
The Prevalence of Human Papillomavirus (HPV) Genotypes in the Oral Mucosae of HIV-Positive Individuals: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
Statistical Methods
3. Results
3.1. Risk of Bias Assessment
3.2. Heterogeneity Analysis
3.3. HPV Prevalence Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HPV | Human papillomavirus |
| HIV | Human immunodeficiency virus |
| OPSCC | Oropharyngeal squamous cell carcinoma |
References
- Tahmasebi, E.; Keshvad, A.; Alam, M.; Abbasi, K.; Rahimi, S.; Nouri, F.; Yazdanian, M.; Tebyaniyan, H.; Heboyan, A.; Fernandes, G.V.O. Current Infections of the Orofacial Region: Treatment, Diagnosis, and Epidemiology. Life 2023, 13, 269. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.E.; Becker, G.L.; Jackson, J.B.; Rysavy, M.B. Human Papillomavirus and Associated Cancers: A Review. Viruses 2024, 16, 680. [Google Scholar] [CrossRef]
- He, M.; He, C.Q.; Ding, N.Z. Human viruses: An ever-increasing list. Virology 2025, 604, 110445. [Google Scholar] [CrossRef]
- Ekström, J.; Mühr, L.S.; Bzhalava, D.; Söderlund-Strand, A.; Hultin, E.; Nordin, P.; Stenquist, B.; Paoli, J.; Forslund, O.; Dillner, J. Diversity of human papillomaviruses in skin lesions. Virology 2013, 447, 300–311. [Google Scholar] [CrossRef] [PubMed]
- Cosper, P.F.; Bradley, S.; Luo, L.; Kimple, R.J. Biology of HPV Mediated Carcinogenesis and Tumor Progression. Semin. Radiat. Oncol. 2021, 31, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Poudel, S.; Rai, S.; Adhikari, S.P.; Dhakal, S.; Rai, N.; Upadhyaya, P.C.; Shah, P. Knowledge and Attitude Towards Human Papilloma Virus and Human Papilloma Virus Vaccine. J. Nepal Health Res. Counc. 2024, 22, 622–626. [Google Scholar] [CrossRef]
- Zadeh Mehrizi, T.; Ataei-Pirkooh, A.; Eshrati, B.; Ebrahimi Shahmabadi, H. Investigating factors affecting the effectiveness of Gardasil 4, Cervarix, and Gardasil 9 vaccines considering the WHO regions in females: A systematic review. Cancer Epidemiol. 2025, 95, 102759. [Google Scholar] [CrossRef]
- Sambo, M.; Bailoni, A.; Mariani, F.; Granai, M.; Calomino, N.; Mancini, V.; D’Antiga, A.; Montagnani, F.; Tumbarello, M.; Lazzi, S.; et al. Prevalence, Incidence and Predictors of Anal HPV Infection and HPV-Related Squamous Intraepithelial Lesions in a Cohort of People Living with HIV. Diagnostics 2025, 15, 198. [Google Scholar] [CrossRef]
- Al-Soneidar, W.A.; Harper, S.; Madathil, S.A.; Schlecht, N.F.; Nicolau, B. Do cutaneous human papillomavirus genotypes affect head and neck cancer? Evidence and bias-correction from a case-control study. Cancer Epidemiol. 2022, 79, 102205. [Google Scholar] [CrossRef]
