

Septic Transfusion Reactions Involving Burkholderia cepacia Complex: A Review
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
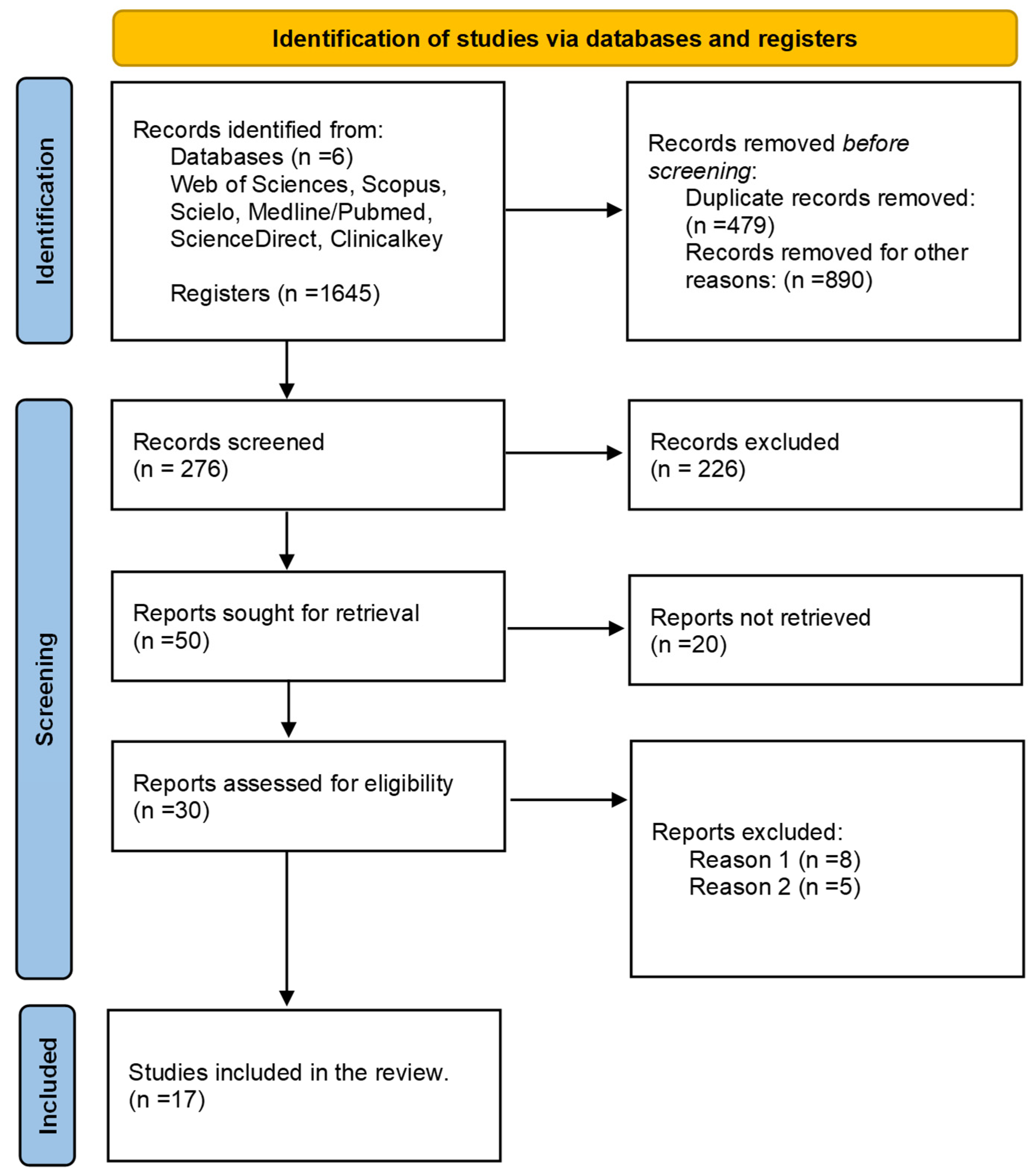
2.1. PICO Question and Search Strategy
