

Molecular Diagnosis of Human Monkeypox Virus during 2022–23 Outbreak: Preliminary Evaluation of Novel Real-Time Qualitative PCR Assays
 , , ,
, , ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Nucleic Acid Extraction
2.2. In-House MPXV PCR Assay
2.3. Research-Use-Only (RUO) Assays for the Molecular Diagnosis of MPXV
2.3.1. Novaplex MPXV Assay
2.3.2. STANDARD M10 MPX/OPX
2.3.3. RealCycler MONK-UX/MONK-GX v.2
2.3.4. RealStar Orthopoxvirus PCR Kit 1.0
2.4. Data Analysis
3. Results
3.1. Diagnostic Performance of four RUO MPXV Molecular Assays
3.2. Cross-Reactivity Assessment
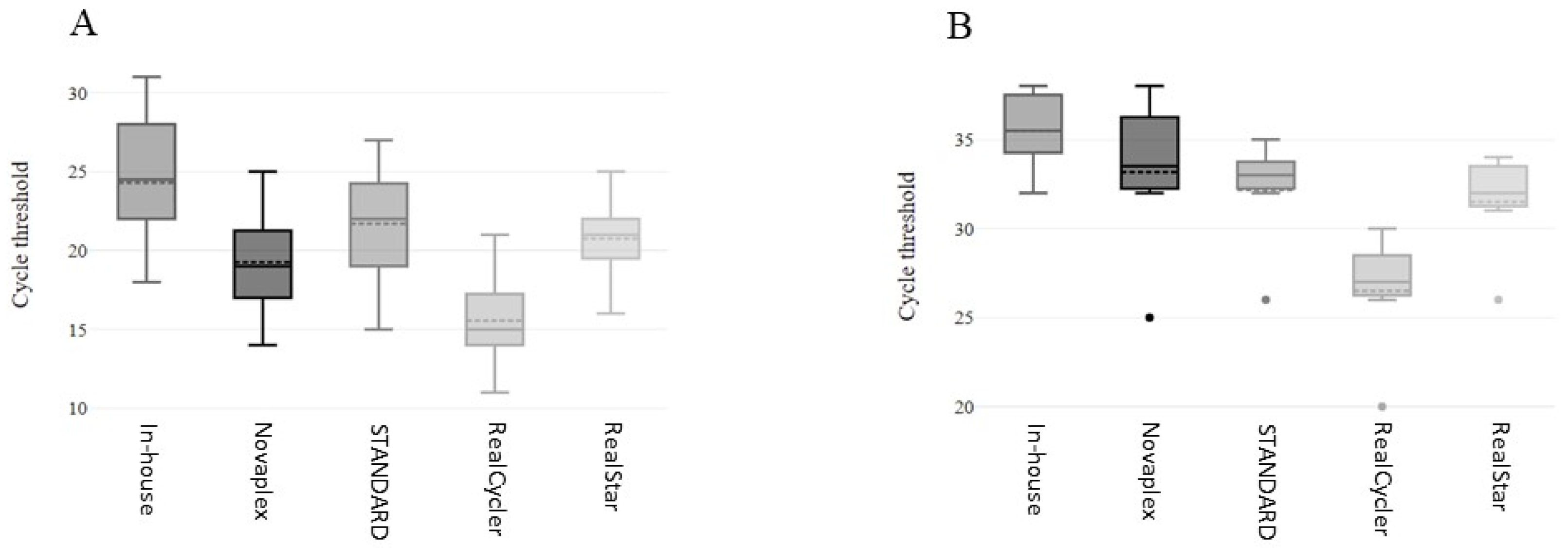
3.3. Comparison of Cycle Threshold Values
3.4. Clinical Summary of Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. 2022–23 Mpox (Monkeypox) Outbreak: Global Trends. Available online: https://worldhealthorg.shinyapps.io/mpx_global/ (accessed on 9 March 2024).
- World Health Organization. Mpox (Monkeypox). Available online: https://www.who.int/health-topics/monkeypox#tab=tab_1 (accessed on 9 March 2024).