- Brickman, C.E.; Propert, K.J.; Merlin, J.S.; Liu, J.C.; Eady, S.; Mcghee-Jez, A.; Ragin, C.; Grover, S.; Cohen, R.B.; Gross, R. Treatment and Outcomes of Oropharyngeal Cancer in People with Human Immunodeficiency Virus. AIDS Res. Hum. Retroviruses 2019, 35, 934–940. [Google Scholar] [CrossRef]
- Biała, M.; Zalewska, M.; Szetela, B.; Gąsiorowski, J.; Leszczyszyn, J.; Inglot, M. Prevalence and genotype distribution of human papillomavirus infection among HIV-infected men who have sex with men living in Lower Silesia, Poland. Postep. Dermatol. I Alergol. 2022, 39, 1128–1133. [Google Scholar] [CrossRef] [PubMed]
- Bottalico, D.; Chen, Z.; Dunne, A.; Ostoloza, J.; McKinney, S.; Sun, C.; Schlecht, N.F.; Fatahzadeh, M.; Herrero, R.; Schiffman, M.; et al. The oral cavity contains abundant known and novel human papillomaviruses from the Betapapillomavirus and Gammapapillomavirus genera. J. Infect. Dis. 2011, 204, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Gaester, K.; Fonseca, L.A.; Luiz, O.; Assone, T.; Fontes, A.S.; Costa, F.; Duarte, A.J.; Casseb, J. Human papillomavirus infection in oral fluids of HIV-1-positive men: Prevalence and risk factors. Sci. Rep. 2014, 4, 6592. [Google Scholar] [CrossRef]
- Ucciferri, C.; Tamburro, M.; Falasca, K.; Sammarco, M.L.; Ripabelli, G.; Vecchiet, J. Prevalence of anal, oral, penile and urethral Human Papillomavirus in HIV infected and HIV uninfected men who have sex with men. J. Med. Virol. 2018, 90, 358–366. [Google Scholar] [CrossRef]
- Sammarco, M.L.; Ucciferri, C.; Tamburro, M.; Falasca, K.; Ripabelli, G.; Vecchiet, J. High prevalence of human papillomavirus type 58 in HIV infected men who have sex with men: A preliminary report in Central Italy. J. Med. Virol. 2016, 88, 911–914. [Google Scholar] [CrossRef]
- Chang, M.S.; Lee, S.W.; Kim, S.; Lee, C.S.; Byeon, S.H.; Kim, S.S.; Kim, Y.J. Incident Noninfectious Uveitis Risk after Immune Checkpoint Inhibitor Treatment. Ophthalmology 2024, 131, 867–869. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Gonçalves, H.M.; Silva, J.; Pintado Maury, I.; Tavares, A.; Campos, C.; Sousa, H.; Jacinto, A.; Aguiar, P.; Caldeira, L.; Medeiros, R. The prevalence and risk-factors of oral HPV DNA detection among HIV-infected men between men who have sex with men and heterosexual men. Infect. Dis. 2021, 53, 19–30. [Google Scholar] [CrossRef]
- Richter, K.L.; van Rensburg, E.J.; van Heerden, W.F.; Boy, S.C. Human papilloma virus types in the oral and cervical mucosa of HIV-positive South African women prior to antiretroviral therapy. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2008, 37, 555–559. [Google Scholar] [CrossRef]
- Steinau, M.; Reddy, D.; Sumbry, A.; Reznik, D.; Gunthel, C.J.; Del Rio, C.; Lennox, J.L.; Unger, E.R.; Nguyen, M.L. Oral sampling and human papillomavirus genotyping in HIV-infected patients. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2012, 41, 288–291. [Google Scholar] [CrossRef]