2.2. Study Inclusion/Exclusion Criteria
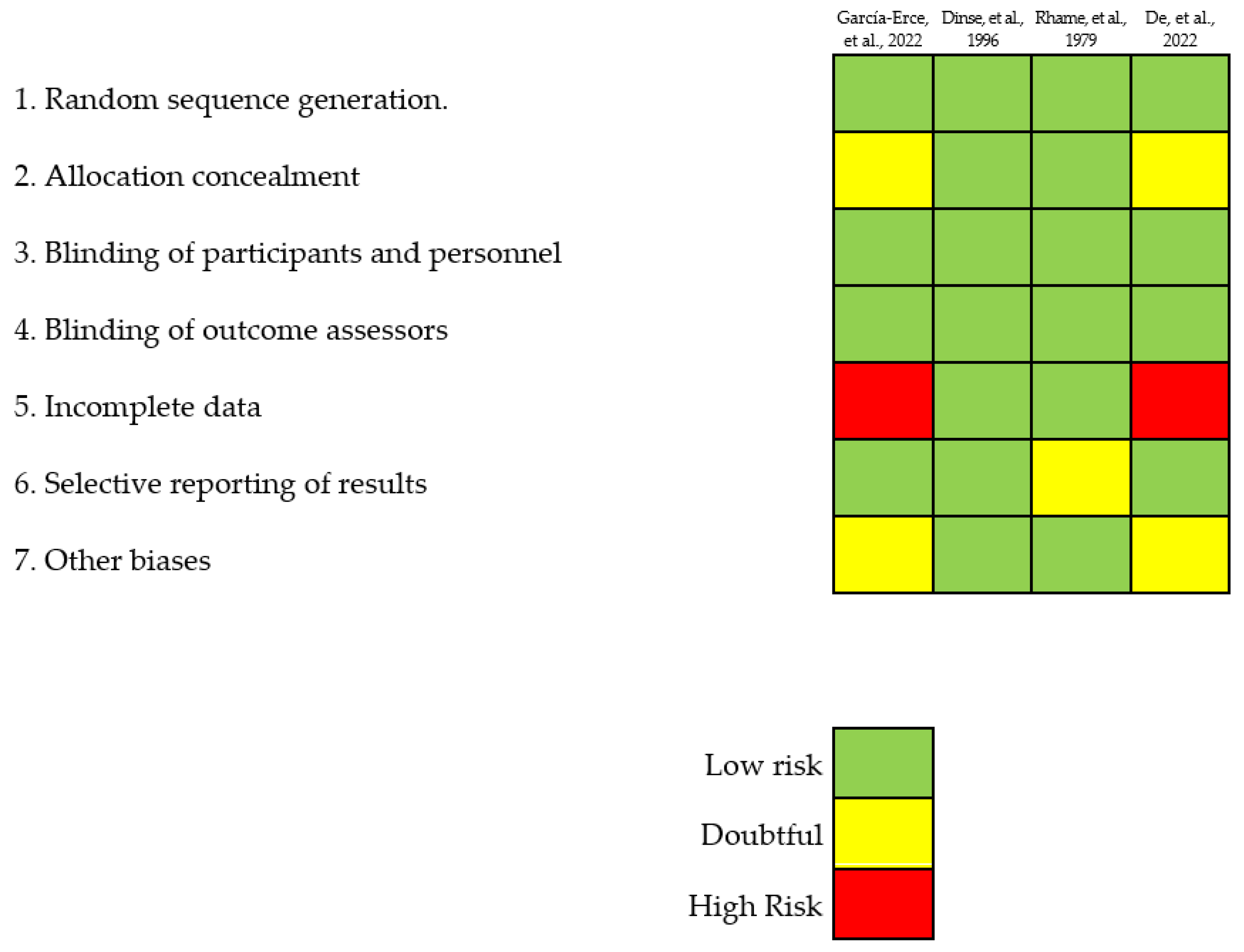
2.3. Quality Assessment and Risk of Bias
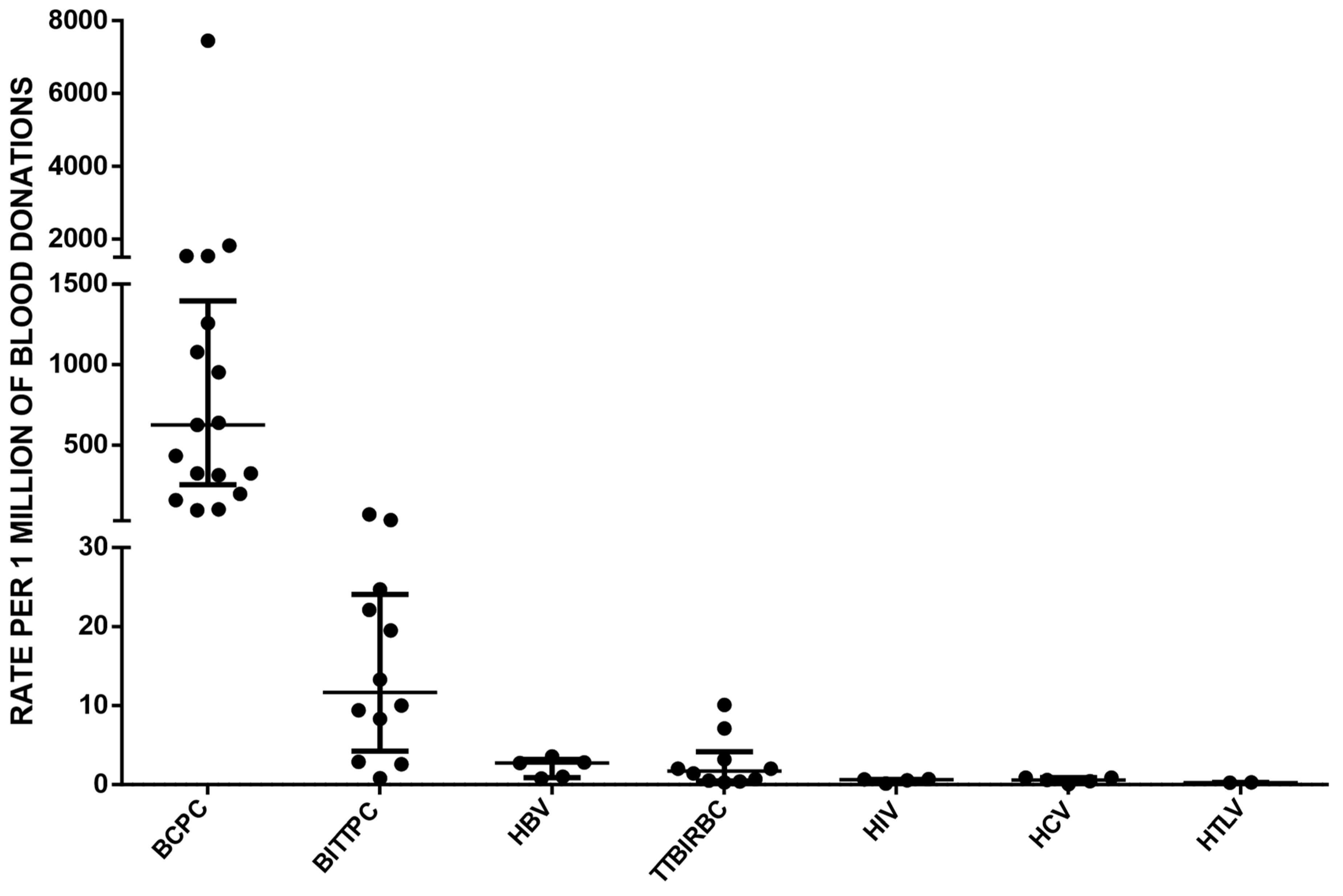
3. Results
