Measurement of Plasma Resistin Concentrations in Horses with Metabolic and Inflammatory Disorders

 ,
,  ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Blood Biochemistry
2.3. Statistical Analysis
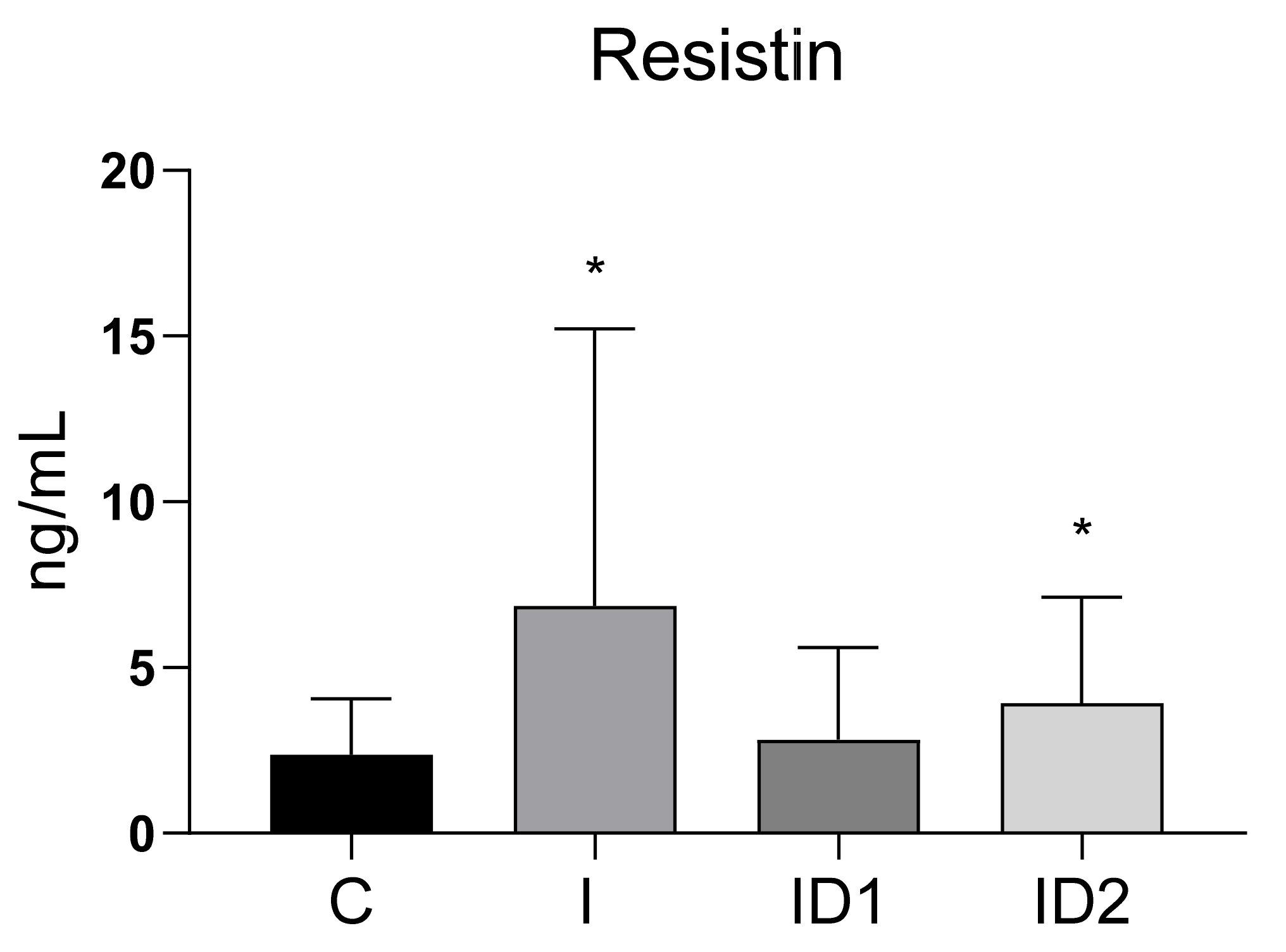
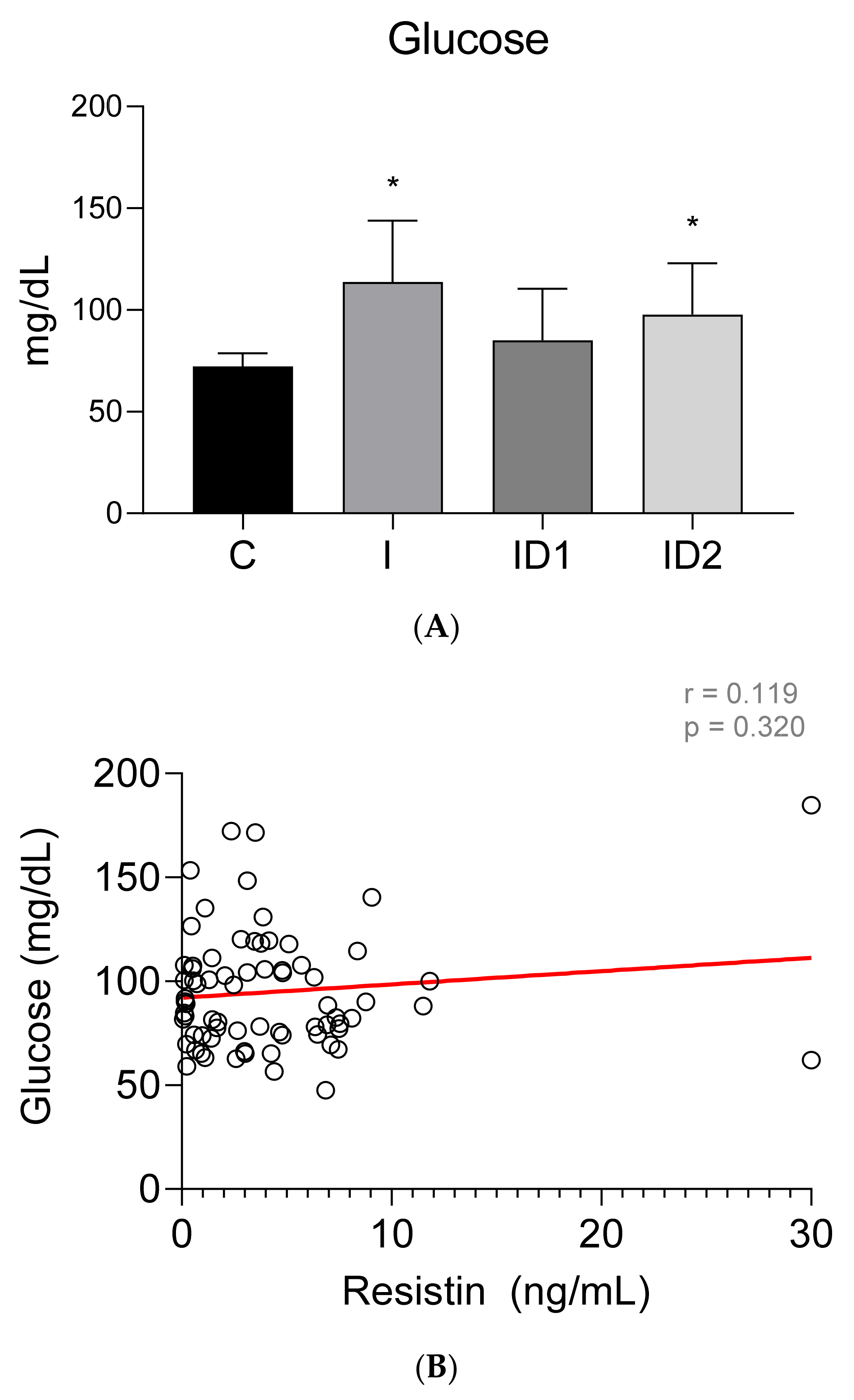
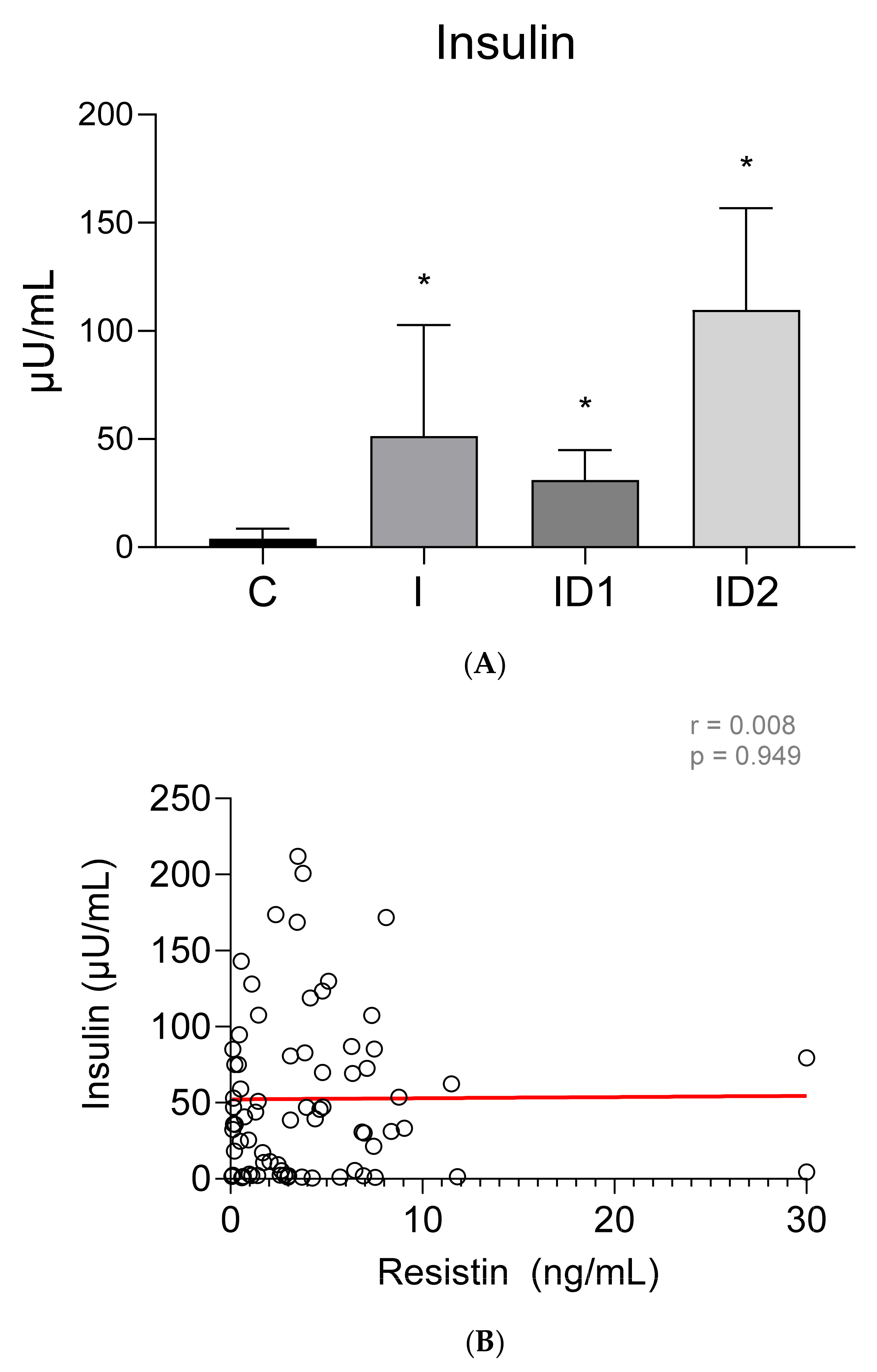
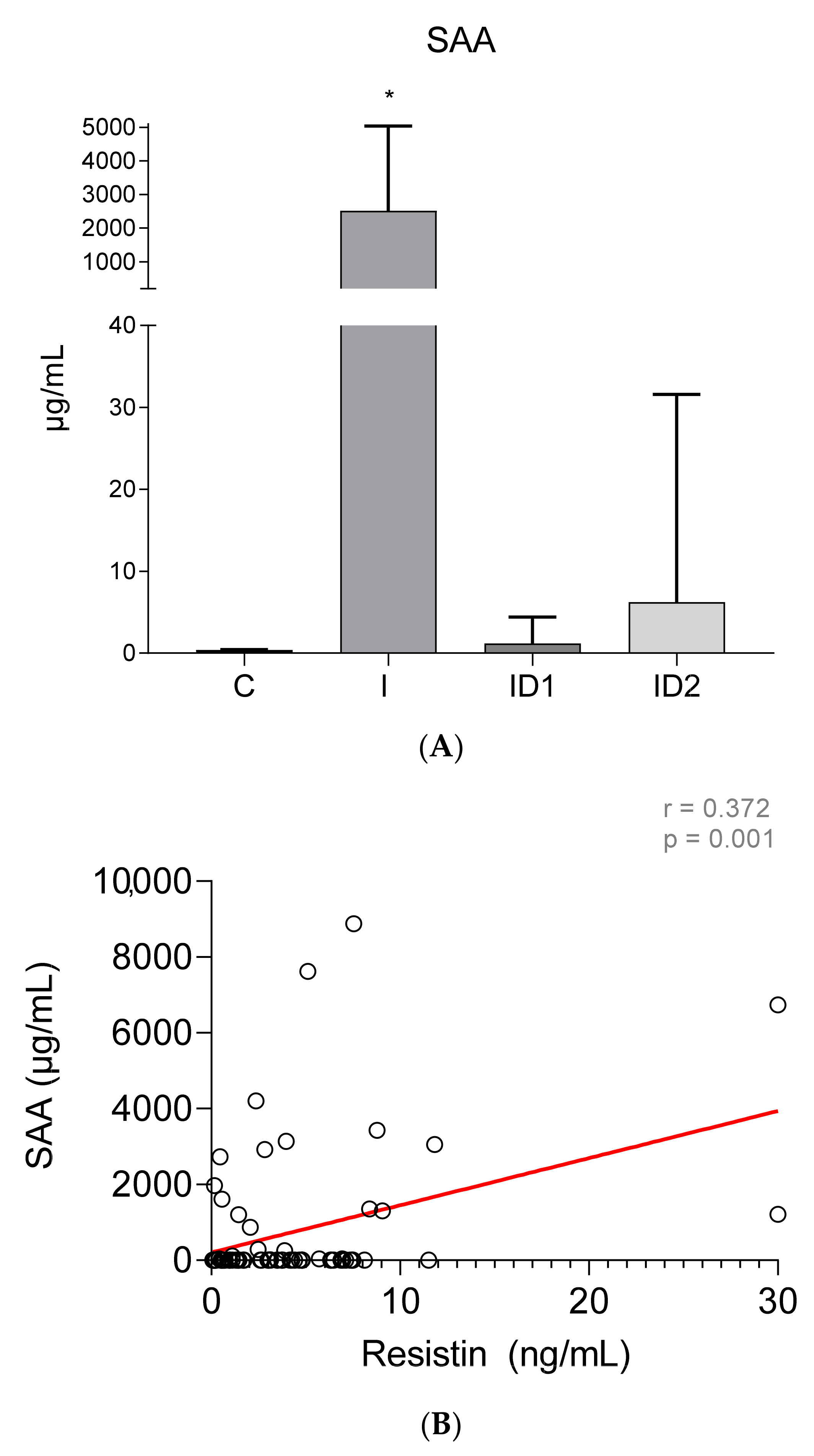
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ertelt, A.; Barton, A.-K.; Schmitz, R.R.; Gehlen, H. Metabolic syndrome: Is equine disease comparable to what we know in humans? Endocr. Connect. 2014, 3, R81–R93. [Google Scholar] [CrossRef] [PubMed]
- Frank, N. Equine Metabolic Syndrome. Vet. Clin. N. Am. Equine Pract. 2011, 27, 73–92. [Google Scholar] [CrossRef] [PubMed]
- Durham, A.E.; Frank, N.; McGowan, C.M.; Menzies-Gow, N.J.; Roelfsema, E.; Vervuert, I.; Feige, K.; Fey, K. ECEIM consensus statement on equine metabolic syndrome. J. Vet. Intern. Med. 2019, 33, 335–349. [Google Scholar] [CrossRef] [PubMed]
- Frank, N.; Tadros, E.M. Insulin dysregulation. Equine Vet. J. 2014, 46, 103–112. [Google Scholar] [CrossRef]
- Kershaw, E.E.; Flier, J.S. Adipose tissue as an endocrine organ. J. Clin. Endocrinol. Metab. 2004, 89, 2548–2556. [Google Scholar] [CrossRef]
- Radin, M.J.; Sharkey, L.C.; Holycross, B.J. Adipokines: A reviewof biological and analytical principles and an update in dogs, cats, and horses. Vet. Clin. Pathol. 2009, 38, 136–156. [Google Scholar] [CrossRef]
- Lago, F.; Dieguez, C.; Gómez-Reino, J.; Gualillo, O. Adipokines as emerging mediators of immune response and inflammation. Nat. Clin. Pract. Rheumatol. 2007, 3, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Wellen, K.E.; Hotamisligil, G.S. Inflammation, stress, and diabetes. J. Clin. Investig. 2005, 115, 1111–1119. [Google Scholar] [CrossRef]
- Steppan, C.M.; Bailey, S.T.; Bhat, S.; Brown, E.J.; Banerjee, R.R.; Wright, C.M.; Patel, H.R.; Ahima, R.S.; Lazar, M.A. The hormone resistin links obesity to diabetes. Nature 2001, 409, 307–312. [Google Scholar] [CrossRef]
