
Causes, Effects and Methods of Monitoring Gas Exchange Disturbances during Equine General Anaesthesia


Abstract
Simple Summary
Abstract
1. Introduction
Chemical Regulation of Ventilation
2. Reasons for Ventilation Impairment during Anaesthesia
2.1. Hypoventilation
2.2. Atelectasis
2.3. V/Q Mismatch and Shunting
2.4. Dead Space
3. Influence of Hypoxaemia and Hypoxia on Haemodynamics—The Respiratory System after Recovery
3.1. Haemodynamics
3.2. Post-Operative Period
3.3. Respiratory System
4. Influence of Hypercapnia
5. Monitoring of Gas Disturbances
- Observation of mucous membrane colour and capillary refill time
- Pulse oximetry
- Blood gas measurement
- Near infrared spectroscopy (NIRS)
- Observation of respiratory rate and rhythm
- Spirometry
- Blood gas measurement
- Capnography
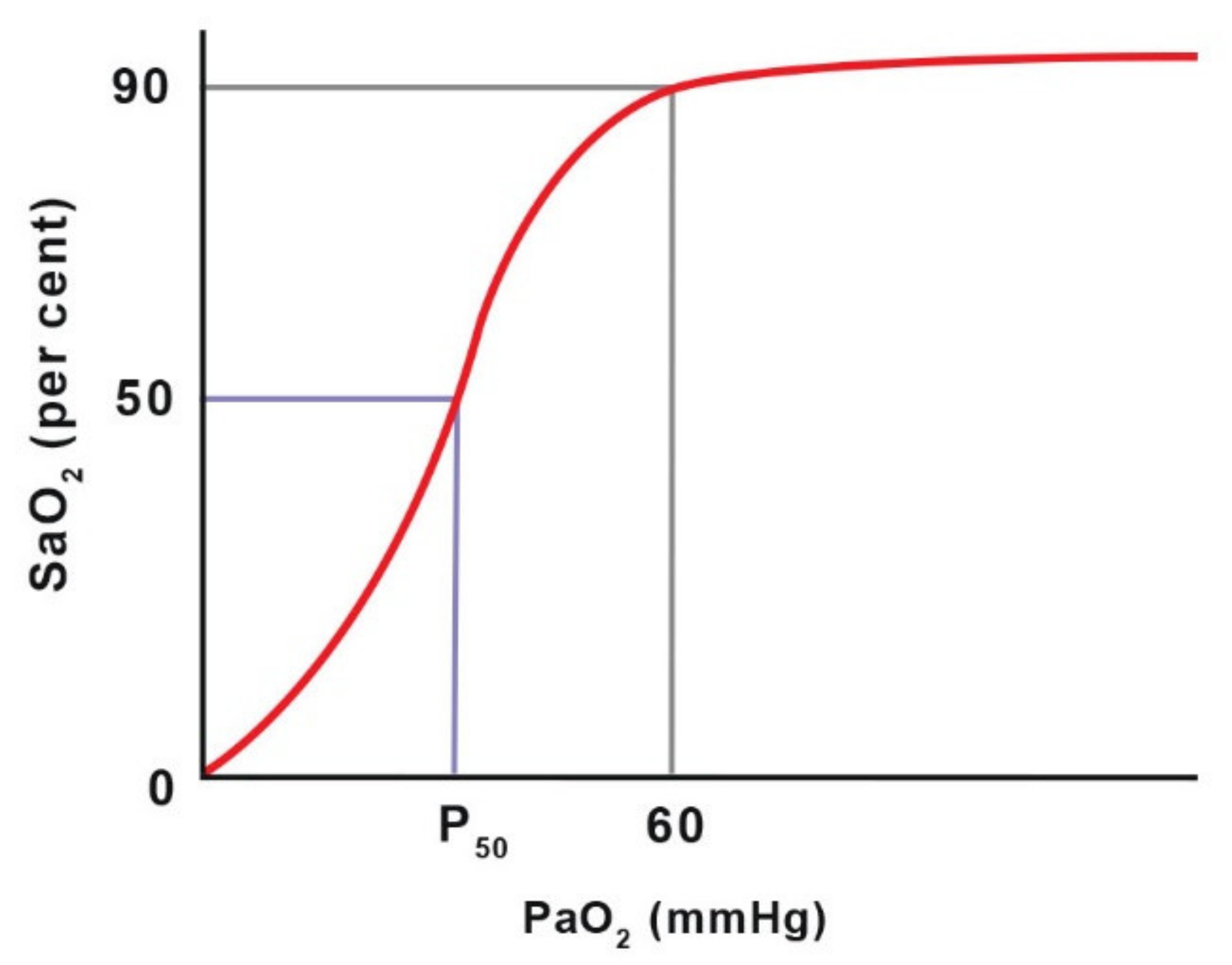
5.1. Pulse Oximetry
5.2. Near Infrared Spectroscopy (NIRS) ß
5.3. Blood Gas Measurements
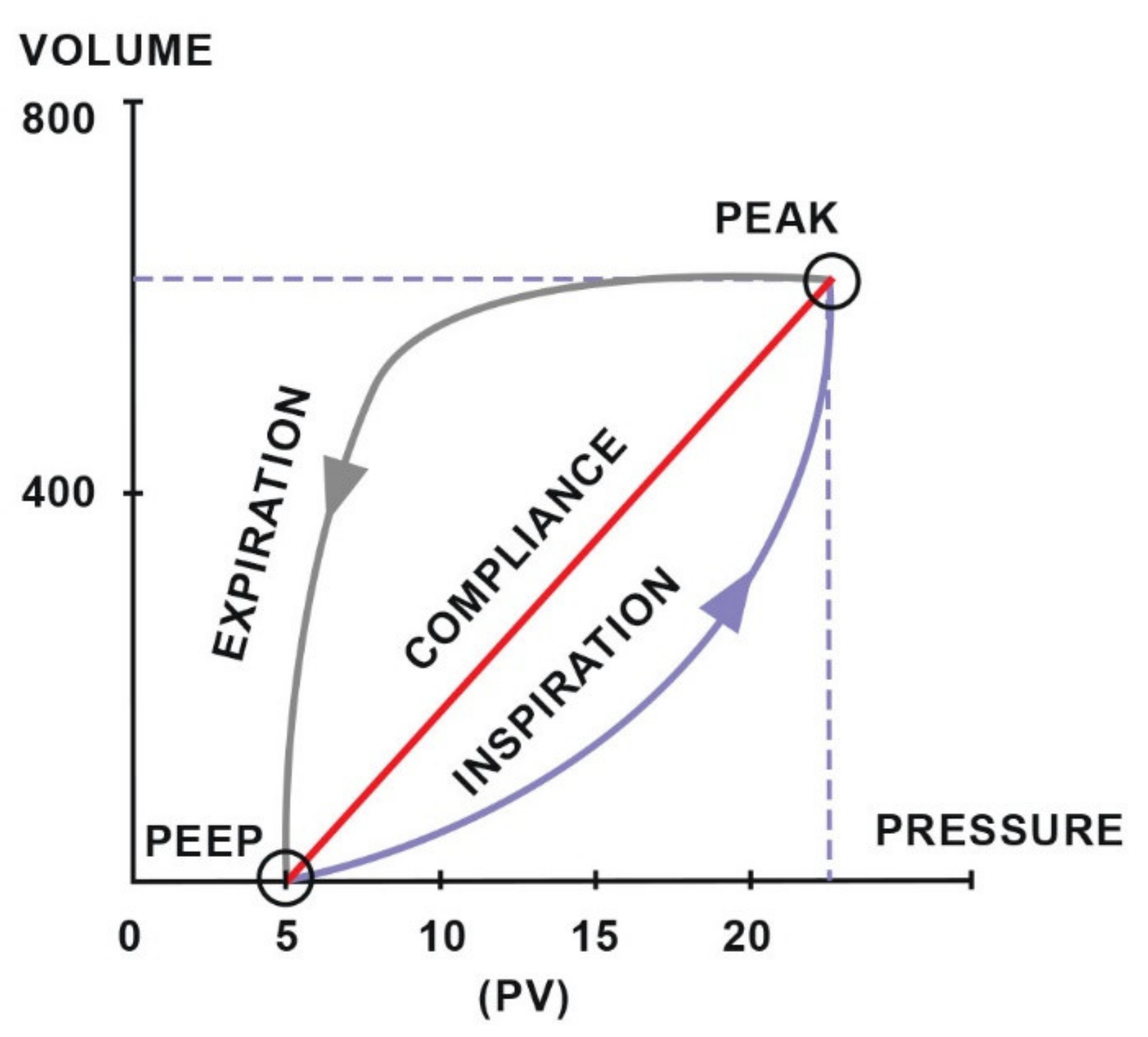
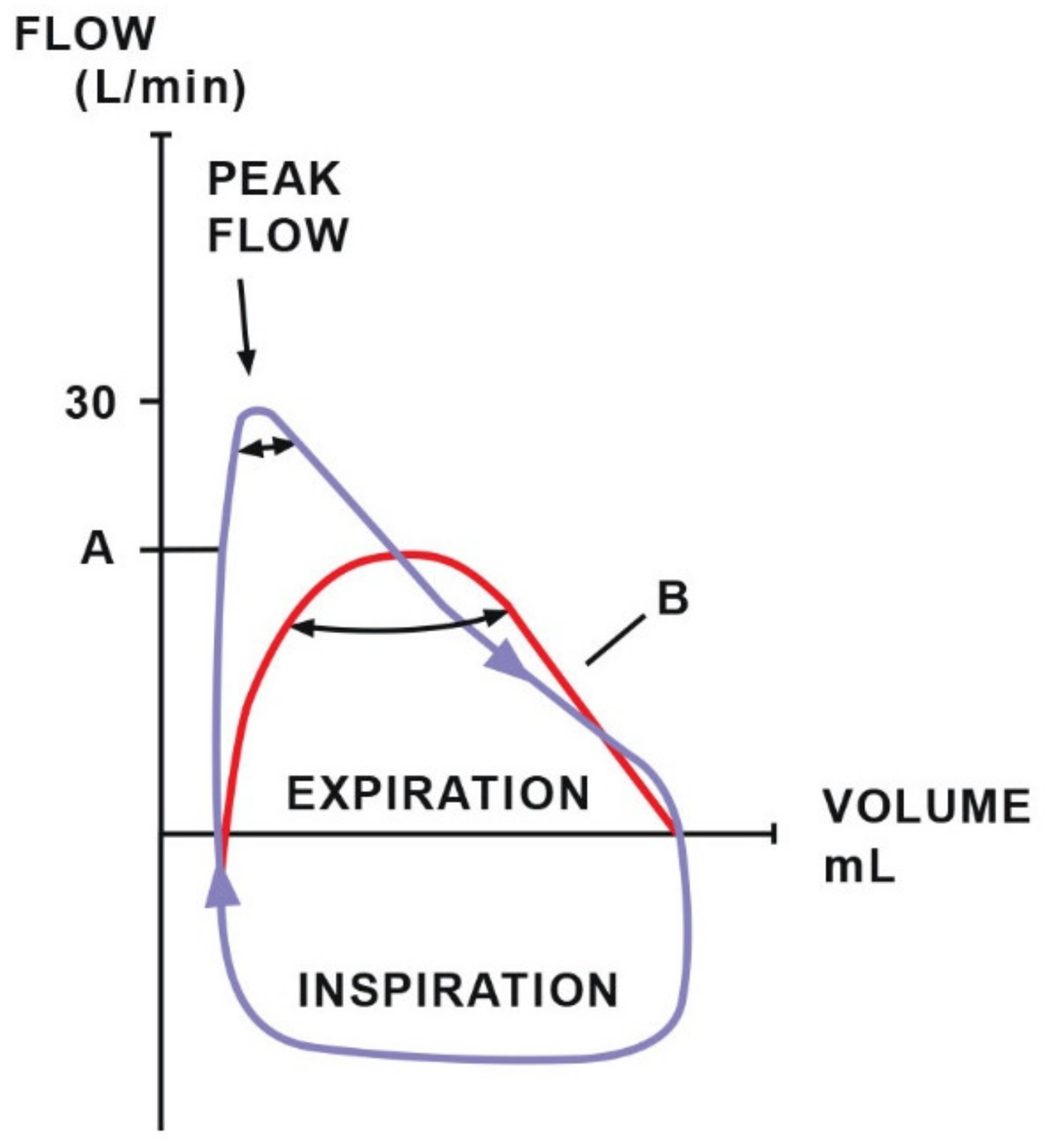
5.4. Spirometry
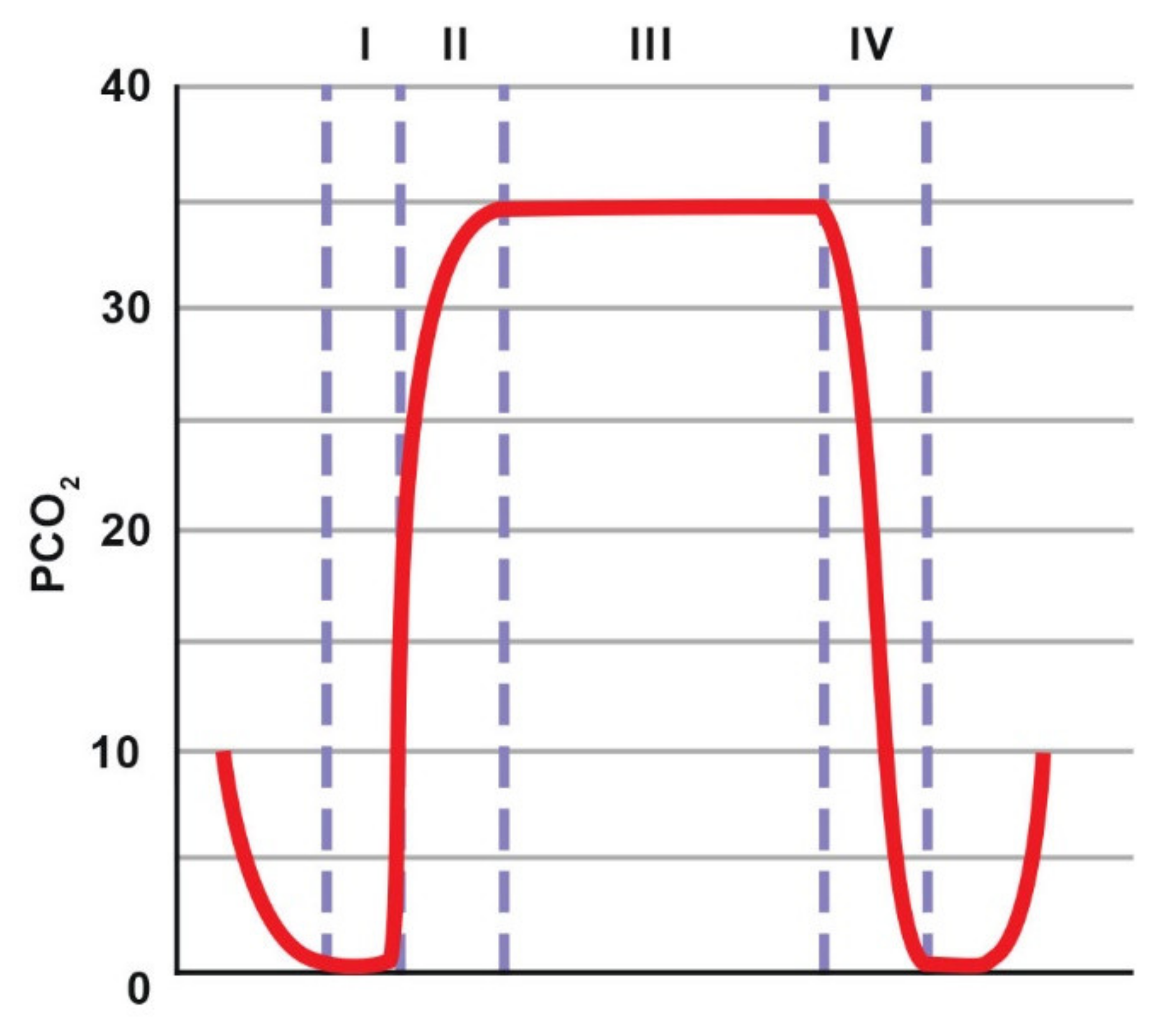
5.5. Capnography
6. Summary
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnston, G.M.; Eastment, J.K.; Wood, J.L.N.; Taylor, P.M. The confidential enquiry into perioperative equine fatalities (CEPEF): Mortality results of Phases 1 and 2. Vet. Anaesth. Analg. 2002, 29, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Brodbelt, D. Perioperative mortality in small animal anaesthesia. Vet. J. 2009, 182, 152–161. [Google Scholar] [CrossRef]
- Koenig, J.; McDonell, W.; Valverde, A. Accuracy of Pulse Oximetry and Capnography in Healthy and Compromised Horses during Spontaneous and Controlled Ventilation. Can. J. Vet. Res. 2003, 67, 169–174. [Google Scholar] [PubMed]
- Gilbert, H.C.; Veder, J.S. Monitoring the anesthetized patient. In Clinical Anesthesia; J. B. Lippincott: Philadephia, PA, USA, 1992; pp. 742–743. [Google Scholar]
- Hubbell, J.A.E.; Muir, W.W. Oxygenation, oxygen delivery and anaesthesia in the horse. Equine Vet. J. 2014, 47, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Nyman, G.; Hedenstierna, G. Ventilation-perfusion relationships in the anaesthetised horse. Equine Vet. J. 1989, 21, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Grosenbaugh, A.D.; Muir, W.W. Cardiorespiratory effects of sevoflurane, isoflurane, and halothane anesthesia in horses. Am. J. Veter Res. 1998, 59, 101–106. [Google Scholar]
- Wagner, P.D. The physiological basis of pulmonary gas exchange: Implications for clinical interpretation of arterial blood gases. Eur. Respir. J. 2014, 45, 227–243. [Google Scholar] [CrossRef] [PubMed]
- Hall, L.W. II Disturbances of Cardiopulmonary Function in Anaesthetised Horses. Equine Vet. J. 1971, 3, 95–98. [Google Scholar] [CrossRef]