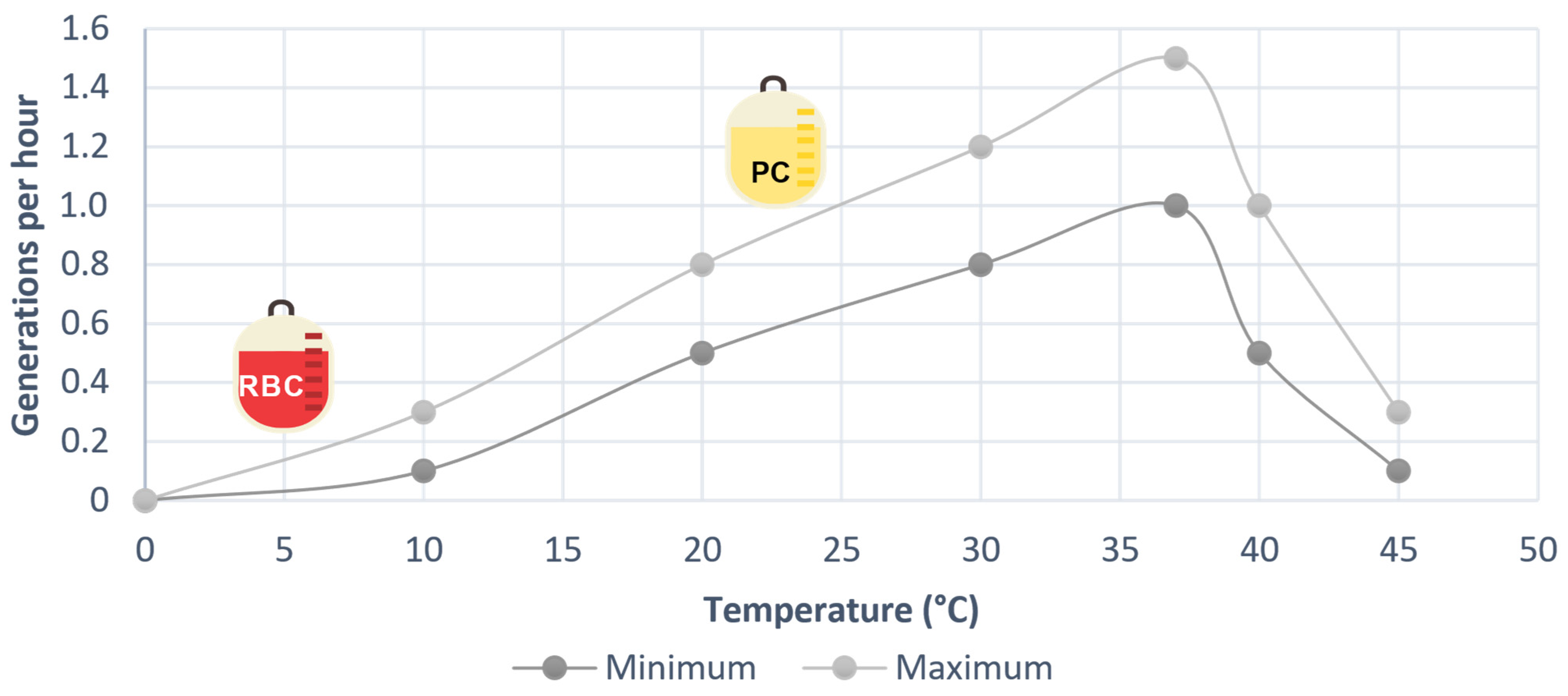
4. Discussion
5. Conclusions and Recommendations
- Ensure healthcare personnel adhere to hand hygiene and WHO guidelines for blood donation, processing, and transfusion.