- Steppan, C.M.; Lazar, M.A. The current biology of resistin. J. Intern. Med. 2004, 255, 439–447. [Google Scholar] [CrossRef]
- Kojta, I.; Chacińska, M.; Błachnio-Zabielska, A. Obesity, bioactive lipids, and adipose tissue inflammation in insulin resistance. Nutrients 2020, 12, 1305. [Google Scholar] [CrossRef] [PubMed]
- Taouis, M.; Benomar, Y. Is resistin the master link between inflammation and inflammation-related chronic diseases? Mol. Cell. Endocrinol. 2021, 533, 111341. [Google Scholar] [CrossRef]
- Patel, L.; Buckels, A.C.; Kinghorn, I.J.; Murdock, P.R.; Holbrook, J.D.; Plumpton, C.; Macphee, C.H.; Smith, S.A. Resistin is expressed in human macrophages and directly regulated by PPARγ activators. Biochem. Biophys. Res. Commun. 2003, 300, 472–476. [Google Scholar] [CrossRef]
- Barnes, K.; Miner, J. Role of Resistin in Insulin Sensitivity in Rodents and Humans. Curr. Protein Pept. Sci. 2009, 10, 96–107. [Google Scholar] [CrossRef]
- Amirhakimi, A.; Karamifar, H.; Moravej, H.; Amirhakimi, G. Serum resistin level in obese male children. J. Obes. 2011, 2011, 10–12. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Boyraz, M.; Cekmez, F.; Karaoǧlu, A.; Cinaz, P.; Durak, M.; Bideci, A. Relationship of adipokines (adiponectin, resistin and RBP4) with metabolic syndrome components in pubertal obese children. Biomark. Med. 2013, 7, 423–428. [Google Scholar] [CrossRef]
- Gerber, M.; Boettner, A.; Seidel, B.; Lammert, A.; Bä, J.; Schuster, E.; Thiery, J.; Kiess, W.; Kratzsch, J. Serum Resistin Levels of Obese and Lean Children and Adolescents: Biochemical Analysis and Clinical Relevance. J. Clin. Endocrinol. Metab. 2005, 90, 4503–4509. [Google Scholar] [CrossRef]
- Park, H.K.; Ahima, R.S. Resistin in Rodents and Humans. Diabetes Metab. J. 2013, 37, 404–414. [Google Scholar] [CrossRef] [PubMed]
- Park, H.K.; Kwak, M.K.; Kim, H.J.; Ahima, R.S. Linking resistin, inflammation, and cardiometabolic diseases. Korean J. Intern. Med. 2017, 32, 239–247. [Google Scholar] [CrossRef]
