
Establishment of an In Vitro System of the Human Intestinal Microbiota: Effect of Cultivation Conditions and Influence of Three Donor Stool Samples


Abstract
1. Introduction
2. Materials and Methods
2.1. Donor Stool
2.2. Cultivation Medium
2.3. Fecal Inoculum
2.4. In Vitro Cultivation System
2.5. Analysis of Facultative Aerobic and Anaerobic Cell Count
2.6. Analysis of Short-Chain Fatty Acids by Means of High-Performance Liquid Chromatography
2.7. Microbial Profiling by Means of 16S rRNA Sequencing
2.8. Statistical Analysis
3. Results and Discussion
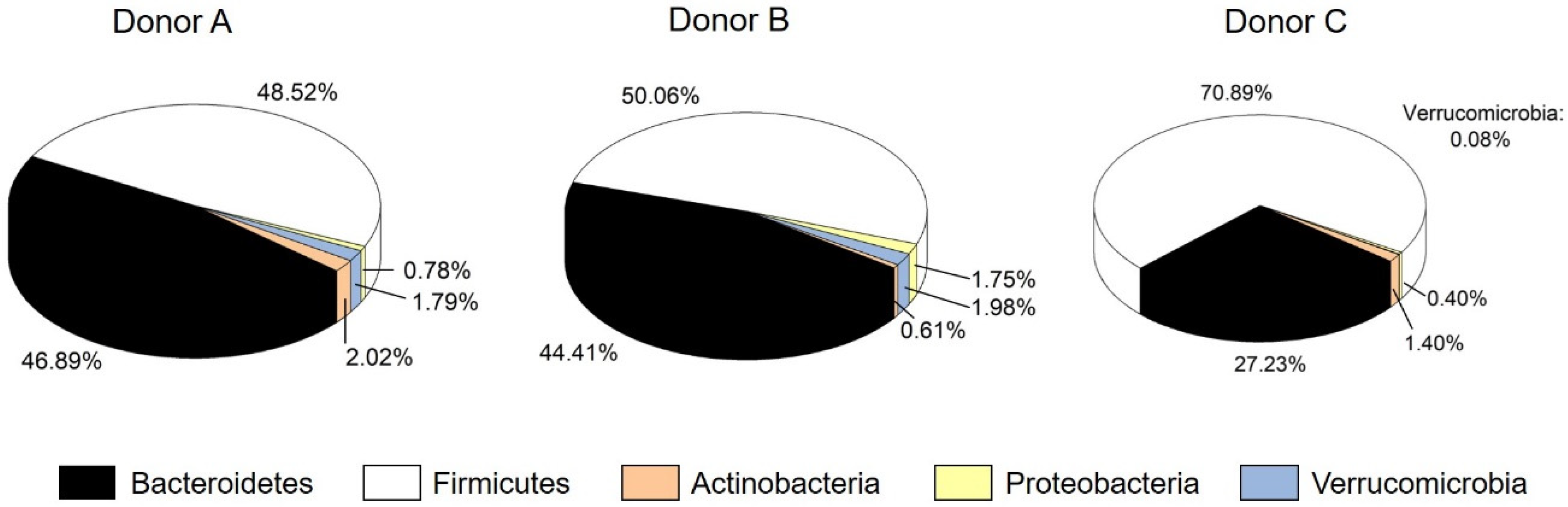
3.1. Characterization of Donor Stools
3.2. Establishment of an In Vitro Microbiota
3.2.1. Cell Count
3.2.2. Metabolic Profile and SCFA Production
3.2.3. Definition of the Stable System
3.2.4. Microbial Composition and Diversity
3.3. Influence of Donor Sample on In Vitro Microbiota in the Stable System
3.4. Comparison of Different Donor Stools
3.5. Comparison with the Inoculum
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eckburg, P.B.; Bik, E.M.; Bernstein, C.N.; Purdom, E.; Dethlefsen, L.; Sargent, M.; Gill, S.R.; Nelson, K.E.; Relman, D.A. Diversity of the human intestinal microbial flora. Science 2005, 308, 1635–1638. [Google Scholar] [CrossRef]
- Gill, S.R.; Pop, M.; Deboy, R.T.; Eckburg, P.B.; Turnbaugh, P.J.; Samuel, B.S.; Gordon, J.I.; Relman, D.A.; Fraser-Liggett, C.M.; Nelson, K.E. Metagenomic analysis of the human distal gut microbiome. Science 2006, 312, 1355–1359. [Google Scholar] [CrossRef]
- Sender, R.; Fuchs, S.; Milo, R. Revised Estimates for the Number of Human and Bacteria Cells in the Body. PLoS Biol. 2016, 14, e1002533. [Google Scholar] [CrossRef]
- Rios-Covian, D.; Salazar, N.; Gueimonde, M.; de Los Reyes-Gavilan, C.G. Shaping the Metabolism of Intestinal Bacteroides Population through Diet to Improve Human Health. Front. Microbiol. 2017, 8, 376. [Google Scholar] [CrossRef] [PubMed]
- de Vadder, F.; Kovatcheva-Datchary, P.; Goncalves, D.; Vinera, J.; Zitoun, C.; Duchampt, A.; Bäckhed, F.; Mithieux, G. Microbiota-generated metabolites promote metabolic benefits via gut-brain neural circuits. Cell 2014, 156, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Grover, S.; Batish, V.K. Hypocholesterolaemic effect of dietary inclusion of two putative probiotic bile salt hydrolase-producing Lactobacillus plantarum strains in Sprague-Dawley rats. Br. J. Nutr. 2011, 105, 561–573. [Google Scholar] [CrossRef]