- Provide continuous training and monitoring of personnel in cleaning and disinfection procedures for blood extraction, avoiding palpation after disinfection.
- Use single-use disposable devices with a mixture of disinfectants for cleaning the puncture area in potential blood donors’ arms.
- Periodically evaluate cleaning substances used on surfaces to determine their sterility.
- Ensure biomedical and cold chain equipment used for blood components is regularly cleaned and disinfected to prevent contamination.
- Reduce PC storage times to less than 85 h.
- Implement pathogen inactivation technologies before 24 h after collection.
- Perform culture methods for 100% of PCs after 36 h of storage and before transfusion.
- Implement rapid detection methods for bacterial contamination prior to transfusion.
- Conduct detailed and rigorous visual inspections of all blood components and tubing before dispatch and transfusion.
- Accurately identify non-hemolytic febrile adverse transfusion reactions and consider bacterial contamination as a possible cause.
- Continuously train healthcare personnel on adverse transfusion reactions to ensure timely identification and management.
- Encourage reporting of adverse events to hemovigilance programs for analysis and improvement plans to prevent such events.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sfeir, M. Burkholderia cepacia Complex Infections: More Complex than the Bacterium Name Suggest. J. Infect. 2018, 77, 166–170. [Google Scholar] [CrossRef]
- Tavares, M.; Kozak, M.; Balola, A.; Sá-Correia, I. Burkholderia cepacia Complex Bacteria: A Feared Contamination Risk in Water-Based Pharmaceutical Products. Clin. Microbiol. Rev. 2020, 33, e00139-19. [Google Scholar] [CrossRef]
- Rawat, A.; Bhattad, S.; Singh, S. Chronic Granulomatous Disease. Indian. J. Pediatr. 2016, 83, 345–353. [Google Scholar] [CrossRef]
- Department of Microbiology, Topiwala National Medical College, Mumbai, Maharashtra, India; De, A.; Shastri, J.S.; Malak, N.I.; Kedia, M.; Sisodia, H. Unusual Violet Coloured Pigment Produced by Burkholderia cepacia Complex—A Report of Five Cases from a Tertiary Care Hospital in Mumbai. JMSH 2022, 8, 173–176. [Google Scholar] [CrossRef]
- Abdallah, M.; Abdallah, H.A.; Memish, Z.A. Burkholderia cepacia Complex Outbreaks among Non-Cystic Fibrosis Patients in the Intensive Care Units: A Review of Adult and Pediatric Literature. Infez Med. 2018, 26, 299–307. [Google Scholar]
- Fehlberg, L.C.C.; Andrade, L.H.S.; Assis, D.M.; Pereira, R.H.V.; Gales, A.C.; Marques, E.A. Performance of MALDI-ToF MS for Species Identification of Burkholderia cepacia Complex Clinical Isolates. Diagn. Microbiol. Infect. Dis. 2013, 77, 126–128. [Google Scholar] [CrossRef]
- Marrs, E.C.L.; Perry, A.; Perry, J.D. Evaluation of Three Culture Media for Isolation of Burkholderia cepacia Complex from Respiratory Samples of Patients with Cystic Fibrosis. Microorganisms 2021, 9, 2604. [Google Scholar] [CrossRef]
- García-Erce, J.; Grasa, J.; Solano, V.; Gimeno, J.; López, A.; Hernández, M.; Marco, M.; Arribas, J.; Giralt, M. Bacterial Contamination of Blood Components Due to Burkholderia cepacia Contamination from Clorhexidine Bottles. Vox Sang. 2002, 83, 70–71. [Google Scholar] [CrossRef]
- Martina, P.F.; Martinez, M.; Rivas, S.; Leguizamón, L.; Von Specht, M.; Ferreras, J. Burkholderia cepacia Complex: 11 Years of Surveillance in Patients with Cystic Fibrosis in Posadas, Argentina. Rev. Argent. Microbiol. 2020, 52, 176–182. [Google Scholar] [CrossRef]
- Nieves, W.; Asakrah, S.; Qazi, O.; Brown, K.; Kurtz, J.; Aucoin, D.; McLachlan, J.; Roy, C.; Morici, L. A Naturally Derived Outer-Membrane Vesicle Vaccine Protects against Lethal Pulmonary Burkholderia pseudomallei Infection. Vaccine 2011, 29, 8381–8389. [Google Scholar] [CrossRef]
- Vardi, A.; Sirigou, A.; Lalayanni, C.; Kachrimanidou, M.; Kaloyannidis, P.; Saloum, R.; Anagnostopoulos, A.; Sotiropoulos, D. An Outbreak of Burkholderia cepacia Bacteremia in Hospitalized Hematology Patients Selectively Affecting Those with Acute Myeloid Leukemia. Am. J. Infect. Control 2013, 41, 312–316. [Google Scholar] [CrossRef]
- Raddaoui, A.; Ben Tanfous, F.; Chebbi, Y.; Mabrouk, A.; Achour, W. An Intermittent Outbreak of Burkholderia cepacia Contaminating Hematopoietic Stem Cells Resulting in Infusate-Related Blood Stream Infections. J. Infect. Prev. 2022, 23, 75–78. [Google Scholar] [CrossRef]
- WHO. The Clinical Use of Blood in Medicine, Obstetrics, Paediatrics, Surgery & Anaesthesia Trauma & Burns; World Health Organization: Geneva, Switzerland, 2001.