- Kumar, N.; Acharya, A.; Gendelman, H.E.; Byrareddy, S.N. The 2022 outbreak and the pathobiology of the monkeypox virus. J. Autoimmun. 2022, 131, 102855. [Google Scholar] [CrossRef] [PubMed]
- Karagoz, A.; Tombuloglu, H.; Alsaeed, M.; Tombuloglu, G.; AlRubaish, A.A.; Mahmoud, A.; Smajlović, S.; Ćordić, S.; Rabaan, A.A.; Alsuhaimi, E. Monkeypox (mpox) virus: Classification, origin, transmission, genome organization, antiviral drugs, and molecular diagnosis. J. Infect. Public Health 2023, 16, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.W.; McFadden, G. Origin and evolution of poxviruses. In Origin and Evolution of Viruses, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2008; pp. 431–446. [Google Scholar]
- Shchelkunov, S.N.; Totmenin, A.V.; Babkin, I.V.; Safronov, P.F.; Ryazankina, O.I.; Petrov, N.A.; Gutorov, V.V.; Uvarova, E.A.; Mikheev, M.V.; Sisler, J.R.; et al. Human monkeypox and smallpox viruses: Genomic comparison. FEBS Lett. 2001, 509, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Shen-Gunther, J.; Cai, H.; Yufeng, W. A customized monkeypox virus genomic database (MPXV DB v1.0) for rapid sequence analysis and phylogenomic discoveries in CLC microbial genomics. Viruses 2023, 15, 40. [Google Scholar] [CrossRef] [PubMed]
- Von Magnus, P.; Andersen, E.K.; Petersen, K.B.; Birch-Andersen, A. A Pox-like Disease in Cynomolgus Monkeys. Acta Pathol. Microbiol. Scand. 2009, 46, 156–176. [Google Scholar] [CrossRef]
- Breman, J.G.; Kalisa-Ruti; Steniowski, M.V.; Zanotto, E.; Gromyko, A.I.; Arita, I. Human monkeypox, 1970–1979. Bull. World Health Organ. 1980, 58, 165–182. [Google Scholar] [PubMed]
- Barnewall, R.E.; Fisher, D.A.; Robertson, A.B.; Vales, P.A.; Knostman, K.A.; Bigger, J.E. Inhalational monkeypox virus infection in cynomolgus macaques. Front Cell. Infect. Microbiol. 2012, 2, 117. [Google Scholar] [CrossRef] [PubMed]
- Falendysz, E.A.; Lopera, J.G.; Doty, J.B.; Nakazawa, Y.; Crill, C.; Lorenzsonn, F.; Kalemba, L.N.; Ronderos, M.D.; Mejia, A.; Malekani, J.M.; et al. Characterization of Monkeypox virus infection in African rope squirrels (Funisciurus sp.). PLoS Negl. Trop. Dis. 2017, 11, e0005809. [Google Scholar] [CrossRef] [PubMed]
- Weiner, Z.P.; Salzer, J.S.; LeMasters, E.; Ellison, J.A.; Kondas, A.V.; Morgan, C.N.; Doty, J.B.; Martin, B.E.; Satheshkumar, P.S.; Olson, V.A.; et al. Characterization of Monkeypox virus dissemination in the black-tailed prairie dog (Cynomys ludovicianus) through in vivo bioluminescent imaging. PLoS ONE 2019, 14, e0222612. [Google Scholar] [CrossRef] [PubMed]
- Tiecco, G.; Degli Antoni, M.; Storti, S.; Tomasoni, L.R.; Castelli, F.; Quiros-Roldan, E. Monkeypox, a Literature Review: What Is New and Where Does This concerning Virus Come From? Viruses 2022, 14, 1894. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Mpox. Available online: https://www.cdc.gov/poxvirus/monkeypox/lab-personnel/index.html (accessed on 9 March 2024).
- World Health Organization. Laboratory Testing for the Monkeypox Virus—Interim Guidance 23 May 2022. Available online: https://www.who.int/publications/i/item/WHO-MPX-laboratory-2022.1 (accessed on 28 June 2023).