- Dethlefsen, L.; McFall-Ngai, M.; Relman, D.A. An ecological and evolutionary perspective on human-microbe mutualism and disease. Nature 2007, 449, 811–818. [Google Scholar] [CrossRef]
- Holmes, E.; Li, J.V.; Athanasiou, T.; Ashrafian, H.; Nicholson, J.K. Understanding the role of gut microbiome-host metabolic signal disruption in health and disease. Trends Microbiol. 2011, 19, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Larsen, N.; Vogensen, F.K.; Van Den Berg, F.W.; Nielsen, D.S.; Andreasen, A.S.; Pedersen, B.K.; Al-Soud, W.A.; Sørensen, S.J.; Hansen, L.H.; Jakobsen, M. Gut microbiota in human adults with type 2 diabetes differs from non-diabetic adults. PLoS ONE 2010, 5, e9085. [Google Scholar] [CrossRef]
- Koliada, A.; Syzenko, G.; Moseiko, V.; Budovska, L.; Puchkov, K.; Perederiy, V.; Gavalko, Y.; Dorofeyev, A.; Romanenko, M.; Tkach, S.; et al. Association between body mass index and Firmicutes/Bacteroidetes ratio in an adult Ukrainian population. BMC Microbiol. 2017, 17, 1–6. [Google Scholar] [CrossRef]
- Ley, R.E.; Bäckhed, F.; Turnbaugh, P.; Lozupone, C.A.; Knight, R.D.; Gordon, J.I. Obesity alters gut microbial ecology. Proc. Natl. Acad. Sci. USA 2005, 102, 11070–11075. [Google Scholar] [CrossRef]
- Lagier, J.-C.; Million, M.; Hugon, P.; Armougom, F.; Raoult, D. Human gut microbiota: Repertoire and variations. Front. Cell. Infect. Microbiol. 2012, 2, 136. [Google Scholar] [CrossRef] [PubMed]
- Manichanh, C.; Rigottier-Gois, L.; Bonnaud, E.; Gloux, K.; Pelletier, E.; Frangeul, L.; Nalin, R.; Jarrin, C.; Chardon, P.; Marteau, P.; et al. Reduced diversity of faecal microbiota in Crohn’s disease revealed by a metagenomic approach. Gut 2006, 55, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, S.; Nikolaus, S.; Rosenstiel, P. Microbiome and nutrition. The way to a future therapy for chronic inflammatory bowel diseases? Internist 2014, 55, 889–897. [Google Scholar] [CrossRef] [PubMed]
- Hill-Burns, E.M.; Debelius, J.W.; Morton, J.T.; Wissemann, W.T.; Lewis, M.R.; Wallen, Z.D.; Peddada, S.D.; Factor, S.A.; Molho, E.; Zabetian, C.P.; et al. Parkinson’s disease and Parkinson’s disease medications have distinct signatures of the gut microbiome. Mov. Disord. 2017, 32, 739–749. [Google Scholar] [CrossRef]