- Ackfeld, T.; Schmutz, T.; Guechi, Y.; Le Terrier, C. Blood Transfusion Reactions—A Comprehensive Review of the Literature Including a Swiss Perspective. J. Clin. Med. 2022, 11, 2859. [Google Scholar] [CrossRef]
- Justiz Vaillant, A.; Sticco, K. Transfusion Transmitted Disease. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Bloch, E.; Benjamin, R.; Ramirez-Arcos, S. Chapter Bacterial Contamination of Blood Components. In Rossi’s Principles of Transfusion Medicine; Wiley Blackwell: Hoboken, NJ, USA, 2022; pp. 533–542. ISBN 978-1-119-71978-6. [Google Scholar]
- Ramirez-Arcos, S.; Goldman, M. Bacterial Contamination. In AABB Transfusion Reactions; AABB: Bethesda, MD, USA, 2021; pp. 115–164. ISBN 978-1-56395-413-9. [Google Scholar]
- García-Otálora, M.-A.; Núñez-Ahumada, M.-A.; Kuperman, S.; Oliveira-Leitão, L.; Silveira, F.; Martins, R.; Pesántez-Pesántez, M.; Gutiérrez, J.-L.; Alcaráz-Paredes, R.-E.; Castagnola, E.R.M.; et al. Bacterial Contamination and Sepsis Associated with Transfusion: Current Status in Latin America. Ann. Blood 2021, 6, 26. [Google Scholar] [CrossRef]
- Prax, M.; Spindler-Raffel, E.; McDonald, C.P.; Bearne, J.; Satake, M.; Kozakai, M.; Rojo, J.; Hanschmann, K.O.; Lambrecht, B.; Grundmann, U.; et al. Establishment of Transfusion-relevant Bacteria Reference Strains for Red Blood Cells. Vox Sang. 2021, 116, 692–701. [Google Scholar] [CrossRef]
- Spindler-Raffel, E.; Benjamin, R.J.; McDonald, C.P.; Ramirez-Arcos, S.; Aplin, K.; Bekeredjian-Ding, I.; De Korte, D.; Gabriel, C.; Gathof, B.; Hanschmann, K.-M.; et al. Enlargement of the WHO International Repository for Platelet Transfusion-Relevant Bacteria Reference Strains. Vox Sang. 2017, 112, 713–722. [Google Scholar] [CrossRef]
- Störmer, M.; Arroyo, A.; Brachert, J.; Carrero, H.; Devine, D.; Epstein, J.S.; Gabriel, C.; Gelber, C.; Goodrich, R.; Hanschmann, K.-M.; et al. Establishment of the First International Repository for Transfusion-Relevant Bacteria Reference Strains: ISBT Working Party Transfusion-Transmitted Infectious Diseases (WP-TTID), Subgroup on Bacteria: International Repository for Transfusion-Relevant Bacteria References. Vox Sang. 2012, 102, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Taha, M.; Kyluik-Price, D.; Kumaran, D.; Scott, M.D.; Toyofuku, W.; Ramirez-Arcos, S. Bacterial Survival in Whole Blood Depends on Plasma Sensitivity and Resistance to Neutrophil Killing. Transfusion 2019, 59, 3674–3682. [Google Scholar] [CrossRef]
- Matsumoto, M.; Kozakai, M.; Furuta, R.A.; Matsubayashi, K.; Satake, M. Association of Staphylococcus aureus in Platelet Concentrates with Skin Diseases in Blood Donors: Limitations of Cultural Bacterial Screening. Transfusion 2022, 62, 621–632. [Google Scholar] [CrossRef]
- Currie, L.; Harper, J.; Allan, H.; Connor, J. Inhibition of Cytokine Accumulation and Bacterial Growth during Storage of Platelet Concentrates at 4 Degrees C with Retention of in Vitro Functional Activity. Transfusion 1997, 37, 18–24. [Google Scholar] [CrossRef]
- Hong, H.; Xiao, W.; Lazarus, H.M.; Good, C.E.; Maitta, R.W.; Jacobs, M.R. Detection of Septic Transfusion Reactions to Platelet Transfusions by Active and Passive Surveillance. Blood 2016, 127, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, M.R.; Good, C.E.; Lazarus, H.M.; Yomtovian, R.A. Relationship between Bacterial Load, Species Virulence, and Transfusion Reaction with Transfusion of Bacterially Contaminated Platelets. Clin. Infect Dis. 2008, 46, 1214–1220. [Google Scholar] [CrossRef]
