
Anti-HTLV-1/2 IgG Antibodies in the Breastmilk of Seropositive Mothers



Abstract
:1. Introduction
2. Materials and Methods
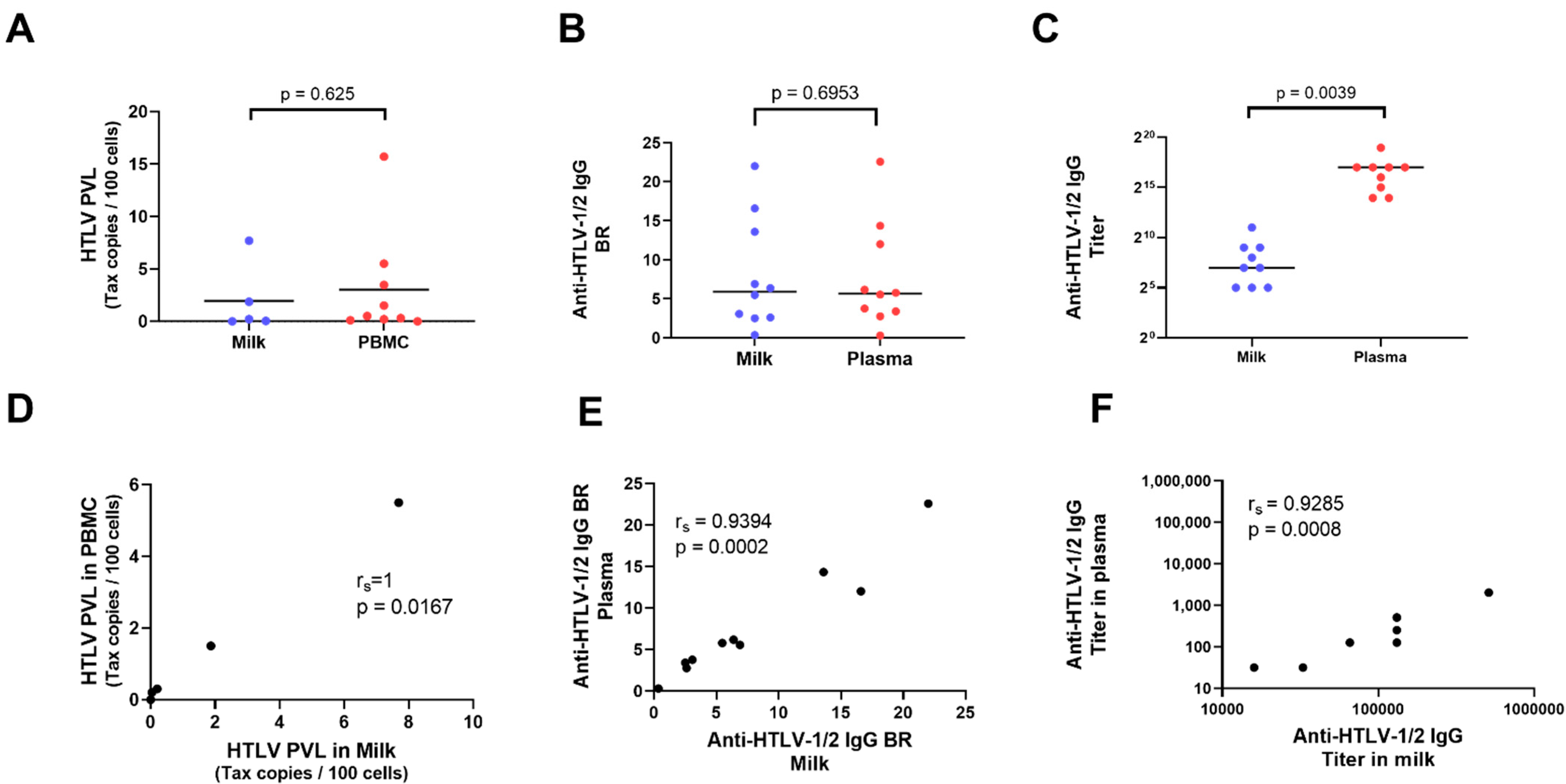
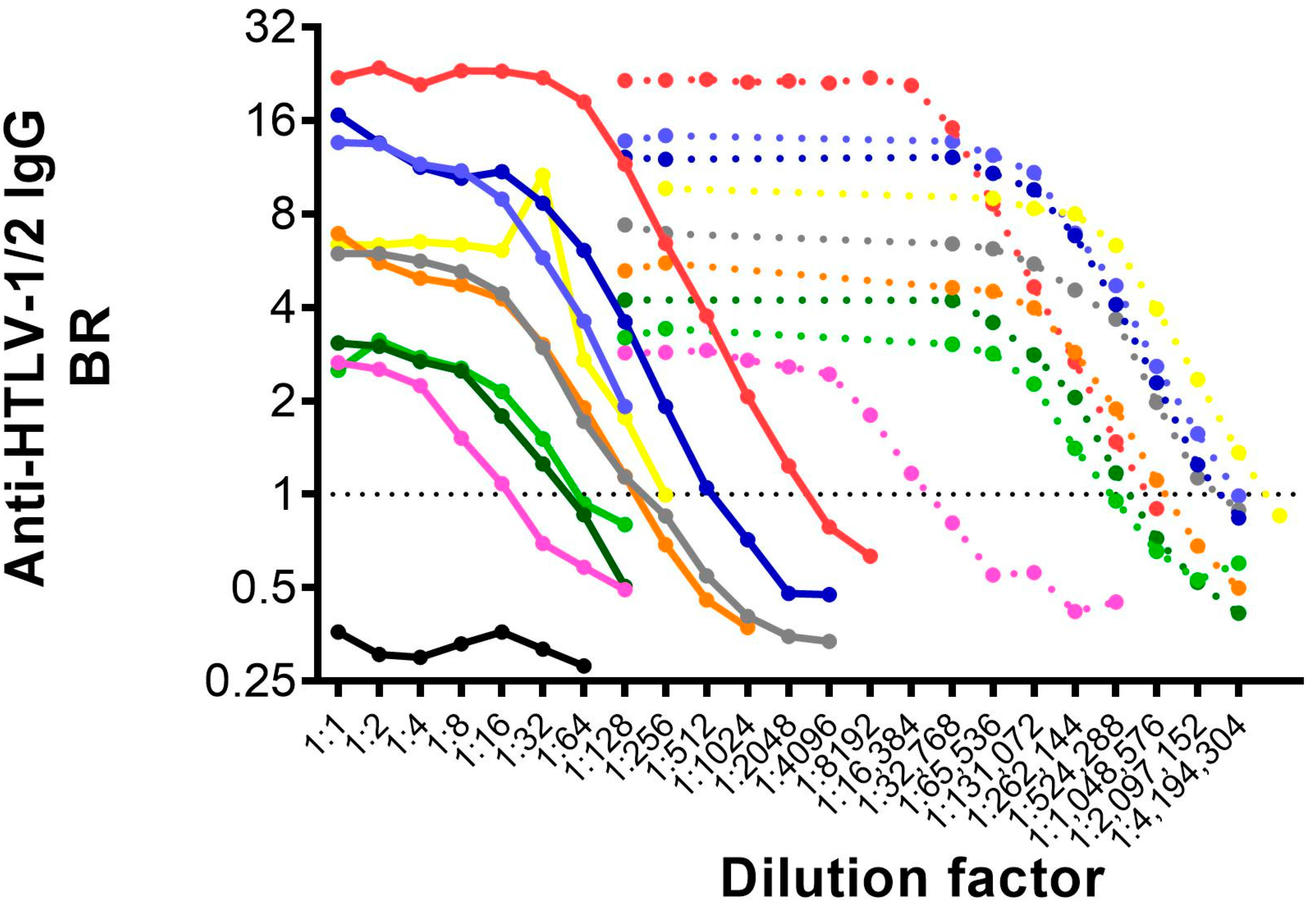
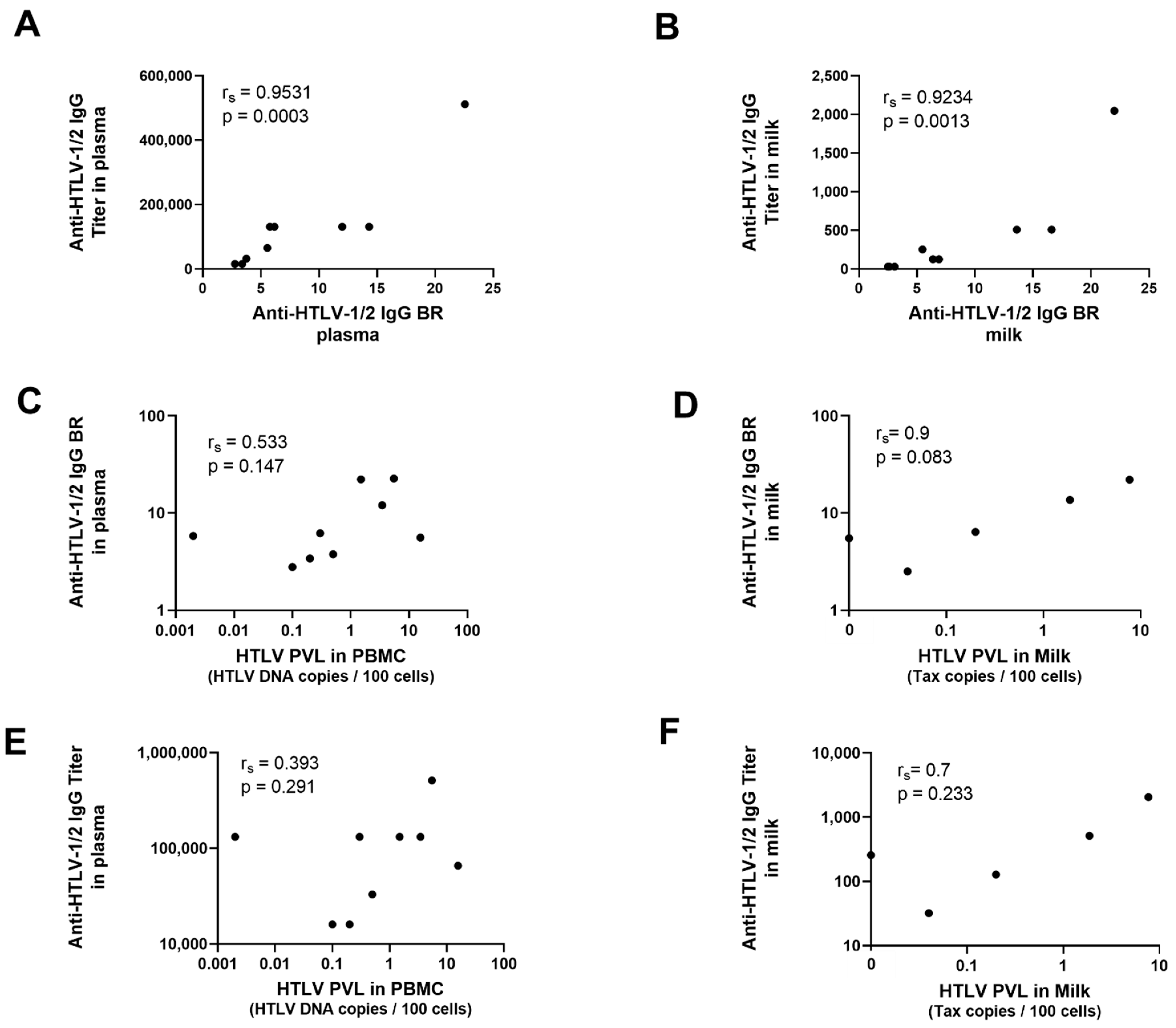
3. Results
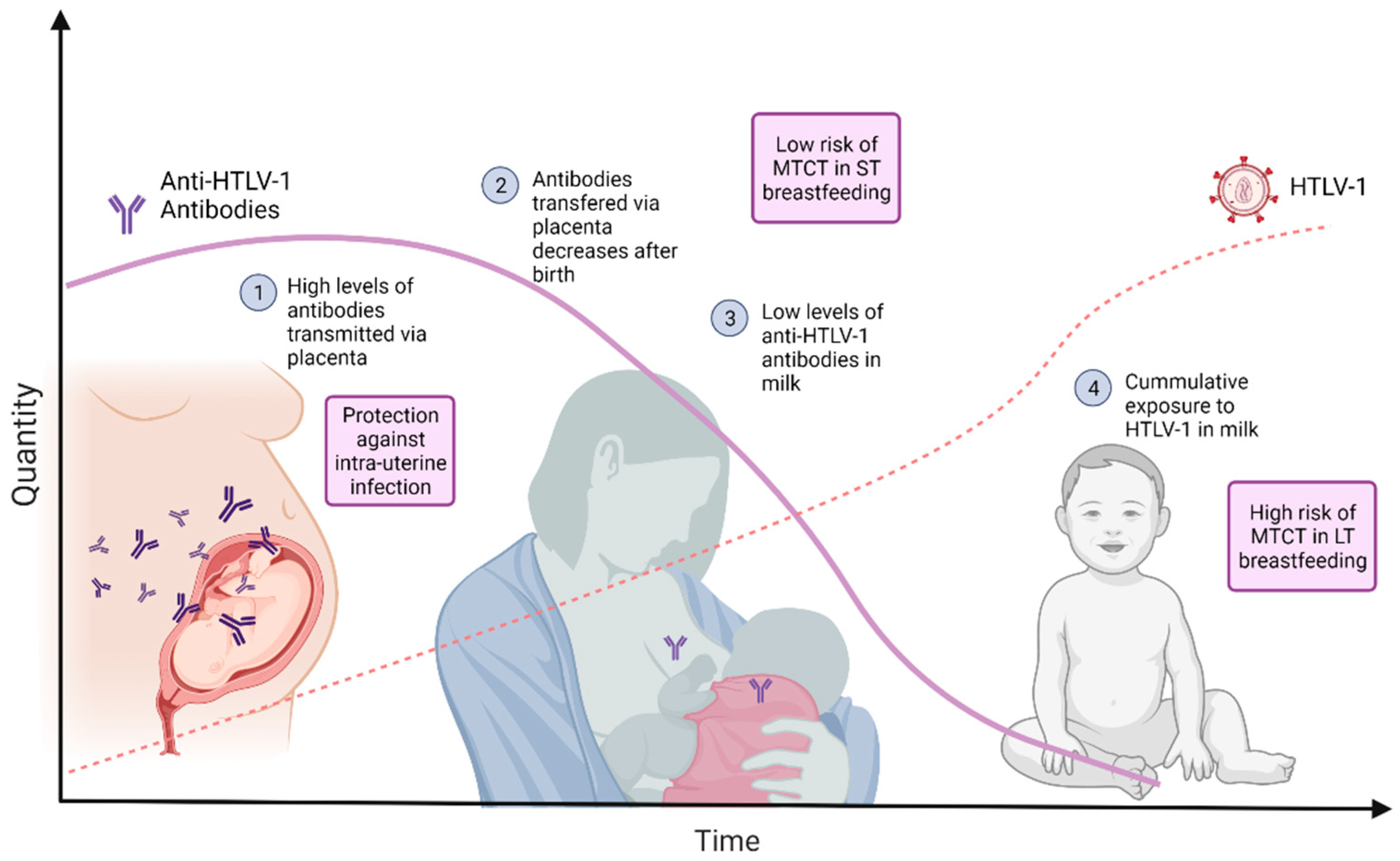
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gessain, A.; Cassar, O. Epidemiological