scholar] [CrossRef]
- Filan, S.L.; Llewellyn-Jones, R.H. Animal-Assisted Therapy for Dementia: A Review of the Literature. Int. Psychogeriatr. 2006, 18, 597–611. [Google Scholar] [CrossRef] [PubMed]
- Nammalwar, R.B.; Rangeeth, P. A Bite out of Anxiety: Evaluation of Animal-Assisted Activity on Anxiety in Children Attending a Pediatric Dental Outpatient Unit. J. Indian Soc. Pedod. Prev. Dent. 2018, 36, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Fierro, N.; Vanegas-Farfano, M.; González-Ramírez, M.T. Dog-Assisted Therapy and Dental Anxiety: A Pilot Study. Animals 2019, 9, 512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Havener, L.; Gentes, L.; Thaler, B.; Megel, M.E.; Baun, M.M.; Driscoll, F.A.; Beiraghi, S.; Agrawal, S. The Effects of a Companion Animal on Distress in Children Undergoing Dental Procedures. Issues Compr. Pediatr. Nurs. 2001, 24, 137–152. [Google Scholar] [CrossRef]
- Charowski, M.; Wells, M.H.; Dormois, L.; Fernandez, J.A.; Scarbecz, M.; Maclin, M. A Randomized Controlled Pilot Study Examining Effects of Animal Assisted Therapy in Children Undergoing Sealant Placement. Pediatr. Dent. 2021, 43, 10–16. [Google Scholar]
- Gupta, N.; Yadav, T. Parents’ Acceptance and Their Children’s Choice of Pet for Animal-Assisted Therapy (A.A.T.) in 3- to 12-Year-Old Children in the Dental Operatory—A Questionnaire-Based Pilot Study. Int. J. Paediatr. Dent. 2018, 28, 373–379. [Google Scholar] [CrossRef]
- Gussgard, A.M.; Weese, J.S.; Hensten, A.; Jokstad, A. Dog-Assisted Therapy in the Dental Clinic: Part A-Hazards and Assessment of Potential Risks to the Health and Safety of Humans. Clin. Exp. Dent. Res. 2019, 5, 692–700. [Google Scholar] [CrossRef] [Green Version]
- Lefebvre, S.L.; Golab, G.C.; Christensen, E.; Castrodale, L.; Aureden, K.; Bialachowski, A.; Gumley, N.; Robinson, J.; Peregrine, A.; Benoit, M.; et al. Guidelines for Animal-Assisted Interventions in Health Care Facilities. Am. J. Infect. Control 2008, 36, 78–85. [Google Scholar] [CrossRef]
- Corah, N.L.; Gale, E.N.; Illig, S.J. Assessment of a Dental Anxiety Scale. J. Am. Dent. Assoc. 1978, 97, 816–819. [Google Scholar] [CrossRef] [PubMed]
- Humphris, G.; Crawford, J.R.; Hill, K.; Gilbert, A.; Freeman, R. UK Population Norms for the Modified Dental Anxiety Scale with Percentile Calculator: Adult Dental Health Survey 2009 Results. BMC Oral Health 2013, 13, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho, C.M.; Suttiwan, P.; Arato, N.; Zsido, A.N. On the Nature of Fear and Anxiety Triggered by COVID-19. Front. Psychol. 2020, 11, 581314. [Google Scholar] [CrossRef]
- Xiong, X.; Wu, Y.; Fang, X.; Sun, W.; Ding, Q.; Yi, Y.; Huang, Y.; Gong, J.; Liu, J.; Wang, J. Mental Distress in Orthodontic Patients during the Coronavirus Disease 2019 Pandemic. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 824–833. [Google Scholar] [CrossRef]
- Jason, D. Can You Get Covid-19 From Your Dog? Here’s What Disease Experts Say. Available online: https://www.wsj.com/articles/can-you-get-covid-19-from-your-dog-heres-what-disease-experts-say-11599494410 (accessed on 5 April 2022).