- Suehiro, T.T.; Damke GM, Z.F.; Damke, E.; de Azevedo Ramos PL, R.; de Andrade Pereira Silva, M.; Pelloso, S.M.; Huh, W.K.; Franco RA, F.; da Silva VR, S.; Scarinci, I.C.; et al. Cervical and oral human papillomavirus infection in women living with human immunodeficiency virus (HIV) and matched HIV-negative controls in Brazil. Infect. Agents Cancer 2020, 15, 31. [Google Scholar] [CrossRef] [PubMed]
- Tsikis, S.; Hoefer, L.; Bethimoutis, G.; Nicolaidou, E.; Paparizos, V.; Antoniou, C.; Chardalias, L.; Stavropoulos, G.E.; Sharma, S.; Long, B.C.; et al. Risk factors, prevalence, and site concordance of human papillomavirus in high-risk Greek men. Eur. J. Cancer Prev. Off. J. Eur. Cancer Prev. Organ. (ECP) 2018, 27, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Uwamungu, S.; Nigussie, B.; Muvunyi, C.M.; Hasséus, B.; Andersson, M.; Giglio, D. Prevalence of Human Papillomavirus in Different Mucous Membranes in HIV Concordant Couples in Rwanda. Viruses 2023, 15, 1005. [Google Scholar] [CrossRef]
- Visalli, G.; Di Pietro, A.; Currò, M.; Pruiti Ciarello, M.; D’Andrea, F.; Nunnari, G.; Pellicanò, G.F.; Facciolà, A. How Much Does HIV Positivity Affect the Presence of Oral HPV? A Molecular Epidemiology Survey. Int. J. Environ. Res. Public Health 2021, 18, 8999. [Google Scholar] [CrossRef] [PubMed]
- Vergori, A.; Garbuglia, A.R.; Piselli, P.; Del Nonno, F.; Sias, C.; Lupi, F.; Lapa, D.; Baiocchini, A.; Cimaglia, C.; Gentile, M.; et al. Oral human Papillomavirus DNA detection in HIV-positive men: Prevalence, predictors, and co-occurrence at anal site. BMC Infect. Dis. 2018, 18, 25. [Google Scholar] [CrossRef]
- Gheit, T.; Rollo, F.; Brancaccio, R.N.; Robitaille, A.; Galati, L.; Giuliani, M.; Latini, A.; Pichi, B.; Benevolo, M.; Cuenin, C.; et al. Oral Infection by Mucosal and Cutaneous Human Papillomaviruses in the Men Who Have Sex with Men from the OHMAR Study. Viruses 2020, 12, 899. [Google Scholar] [CrossRef]
- Hernandez, A.L.; Karthik, R.; Sivasubramanian, M.; Raghavendran, A.; Lensing, S.; Lee, J.Y.; Abraham, P.; Mathai, D.; Palefsky, J.M. Prevalence of oral human papillomavirus infection among Indian HIV-positive men who have sex with men: A cross-sectional study. BMC Infect. Dis. 2021, 21, 675. [Google Scholar] [CrossRef]
- Sias, C.; Salichos, L.; Lapa, D.; Del Nonno, F.; Baiocchini, A.; Capobianchi, M.R.; Garbuglia, A.R. Alpha, Beta, gamma human PapillomaViruses (HPV) detection with a different sets of primers in oropharyngeal swabs, anal and cervical samples. Virol. J. 2019, 16, 27. [Google Scholar] [CrossRef]
- Rajendra Santosh, A.B.; Christian, N.A.; Jones, T.; Thoms-Rodriguez, C.A.; Condappa, A.; Thompson, T.; Pinkney, J.; Barton, E.N.; Lindo, J. Molecular epidemiology of human papillomavirus genotypes in oral rinses from HIV-positive and HIV-negative Jamaican patients. J. Investig. Clin. Dent. 2019, 10, e12365. [Google Scholar] [CrossRef]