Aspects and World Distribution of HTLV-1 Infection. Front. Microbiol. 2012, 3, 388. [Google Scholar] [CrossRef] [Green Version]
- Schierhout, G.; McGregor, S.; Gessain, A.; Einsiedel, L.; Martinello, M.; Kaldor, J. Association between HTLV-1 infection and adverse health outcomes: A systematic review and meta-analysis of epidemiological studies. Lancet Infect. Dis. 2020, 20, 133–143. [Google Scholar] [CrossRef]
- Demontis, M.A.; Sadiq, M.T.; Golz, S.; Taylor, G.P. HTLV-1 viral RNA is detected rarely in plasma of HTLV-1 infected subjects. J. Med. Virol. 2015, 87, 2130–2134. [Google Scholar] [CrossRef] [PubMed]
- Rosadas, C.; Taylor, G.P. Mother-to-Child HTLV-1 Transmission: Unmet Research Needs. Front. Microbiol. 2019, 10, 999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishijima, T.; Shimada, S.; Noda, H.; Miyake, K. Towards the elimination of HTLV-1 infection in Japan. Lancet Infect. Dis. 2019, 19, 15–16. [Google Scholar] [CrossRef]
- WHO. Human T-lymphotropic Virus Type 1: Technical Report. [Internet]. 2021. Available online: https://www.who.int/publications/i/item/9789240020221 (accessed on 1 June 2021).