- Helmink, B.A.; Khan, M.A.W.; Hermann, A.; Gopalakrishnan, V.; Wargo, J.A. The microbiome, cancer, and cancer therapy. Nat. Med. 2019, 25, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Heidebrecht, H.-J.; Weiss, W.J.; Pulse, M.; Lange, A.; Gisch, K.; Kliem, H.; Mann, S.; Pfaffl, M.W.; Kulozik, U.; Von Eichel-Streiber, C. Treatment and Prevention of Recurrent Clostridium difficile Infection with Functionalized Bovine Antibody-Enriched Whey in a Hamster Primary Infection Model. Toxins 2019, 11, 98. [Google Scholar] [CrossRef]
- Zar, F.A.; Bakkanagari, S.R.; Moorthi, K.M.L.S.T.; Davis, M.B. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin. Infect. Dis. 2007, 45, 302–307. [Google Scholar] [CrossRef]
- Baktash, A.; Terveer, E.M.; Zwittink, R.D.; Hornung, B.V.H.; Corver, J.; Kuijper, E.J.; Smits, W.K. Mechanistic Insights in the Success of Fecal Microbiota Transplants for the Treatment of Clostridium difficile Infections. Front. Microbiol. 2018, 9, 1242. [Google Scholar] [CrossRef]
- Xiao, Y.; Angulo, M.T.; Lao, S.; Weiss, S.T.; Liu, Y.-Y. An ecological framework to understand the efficacy of fecal microbiota transplantation. Nat. Commun. 2020, 11, 3329. [Google Scholar] [CrossRef]
- Aroniadis, O.C.; Brandt, L.J. Fecal microbiota transplantation: Past, present and future. Curr. Opin. Gastroenterol. 2013, 29, 79–84. [Google Scholar] [CrossRef]
- Gough, E.; Shaikh, H.; Manges, A.R. Systematic review of intestinal microbiota transplantation (fecal bacteriotherapy) for recurrent Clostridium difficile infection. Clin. Infect. Dis. 2011, 53, 994–1002. [Google Scholar] [CrossRef] [PubMed]
- Van Schooneveld, T.C.; Gross, A.; Kalil, A.C. Duodenal infusion of donor feces for recurrent Clostridium difficile. N. Engl. J. Med. 2013, 368, 407–415. [Google Scholar] [CrossRef]
- Bircher, L.; Schwab, C.; Geirnaert, A.; Lacroix, C. Cryopreservation of artificial gut microbiota produced with in vitro fermentation technology. Microb. Biotechnol. 2018, 11, 163–175. [Google Scholar] [CrossRef]
- Vigvári, S.; Sipos, D.; Solt, J.; Vincze, Á.; Kocsis, B.; Nemes, Z.; Kappéter, Á.; Feiszt, Z.; Kovács, B.; Péterfi, Z. Faecal microbiota transplantation for Clostridium difficile infection using a lyophilized inoculum from non-related donors: A case series involving 19 patients. Acta Microbiol. Immunol. Hung. 2019, 66, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.J.; Weingarden, A.R.; Sadowsky, M.J.; Khoruts, A. Standardized frozen preparation for transplantation of fecal microbiota for recurrent Clostridium difficile infection. Am. J. Gastroenterol. 2012, 107, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Jalili-Firoozinezhad, S.; Gazzaniga, F.S.; Calamari, E.L.; Camacho, D.M.; Fadel, C.W.; Nestor, B.; Cronce, M.J.; Tovaglieri, A.; Levy, O.; Gregory, K.E.; et al. Complex human gut microbiome cultured in anaerobic human intestine chips. bioRxiv 2018, 421404. [Google Scholar] [CrossRef]