- Su, K.Z.; Li, Y.R.; Zhang, D.; Yuan, J.H.; Zhang, C.S.; Liu, Y.; Song, L.M.; Lin, Q.; Li, M.W.; Dong, J. Relation of Circulating Resistin to Insulin Resistance in Type 2 Diabetes and Obesity: A Systematic Review and Meta-Analysis. Front. Physiol. 2019, 10, 1399. [Google Scholar] [CrossRef]
- Komatsu, T.; Itoh, F.; Mikawa, S.; Hodate, K. Gene expression of resistin in adipose tissue and mammary gland of lactating and non-lactating cows. J. Endocrinol. 2003, 178, 3–7. [Google Scholar] [CrossRef][Green Version]
- Dai, M.H.; Xia, T.; Chen, X.D.; Gan, L.; Feng, S.Q.; Qiu, H.; Peng, Y.; Yang, Z.Q. Cloning and characterization of porcine resistin gene. Domest. Anim. Endocrinol. 2006, 30, 88–97. [Google Scholar] [CrossRef]
- Takashima, S.; Nishii, N.; Kobatake, Y.; Kiyosue, M.; Kimura, S.; Kitagawa, H. Concentrations of leptin, adiponectin, and resistin in the serum of obese cats during weight loss. J. Vet. Med. Sci. 2019, 81, 1294–1300. [Google Scholar] [CrossRef]
- Reverchon, M.; Ramé, C.; Cognié, J.; Briant, E.; Elis, S.; Guillaume, D.; Dupont, J. Resistin in dairy cows: Plasma concentrations during early lactation, expression and potential role in adipose tissue. PLoS ONE 2014, 9, e93198. [Google Scholar] [CrossRef]
- Mellouk, N.; Rame, C.; Touzé, J.L.; Briant, E.; Ma, L.; Guillaume, D.; Lomet, D.; Caraty, A.; Ntallaris, T.; Humblot, P.; et al. Involvement of plasma adipokines in metabolic and reproductive parameters in Holstein dairy cows fed with diets with differing energy levels. J. Dairy Sci. 2017, 100, 8518–8533. [Google Scholar] [CrossRef]
- Weber, M.; Locher, L.; Huber, K.; Kenéz, A.; Rehage, J.; Tienken, R.; Meyer, U.; Dänicke, S.; Sauerwein, H.; Mielenz, M. Longitudinal changes in adipose tissue of dairy cows from late pregnancy to lactation. Part 1: The adipokines apelin and resistin and their relationship to receptors linked with lipolysis. J. Dairy Sci. 2016, 99, 1549–1559. [Google Scholar] [CrossRef]
- Guzel, S.; Belenli, D. The interrelationship between resistin and amylin plasma concentrations and their relation to the concentrations of selected reproductive and metabolic hormones and biochemical variables in the early lactation stage of Saanen goats. Rev. Med. Vet. 2015, 166, 229–233. [Google Scholar]