- Dupont, J.; Serteyn, D.; Sandersen, C. Prolonged Recovery from General Anesthesia Possibly Related to Persistent Hypoxemia in a Draft Horse. Front. Vet. Sci. 2018, 5, 5. [Google Scholar] [CrossRef]
- McMurphy, R.M.; Cribb, P.H. Alleviation of postanesthetic hypoxemia in the horse. Can. Vet. J. La Rev. Vet. Can. 1989, 30, 37–41. [Google Scholar]
- Yoon, S.; Zuccarello, M.; Rapoport, R.M. pCO2 and pH regulation of cerebral blood flow. Front. Physiol. 2012, 3, 365. [Google Scholar] [CrossRef]
- Bayly, W.M.; Hodgson, D.R.; Schulz, D.A.; Dempsey, J.A.; Gollnick, P.D. Exercise-induced hypercapnia in the horse. J. Appl. Physiol. 1989, 67, 1958–1966. [Google Scholar] [CrossRef] [PubMed]
- Muir, W.W.; Moore, A.C.; Hamlin, R.L. Ventilatory alterations in normal horses in response to changes in inspired oxygen and carbon dioxide. Am. J. Vet. Res. 1975, 36, 155–159. [Google Scholar]
- Pelletier, N.; Leith, D.E. Ventilation and carbon dioxide exchange in exercising horses: Effect of inspired oxygen fraction. J. Appl. Physiol. 1995, 78, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.E. The importance of hypoxaemia and hypercapnia in anaesthetised horses. Equine Vet. Educ. 1993, 5, 207–211. [Google Scholar] [CrossRef]
- Grandy, J.L.; Steffey, E.P.; Hodgson, D.S. Arterial Hypotension and the Development of Postanesthetic Myopathy in Halotane-Anaesthetized Horses. Am. J. Vet. Res. 1987, 48, 192–197. [Google Scholar] [PubMed]
- Brosnan, R.J. Inhaled Anesthetics in Horses. Veterinary Clinics of North. Am. Equine Pract. 2013, 29, 69–87. [Google Scholar] [CrossRef]
- Nyman, G.; Grubb, T.L.; Heinonen, E.; Frendin, J.; Edner, A.; Malavasi, L.M.; Frostell, C.; Högman, M. Pulsed delivery of inhaled nitric oxide counteracts hypoxaemia during 2.5 hours of inhalation anaesthesia in dorsally recumbent horses. Vet. Anaesth. Analg. 2012, 39, 480–487. [Google Scholar] [CrossRef]
- Koterba, A.M.; Kosch, P.C.; Beech, J.; Whitlock, T. Breathing strategy of the adult horse (Equus caballus) at rest. J. Appl. Physiol. 1988, 64, 337–346. [Google Scholar] [CrossRef]
- Sarkar, M.; Niranjan, N.; Banyal, P. Mechanisms of hypoxemia. Lung India 2017, 34, 47. [Google Scholar] [CrossRef]
- Saraswat, V. Effects of anaesthesia techniques and drugs on pulmonary function. Indian J. Anaesth. 2015, 59, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Brosnan, R.J.; Steffey, E.P.; Escobar, A. Effects of hypercapnic hyperpnea on recovery from isoflurane or sevoflurane anesthesia in horses. Vet. Anaesth. Analg. 2012, 39, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Nyman, G.; Funkquist, B.; Kvart, C.; Frostell, C.; Tokics, L.; Strandberg, Å.; Lundquist, H.; Lundh, B.; Brismar, B.; Hedenstierna, G. Atelectasis causes gas exchange impairment in the anaesthetised horse. Equine Vet. J. 1990, 22, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Mosing, M.; Senior, J.M. Maintenance of equine anaesthesia over the last 50 years: Controlled inhalation of volatile anaesthetics and pulmonary ventilation. Equine Vet. J. 2018, 50, 282–291. [Google Scholar] [CrossRef]