- Bein, A.; Shin, W.; Jalili-Firoozinezhad, S.; Park, M.H.; Sontheimer-Phelps, A.; Tovaglieri, A.; Chalkiadaki, A.; Kim, H.J.; Ingber, D.E. Microfluidic Organ-on-a-Chip Models of Human Intestine. Cell. Mol. Gastroenterol. Hepatol. 2018, 5, 659–668. [Google Scholar] [CrossRef]
- Li, L.; Abou-Samra, E.; Ning, Z.; Zhang, X.; Mayne, J.; Wang, J.; Cheng, K.; Walker, K.; Stintzi, A.; Figeys, D. An in vitro model maintaining taxon-specific functional activities of the gut microbiome. Nat. Commun. 2019, 10, 4146. [Google Scholar] [CrossRef] [PubMed]
- Mennigen, R.; Bruewer, M. Effect of probiotics on intestinal barrier function. Ann. N. Y. Acad. Sci. 2009, 1165, 183–189. [Google Scholar] [CrossRef]
- Le Blay, G.; Rytka, J.; Zihler, A.; Lacroix, C. New in vitro colonic fermentation model for Salmonella infection in the child gut. FEMS Microbiol. Ecol. 2009, 67, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Meunier, V.; Bourrié, M.; Berger, Y.; Fabre, G. The human intestinal epithelial cell line Caco-2; pharmacological and pharmacokinetic applications. Cell Biol. Toxicol. 1995, 11, 187–194. [Google Scholar] [CrossRef]
- Hemarajata, P.; Versalovic, J. Effects of probiotics on gut microbiota: Mechanisms of intestinal immunomodulation and neuromodulation. Therap. Adv. Gastroenterol. 2013, 6, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Minekus, M.; Smeets-Peeters, M.; Bernalier, A.; Marol-Bonnin, S.; Havenaar, R.; Marteau, P.; Alric, M.; Fonty, G.; Huis in’t Veld, J.H. A computer-controlled system to simulate conditions of the large intestine with peristaltic mixing, water absorption and absorption of fermentation products. Appl. Microbiol. Biotechnol. 1999, 53, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Molly, K.; Woestyne, M.V.; de Smet, I.; Verstraete, W. Validation of the Simulator of the Human Intestinal Microbial Ecosystem (SHIME) Reactor Using Microorganism-associated Activities. Microb. Ecol. Health Dis. 1994, 7, 191–200. [Google Scholar] [CrossRef]
- McDonald, J. Development of an In Vitro Fermentation Model to Culture the Human Distal Gut Microbiota. Dissertation, University of Guelph, Guelph, ON, Canada, 2013. Available online: https://Atrium.Lib.Uoguelph.Ca/Xmlui/Handle/10214/7149 (accessed on 11 May 2021).