- Johnson, P.J. The equine metabolic syndrome. Peripheral Cushing’s syndrome. Vet. Clin. N. Am. Equine Pract. 2002, 18, 271–293. [Google Scholar] [CrossRef]
- Staub, C.; Venturi, E.; Cirot, M.; Léonard, L.; Barrière, P.; Blard, T.; Gaudé, Y.; Gascogne, T.; Yvon, J.M.; Lecompte, F.; et al. Ultrasonographic measures of body fatness and their relationship with plasma levels and adipose tissue expression of four adipokines in Welsh pony mares. Domest. Anim. Endocrinol. 2019, 69, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Henneke, D.R.; Potter, G.D.; Kreider, J.L.; Yeates, B.F. Relationship between condition score, physical measurements and body fat percentage in mares. Equine Vet. J. 1983, 15, 371–372. [Google Scholar] [CrossRef] [PubMed]
- Carter, R.A.; Geor, R.J.; Burton Staniar, W.; Cubitt, T.A.; Harris, P.A. Apparent adiposity assessed by standardised scoring systems and morphometric measurements in horses and ponies. Vet. J. 2009, 179, 204–210. [Google Scholar] [CrossRef]
- Frank, N.; Bailey, S.R.; Bertin, F.R.; De Laat, M.A.; Durham, A.E.; Kritchevsky, J.; Menzies-Gow, N.J. Recommendations for the Diagnosis and Treatment of Equine Metabolic Syndrome (EMS); University of Tufts: Medford, MA, USA, 2020. [Google Scholar]
- Jocelyn, N.A.; Harris, P.A.; Menzies-Gow, N.J. Effect of varying the dose of corn syrup on the insulin and glucose response to the oral sugar test. Equine Vet. J. 2018, 50, 836–841. [Google Scholar] [CrossRef]
- Warnken, T.; Huber, K.; Feige, K. Comparison of three different methods for the quantification of equine insulin. BMC Vet. Res. 2016, 12, 196. [Google Scholar] [CrossRef] [PubMed]
- Jamaluddin, M.S.; Weakley, S.M.; Yao, Q.; Chen, C. Resistin: Functional roles and therapeutic considerations for cardiovascular disease. Br. J. Pharmacol. 2012, 165, 622–632. [Google Scholar] [CrossRef]