- Li, Y.; Zhao, H.; Wilkins, K.; Hughes, C.; Damon, I.K. Real-time PCR assays for the specific detection of monkeypox virus West African and Congo Basin strain DNA. J. Virol. Methods 2010, 169, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Ciccarese, G.; Di Biagio, A.; Bruzzone, B.; Guadagno, A.; Taramasso, L.; Oddenino, G.; Brucci, G.; Labate, L.; De Pace, V.; Mastrolonardo, M.; et al. Monkeypox outbreak in Genoa, Italy: Clinical, laboratory, histopathologic features, management, and outcome of the infected patients. J. Med. Virol. 2023, 95, e28560. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, R.P.; Fogel, R.; Limson, J. Overview of Diagnostic Methods, Disease Prevalence and Transmission of Mpox (Formerly Monkeypox) in Humans and Animal Reservoirs. Microorganisms 2023, 11, 1186. [Google Scholar] [CrossRef] [PubMed]
- Elbaz, M.; Halutz, O.; Ali, Y.; Adler, A. Diagnosis of Monkeypox infection: Validation of two diagnostic kits for viral detection using RT-PCR. J. Virol. Methods 2023, 312, 114653. [Google Scholar] [CrossRef] [PubMed]
- Tan, N.K.; Madona, C.P.; Taylor, J.F.; Fourali, L.H.; Sehmi, J.K.; Stone, M.J.; Pond, M.J.; Cliff, P.R.; Pope, C.F. Performance evaluation of the Viasure PCR assay for the diagnosis of monkeypox: A multicentre study. J. Clin. Virol. 2023, 158, 105350. [Google Scholar] [CrossRef] [PubMed]
- Papadakis, G.; Tran, T.; Druce, J.; Lim, C.K.; Williamson, D.A.; Jackson, K. Evaluation of 16 molecular assays for the detection of orthopox and mpox viruses. J. Clin. Virol. 2023, 161, 105424. [Google Scholar] [CrossRef] [PubMed]
- Paniz-Mondolfi, A.; Guerra, S.; Muñoz, M.; Luna, N.; Hernandez, M.M.; Patino, L.H.; Reidy, J.; Banu, R.; Shrestha, P.; Liggayu, B. Evaluation and validation of an RT-PCR assay for specific detection of monkeypox virus (MPXV). J. Med. Virol. 2023, 95, e28247. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| MPXV Real-Time PCR Assays | Accuracy (%) | Sensitivity (%) | Specificity (%) | Cohen’s Kappa | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| RealStar Orthopoxvirus PCR Kit 1.0 | 100 (90.6–100) | 100 (87.54–100) | 100 (72.25–100) | 1.00 (0.67–1.00) | 100 (87.5–100) | 100 (72.25–100) |
| RealCycler MONK-UX/-GX v.2 | 97.3 (86.2–99.5) | 96.3 (81.72–99.34) | 100 (72.25–100) | 0.93 (0.61–1.00) | 100 (87.1–100) | 90.9 (62.2–98.4) |
| Novaplex MPXV Assay | 100 (90.6–100) | 100 (87.54–100) | 100 (72.25–100) | 1.00 (0.67–1.00) | 100 (87.54–100) | 100 (72.25–100) |
| STANDARD M10 MPX/OPX | 97.3 (86.2–99.5) | 96.3 (81.72–99.34) | 100 (72.25–100) | 0.93 (0.61–1.00) | 100 (87.1–100) | 90.9 (62.2–98.4) |
| In-House | |||
|---|---|---|---|
| + | − | ||
| Novaplex MPXV Assay | + | 27 | 0 |
| − | 0 | 10 | |
| STANDARD M10 MPX/OPX | + | 26 | 0 |
| − | 1 | 10 | |
| RealCycler MONK-UX/MONK-GX v.2 | + | 26 | 0 |
| − | 1 | 10 | |
| RealStar Orthopoxvirus PCR Kit 1.0 | + | 27 | 0 |