- Walker, A.W.; Duncan, S.H.; McWilliam Leitch, E.C.; Child, M.W.; Flint, H.J. pH and peptide supply can radically alter bacterial populations and short-chain fatty acid ratios within microbial communities from the human colon. Appl. Environ. Microbiol. 2005, 71, 3692–3700. [Google Scholar] [CrossRef] [PubMed]
- Duncan, S.H.; Louis, P.; Thomson, J.M.; Flint, H.J. The role of pH in determining the species composition of the human colonic microbiota. Environ. Microbiol. 2009, 11, 2112–2122. [Google Scholar] [CrossRef] [PubMed]
- Duncan, S.H.; Scott, K.P.; Ramsay, A.G.; Harmsen, H.J.M.; Welling, G.W.; Stewart, C.S.; Flint, H.J. Effects of alternative dietary substrates on competition between human colonic bacteria in an anaerobic fermentor system. Appl. Environ. Microbiol. 2003, 69, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Takagi, R.; Sasaki, K.; Sasaki, D.; Fukuda, I.; Tanaka, K.; Yoshida, K.-I.; Kondo, A.; Osawa, R. A Single-Batch Fermentation System to Simulate Human Colonic Microbiota for High-Throughput Evaluation of Prebiotics. PLoS ONE 2016, 11, e0160533. [Google Scholar] [CrossRef]
- Zamora-Gasga, V.M.; Cárdenas-Castro, A.P.; Montalvo-González, E.; Loarca-Piña, M.G.F.; Pedro Alberto, V.-L.; Tovar, J.; Sáyago-Ayerdi, S.G. In vitro human colonic fermentation of indigestible fraction isolated from lunch menus: Impact on the gut metabolites and antioxidant capacity. Int. J. Food Sci. Nutr. 2018, 69, 718–728. [Google Scholar] [CrossRef]
- Campos-Vega, R.; Reynoso-Camacho, R.; Pedraza-Aboytes, G.; Acosta-Gallegos, J.A.; Guzman-Maldonado, S.H.; Paredes-Lopez, O.; Oomah, B.D.; Loarca-Piña, G. Chemical composition and in vitro polysaccharide fermentation of different beans (Phaseolus vulgaris L.). J. Food Sci. 2009, 74, T59–T65. [Google Scholar] [CrossRef]
- Macfarlane, G. Validation of a Three-Stage Compound Continuous Culture System for Investigating the Effect of Retention Time on the Ecology and Metabolism of Bacteria in the Human Colon. Microb. Ecol. 1998, 35, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.R.; Rhee, P.-L. How to interpret a functional or motility test—Colon transit study. J. Neurogastroenterol. Motil. 2012, 18, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Terveer, E.M.; van Beurden, Y.H.; Goorhuis, A.; Seegers, J.F.M.L.; Bauer, M.P.; van Nood, E.; Dijkgraaf, M.G.W.; Mulder, C.J.J.; Vandenbroucke-Grauls, C.M.J.E.; Verspaget, H.W.; et al. How to: Establish and run a stool bank. Clin. Microbiol. Infect. 2017, 23, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Payne, A.N.; Zihler, A.; Chassard, C.; Lacroix, C. Advances and perspectives in in vitro human gut fermentation modeling. Trends Biotechnol. 2012, 30, 17–25. [Google Scholar] [CrossRef]
- Reitmeier, S.; Kiessling, S.; Neuhaus, K.; Haller, D. Comparing Circadian Rhythmicity in the Human Gut Microbiome. STAR Protoc. 2020, 1, 100148. [Google Scholar] [CrossRef] [PubMed]