- Gammon, R.R.; Reik, R.A.; Stern, M.; Vassallo, R.R.; Waxman, D.A.; Young, P.P.; Benjamin, R.J. Acquired Platelet Storage Container Leaks and Contamination with Environmental Bacteria: A Preventable Cause of Bacterial Sepsis. Transfusion 2022, 62, 641–650. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Rhame, F.; McCullough, J.; Cameron, S.; Streifel, A.; White, K. Pseudomonas cepacia Infections Caused by Thawing Cryoprecipitate in a Contaminated Water Bath (Abstract). In Proceedings of the American Association of Blood Banks 32nd Annual Meeting, Las Vegas, NV, USA, 3–8 November 1979; Volume 19, p. 653. [Google Scholar]
- Dinse, H.; Deusch, H. Sepsis Following Autologous Blood Transfusion. Anaesthesist 1996, 45, 460–463. [Google Scholar] [CrossRef]
- ISBT, I. Proposed Standard Definitions for Surveillance of Non Infectious Adverse Transfusion Reactions. Incorporating Correction to TRALI Definition (as Adopted June 2013). In An Effective Tool for Improving Transfusion Safety, 1st ed.; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2012; Volume 1, Appendix-B. [Google Scholar]
- Ramirez-Arcos, S.; Garcia-Otalora, M.; McDonald, C. ISBT Transfusion-Transmitted Infectious Diseases Working Party, Subgroup on Bacteria Microbiological Environmental Contamination in the Blood Supply Chain: An International Survey by the Bacterial Subgroup of the ISBT Transfusion-Transmitted Infectious Diseases Working Party. Vox Sang. 2023, 2023, 4–10. [Google Scholar] [CrossRef]
- Taylor, C.J.; Anderson, A.J.; Wilkinson, S.G. Phenotypic Variation of Lipid Composition in Burkholderia cepacia: A Response to Increased Growth Temperature Is a Greater Content of 2-Hydroxy Acids in Phosphatidylethanolamine and Ornithine Amide Lipid. Microbiology 1998, 144, 1737–1745. [Google Scholar] [CrossRef]
- Moody, S.C.; Bull, J.C.; Dudley, E.; Loveridge, E.J. The Impact of Combinatorial Stress on the Growth Dynamics and Metabolome of Burkholderia mesoacidophila Demonstrates the Complexity of Tolerance Mechanisms. J. Appl. Microbiol. 2019, 127, 1521–1531. [Google Scholar] [CrossRef]
- Mariappan, V.; Vellasamy, K.M.; Hashim, O.H.; Vadivelu, J. Profiling of Burkholderia cepacia Secretome at Mid-Logarithmic and Early-Stationary Phases of Growth. PLoS ONE 2011, 6, e26518. [Google Scholar] [CrossRef]
- Bertrand, R.L. Lag Phase Is a Dynamic, Organized, Adaptive, and Evolvable Period That Prepares Bacteria for Cell Division. J. Bacteriol. 2019, 201, 10–128. [Google Scholar] [CrossRef]
- White, J.G. Platelets Are Covercytes, Not Phagocytes: Uptake of Bacteria Involves Channels of the Open Canalicular System. Platelets 2005, 16, 121–131. [Google Scholar] [CrossRef]
- Yousuf, B.; Pasha, R.; Pineault, N.; Ramirez-Arcos, S. Contamination of Platelet Concentrates with Staphylococcus Aureus Induces Significant Modulations in Platelet Functionality. Vox Sang. 2022, 117, 1318–1322. [Google Scholar] [CrossRef] [PubMed]
- Kamel, H.; Ramirez-Arcos, S.; McDonald, C.; ISBT Transfusion-Transmitted Infectious Disease Bacterial Working Party Bacterial Subgroup. The International Experience of Bacterial Screen Testing of Platelet Components with Automated Microbial Detection Systems: An Update. Vox Sang. 2022, 117, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Boudjedir, K.; Drougard, S.; Freyche, C. 19eme Rapport National D’hemovigilance, 1st ed.; Agence nationale de sécurité du médicament et des produits de santé: Paris, France, 2023. [Google Scholar]
- Narayan, S.; Poles, D. The 2021 Annual SHOT Report on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group; SHOT: Manchester, UK, 2022; ISBN 978-1-9995968-4-2. [Google Scholar]
- Morley, S.; Sadani, D.; Badami, S. Haemovigilance Annual Report. 2021, 1st ed.; NZBlood te Ratonga Toto O Aotearoa: Auckland, New Zealand, 2022; Available online: https://www.nzblood.co.nz/assets/Uploads/NZBS-Annual-HV-Report-2021-Hi-Res-Compressed-2022-08-16.pdf (accessed on 30 July 2023).