- Joyce, C.J.; Baker, A.B. What is the Role of Absorption Atelectasis in the Genesis of Perioperative Pulmonary Collapse? Anaesth. Intensive Care 1995, 23, 691–696. [Google Scholar] [CrossRef]
- Guedes, A. Blood gases. In Interpretation of Equine Laboratory Diagnostics; John Wiley & Sons: Hoboken, NJ, USA, 2018; pp. 57–65. [Google Scholar]
- Dobson, A.; Gleed, R.D.; Meyer, R.E.; Stewart, B.J. Changes in Blood Flow Distribution in Equine Lungs Induced by Anaesthesia. Q. J. Exp. Physiol. 1985, 70, 283–297. [Google Scholar] [CrossRef] [PubMed]
- Trim, C.M.; Wan, P.Y. Hypoxaemia during anaesthesia in seven horses with colic. J. Assoc. Vet. Anaesth. 1990, 17, 45–49. [Google Scholar] [CrossRef]
- Mosing, M.; Böhm, S.H.; Rasis, A.; Hoosgood, G.; Auer, U.; Tusman, G.; Bettschart-Wolfensberger, R.; Schramel, J.P. Physiologic Factors Influencing the Arterial-To-End-Tidal CO2 Difference and the Alveolar Dead Space Fraction in Spontaneously Breathing Anesthetised Horses. Front. Vet. Sci. 2018, 5, 58. [Google Scholar] [CrossRef]
- Drábková, Z.; Schramel, J.P.; Kabeš, R. Determination of physiological dead space in anaesthetized horses: A method-comparison study. Vet. Anaesth. Analg. 2018, 45, 73–77. [Google Scholar] [CrossRef]
- Gallivan, G.; McDonell, W.; Forrest, J. Comparative ventilation and gas exchange in the horse and the cow. Res. Vet. Sci. 1989, 46, 331–336. [Google Scholar] [CrossRef]
- Robertson, H.T. Erratum: Dead Space: The Physiology of Wasted Ventilation. Eur. Respir J. 2015, 45, 1704–1716. [Google Scholar] [CrossRef] [PubMed]
- Edner, A.; Nyman, G.; Essén-Gustavsson, B. The effects of spontaneous and mechanical ventilation on central cardiovascular function and peripheral perfusion during isoflurane anaesthesia in horses. Vet. Anaesth. Analg. 2005, 32, 136–146. [Google Scholar] [CrossRef]
- Ambrósio, A.M.; Ida, K.K.; Souto, M.T.; Oshiro, A.H.; Fantoni, D.T. Effects of positive end-expiratory pressure titration on gas exchange, respiratory mechanics and hemodynamics in anesthetized horses. Vet. Anaesth. Analg. 2013, 40, 564–572. [Google Scholar] [CrossRef]
- Kurt Grimm, J.A.; Lamont, L.A.; Tranquilli, W.J.; Greene, S.A.; Robertson, S.A.; McDonell, W.N.; Kerr, C.L. Section 5 Respiratory System Veterinary Anesthesia and Analgesia: The Fifth Edition of Lumb and 27 Physiology, Pathophysiology, and Anesthetic Management of Patients with Respiratory Disease; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Abboud, F.M.; Heistad, D.D.; Mark, A.L.; Schmid, P.G. Reflex control of the peripheral circulation. Prog. Cardiovasc. Dis. 1976, 18, 371–403. [Google Scholar] [CrossRef]