- Lagkouvardos, I.; Joseph, D.; Kapfhammer, M.; Giritli, S.; Horn, M.; Haller, D.; Clavel, T. IMNGS: A comprehensive open resource of processed 16S rRNA microbial profiles for ecology and diversity studies. Sci. Rep. 2016, 6, 33721. [Google Scholar] [CrossRef]
- Reitmeier, S.; Hitch, T.C.A.; Fikas, N.; Hausmann, B.; Ramer-Tait, A.E.; Neuhaus, K.; Berry, D.; Haller, D.; Lagkouvardos, I.; Clavel, T. Handling of spurious sequences affects the outcome of high-throughput 16S rRNA gene amplicon profiling. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Lagkouvardos, I.; Fischer, S.; Kumar, N.; Clavel, T. Rhea: A transparent and modular R pipeline for microbial profiling based on 16S rRNA gene amplicons. PeerJ 2017, 5, e2836. [Google Scholar] [CrossRef]
- Reitmeier, S.; Kiessling, S.; Clavel, T.; List, M.; Almeida, E.L.; Ghosh, T.S.; Neuhaus, K.; Grallert, H.; Linseisen, J.; Skurk, T.; et al. Arrhythmic Gut Microbiome Signatures Predict Risk of Type 2 Diabetes. Cell Host Microbe 2020, 28, 258–272.e6. [Google Scholar] [CrossRef]
- Schwiertz, A.; Taras, D.; Schäfer, K.; Beijer, S.; Bos, N.A.; Donus, C.; Hardt, P.D. Microbiota and SCFA in lean and overweight healthy subjects. Obesity 2010, 18, 190–195. [Google Scholar] [CrossRef]
- De Filippis, F.; Ercolini, D. Microbiome and Diet. In The Gut Microbiome in Health and Disease; Haller, D., Ed.; Springer International Publishing: Cham, Switzerland, 2018; pp. 79–88. ISBN 978-3-319-90544-0. [Google Scholar]
- Mitsou, E.K.; Kirtzalidou, E.; Oikonomou, I.; Liosis, G.; Kyriacou, A. Fecal microflora of Greek healthy neonates. Anaerobe 2008, 14, 94–101. [Google Scholar] [CrossRef]
- Rowland, I.; Gibson, G.; Heinken, A.; Scott, K.; Swann, J.; Thiele, I.; Tuohy, K. Gut microbiota functions: Metabolism of nutrients and other food components. Eur. J. Nutr. 2018, 57, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, G.T.; Gibson, G.R.; Cummings, J.H. Comparison of fermentation reactions in different regions of the human colon. J. Appl. Bacteriol. 1992, 72, 57–64. [Google Scholar] [CrossRef]
- Flint, H.J.; Scott, K.P.; Duncan, S.H.; Louis, P.; Forano, E. Microbial degradation of complex carbohydrates in the gut. Gut Microbes 2012, 3, 289–306. [Google Scholar] [CrossRef]
- Miquel, S.; Martín, R.; Rossi, O.; Bermúdez-Humarán, L.G.; Chatel, J.M.; Sokol, H.; Thomas, M.; Wells, J.M.; Langella, P. Faecalibacterium prausnitzii and human intestinal health. Curr. Opin. Microbiol. 2013, 16, 255–261. [Google Scholar] [CrossRef]
- Adlerberth, I.; Wold, A.E. Establishment of the gut microbiota in Western infants. Acta Paediatr. 2009, 98, 229–238. [Google Scholar] [CrossRef]
- Zihler Berner, A.; Fuentes, S.; Dostal, A.; Payne, A.N.; Vazquez Gutierrez, P.; Chassard, C.; Grattepanche, F.; de Vos, W.M.; Lacroix, C. Novel Polyfermentor intestinal model (PolyFermS) for controlled ecological studies: Validation and effect of pH. PLoS ONE 2013, 8, e77772. [Google Scholar] [CrossRef]