- Satake, M.; Kozakai, M.; Matsumoto, M.; Matsubayashi, K.; Taira, R.; Goto, N. Platelet Safety Strategies in Japan: Impact of Short Shelf Life on the Incidence of Septic Reactions. Transfusion 2020, 60, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Organización Panamericana de la Salud. Suministro de Sangre Para Transfusiones En Los Países de América Latina y El Caribe 2016–2017, 1st ed.; OPS: Washington, DC, USA, 2020; ISBN 978-92-75-32171-3. [Google Scholar]
- Ebner, W.; Meyer, E.; Schulz-Huotari, C.; Scholz, R.; Zilow, G.; Daschner, F. Pseudocontamination of Blood Components with Burkholderia cepacia during Quality Controls. Transfus. Med. 2005, 15, 241–242. [Google Scholar] [CrossRef]
- Panlilio, A.L.; Beck-Sague, C.M.; Siegel, J.D.; Anderson, R.L.; Yetts, S.Y.; Clark, N.C.; Duer, P.N.; Thomassen, K.A.; Vess, R.W.; Hill, B.C.; et al. Infections and Pseudoinfections Due to Povidone-Iodine Solution Contaminated with Pseudomonas cepacia. Clin. Infect. Dis. 1992, 14, 1078–1083. [Google Scholar] [CrossRef]
- Vonberg, R.; Gastmeier, P. Hospital-Acquired Infections Related to Contaminated Substances. J. Hosp. Infect. 2007, 65, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Fadeyi, E.A.; Wagner, S.J.; Goldberg, C.; Lu, T.; Young, P.; Bringmann, P.W.; Meier, N.M.; Namen, A.M.; Benjamin, R.J.; Palavecino, E. Fatal Sepsis Associated with a Storage Container Leak Permitting Platelet Contamination with Environmental Bacteria after Pathogen Reduction. Transfusion 2021, 61, 641–648. [Google Scholar] [CrossRef]
- Green, A.; Chiaraviglio, L.; Truelson, K.; Zulauf, K.; Cui, M.; Zhang, Z.; Ware, M.; Flegel, W.; Haspel, R.; Yu, E.; et al. RND Pump-Mediated Efflux of Amotosalen, a Compound Used in Pathogen Inactivation Technology to Enhance Safety of Blood Transfusion Products, May Compromise Its Gram-Negative Anti-Bacterial Activity. mSphere 2023, 20, e00673-22. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Equation |
|---|---|
| Medline/PubMed | ((“Burkholderia*” [Title/Abstract] OR “cepacia*” [Title/Abstract] OR “Burkholderia cepacia” [Title/Abstract] OR “Pseudomonas cepacia” [Title/Abstract] AND “septic transfusion reaction” [Title/Abstract] OR “transfusion adverse event” [Title/Abstract] OR “transfusion*” [Title/Abstract])) |
| Web of Science | (“Burkholderia*” or “cepacia*” or “Burkholderia cepacia” or “Pseudomonas cepacia”) AND (“septic transfusion reaction” OR “transfusion adverse event” OR “transfusion*”) |
| Scopus | (TITLE-ABS-KEY (“Burkholderia*”) AND TITLE-ABS-KEY (“septic transfusion reaction”) OR TITLE-ABS-KEY (“Burkholderia cepacia”) OR TITLE-ABS-KEY (“Pseudomonas cepacia”) OR TITLE-ABS-KEY AND (“transfusion adverse event”) OR TITLE-ABS-KEY (“transfusion*”) |
| Scielo | “Burkholderia*” or “cepacia*” or “Burkholderia cepacia” or “Pseudomonas cepacia” AND “septic transfusion reaction” OR “transfusion adverse event” OR “transfusion*” |
| ScienceDirect | “Burkholderia cepacia or “Pseudomonas cepacia” AND “Blood product” |
| ClinicalKey | “Burkholderia cepacia or “Pseudomonas cepacia” AND “Blood product” |
| Case | Sex | Age | Primary Diagnosis | Signs and Symptoms during/after Transfusion | Time Elapsed between Transfusion and Onset of Symptoms | Storage Time of the Blood Component before Transfusion | Transfused Blood Component | Microbiological Culture of the Patient | Microbiological Culture of Blood Units | Treatment Post Sepsis Diagnosis | Outcome | Source of Contamination | Imputability of TTBI | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Unknown | Unknown | Unknown | Septicemia | Not reported | Not reported | Cryoprecipitate pool | Growth of B. cepacia | Not reported | Not reported | Not reported | Serological bath where the cryoprecipitates were thawed | Definitive | [29] |
| 2 | Unknown | Unknown | Unknown | Septicemia | Not reported | Not reported | Cryoprecipitate pool | Growth of B. cepacia | Not reported | Not reported | Not reported | Serological bath where the cryoprecipitates were thawed | Definitive | [29] |