- Auckburally, A.; Nyman, G. Review of hypoxaemia in anaesthetized horses: Predisposing factors, consequences and management. Vet. Anaesth. Analg. 2017, 44, 397–408. [Google Scholar] [CrossRef]
- Rosenberg, J.; Rasmussen, V.; von Jessen, F.; Ullstad, T.; Kehlet, H. Late Postoperative Episodic and Constant Hypoxaemia and Associated ECG Abnormalities. Br. J. Anaesth. 1990, 65, 684–691. [Google Scholar] [CrossRef]
- Cargill, R.; Kiely, D.G.; Lipworth, B.J. Adverse Effects of Hypoxaemia on Diastolic Filling in Humans. Clin. Sci. 1995, 89, 165–169. [Google Scholar] [CrossRef]
- Lindsay, W.A.; Robinson, G.M.; Brunson, D.B. Induction of Equine Postanaesthetic Myositis after Halotane-Induced Hypotension. Am. J. Vet. Res. 1989, 50, 404–410. [Google Scholar] [PubMed]
- Romer, L.M.; Haverkamp, H.C.; Lovering, A.; Pegelow, D.F.; Dempsey, J.A. Effect of exercise-induced arterial hypoxemia on quadriceps muscle fatigue in healthy humans. Am. J. Physiol. Integr. Comp. Physiol. 2006, 290, R365–R375. [Google Scholar] [CrossRef] [PubMed]
- Costa-Farré, C.; Prades, M.; Ribera, T.; Valero, O.; Taurá, P. Does intraoperative low arterial partial pressure of oxygen increase the risk of surgical site infection following emergency exploratory laparotomy in horses? Vet. J. 2014, 200, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Obert, R.; Reif, G.; Kça, Z.A.; Rnst, P.; Eter, E.; Orn, H.; Ndrea, A.; Urz, K.; Aniel, D.; Essler, I.S. Supplemental Perioperative Oxygen to Reduce the Incidence of Surgical-Wound Infection Abstract Background Destruction by Oxidation, or Oxidative. N. Engl. J. Med. 2000, 342, 161–167. [Google Scholar]
- Moore, J.N.; A White, N.; Berg, J.N.; Trim, C.M.; Garner, H.E. Endotoxemia following experimental intestinal strangulation obstruction in ponies. Can. J. Comp. Med. Rev. Can. Med. Comp. 1981, 45, 330–332. [Google Scholar]
- Nelson, D.P.; Samsel, R.W.; Wood, L.D.; Schumacker, P.T. Pathological supply dependence of systemic and intestinal O2 uptake during endotoxemia. J. Appl. Physiol. 1988, 64, 2410–2419. [Google Scholar] [CrossRef]
- Trim, C.M. Monitoring during anaesthesia: Techniques and interpretation. Equine Veter Educ. 2010, 15, 30–40. [Google Scholar] [CrossRef]
- Laurenza, C.; Ansart, L.; Portier, K. Risk Factors of Anesthesia-Related Mortality and Morbidity in One Equine Hospital: A Retrospective Study on 1,161 Cases Undergoing Elective or Emergency Surgeries. Front. Veter Sci. 2020, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Holcombe, S.J. Neuromuscular Regulation of the Larynx and Nasopharynx in the Horse. AAEP Proc. 1998, 44, 26–29. [Google Scholar]
- Dugdale, A.H.; Taylor, P.M. Equine anaesthesia-associated mortality: Where are we now? Vet. Anaesth. Analg. 2016, 43, 242–255. [Google Scholar] [CrossRef]