- Derosa, G.; Fogari, E.; Angelo, A.D.; Bianchi, L.; Bonaventura, A.; Romano, D.; Maffioli, P. Adipocytokine Levels in Obese and Non-obese Subjects: An Observational Study. Inflammation 2013, 36, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Tsuji, H.; Ishida-Yamamoto, A.; Iizuka, H. Serum level of adiponectin increases and those of leptin and resistin decrease following the treatment of psoriasis. J. Dermatol. 2013, 40, 475–476. [Google Scholar] [CrossRef]
- Koch, A.; Gressner, O.A.; Sanson, E.; Tacke, F.; Trautwein, C. Serum resistin levels in critically ill patients are associated with inflammation, organ dysfunction and metabolism and may predict survival of non-septic patients. Crit. Care 2009, 13, R95. [Google Scholar] [CrossRef] [PubMed]
- Sundén-Cullberg, J.; Nyström, T.; Lee, M.L.; Mullins, G.E.; Tokics, L.; Andersson, J.; Norrby-Teglund, A.; Treutiger, C.J. Pronounced elevation of resistin correlates with severity of disease in severe sepsis and septic shock. Crit. Care Med. 2007, 35, 1536–1542. [Google Scholar] [CrossRef]
- Tripathi, D.; Kant, S.; Pandey, S.; Ehtesham, N.Z. Resistin in metabolism, inflammation, and disease. FEBS J. 2020, 287, 3141–3149. [Google Scholar] [CrossRef]
- Kaser, S.; Kaser, A.; Sandhofer, A.; Ebenbichler, C.F.; Tilg, H.; Patsch, J.R. Resistin messenger-RNA expression is increased by proinflammatory cytokines in vitro. Biochem. Biophys. Res. Commun. 2003, 309, 286–290. [Google Scholar] [CrossRef]
- Codoñer-Franch, P.; Alonso-Iglesias, E. Resistin: Insulin resistance to malignancy. Clin. Chim. Acta 2015, 438, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Lehrke, M.; Reilly, M.P.; Millington, S.C.; Iqbal, N.; Rader, D.J.; Lazar, M.A. An inflammatory cascade leading to hyperresistinemia in humans. PLoS Med. 2004, 1, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.D.; Mehta, N.N.; Wolfe, M.L.; Hinkle, C.C.; Pruscino, L.; Comiskey, L.L.; Tabita-Martinez, J.; Sellers, K.F.; Rickels, M.R.; Ahima, R.S.; et al. Innate immunity modulates adipokines in humans. J. Clin. Endocrinol. Metab. 2007, 92, 2272–2279. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.R.; Lazar, M.A. Human Resistin: Found in Translation From Mouse to Man. Trends Endocrinol. Metab. 2011, 22, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Pine, G.M.; Batugedara, H.M.; Nair, M.G. Here, there and everywhere: Resistin-like molecules in infection, inflammation, and metabolic disorders. Cytokine 2018, 110, 442–451. [Google Scholar] [CrossRef]