- World Organization for Animal Health. Infection with SARS-CoV-2 in Animals. Available online: https://www.woah.org/app/uploads/2021/11/en-factsheet-sars-cov-2-20211025.pdf (accessed on 11 July 2022).
- Sila, T.; Sunghan, J.; Laochareonsuk, W.; Surasombatpattana, S.; Kongkamol, C.; Ingviya, T.; Siripaitoon, P.; Kositpantawong, N.; Kanchanasuwan, S.; Hortiwakul, T.; et al. Suspected Cat-to-Human Transmission of SARS-CoV-2, Thailand, July–September 2021. Emerg. Infect. Dis. 2022, 28, 1485–1488. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Animals and COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/animals.html (accessed on 11 July 2022).
- American Veterinary Medical Association. SARS-CoV-2 in Animals. Available online: https://www.avma.org/resources-tools/one-health/covid-19/sars-cov-2-animals-including-pets (accessed on 11 July 2022).
- Sit, T.H.C.; Brackman, C.J.; Ip, S.M.; Tam, K.W.S.; Law, P.Y.T.; To, E.M.W.; Yu, V.Y.T.; Sims, L.D.; Tsang, D.N.C.; Chu, D.K.W.; et al. Infection of Dogs with SARS-CoV-2. Nature 2020, 586, 776–778. [Google Scholar] [CrossRef]
- Bosco-Lauth, A.M.; Hartwig, A.E.; Porter, S.M.; Gordy, P.W.; Nehring, M.; Byas, A.D.; VandeWoude, S.; Ragan, I.K.; Maison, R.M.; Bowen, R.A. Experimental Infection of Domestic Dogs and Cats with SARS-CoV-2: Pathogenesis, Transmission, and Response to Reexposure in Cats. Proc. Natl. Acad. Sci. USA 2020, 117, 26382–26388. [Google Scholar] [CrossRef]
- Patterson, E.I.; Elia, G.; Grassi, A.; Giordano, A.; Desario, C.; Medardo, M.; Smith, S.L.; Anderson, E.R.; Prince, T.; Patterson, G.T.; et al. Evidence of Exposure to SARS-CoV-2 in Cats and Dogs from Households in Italy. Nat. Commun. 2020, 11, 6231. [Google Scholar] [CrossRef]
- Calvet, G.A.; Pereira, S.A.; Ogrzewalska, M.; Pauvolid-Corrêa, A.; Resende, P.C.; de Tassinari, W.S.; de Costa, A.P.; Keidel, L.O.; da Rocha, A.S.B.; da Silva, M.F.B.; et al. In-vestigation of SARS-CoV-2 Infection in Dogs and Cats of Humans Diagnosed with COVID-19 in Rio de Janeiro, Brazil. PLoS ONE 2021, 16, e0250853. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Guidance for Handlers of Service and Therapy Animals. Available online: https://www.cdc.gov/healthypets/covid-19/service-therapy-animals.html (accessed on 11 July 2022).
- Centers for Disease Control and Prevention. What You Should Know about COVID-19 and Pets. Available online: https://www.cdc.gov/healthypets/covid-19/pets.html#:~:text=Pets%20worldwide%2C%20including%20cats%20and,19%20to%20people%20is%20low (accessed on 11 July 2022).