- Lumb, A.B.; Slinger, P. Hypoxic Pulmonary Vasoconstriction: Physiology and Anesthetic Implications. Anesthesiology 2015, 122, 932–946. [Google Scholar] [CrossRef]
- Nagendran, J.; Stewart, K.; Hoskinson, M.; Archer, S.L. An anesthesiologist’s guide to hypoxic pulmonary vasoconstriction: Implications for managing single-lung anesthesia and atelectasis. Curr. Opin. Anaesthesiol. 2006, 19, 34–43. [Google Scholar] [CrossRef]
- Khanna, A.K.; McDonell, W.N.; Dyson, D.H.; Taylor, P.M. Cardiopulmonary effects of hypercapnia during controlled intermittent positive pressure ventilation in the horse. Can. J. Vet. Res. Rev. Can. Rech. Vet. 1995, 59, 213–221. [Google Scholar]
- Crystal, G.J. Carbon Dioxide and the Heart: Physiology and Clinical Implications. Anesth. Analg. 2015, 121, 610–623. [Google Scholar] [CrossRef] [PubMed]
- Reiners, J.K.; Rossdeutscher, W.; Hopster, K.; Kästner, S. Development and clinical evaluation of a new sensor design for buccal pulse oximetry in horses. Equine Vet. J. 2017, 50, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Magdesian, K. Monitoring the critically ill equine patient. Vet. Clin. N. Am. Equine Pract. 2004, 20, 11–39. [Google Scholar] [CrossRef] [PubMed]
- Hubbell, J.A.E. A Review of the American College of Veterinary Anesthesiologists Guidelines for Anesthesia of Horses. AAEP Proc. 2008, 54, 48–53. [Google Scholar]
- Variane, G.F.T.; Chock, V.Y.; Netto, A.; Pietrobom, R.F.R.; Van Meurs, K.P. Simultaneous Near-Infrared Spectroscopy (NIRS) and Amplitude-Integrated Electroencephalography (aEEG): Dual Use of Brain Monitoring Techniques Improves Our Understanding of Physiology. Front. Pediatr. 2020, 7, 560. [Google Scholar] [CrossRef] [PubMed]
- Zoff, A.H.A.; Dugdale, A.; Scarabelli, S.; Rioja, E. Evaluation of pulse co-oximetry to determine haemoglobin saturation with oxygen and haemoglobin concentration in anaesthetized horses: A retrospective study. Vet. Anaesth. Analg. 2019, 46, 452–457. [Google Scholar] [CrossRef]
- Drewnowska, O.; Lisowska, B.; Turek, B. Equine general anesthesia monitoring–review of the methods and current knowledge. Med. Weter. 2018, 74, 67–77. [Google Scholar] [CrossRef]
- Barker, S.J.; Tremper, K.K. Pulse Oximetry: Applications and Limitations. Int. Anesthesiol. Clin. 1987, 25, 155–175. [Google Scholar] [CrossRef]
- Barton, L.J.; Devey, J.J.; Gorski, S.; Mainiero, L.; DeBehnke, D. Evaluation of Transmittance and Reflectance Pulse Oximetry in a Canine Model of Hypotension and Desaturation. J. Vet. Emerg. Crit. Care 1996, 6, 21–28. [Google Scholar] [CrossRef]
- Auckburally, A. Pulse oximetry and oxygenation assessment in small animal practice. Practice 2016, 38, 50–58. [Google Scholar] [CrossRef]
- Odette, O.; Cooley, K.G.; Johnson, R.A. Veterinary Anesthetic and Monitoring Equipment; Wiley & Sons: Hoboken, NJ, USA, 2018; pp. 223–233. [Google Scholar]