- Huang, X.; Yang, Z. Resistin’s, obesity and insulin resistance: The continuing disconnect between rodents and humans. J. Endocrinol. Investig. 2016, 39, 607–615. [Google Scholar] [CrossRef]
- Filková, M.; Haluzík, M.; Gay, S.; Šenolt, L. The role of resistin as a regulator of inflammation: Implications for various human pathologies. Clin. Immunol. 2009, 133, 157–170. [Google Scholar] [CrossRef]
- Calabrò, P.; Golia, E.; Maddaloni, V.; Malvezzi, M.; Casillo, B.; Marotta, C.; Calabrò, R.; Golino, P. Adipose tissue-mediated inflammation: The missing link between obesity and cardiovascular disease? Intern. Emerg. Med. 2009, 4, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Jamaluddin, M.S.; Yan, S.; Lü, J.; Liang, Z.; Yao, Q.; Chen, C. Resistin increases monolayer permeability of human coronary artery endothelial cells. PLoS ONE 2013, 8, e84576. [Google Scholar] [CrossRef]
- Utzschneider, K.M.; Carr, D.B.; Tong, J.; Wallace, T.M.; Hull, R.L.; Zraika, S.; Xiao, Q.; Mistry, J.S.; Retzlaff, B.M.; Knopp, R.H.; et al. Resistin is not associated with insulin sensitivity or the metabolic syndrome in humans. Diabetologia 2005, 48, 2330–2333. [Google Scholar] [CrossRef]
- Højbjerre, L.; Sonne, M.P.; Alibegovic, A.C.; Nielsen, N.B.; Dela, F.; Vaag, A.; Bruun, J.M.; Stallknecht, B. Impact of physical inactivity on adipose tissue low-grade inflammation in first-degree relatives of type 2, diabetic patients. Diabetes Care 2011, 34, 2265–2272. [Google Scholar] [CrossRef] [PubMed]
- Janke, J.; Engeli, S.; Gorzelniak, K.; Luft, F.C.; Sharma, A.M. Resistin Gene Expression in Human Adipocytes Is Not Related to Insulin Resistance. Obes. Res. 2002, 10, 1–5. [Google Scholar] [CrossRef]
- Al-Harithy, R.N.; Al-Ghamdi, S. Serum resistin, adiposity and insulin resistance in Saudi women with type 2 diabetes mellitus. Ann. Saudi Med. 2005, 25, 283–287. [Google Scholar] [CrossRef]