- Chuerduangphui, J.; Proyrungroj, K.; Pientong, C.; Hinkan, S.; Budkaew, J.; Pimson, C.; Chumworathayi, B.; Hanond, P.; Ekalaksananan, T. Prevalence and anatomical sites of human papillomavirus, Epstein-Barr virus and herpes simplex virus infections in men who have sex with men, Khon Kaen, Thailand. BMC Infect. Dis. 2018, 18, 509. [Google Scholar] [CrossRef]
- Castillejos-García, I.; Ramírez-Amador, V.A.; Carrillo-García, A.; García-Carrancá, A.; Lizano, M.; Anaya-Saavedra, G. Type-specific persistence and clearance rates of HPV genotypes in the oral and oropharyngeal mucosa in an HIV/AIDS cohort. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2018, 47, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Robbins, H.A.; Fennell, C.E.; Gillison, M.; Xiao, W.; Guo, Y.; Wentz, A.; Kirk, G.D.; Mehta, S.H.; D’Souza, G. Prevalence of and Risk Factors for Oral Human Papillomavirus Infection among HIV-Positive and HIV-Negative People Who Inject Drugs. PLoS ONE 2015, 10, e0143698. [Google Scholar] [CrossRef]
- Blas, M.M.; Brown, B.; Menacho, L.; Alva, I.E.; Silva-Santisteban, A.; Carcamo, C. HPV Prevalence in Multiple Anatomical Sites among Men Who Have Sex with Men in Peru. PLoS ONE 2015, 10, e0139524. [Google Scholar] [CrossRef]
- Ong, J.J.; Read, T.R.; Vodstrcil, L.A.; Walker, S.; Chen, M.; Bradshaw, C.S.; Garland, S.M.; Tabrizi, S.N.; Cornall, A.; Grulich, A.; et al. Detection of oral human papillomavirus in HIV-positive men who have sex with men 3 years after baseline: A follow up cross-sectional study. PLoS ONE 2014, 9, e0102138. [Google Scholar] [CrossRef] [PubMed]
- Olsen, M.H.; Frederiksen, K.; Lassen, P.; Rotbøl, C.; Kjaer, T.K.; Johansen, J.; Primdahl, H.; Andersen, E.; Kristensen, C.A.; Andersen, M.; et al. Association of Smoking, comorbidity, clinical stage, and treatment intent with socioeconomic differences in survival after oropharyngeal squamous cell carcinoma in Denmark. JAMA Netw. Open 2022, 5, e2245510. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; Didzbalis, C.J.; Tseng, C.C.; Talmor, G.; Park, R.C.W. Facility volume and survival: Human papilloma virus positive oropharyngeal squamous cell carcinoma. Am. J. Otolaryngol. 2023, 44, 103762. [Google Scholar] [CrossRef]
- Mazul, A.L.; Hartman, C.M.; Mowery, Y.M.; Kramer, J.R.; White, D.L.; Royse, K.E.; Raychaudhury, S.; Sandulache, V.C.; Ahmed, S.T.; Zevallos, J.P.; et al. Risk and incidence of head and neck cancers in veterans living with HIV and matched HIV-negative veterans. Cancer 2022, 128, 3310–3318. [Google Scholar] [CrossRef]