- Shah, N.; Ragaswamy, H.B.; Govindugari, K.; Estanol, L. Performance of three new-generation pulse oximeters during motion and low perfusion in volunteers. J. Clin. Anesthesia 2012, 24, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Tusman, G.; Bohm, S.H.; Suarez-Sipmann, F. Advanced Uses of Pulse Oximetry for Monitoring Mechanically Ventilated Patients. Anesthesia Analg. 2017, 124, 62–71. [Google Scholar] [CrossRef] [PubMed]
- McConnell, E.J.; Rioja, E.; Bester, L.; Sanz, M.G.; Fosgate, G.T.; Saulez, M.N. Use of near-infrared spectroscopy to identify trends in regional cerebral oxygen saturation in horses. Equine Vet. J. 2012, 45, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Gingold, B.M.; Killos, M.B.; Griffith, E.; Posner, L. Measurement of peripheral muscle oxygen saturation in conscious healthy horses using a near-infrared spectroscopy device. Vet. Anaesth. Analg. 2019, 46, 789–795. [Google Scholar] [CrossRef]
- Gay, A.N.; Lazar, D.A.; Stoll, B.; Naik-Mathuria, B.; Mushin, O.P.; Rodriguez, M.A.; Burrin, D.; Olutoye, O.O. Near-infrared spectroscopy measurement of abdominal tissue oxygenation is a useful indicator of intestinal blood flow and necrotizing enterocolitis in premature piglets. J. Pediatr. Surg. 2011, 46, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Murkin, J.M.; Arango, M. Near-infrared spectroscopy as an index of brain and tissue oxygenation. Br. J. Anaesth. 2009, 103, i3–i13. [Google Scholar] [CrossRef]
- Casati, A.; Spreafico, E.; Putzu, M.; Fanelli, G. New technology for noninvasive brain monitoring: Continuous cerebral oximetry. Minerva Anestesiol. 2006, 72. [Google Scholar]
- Greisen, G.; Leung, T.; Wolf, M. Has the time come to use near-infrared spectroscopy as a routine clinical tool in preterm infants undergoing intensive care? Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2011, 369, 4440–4451. [Google Scholar] [CrossRef]
- Cope, M.; Delpy, D.T.; Reynolds, E.O.R.; Wray, S.; Wyatt, J.; Van Der Zee, P. Methods of Quantitating Cerebral Near Infrared Spectroscopy Data. Adv. Exp. Med. Biol. 1988, 222, 183–189. [Google Scholar] [CrossRef]
- O’Leary, H.; Gregas, M.C.; Limperopoulos, C.; Zaretskaya, I.; Bassan, H.; Soul, J.; Di Salvo, D.N.; Du Plessis, A.J. Elevated Cerebral Pressure Passivity Is Associated with Prematurity-Related Intracranial Hemorrhage. Pediatrics 2009, 124, 302–309. [Google Scholar] [CrossRef]
- Armstead, W.M. Cerebral Blood Flow Autoregulation and Dysautoregulation. Anesthesiol. Clin. 2016, 34, 465–477. [Google Scholar] [CrossRef]
- Jeawon, S.S.; Katz, L.M.; Galvin, N.P.; Fogarty, U.M.; Duggan, V.E. Determination of reference intervals for umbilical cord arterial and venous blood gas analysis of healthy Thoroughbred foals. Theriogenology 2018, 118, 1–6. [Google Scholar] [CrossRef]