- Zaidi, S.I.Z.; Shirwany, T.A.K. Relationship of serum resistin with insulin resistance and obesity. J. Ayub Med. Coll. Abbottabad 2015, 27, 552–555. [Google Scholar] [PubMed]
- Gregor, M.F.; Hotamisligil, G.S. Inflammatory Mechanisms in Obesity. Annu. Rev. Immunol. 2011, 29, 415–445. [Google Scholar] [CrossRef]
- Pleasant, R.S.; Suagee, J.K.; Thatcher, C.D.; Elvinger, F.; Geor, R.J. Adiposity, plasma insulin, leptin, lipids, and oxidative stress in mature light breed horses. J. Vet. Intern. Med. 2013, 27, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Suagee, J.K.; Corl, B.A.; Crisman, M.V.; Hulver, M.W.; McCutcheon, L.J.; Geor, R.J. Effects of acute hyperinsulinemia on inflammatory proteins in horses. Vet. Immunol. Immunopathol. 2011, 142, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Rasouli, N.; Kern, P.A. Adipocytokines and the metabolic complications of obesity. J. Clin. Endocrinol. Metab. 2008, 93, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, N.; Seshadri, P.; Stern, L.; Loh, J.; Kundu, S.; Jafar, T.; Samaha, F.F. Serum resistin is not associated with obesity or insulin resistance in humans. Eur. Rev. Med. Pharmacol. Sci. 2005, 9, 161–165. [Google Scholar]
- Azzam, E.Z.; Elneily, D.; Elgayar, N.; Elfatatry, A.; Saad, M. Serum levels of resistin and its relationship with some pro-inflammatory cytokines in a cohort of Egyptian patients with Alzheimer’s disease. Endocr. Metab. Sci. 2020, 1, 100054. [Google Scholar] [CrossRef]
- De Luis, D.A.; Sagrado, M.G.; Conde, R.; Aller, R.; Izaola, O. Resistin levels and inflammatory markers in patients with morbid obesity. Nutr Hosp. 2010, 25, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Melone, M.; Wilsie, L.; Palyha, O.; Strack, A.; Rashid, S. Discovery of a new role of human resistin in hepatocyte low-density lipoprotein receptor suppression mediated in part by proprotein convertase subtilisin/kexin type 9. J. Am. Coll. Cardiol. 2012, 59, 1697–1705. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.H.; Li, L.; Li, J.Y.; Song, Q.; Jin, M.M.; Liu, J.X. Serum resistin positively correlates with serum lipids, but not with insulin resistance, in first-degree relatives of type-2 diabetes patients: An observational study in China. Medicine 2017, 96, e6622. [Google Scholar] [CrossRef]