- Vincent, A.; Easton, S.; Sterman, J.; Farkas, K.; Heima, M. Acceptability and Demand of Therapy Dog Support Among Oral Health Care Providers and Caregivers of Pediatric Patients. Pediatr. Dent. 2020, 42, 16–21. [Google Scholar]
- Roy, J.; Dempster, L.J. Dental Anxiety Associated with Orthodontic Care: Prevalence and Contributing Factors. Semin. Orthod. 2018, 24, 233–241. [Google Scholar] [CrossRef]
- Murata, S.; Rezeppa, T.; Thoma, B.; Marengo, L.; Krancevich, K.; Chiyka, E.; Hayes, B.; Goodfriend, E.; Deal, M.; Zhong, Y.; et al. The Psychiatric Sequelae of the COVID-19 Pandemic in Adolescents, Adults, and Health Care Workers. Depress. Anxiety 2021, 38, 233–246. [Google Scholar] [CrossRef] [PubMed]
- Ng, Z.; Griffin, T.C.; Braun, L. The New Status Quo: Enhancing Access to Human–Animal Interactions to Alleviate Social Isolation & Loneliness in the Time of COVID-19. Animals 2021, 11, 2769. [Google Scholar] [CrossRef]
- Meers, L.L.; Contalbrigo, L.; Stevens, V.A.; Ulitina, O.M.; Laufer, S.J.; Samuels, W.E. The State of Animal-Assisted Interventions: COVID-19 Safety Protocols and Ethical Considerations. J. Appl. Anim. Ethics Res. 2021, 3, 103–125. [Google Scholar] [CrossRef]
- Kiros, M.; Andualem, H.; Kiros, T.; Hailemichael, W.; Getu, S.; Geteneh, A.; Alemu, D.; Abegaz, W.E. COVID-19 Pandemic: Current Knowledge about the Role of Pets and Other Animals in Disease Transmission. Virol. J. 2020, 17, 143. [Google Scholar] [CrossRef] [PubMed]
- Brunekreef, B.; Groot, B.; Hoek, G. Pets, Allergy and Respiratory Symptoms in Children. Int. J. Epidemiol. 1992, 21, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Comrey, A.L.; Lee, H.B. A First Course in Factor Analysis, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1992; Volume XII, ISBN 9781315827506. [Google Scholar]
- Guadagnoli, E.; Velicer, W.F. Relation of Sample Size to the Stability of Component Patterns. Psychol. Bull. 1988, 103, 265–275. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Group | Frequency (%) and Number (n) per Group * |
|---|---|---|
| Participant groups | Patients who are minors under 18 | 44.0% (n = 352) |
| Adult patients over 18 | 25.5% (n = 204) | |
| Caregivers | 30.5% (n = 244) | |
| Race | Caucasian | 68.8% (n = 391) |
| Black | 21.7% (n = 123) | |
| Asian | 7.6% (n = 43) | |
| Other | 1.9% (n = 11) | |
| Prefer to not answer | n = 232 | |
| Ethnicity | Hispanic | 18.8% (n = 150) |
| Not Hispanic | 81.3% (n = 650) | |
| Sex | Female | 65.7% (n = 460) |
| Male | 34.3% (n = 240) | |
| Prefer to not answer | n = 100 | |
| Dog Allergy | Diagnosed allergy to dogs | 4.1% (n = 30) |
| No allergy | 95.9% (n = 706) | |
| Fear of dogs | Not at all afraid of dogs | 77.1% (n = 566) |
| Only a little afraid of dogs | 17.0% (n = 125) | |
| Somewhat afraid of dogs | 4.1% (n = 30) | |
| Very afraid | 1.8% (n = 13) | |
| Dog Presence ** | Dog present ** | 41.0% (n = 328) |
| No dog present ** | 59.0% (n = 472) | |