- David, L.A.; Materna, A.C.; Friedman, J.; Campos-Baptista, M.I.; Blackburn, M.C.; Perrotta, A.; Erdman, S.E.; Alm, E.J. Host lifestyle affects human microbiota on daily timescales. Genome Biol. 2014, 15, R89. [Google Scholar] [CrossRef]
- Brandt, L.J.; Aroniadis, O.C.; Mellow, M.; Kanatzar, A.; Kelly, C.; Park, T.; Stollman, N.; Rohlke, F.; Surawicz, C. Long-term follow-up of colonoscopic fecal microbiota transplant for recurrent Clostridium difficile infection. Am. J. Gastroenterol. 2012, 107, 1079–1087. [Google Scholar] [CrossRef]
- Weingarden, A.; Gonzalez, A.; Vazquez-Baeza, Y.; Weiss, S.; Humphry, G.; Berg-Lyons, D.; Knights, D.; Unno, T.; Bobr, A.; Kang, J.; et al. Dynamic changes in short- and long-term bacterial composition following fecal microbiota transplantation for recurrent Clostridium difficile infection. Microbiome 2015, 3. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stock Solution | Reagent | Manufacturer | Weight [g] | Dissolution in Double Distilled H2O [mL] |
|---|---|---|---|---|
| l | Casein peptone | Gerbu Biotechnik, Heidelberg, Germany | 1.3 | 800 |
| Yeast extract | Gerbu Biotechnik, Heidelberg, Germany | 2 | ||
| NaHCO3 | Bernd Kraft, Duisburg, Germany | 2 | ||
| CaCl2 | Sigma-Aldrich, Saint-Louis, MO, USA | 0.01 | ||
| Pectin from citrus | Sigma-Aldrich, Saint-Louis, MO, USA | 2 | ||
| Xylan from beechwood | Iris Biotech, Marktredwitz, Germany | 2 | ||
| Arabinogalactan | Sigma-Aldrich, Saint-Louis, MO, USA | 2 | ||
| Starch | Merck KGaA, Darmstadt, Germany | 5 | ||
| Casein | Sigma-Aldrich, Saint-Louis, MO, USA | 3 | ||
| Inulin from Dahlia tubers | Sigma-Aldrich, Saint-Louis, MO, USA | 1 | ||
| NaCl | Carl Roth GmbH, Karlsruhe, Germany | 0.75 | ||
| 2 | K2HPO4 | Sigma-Aldrich, Saint-Louis, MO, USA | 0.04 | 50 |
| KH2PO4 | Sigma-Aldrich, Saint-Louis, MO, USA | 0.04 | ||
| MgSO4 | Sigma-Aldrich, Saint-Louis, MO, USA | 0.01 | ||
| 3 | Bile salts | Sigma-Aldrich, Saint-Louis, MO, USA | 0.5 | 50 |
| L-Cysteine | Gerbu Biotechnik, Heidelberg, Germany | 0.5 | ||
| 4 | Porcine gastric mucin (type II) | Sigma-Aldrich, Saint-Louis, MO, USA | 4 | 100 |
| 5 | Hemin solution | Sigma-Aldrich, Saint-Louis, MO, USA | 10 | - |
| 6 | Vitamin K1 solution | Alfa Aesar, Karlsruhe, Germany | 0.2 | - |
| Donor A | Donor B | Donor C | ||
|---|---|---|---|---|
| Cell count | Aerobic [105 CFU mL−1] | 0.7 ± 0.4 | 10 ± 9 | 9 ± 1 |
| Anaerobic [108 CFU mL−1] | 4 ± 3 | 2 ± 0.02 | 4 ± 0.6 | |
| Metabolic profile | Acetate [mg mL−1] | 3.17 ± 0.21 | 2.74 ± 0.07 | 2.59 ± 0.54 |
| Propionate [mg mL−1] | 2.00 ± 0.16 | 1.15 ± 0.04 | 1.02 ± 0.16 | |
| Butyrate [mg mL−1] | 1.48 ± 0.08 | 0.99 ± 0.03 | 2.14 ± 0.26 | |
| Isovalerate [mg mL−1] | 0.15 ± 0.02 | 0.24 ± 0.00 | 0.34 ± 0.04 | |
| Σ SCFAs [mg mL−1] | 6.80 ± 0.47 | 5.12 ± 0.14 | 6.09 ± 1.00 | |
| Microbial profile | Richness [-] | 100 | 123 | 122 |