- Yamanouchi, K.; Kinoshita, K.; Moriuchi, R.; Katamine, S.; Amagasaki, T.; Ikeda, S.; Ichimaru, M.; Miyamoto, T.; Hino, S. Oral transmission of human T-cell leukemia virus type-I into a common marmoset (Callithrix jacchus) as an experimental model for milk-borne transmission. Jpn. J. Cancer Res. 1985, 76, 481–487. [Google Scholar] [PubMed]
- Kinoshita, K.; Hino, S.; Amagaski, T.; Ikeda, S.; Yamada, Y.; Suzuyama, J.; Momita, S.; Toriya, K.; Kamihira, S.; Ichimaru, M. Demonstration of adult T-cell leukemia virus antigen in milk from three sero-positive mothers. Gan 1984, 75, 103–105. [Google Scholar] [PubMed]
- Kinoshita, K.; Amagasaki, T.; Hino, S.; Doi, H.; Yamanouchi, K.; Ban, N.; Momita, S.; Ikeda, S.; Kamihira, S.; Ichimaru, M. Milk-borne transmission of HTLV-I from carrier mothers to their children. Jpn. J. Cancer Res. 1987, 78, 674–680. [Google Scholar]
- Woo, T.; Rosadas, C.; Ijaz, S.; Dicks, S.; Tosswill, J.H.C.; Tedder, R.S.; Taylor, G.P. Noninvasive Detection of Antibodies to Human T-Cell Lymphotropic Virus Types 1 and 2 by Use of Oral Fluid. J. Clin. Microbiol. 2019, 57, e01179-19. [Google Scholar] [CrossRef]
- Demontis, M.A.; Hilburn, S.; Taylor, G.P. Human T Cell Lymphotropic Virus Type 1 Viral Load Variability and Long-Term Trends in Asymptomatic Carriers and in Patients with Human T Cell Lymphotropic Virus Type 1-Related Diseases. AIDS Res. Hum. Retrovir. 2013, 29, 359–364. [Google Scholar] [CrossRef]
- Tosswill, J.; Taylor, G.; Clewley, J.; Weber, J. Quantification of proviral DNA load in human T-cell leukaemia virus type I infections. J. Virol. Methods 1998, 75, 21–26. [Google Scholar] [CrossRef]
- Rosadas, C.; Tosswill, J.H.; Tedder, R.; Taylor, G.P. Pregnancy does not adversely impact diagnostic tests for HTLV-1/2 infection. PLoS Negl. Trop. Dis. 2019, 13, e0007736. [Google Scholar] [CrossRef] [PubMed]
- Fuchi, N.; Miura, K.; Tsukiyama, T.; Sasaki, D.; Ishihara, K.; Tsuruda, K.; Hasegawa, H.; Miura, S.; Yanagihara, K.; Masuzaki, H. Natural Course of Human T-Cell Leukemia Virus Type 1 Proviral DNA Levels in Carriers During Pregnancy. J. Infect. Dis. 2018, 217, 1383–1389. [Google Scholar] [CrossRef] [PubMed]
- Tezuka, K.; Fuchi, N.; Okuma, K.; Tsukiyama, T.; Miura, S.; Hasegawa, Y.; Nagata, A.; Komatsu, N.; Hasegawa, H.; Sasaki, D.; et al. HTLV-1 targets human placental trophoblasts in seropositive pregnant women. J. Clin. Investig. 2020, 130, 6171–6186. [Google Scholar] [CrossRef] [PubMed]
- Coe, C.L.; Lubach, G.R. Vital and vulnerable functions of the primate placenta critical for infant health and brain development. Front. Neuroendocr. 2014, 35, 439–446. [Google Scholar] [CrossRef] [Green Version]
- Van De Perre, P. Transfer of antibody via mother’s milk. Vaccine 2003, 21, 3374–3376. [Google Scholar] [CrossRef]
- Matsubara, F.; Haraguchi, K.; Harada, K.; Koizumi, A. Screening for Antibodies to Human T-Cell Leukemia Virus Type I in Japanese Breast Milk. Biol. Pharm. Bull. 2012, 35, 773–776. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Biggar, R.J.; Miley, W.J.; Maloney, E.M.; Cranston, B.; Hanchard, B.; Hisada, M. Provirus Load in Breast Milk and Risk of Mother-to-Child Transmission of Human T Lymphotropic Virus Type I. J. Infect. Dis. 2004, 190, 1275–1278. [Google Scholar] [CrossRef]