| COVID ^ | Pre-shutdown ^ | 16.1% (n = 129) |
| Post-shutdown ^ | 83.9% (n = 671) | |
| Pet at home ^^ | Pet(s) at home of any species | 71.0% (n = 512) |
| No pet at home | 29.0% (n = 288) | |
| Pet dog(s) ^^ | 60.1% (n = 434) | |
| No pet dog ^^ | 39.9% (n = 288) | |
| Total n = 800 |
| When Thinking about a Therapy Dog in a Dental Setting, How Much Concern Would You Have for Each of the Following? (Q10) | ||||||
|---|---|---|---|---|---|---|
| Little to No Concern | Medium to Large Concern | n ^ | p-Value * | |||
| Age Groups | Cleanliness | Overall | 83% | 17% | 721 ^ | 0.5106 |
| 599 ^ | 122 ^ | |||||
| Under 18 ** | 83.8% | 16.2% | ||||
| 244 ^ | 47 ^ | |||||
| Over 18 ** | 80.9% | 19.1% | ||||
| 157 | 37 | |||||
| Caregivers ** | 83.9% | 16.1% | ||||
| 198 | 38 | |||||
| Allergies | Overall | 81% | 19% | 718 | 0.3436 | |
| 583 | 135 | |||||
| Under 18 | 79.3% | 20.7% | ||||
| 230 | 60 | |||||
| Over 18 | 84.4% | 15.6% | ||||
| 162 | 30 | |||||
| Caregivers | 80.9% | 19.1% | ||||
| 191 | 45 | |||||
| Safety | Overall | 89% | 11% | 718 | 0.9829 | |
| 642 | 76 | |||||
| Under 18 | 89.7% | 10.3% | ||||
| 260 | 30 | |||||
| Over 18 | 89.1% | 10.9% | ||||
| 171 | 21 | |||||
| Caregivers | 89.4% | 10.6% | ||||
| 211 | 25 | |||||
| Dog vs. No Dog in Clinic ** | Cleanliness | Dog *** | 87% | 13% | 721 | 0.0213 * |
| 256 | 39 | |||||
| No Dog *** | 81% | 19% | ||||
| 343 | 83 | |||||
| Allergies | Dog | 83% | 17% | 718 | 0.2877 | |
| 246 | 49 | |||||
| No Dog | 80% | 20% | ||||
| 337 | 86 | |||||
| Safety | Dog | 93% | 7% | 718 | 0.0185 * | |
| 274 | 21 | |||||
| No Dog | 87% | 13% | ||||
| 368 | 55 | |||||
| Pet dog vs. No pet dog ^^ | Cleanliness | Pet ^^ | 86.8% | 13.2% | 721 | 0.00005 * |
| 382 | 58 | |||||
| No Pet Dog ^^ | 77.2% | 22.8% | ||||
| 217 | 64 | |||||
| Allergies | Pet | 84.2% | 15.8% | 718 | 0.0040 * | |
| 369 | 69 | |||||
| No Pet Dog | 76.4% | 23.6% | ||||
| 214 | 66 | |||||
| Safety | Pet | 92.4% | 7.6% | 718 | 0.00009 * | |
| 404 | 33 | |||||
| No Pet Dog | 84.7% | 15.3% | ||||
| 238 | 43 | |||||
| If You Were Making a Choice Between Two Similar Orthodontic Practices, Would the Presence of a Dog Matter to You? (Q19) | ||||
|---|---|---|---|---|
| Yes | No | n ^ | p-Value | |
| Overall | 48.1% | 51.9% | 695 ^ | 0.0210 * |
| 334 ^ | 361 ^ | |||
| Under 18 ** | 54.5% | 45.5% | 279 | |
| 152 | 127 | |||
| Over 18 ** | 43.2% | 56.8% | 185 | |
| 80 | 105 | |||
| Caregivers ** | 44.2% | 55.8% | 231 | |
| 102 | 129 | |||
| Pet Dog ^^ | 53.8% | 46.2% | 422 | 0.0017 * |
| 227 | 195 | |||
| No Pet Dog ^^ | 39.2% | 60.8% | 273 | |
| 107 | 166 | |||
| If Answered “Yes” Above, Which Practice Would You Pick? (Q20) | ||||
| With Dog | Without Dog | n ^ | p-Value | |
| Overall | 92.2% | 7.8% | 334 ^ | 0.0523 * |
| 308^ | 26^ | |||
| Under 18 | 96.1% | 3.9% | 152 | |
| 146 | 6 | |||
| Over 18 | 90.0% | 10.0% | 80 | |
| 72 | 8 | |||
| Caregivers | 88.2% | 11.8% | 102 | |
| 90 | 12 | |||