- Chew, E.Y.; Hartman, C.M.; Richardson, P.A.; Zevallos, J.P.; Sikora, A.G.; Kramer, J.R.; Chiao, E.Y. Risk factors for oropharynx cancer in a cohort of HIV-infected veterans. Oral Oncol. 2017, 68, 60–66. [Google Scholar] [CrossRef]
- Zhou, L.; Li, Y.; Wang, H.; Qin, R.; Han, Z.; Li, R. Global cervical cancer elimination: Quantifying the status, progress, and gaps. BMC Med. 2025, 23, 67. [Google Scholar] [CrossRef]
- Pugliese, D.B.; Bruzzesi, G.; Montaldo, C.; Porcu, L.; Landi, M.; Mastinu, A.; Torri, V.; Licitra, L.; Locati, L.D. Oral prevalence and clearance of oncogenic human papilloma virus in a rehabilitation community for substance abusers in Italy: A case of behavioral correction? J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2015, 44, 728–733. [Google Scholar] [CrossRef]
- Fatahzadeh, M.; Schlecht, N.F.; Chen, Z.; Bottalico, D.; McKinney, S.; Ostoloza, J.; Dunne, A.; Burk, R.D. Oral Human Papillomavirus Detection in Older Adults Who Have Human Immunodeficiency Virus Infection. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 505–514. [Google Scholar] [CrossRef]
- Morais, A.C.C.D.; Ferreira, A.S.; Barbosa, C.D.T.; Lima, M.F.B.; Fook, K.D.; Carvalho, M.M.; Muniz, A.C.S.; Araújo, D.R.; Monteiro, P.M.; Araújo, M.J.A.M.; et al. Human Papillomavirus in Women Infected with Human Immunodeficiency Virus: Association with Viral Load and Lymphocyte Count. Rev. Inst. Med. Trop. Sao Paulo 2024, 66, e36. [Google Scholar] [CrossRef]
- Wood, N.H.; Makua, K.S.; Lebelo, R.L.; Redzic, N.; Benoy, I.; Vanderveken, O.M.; Bogers, J. Human Papillomavirus Prevalence in Oral and Oropharyngeal Rinse and Gargle Specimens of Dental Patients and of an HIV-Positive Cohort from Pretoria, South Africa. Adv. Virol. 2020, 2020, 2395219. [Google Scholar] [CrossRef] [PubMed]
- Nemcova, J.; Riegert, J.; Cerna, K.; Rob, F.; Smahelova, J.; Hercogova, J.T.; Martinek, P.; Ondic, O. Prevalence of Oral and Anal Human Papillomavirus Infection in Czech Predominantly HIV-Positive Men Having Sex with Men–Data from a Previously Unreported Population. Int. J. STD AIDS 2022, 33, 1054–1064. [Google Scholar] [CrossRef] [PubMed]
- Abbas, S.R.; Abbas, Z.; Zahir, A.; Lee, S.W. Federated Learning in Smart Healthcare: A Comprehensive Review on Privacy, Security, and Predictive Analytics with IoT Integration. Healthcare 2025, 12, 2587. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.M.; Jung, S.Y.; Kim, M.S.; Lee, S.W.; Yon, D.K.; Shin, J.I.; Lee, J.Y. Cardiovascular and Cerebrovascular Adverse Events Associated with Intravitreal Anti-VEGF Monoclonal Antibodies: A World Health Organization Pharmacovigilance Study. Ophthalmology 2025, 132, 62–78. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
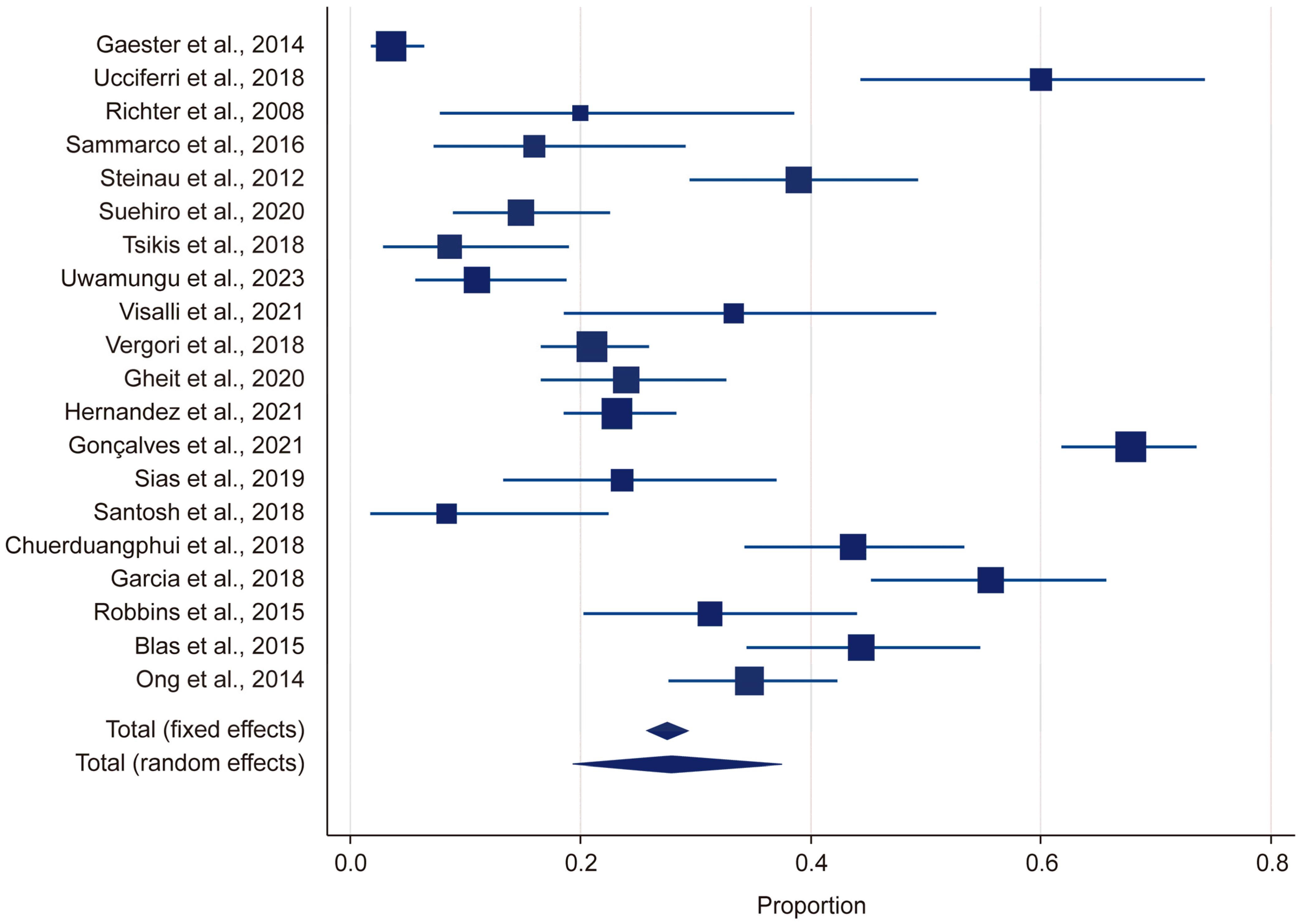
| Study | Sample Size | Proportion (%) | 95% CI | Weight (%) Random |
|---|---|---|---|---|