- Miyazawa, T.; Hasebe, Y.; Murase, M.; Sakurai, M.; Itabashi, K.; Yonemoto, N. The Effect of Early Postnatal Nutrition on Human T Cell Leukemia Virus Type 1 Mother-to-Child Transmission: A Systematic Review and Meta-Analysis. Viruses 2021, 13, 819. [Google Scholar] [CrossRef]
- Itabashi, K.; Miyazawa, T.; Nerome, Y.; Sekizawa, A.; Moriuchi, H.; Saito, S.; Yonemoto, N. Issues of infant feeding for postnatal prevention of human T-cell leukemia/lymphoma virus type-1 mother-to-child transmission. Pediatr. Int. 2020, 63, 284–289. [Google Scholar] [CrossRef]
- Ando, Y.; Matsumoto, Y.; Nakano, S.; Saito, K.; Kakimoto, K.; Tanigawa, T.; Ekuni, Y.; Kawa, M.; Toyama, T. Long-term Follow up Study of Vertical HTLV-I Infection in Children Breast-fed by Seropositive Mothers. J. Infect. 2003, 46, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Ando, Y.; Kakimoto, K.; Tanigawa, T.; Furuki, K.; Saito, K.; Nakano, S.; Hashimoto, H.; Moriyama, I.; Ichijo, M.; Toyama, T. Effect of Freeze-Thawing Breast Milk on Vertical HTLV-I Transmission from Seropositive Mothers to Children. Jpn. J. Cancer Res. 1989, 80, 405–407. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample ID | Age (Years) | Time Since Delivery (Days) | Blood | Milk | ||||
|---|---|---|---|---|---|---|---|---|
| PVL | BR | Titer | PVL | BR | Titer | |||
| 1 | 37 | 92 | 5.5 | 22.58 | 524,288 | 7.69 | 22 | 2048 |
| 2 | 27 | 71 | 0.3 | 6.17 | 131,584 | 0.2 | 6.38 | 128 |
| 3 | 26 | 58 | 0.002 | 5.79 | 131,584 | 0 | 5.48 | 256 |
| 4 * | 32 | 14 | 0.1 | 2.77 | 16,448 | NA | 2.62 | 32 |
| 5 | 28 | 456 | 15.7 | 5.56 | 65,792 | NA | 6.9 | 128 |
| 6 a | 33 | 11 | 0.5 | 3.75 | 32,896 | NA | 3.07 | 32 |
| 7 b | 36 | 17 | 0.2 | 3.4 | 16,448 | 0.04 | 2.5 | 32 |
| 8 # | 49 | 8 | 1.5 | 14.33 | 131,584 | 1.87 | 13.6 | 512 |
| 9 # | 49 | 52 | 3.48 | 12 | 131,584 | NA | 17 | 512 |
| Neg. | 35 | 111 | Neg. | 0.31 | Neg. | Neg. | 0.36 | Neg. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosadas, C.; Woo, T.; Haddow, J.; Rowan, A.; Taylor, G.P. Anti-HTLV-1/2 IgG Antibodies in the Breastmilk of Seropositive Mothers. Microorganisms 2021, 9, 1413. https://doi.org/10.3390/microorganisms9071413
Rosadas C, Woo T, Haddow J, Rowan A, Taylor GP. Anti-HTLV-1/2 IgG Antibodies in the Breastmilk of Seropositive Mothers. Microorganisms. 2021; 9(7):1413. https://doi.org/10.3390/microorganisms9071413
Chicago/Turabian StyleRosadas, Carolina, Timothy Woo, Jana Haddow, Aileen Rowan, and Graham P. Taylor. 2021. "Anti-HTLV-1/2 IgG Antibodies in the Breastmilk of Seropositive Mothers" Microorganisms 9, no. 7: 1413. https://doi.org/10.3390/microorganisms9071413
APA StyleRosadas, C., Woo, T., Haddow, J., Rowan, A., & Taylor, G. P. (2021). Anti-HTLV-1/2 IgG Antibodies in the Breastmilk of Seropositive Mothers. Microorganisms, 9(7), 1413. https://doi.org/10.3390/microorganisms9071413