- Krueger, C.R.; Hackett, E.S.; Hess, A.M.; Mama, K.R. Evaluation of the Element point-of-care blood gas analyzer for use in horses. J. Veter Emerg. Crit. Care 2020, 30, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Castro, T.F.; González, F. Blood Gas Analysis in Mangalarga Marchador Horses with Colic Análisis de Gases Sanguíneos En Caballos Mangalarga Marchador Con Cólico. Rev. MVZ Córdoba 2015, 20, 4447–4454. [Google Scholar] [CrossRef][Green Version]
- Aguilera-Tejero, E.; Estepa, J.C.; López, I.; Mayer-Valor, R.; Rodriguez, M. Arterial blood gases and acid-base balance in healthy young and aged horses. Equine Vet. J. 1998, 30, 352–354. [Google Scholar] [CrossRef]
- Wong, D.M.; Hepworth-Warren, K.; Sponseller, B.T.; Howard, J.M.; Wang, C. Measured and calculated variables of global oxygenation in healthy neonatal foals. Am. J. Vet. Res. 2017, 78, 230–238. [Google Scholar] [CrossRef]
- Hackett, E.S.; Traub-Dargatz, J.L., Jr.; Tarr, S.F.; Dargatz, D.A. Arterial blood gas parameters of normal foals born at 1500 metres elevation. Equine Vet. J. 2009, 42, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, D.R. Blood Gas and Acid-Base Changes in the Neonatal Foal. Vet. Clin. N. Am. Equine Pract. 1987, 3, 617–629. [Google Scholar] [CrossRef]
- Picandet, V.; Jeanneret, S.; Lavoie, J.-P. Effects of Syringe Type and Storage Temperature on Results of Blood Gas Analysis in Arterial Blood of Horses. J. Vet. Intern. Med. 2007, 21, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Eastwood, G.M.; Suzuki, S.; Lluch, C.; Schneider, A.G.; Bellomo, R.; Candal, C.L. A pilot assessment of alpha-stat vs pH-stat arterial blood gas analysis after cardiac arrest. J. Crit. Care 2015, 30, 138–144. [Google Scholar] [CrossRef]
- Moens, Y. Mechanical Ventilation and Respiratory Mechanics During Equine Anesthesia. Veter Clin. N. Am. Equine Pract. 2013, 29, 51–67. [Google Scholar] [CrossRef]
- Moens, Y.P.S. Clinical application of continuous spirometry with a pitot-based flow meter during equine anaesthesia. Equine Vet. Educ. 2010, 22, 354–360. [Google Scholar] [CrossRef]
- Herholz, C. Clinical application of continuous spirometry during equine anaesthesia and in spontaneous breathing, awake horses. Equine Vet. Educ. 2010, 22, 361–363. [Google Scholar] [CrossRef]
- Schramel, J.P.; Wimmer, K.; Ambrisko, T.D.; Moens, Y.P. A novel flow partition device for spirometry during large animal anaesthesia. Vet. Anaesth. Analg. 2014, 41, 191–195. [Google Scholar] [CrossRef]
- Moens, Y.P.S.; Gootjes, P.; Ionita, J.; Heinonen, E.; Schatzmann, U. In vitro validation of a Pitot-based flow meter for the measurement of respiratory volume and flow in large animal anaesthesia. Vet. Anaesth. Analg. 2009, 36, 209–219. [Google Scholar] [CrossRef]