| 3 | Unknown | Unknown | Unknown | Mediastinal wound infection | Not reported | Not reported | Cryoprecipitate pool | Growth of B. cepacia | Not reported | Not reported | Not reported | Serological bath where the cryoprecipitates were thawed | Definitive | [29] |
| 4 | Female | 58 | Postoperative vaginal hysterectomy | Fever, signs and symptoms of DIC; progressed to septic shock | Not reported | Not reported | Two red blood cell units | Growth of B. capacia and Serratia marcesens | Growth of B. capacia and Serratia marcesens. At 24 h, later growth of Staphylococcus epidermidis | Not reported | Not reported | Unknown | Definitive | [30] |
| 5 | Male | 68 | Rectal cancer | Fever, chills, shock, tachycardia, hypotension, stupor; onset immediately after transfusion | Immediately start the transfusion | Not reported | Red blood cell unit | Growth of B. cepacia | Growth of B. cepacia | Not reported | Not reported | 0.5% chlorhexidine aqueous solution | Definitive | [8] |
| 6 | Male | 28 | Acute lymphoblastic leukemia | Fever, tachycardia | Not reported | Not reported | Red blood cell unit | Growth of B. cepacia | Not performed | Not reported | Not reported | 0.5% chlorhexidine aqueous solution | Probable | [8] |
| 7 | Female | 59 | Gastric bleeding | Fever, chills, shock, tachycardia | Not reported | Not reported | Red blood cell unit | Growth of B. cepacia | Not performed | Not reported | Not reported | 0.5% chlorhexidine aqueous solution | Probable | [8] |
| 8 | Female | * | Myelodysplastic syndrome, arterial hypertension, hypothyroidism | Diaphoresis, dyspnea, tachycardia, tachypnea, fever, septic shock | 25 min | 4 days | Apheresis PC | Growth of B. cepacia | Growth of B. cepacia | Cefepime and vancomycin | Hospitalization; she died on 03/10/2021 due to underlying disease | Unknown | Definitive | Institutional Haemovigilance Program. Sociedad de Cirugía de Bogotá-Hospital de San José |
| 9 | Male | * | Myelodysplastic syndrome | Diaphoresis, dyspnea, tachycardia, tachypnea, fever, septic shock | 25 min | 5 days | Apheresis PC | Growth of B. cepacia | Growth of B. cepacia | Piperacillin tazobactam and vancomycin and daptomycin | Required ICU; he died 12/15/2020 due to underlying disease | Unknown | Definitive | Institutional Haemovigilance Program. Sociedad de Cirugía de Bogotá-Hospital de San José |
| 10 | Male | * | myelodysplastic syndrome- hemosiderosis | Severe dyspnea, diaphoresis, tachycardia, fever, tachypnea, ambient desaturation, hypotension, septic shock | 35 min | 5 days | Apheresis PC | Growth of B. cepacia | Growth of B. cepacia | Meropenem and vancomycin | Required ICU; recovered from transfusion sepsis but was infected with COVID-19 and passed away 10/27/2020 | Unknown | Definitive | Institutional Haemovigilance Program. Sociedad de Cirugía de Bogotá-Hospital de San José |
| 11 | Male | 57 | Acute myeloid leukemia | Septicemia | Not reported | Not reported | PCs and red blood cells | Growth of B. cepacia violet pigment | Not reported | Ceftazidime, cotrimoxazole and Imipenem | Not reported | Unknown | Possible | [4] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salamanca-Pachon, M.; Guayacan-Fuquene, N.I.; Garcia-Otalora, M.-A. Septic Transfusion Reactions Involving Burkholderia cepacia Complex: A Review. Microorganisms 2024, 12, 40. https://doi.org/10.3390/microorganisms12010040
Salamanca-Pachon M, Guayacan-Fuquene NI, Garcia-Otalora M-A. Septic Transfusion Reactions Involving Burkholderia cepacia Complex: A Review. Microorganisms. 2024; 12(1):40. https://doi.org/10.3390/microorganisms12010040
Chicago/Turabian StyleSalamanca-Pachon, Margarita, Nohora Isabel Guayacan-Fuquene, and Michel-Andres Garcia-Otalora. 2024. "Septic Transfusion Reactions Involving Burkholderia cepacia Complex: A Review" Microorganisms 12, no. 1: 40. https://doi.org/10.3390/microorganisms12010040
APA StyleSalamanca-Pachon, M., Guayacan-Fuquene, N. I., & Garcia-Otalora, M.-A. (2024). Septic Transfusion Reactions Involving Burkholderia cepacia Complex: A Review. Microorganisms, 12(1), 40. https://doi.org/10.3390/microorganisms12010040