- Costandi, J.; Melone, M.; Zhao, A.; Rashid, S. Human Resistin Stimulates Hepatic Overproduction of Atherogenic ApoB-Containing Lipoprotein Particles by Enhancing ApoB Stability and Impairing Intracellular Insulin Signaling. Circ. Res. 2011, 108, 727–742. [Google Scholar] [CrossRef] [PubMed]
- Cappai, M.G.; Lunesu, M.G.A.; Accioni, F.; Liscia, M.; Pusceddu, M.; Burrai, L.; Nieddu, M.; Dimauro, C.; Boatto, G.; Pinna, W. Blood serum retinol levels in Asinara white donkeys reflect albinism-induced metabolic adaptation to photoperiod at Mediterranean latitudes. Ecol. Evol. 2017, 7, 390–398. [Google Scholar] [CrossRef] [PubMed]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuentes-Romero, B.; Muñoz-Prieto, A.; Cerón, J.J.; Martín-Cuervo, M.; Iglesias-García, M.; Aguilera-Tejero, E.; Díez-Castro, E. Measurement of Plasma Resistin Concentrations in Horses with Metabolic and Inflammatory Disorders. Animals 2022, 12, 77. https://doi.org/10.3390/ani12010077
Fuentes-Romero B, Muñoz-Prieto A, Cerón JJ, Martín-Cuervo M, Iglesias-García M, Aguilera-Tejero E, Díez-Castro E. Measurement of Plasma Resistin Concentrations in Horses with Metabolic and Inflammatory Disorders. Animals. 2022; 12(1):77. https://doi.org/10.3390/ani12010077
Chicago/Turabian StyleFuentes-Romero, Beatriz, Alberto Muñoz-Prieto, José J. Cerón, María Martín-Cuervo, Manuel Iglesias-García, Escolástico Aguilera-Tejero, and Elisa Díez-Castro. 2022. "Measurement of Plasma Resistin Concentrations in Horses with Metabolic and Inflammatory Disorders" Animals 12, no. 1: 77. https://doi.org/10.3390/ani12010077
APA StyleFuentes-Romero, B., Muñoz-Prieto, A., Cerón, J. J., Martín-Cuervo, M., Iglesias-García, M., Aguilera-Tejero, E., & Díez-Castro, E. (2022). Measurement of Plasma Resistin Concentrations in Horses with Metabolic and Inflammatory Disorders. Animals, 12(1), 77. https://doi.org/10.3390/ani12010077