- Duke-Novakovski, T. Basics of monitoring equipment. Can. Vet. J. La Rev. Vet. Can. 2017, 58, 1200–1208. [Google Scholar]
- Thawley, V.; Waddell, L.S. Pulse Oximetry and Capnometry. Top. Companion Anim. Med. 2013, 28, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Bednarski, R.M.; Muir, W. Capnography in veterinary medicine. In Capnography; Cambridge University Press (CUP): Cambridge, UK, 2011; pp. 272–280. [Google Scholar]
- Hardman, J.; Curran, J.; Mahajan, R.P. End-tidal carbon dioxide measurement and breathing system filters. Anaesthesia 1997, 52, 646–648. [Google Scholar] [CrossRef]
- Hubbell, J.A.E. Review of Support of Ventilation in the Anesthetized Horse. AAEP Proc. 2010, 56, 33–37. [Google Scholar]
- Rainger, J.; Dart, C.; Perkins, N. Factors affecting the relationship between arterial and end-tidal carbon dioxide pressures in the anaesthetised horse. Aust. Vet. J. 2010, 88, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.E.; Jaffe, M.B. Capnographic waveforms in the mechanically ventilated patient. Respir. Care 2005, 50, 100. [Google Scholar] [PubMed]
- Siobal, M.S. Monitoring Exhaled Carbon Dioxide. Respir. Care 2016, 61, 1397–1416. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Function of the System | Measurement Method | Parameters Measured | Normal Values | ||
| Respiratory | Ventilation | Clinical exam | Respiratory rate (breaths/minute) | 6–20 | |
| Spirometry | Tidal volume (mL/kg) | 10 | |||
| Resistance (cm H2O/L/s) | <1.2 | ||||
| Compliance (L/cm H2O) | 2.4 | ||||
| Blood gas | Arterial blood pH PaCO2 (mm Hg) | 7.30–7.45 40–60 | |||
| Capnography | EtCO2 (mm Hg) | 30–50 | |||
| Respiratory and cardiovascular | Oxygenation | Pulse oximetry | SpO2 (%) | 93–100 | |
| Blood gas | PaO2 (mm Hg) | 100–500 (depending on FiO2) | |||
| NIRS | O3 (%) | 55–85 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefanik, E.; Drewnowska, O.; Lisowska, B.; Turek, B. Causes, Effects and Methods of Monitoring Gas Exchange Disturbances during Equine General Anaesthesia. Animals 2021, 11, 2049. https://doi.org/10.3390/ani11072049
Stefanik E, Drewnowska O, Lisowska B, Turek B. Causes, Effects and Methods of Monitoring Gas Exchange Disturbances during Equine General Anaesthesia. Animals. 2021; 11(7):2049. https://doi.org/10.3390/ani11072049
Chicago/Turabian StyleStefanik, Elżbieta, Olga Drewnowska, Barbara Lisowska, and Bernard Turek. 2021. "Causes, Effects and Methods of Monitoring Gas Exchange Disturbances during Equine General Anaesthesia" Animals 11, no. 7: 2049. https://doi.org/10.3390/ani11072049
APA StyleStefanik, E., Drewnowska, O., Lisowska, B., & Turek, B. (2021). Causes, Effects and Methods of Monitoring Gas Exchange Disturbances during Equine General Anaesthesia. Animals, 11(7), 2049. https://doi.org/10.3390/ani11072049