| Gaester et al., 2014 [13] | 283 | 3.53 | 1.71 to 6.41 | 5.23 |
| Ucciferri et al., 2018 [14] | 45 | 60 | 44.33 to 74.31 | 4.80 |
| Richter et al., 2008 [19] | 30 | 20 | 7.71 to 38.57 | 4.59 |
| Sammarco et al., 2016 [15] | 50 | 16 | 7.14 to 29.11 | 4.85 |
| Steinau et al., 2012 [20] | 100 | 39 | 29.40 to 49.27 | 5.07 |
| Suehiro et al., 2020 [21] | 115 | 14.78 | 8.85 to 22.61 | 5.10 |
| Tsikis et al., 2018 [22] | 58 | 8.62 | 2.86 to 18.98 | 4.91 |
| Uwamungu et al., 2023 [23] | 100 | 11 | 5.62 to 18.83 | 5.07 |
| Visalli et al., 2021 [24] | 36 | 33.33 | 18.56 to 50.97 | 4.69 |
| Vergori et al., 2018 [25] | 305 | 20.98 | 16.55 to 25.99 | 5.23 |
| Gheit et al., 2020 [26] | 117 | 23.93 | 16.53 to 32.69 | 5.10 |
| Hernandez et al., 2021 [27] | 302 | 23.18 | 18.54 to 28.35 | 5.23 |
| Gonçalves et al., 2021 [18] | 255 | 67.84 | 61.73 to 73.53 | 5.22 |
| Sias et al., 2019 [28] | 55 | 23.64 | 13.23 to 37.02 | 4.89 |
| Santosh et al., 2018 [29] | 36 | 8.33 | 1.75 to 22.47 | 4.69 |
| Chuerduangphui et al., 2018 [30] | 110 | 43.64 | 34.21 to 53.42 | 5.09 |
| Garcia et al., 2018 [31] | 97 | 55.67 | 45.23 to 65.76 | 5.06 |
| Robbins et al., 2015 [32] | 64 | 31.25 | 20.24 to 44.06 | 4.94 |
| Blas et al., 2015 [33] | 99 | 44.44 | 34.45 to 54.78 | 5.07 |
| Ong et al., 2014 [34] | 173 | 34.68 | 27.62 to 42.28 | 5.17 |
| Total (random effects) | 2430 | 27.97 | 19.34 to 37.51 | 100 |
| Study | Sample Size | Proportion (%) | 95% CI | Weight (%) Random |
|---|---|---|---|---|
| Gaester et al., 2014 [13] | 283 | 3.53 | 1.71 to 6.41 | 5.19 |
| Ucciferri et al., 2018 [14] | 45 | 57.78 | 42.15 to 74.34 | 4.84 |
| Richter et al., 2008 [19] | 30 | 20 | 7.71 to 38.57 | 4.65 |
| Sammarco et al., 2016 [15] | 50 | 16 | 7.14 to 29.11 | 4.87 |
| Steinau et al., 2012 [20] | 100 | 39 | 29.40 to 49.27 | 5.06 |
| Suehiro et al., 2020 [21] | 115 | 14.78 | 8.85 to 22.61 | 5.08 |
| Tsikis et al., 2018 [22] | 58 | 8.62 | 2.86 to 18.98 | 4.92 |
| Uwamungu et al., 2023 [23] | 100 | 11 | 5.62 to 18.83 | 5.06 |
| Visalli et al., 2021 [24] | 36 | 33.33 | 18.56 to 50.97 | 4.74 |
| Vergori et al., 2018 [25] | 305 | 20.98 | 16.55 to 25.99 | 5.19 |
| Gheit et al., 2020 [26] | 117 | 23.93 | 16.53 to 32.69 | 5.09 |
| Hernandez et al., 2021 [27] | 302 | 5.63 | 3.13 to 8.86 | 5.19 |
| Gonçalves et al., 2021 [18] | 255 | 67.84 | 61.73 to 73.53 | 5.18 |
| Sias et al., 2019 [28] | 55 | 23.64 | 13.23 to 37.02 | 4.91 |
| Santosh et al., 2018 [29] | 36 | 8.33 | 1.75 to 22.47 | 4.74 |
| Chuerduangphui et al., 2018 [30] | 110 | 43.64 | 34.21 to 53.42 | 5.08 |
| Garcia et al., 2018 [31] | 97 | 55.67 | 45.23 to 65.76 | 5.05 |
| Robbins et al., 2015 [32] | 64 | 31.25 | 20.24 to 44.06 | 4.95 |
| Blas et al., 2015 [33] | 99 | 44.44 | 34.45 to 54.78 | 5.06 |
| Ong et al., 2014 [34] | 173 | 34.68 | 27.62 to 42.28 | 5.14 |