| Pet Dog | 95.6% | 4.4% | 227 | 0.0080 * |
| 217 | 10 | |||
| No Pet Dog | 85.0% | 15.0% | 107 | |
| 91 | 16 | |||
| Corah Dental Anxiety Category ^^ | Orthodontic Anxiety Category ^^ | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | Total n ^ | Limited | Moderate | High | Severe | Group p-Value | Limited | Moderate | High | Severe | Group p-Value | p-Value Dent v. Ortho ^^ |
| All | 664 ^ | 364 ^ | 221 ^ | 39 ^ | 40 ^ | 416 ^ | 191 ^ | 30 ^ | 27 ^ | 0.0030 * | ||
| 54.8% | 33.4% | 5.9% | 5.9% | 62.65% | 28.76% | 4.52% | 4.07% | |||||
| Gender | 0.0001 * | 0.0066 * | ||||||||||
| Males | 224 | 146 | 70 | 6 | 8 | 150 | 63 | 9 | 2 | 0.2360 | ||
| 63.5% | 30.4% | 2.6% | 3.5% | 63.5% | 30.4% | 2.6% | 3.5% | |||||
| Females | 432 | 220 | 155 | 34 | 32 | 261 | 125 | 21 | 25 | 0.0001 * | ||
| 49.9% | 35.2% | 7.7% | 7.3% | 60.4% | 28.9% | 4.9% | 5.8% | |||||
| Age group | 0.0079 * | 0.0007 * | ||||||||||
| Patients Under 18 | 266 | 153 | 94 | 12 | 13 | 172 | 74 | 13 | 7 | 0.0059 * | ||
| 56.3% | 34.6% | 4.4% | 4.8% | 64.7% | 27.8% | 4.9% | 2.6% | |||||
| Patients Over 18 | 174 | 109 | 53 | 9 | 8 | 127 | 35 | 6 | 6 | 0.0341 * | ||
| 60.9% | 29.6% | 5.0% | 4.5% | 73.0% | 20.1% | 3.5% | 3.5% | |||||
| Caregiver | 224 | 110 | 80 | 19 | 19 | 117 | 82 | 11 | 14 | 0.0907 | ||
| 48.3% | 35.1% | 8.3% | 8.3% | 52.2% | 36.6% | 4.9% | 6.2% | |||||
| Dog/No Dog | 0.1586 | 0.0389 * | ||||||||||
| Dog present | 278 | 114 | 93 | 26 | 15 | 155 | 88 | 14 | 13 | 0.1664 | ||
| 51.8% | 33.5% | 9.4% | 5.4% | 57.4% | 32.6% | 5.2% | 4.8% | |||||
| No dog present | 401 | 228 | 134 | 14 | 2 | 261 | 104 | 16 | 14 | 0.0007 * | ||
| 56.9% | 33.4% | 3.5% | 6.2% | 66.2% | 26.1% | 4.1% | 3.6% | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cass, K.; Bocklage, C.; Sulkowski, T.; Graves, C.; Ghaltakhchyan, N.; Rapolla, A.; Jackson, T.; Divaris, K.; Wiesen, C.; Strauman, T.; et al. Patient and Caregiver Perceptions of Animal Assisted Activity in Orthodontics. Animals 2022, 12, 1862. https://doi.org/10.3390/ani12141862
Cass K, Bocklage C, Sulkowski T, Graves C, Ghaltakhchyan N, Rapolla A, Jackson T, Divaris K, Wiesen C, Strauman T, et al. Patient and Caregiver Perceptions of Animal Assisted Activity in Orthodontics. Animals. 2022; 12(14):1862. https://doi.org/10.3390/ani12141862
Chicago/Turabian StyleCass, Katelyn, Clare Bocklage, Taylor Sulkowski, Christina Graves, Nare Ghaltakhchyan, Allen Rapolla, Tate Jackson, Kimon Divaris, Chris Wiesen, Timothy Strauman, and et al. 2022. "Patient and Caregiver Perceptions of Animal Assisted Activity in Orthodontics" Animals 12, no. 14: 1862. https://doi.org/10.3390/ani12141862
APA StyleCass, K., Bocklage, C., Sulkowski, T., Graves, C., Ghaltakhchyan, N., Rapolla, A., Jackson, T., Divaris, K., Wiesen, C., Strauman, T., & Jacox, L. (2022). Patient and Caregiver Perceptions of Animal Assisted Activity in Orthodontics. Animals, 12(14), 1862. https://doi.org/10.3390/ani12141862