| − | 0 | 10 | |
| Number | 14 |
| Age (y) | 34 (IQR: 27–43) |
| Male | 14 (100%) |
| Homosexual | 13 (92.9%) |
| Bisexual | 1 (7.1%) |
| Smallpox vaccination history | 1 (7.1%) |
| Other sexually transmitted diseases | 11 (78.6%) |
| HIV | 3 (21.4%) |
| Syphilis | 8 (57.1%) |
| HR-HPV | 5 (35.7%) |
| Ureaplasma/Mycoplasma spp. | 5 (35.7%) |
| Chlamydia trachomatis | 1 (7.1%) |
| Neisseria gonorrhoeae | 3 (21.4%) |
| PrEP | 3 (21.4%) |
| Onset of illness | |
| Prodromal signs/symptoms | 11 (78.6%) |
| Fever | 5 (35.7%) |
| Myalgia | 1 (7.1%) |
| Asthenia | 3 (21.4%) |
| Headache | 2 (14.3%) |
| Urticaria | 1 (7.1%) |
| Mucorrhea | 1 (7.1%) |
| Rectorrhagia/Proctorrhagia | 2 (14.3%) |
| Ano/Rectal pain | 5 (35.7%) |
| Itch | 3 (21.4%) |
| Pharyngodynia | 2 (14.3%) |
| Lymphadenopathy | 4 (28.6%) |
| Tenesmus | 1 (7.1%) |
| Skin/mucosal manifestation at diagnosis | 12 (85.7%) |
| Approximate number of lesions (mucosal or cutaneous) | |
| <10 | 9 (64.3%) |
| 10–20 | 3 (21.4%) |
| >20 | 2 (14.3%) |
| Resolution without scarring | 12 (85.7%) |
| Unconventional specimens with monkeypox viral DNA (a) | |
| Blood (Whole blood, serum or plasma) | 4 of 7 (57%) |
| Nasopharyngeal swab | 6 of 10 (60%) |
| Rectal/Anal swab | 7 of 7 (100%) |
| Antiviral therapy | 1 (7.1%) |
| Hospitalization | 3 (21.4%) |
| Days of hospital admission | 4 (2–5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Pace, V.; Bruzzone, B.; Ricucci, V.; Domnich, A.; Guarona, G.; Garzillo, G.; Qosja, R.; Ciccarese, G.; Di Biagio, A.; Orsi, A.; et al. Molecular Diagnosis of Human Monkeypox Virus during 2022–23 Outbreak: Preliminary Evaluation of Novel Real-Time Qualitative PCR Assays. Microorganisms 2024, 12, 664. https://doi.org/10.3390/microorganisms12040664
De Pace V, Bruzzone B, Ricucci V, Domnich A, Guarona G, Garzillo G, Qosja R, Ciccarese G, Di Biagio A, Orsi A, et al. Molecular Diagnosis of Human Monkeypox Virus during 2022–23 Outbreak: Preliminary Evaluation of Novel Real-Time Qualitative PCR Assays. Microorganisms. 2024; 12(4):664. https://doi.org/10.3390/microorganisms12040664
Chicago/Turabian StyleDe Pace, Vanessa, Bianca Bruzzone, Valentina Ricucci, Alexander Domnich, Giulia Guarona, Giada Garzillo, Rexhina Qosja, Giulia Ciccarese, Antonio Di Biagio, Andrea Orsi, and et al. 2024. "Molecular Diagnosis of Human Monkeypox Virus during 2022–23 Outbreak: Preliminary Evaluation of Novel Real-Time Qualitative PCR Assays" Microorganisms 12, no. 4: 664. https://doi.org/10.3390/microorganisms12040664
APA StyleDe Pace, V., Bruzzone, B., Ricucci, V., Domnich, A., Guarona, G., Garzillo, G., Qosja, R., Ciccarese, G., Di Biagio, A., Orsi, A., & Icardi, G. (2024). Molecular Diagnosis of Human Monkeypox Virus during 2022–23 Outbreak: Preliminary Evaluation of Novel Real-Time Qualitative PCR Assays. Microorganisms, 12(4), 664. https://doi.org/10.3390/microorganisms12040664