| Total (random effects) | 2430 | 26.65 | 17.43 to 37.04 | 100 |
| Study | Sample Size | Proportion (%) | 95% CI | Weight (%) Random |
|---|---|---|---|---|
| Gaester et al., 2014 [13] | 283 | 3534 | 1707 to 6402 | 5.19 |
| Ucciferri et al., 2018 [14] | 45 | 57,778 | 42,150 to 72,343 | 4.84 |
| Richter et al., 2008 [19] | 30 | 20 | 7714 to 38,567 | 4.65 |
| Sammarco et al., 2016 [15] | 50 | 16 | 7170 to 29,113 | 4.87 |
| Steinau et al., 2012 [20] | 100 | 39 | 29,401 to 49,269 | 5.06 |
| Suehiro et al., 2020 [21] | 115 | 14,783 | 8854 to 22,610 | 5.08 |
| Tsikis et al., 2018 [22] | 58 | 8621 | 2859 to 18,983 | 4.92 |
| Uwamungu et al., 2023 [23] | 100 | 11 | 5621 to 18,830 | 5.06 |
| Visalli et al., 2021 [24] | 36 | 33,333 | 18,556 to 50,970 | 4.74 |
| Vergori et al., 2018 [25] | 305 | 20,984 | 16,551 to 25,989 | 5.19 |
| Gheit et al., 2020 [26] | 117 | 23,932 | 16,529 to 32,698 | 5.09 |
| Hernandez et al., 2021 [27] | 302 | 5629 | 3313 to 8860 | 5.19 |
| Gonçalves et al., 2021 [18] | 255 | 67,843 | 61,731 to 73,534 | 5.18 |
| Sias et al., 2019 [28] | 55 | 23,636 | 13,228 to 37,020 | 4.91 |
| Santosh et al., 2018 [29] | 36 | 8333 | 1753 to 22,469 | 4.74 |
| Chuerduangphui et al., 2018 [30] | 110 | 43,636 | 34,202 to 53,422 | 5.08 |
| Garcia et al., 2018 [31] | 97 | 55,67 | 45,227 to 65,757 | 5.05 |
| Robbins et al., 2015 [32] | 64 | 31,25 | 20,242 to 44,059 | 4.95 |
| Blas et al., 2015 [33] | 99 | 44,444 | 34,454 to 54,776 | 5.06 |
| Ong et al., 2014 [34] | 173 | 34,682 | 27,620 to 42,280 | 5.14 |
| Total (random effects) | 2430 | 26,654 | 17,428 to 37,043 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bayram, G.; Simsek Yildirim, T.; Ertas, E.; Kanik, A. The Prevalence of Human Papillomavirus (HPV) Genotypes in the Oral Mucosae of HIV-Positive Individuals: A Systematic Review and Meta-Analysis. Microorganisms 2025, 13, 646. https://doi.org/10.3390/microorganisms13030646
Bayram G, Simsek Yildirim T, Ertas E, Kanik A. The Prevalence of Human Papillomavirus (HPV) Genotypes in the Oral Mucosae of HIV-Positive Individuals: A Systematic Review and Meta-Analysis. Microorganisms. 2025; 13(3):646. https://doi.org/10.3390/microorganisms13030646
Chicago/Turabian StyleBayram, Gul, Tugce Simsek Yildirim, Elif Ertas, and Arzu Kanik. 2025. "The Prevalence of Human Papillomavirus (HPV) Genotypes in the Oral Mucosae of HIV-Positive Individuals: A Systematic Review and Meta-Analysis" Microorganisms 13, no. 3: 646. https://doi.org/10.3390/microorganisms13030646
APA StyleBayram, G., Simsek Yildirim, T., Ertas, E., & Kanik, A. (2025). The Prevalence of Human Papillomavirus (HPV) Genotypes in the Oral Mucosae of HIV-Positive Individuals: A Systematic Review and Meta-Analysis. Microorganisms, 13(3), 646. https://doi.org/10.3390/microorganisms13030646