| Shannon effective index [-] | 21.42 | 38.43 | 46.34 | |
| Ratio F:B | 1.03 | 1.13 | 2.60 |
| Processing Time | ||||||
|---|---|---|---|---|---|---|
| Inoculum | After Inoculation (<1.0 h) | 8.3 ± 2.6 h | 24.6 ± 0.6 h | 48.0 ± 1.3 h | Stable System (>77.0 h) | |
| Actinobacteria [%] | 3.44 ± 0.83 | 3.16 ± 0.32 | 2.58 ± 1.01 | 2.27 ± 1.33 | 0.23 ± 0.02 | 0.09 ± 0.05 |
| Bacteroidetes [%] | 1.59 ± 1.09 | 0.90 ± 0.12 | 0.63 ± 0.67 | 37.91 ± 1.65 | 73.20 ± 1.46 | 75.99 ± 1.78 |
| Firmicutes [%] | 94.82 ± 0.75 | 95.78 ± 0.11 | 85.41 ± 7.62 | 49.20 ± 2.12 | 21.64 ± 1.69 | 16.92 ± 1.96 |
| Proteobacteria [%] | 0.12 ± 0.06 | 0.12 ± 0.14 | 11.37 ± 7.69 | 10.60 ± 3.81 | 3.83 ± 0.94 | 4.38 ± 2.42 |
| Verrucomicrobia [%] | 0.03 ± 0.01 | 0.04 ± 0.01 | 0.01 ± 0.01 | 0.02 ± 0.02 | 1.10 ± 0.76 | 2.22 ± 0.72 |
| Richness [-] | 103.40 ± 5.68 | 94.33 ± 10.02 | 11.00 ± 4.36 | 96.33 ± 12.66 | 95.00 ± 11.14 | 105.17 ± 5.71 |
| Shannon effective index [-] | 23.35 ± 2.76 | 18.69 ± 0.86 | 8.32 ± 4.23 | 24.21 ± 1.35 | 19.28 ± 1.65 | 17.28 ± 1.14 |
| Donor A | Donor B | Donor C | ||
|---|---|---|---|---|
| Cell count | Aerobic [108 CFU mL−1] | 1 ± 0.6 | 2 ± 1 | 0.7 ± 0.07 |
| Anaerobic [1010 CFU mL−1] | 0.9 ± 0.2 | 1 ± 0.3 | 1 ± 0.004 | |
| Metabolic profile | Acetate [ mg mL−1] | 3.46 ± 0.22 | 3.82 ± 0.14 | 3.52 ± 0.05 |
| Propionate [ mg mL−1] | 2.94 ± 0.13 | 2.94 ± 0.13 | 3.00 ± 0.07 | |
| Butyrate [ mg mL−1] | 1.64 ± 0.16 | 1.57 ± 0.16 | 2.39 ± 0.15 | |
| Isovalerate [ mg mL−1] | 0.24 ± 0.04 | 0.36 ± 0.08 | 0.31 ± 0.00 | |
| Σ SCFAs [ mg mL−1] | 8.29 ± 0.55 | 8.68 ± 0.51 | 9.22 ± 0.27 | |
| Microbial profile | Richness [-] | 105.17 ± 5.71 | 96.00 ± 7.07 | 115.00 ± 2.83 |
| Shannon effective index [-] | 17.28 ± 1.14 | 24.40 ± 1.75 | 21.56 ± 1.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haindl, R.; Engel, J.; Kulozik, U. Establishment of an In Vitro System of the Human Intestinal Microbiota: Effect of Cultivation Conditions and Influence of Three Donor Stool Samples. Microorganisms 2021, 9, 1049. https://doi.org/10.3390/microorganisms9051049
Haindl R, Engel J, Kulozik U. Establishment of an In Vitro System of the Human Intestinal Microbiota: Effect of Cultivation Conditions and Influence of Three Donor Stool Samples. Microorganisms. 2021; 9(5):1049. https://doi.org/10.3390/microorganisms9051049
Chicago/Turabian StyleHaindl, Regina, Julia Engel, and Ulrich Kulozik. 2021. "Establishment of an In Vitro System of the Human Intestinal Microbiota: Effect of Cultivation Conditions and Influence of Three Donor Stool Samples" Microorganisms 9, no. 5: 1049. https://doi.org/10.3390/microorganisms9051049
APA StyleHaindl, R., Engel, J., & Kulozik, U. (2021). Establishment of an In Vitro System of the Human Intestinal Microbiota: Effect of Cultivation Conditions and Influence of Three Donor Stool Samples. Microorganisms, 9(5), 1049. https://doi.org/10.3390/microorganisms9051049