
Development of a Highly Sensitive Nested PCR and Its Application for the Diagnosis of Cutaneous Leishmaniasis in Sri Lanka

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area and Samples
2.2. Giemsa Stained Slit Skin Smears
2.3. Molecular Diagnosis
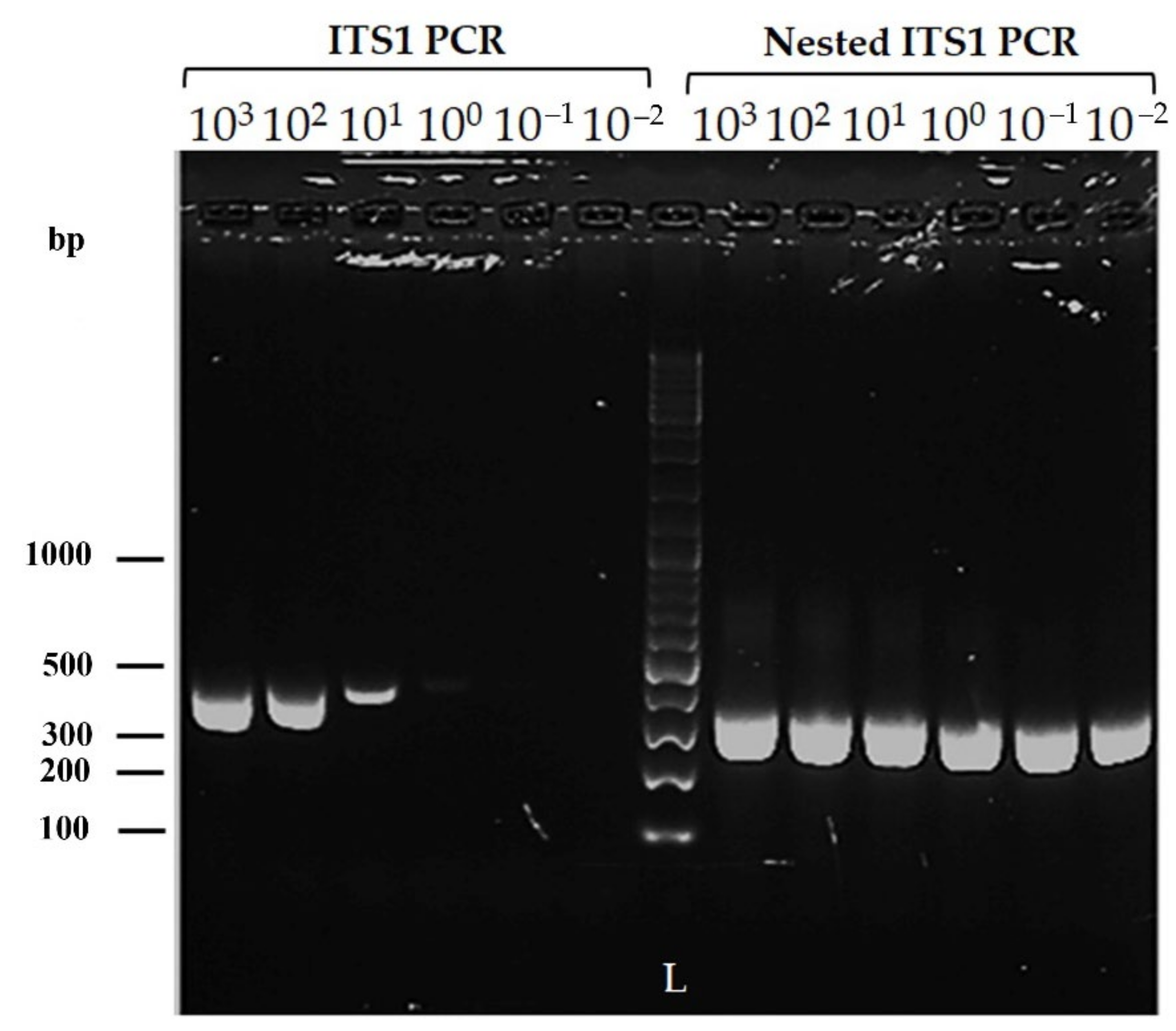
2.3.1. Sensitivity of the Modified Nested ITS1 PCR
2.3.2. DNA Extraction
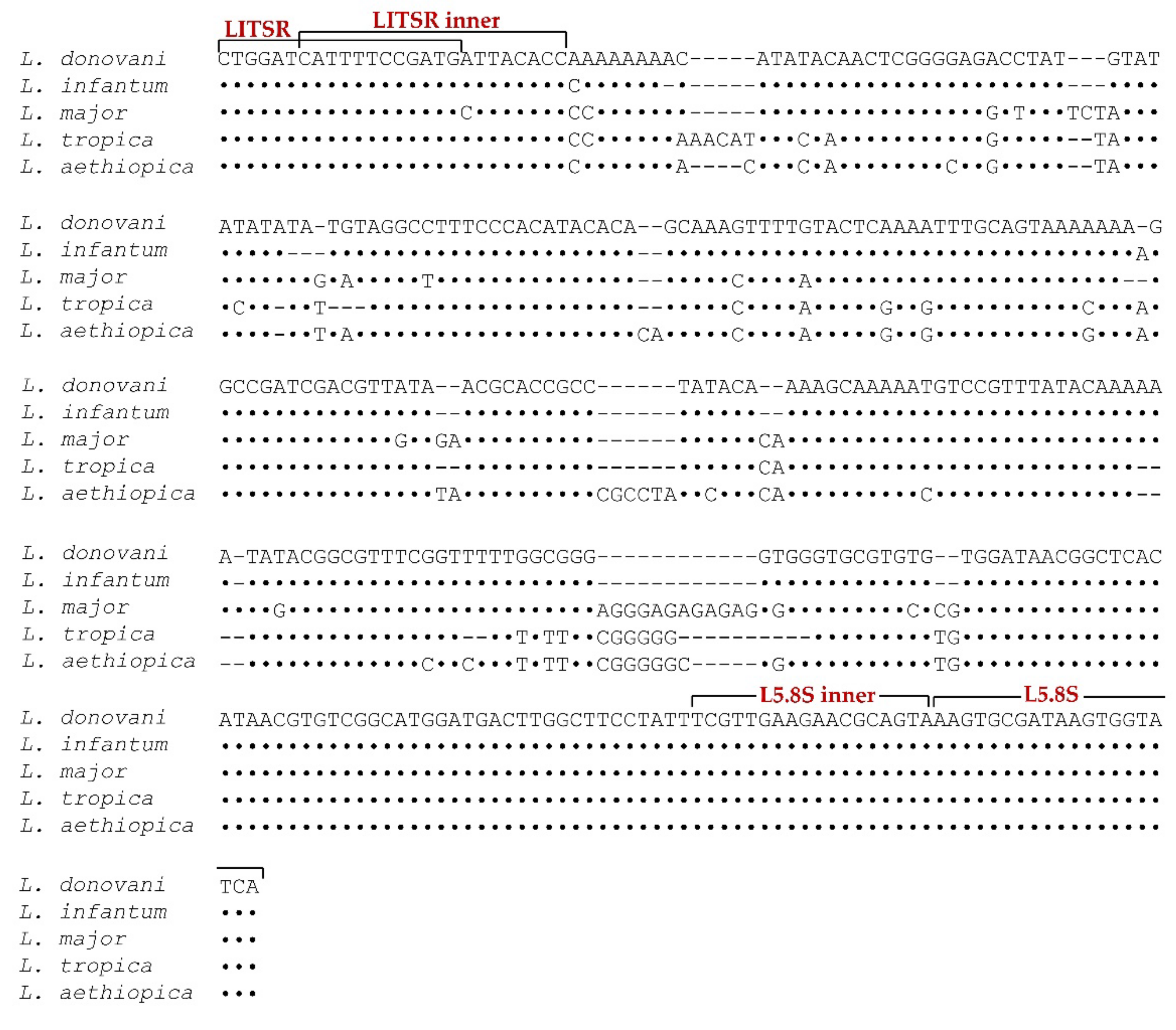
2.3.3. Modified Nested ITS1 PCR
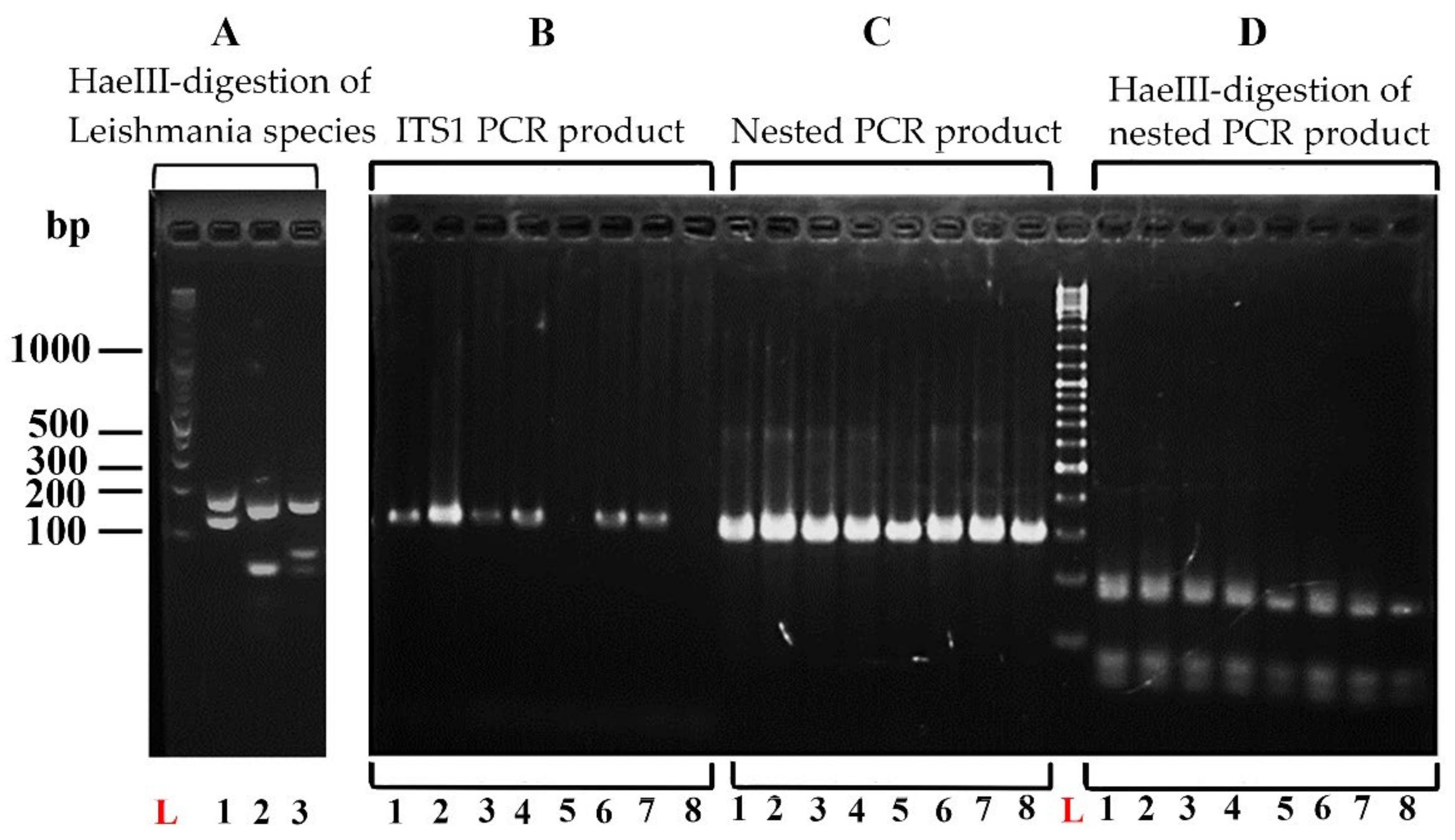
2.3.4. Restriction Fragment Length Polymorphism (RFLP) Analysis
2.4. Data Management and Statistical Analysis
3. Results
3.1. Clinical Examination and Slit Skin Smear Microscopy
3.2. Sensitivity of the Modified Nested ITS 1 PCR
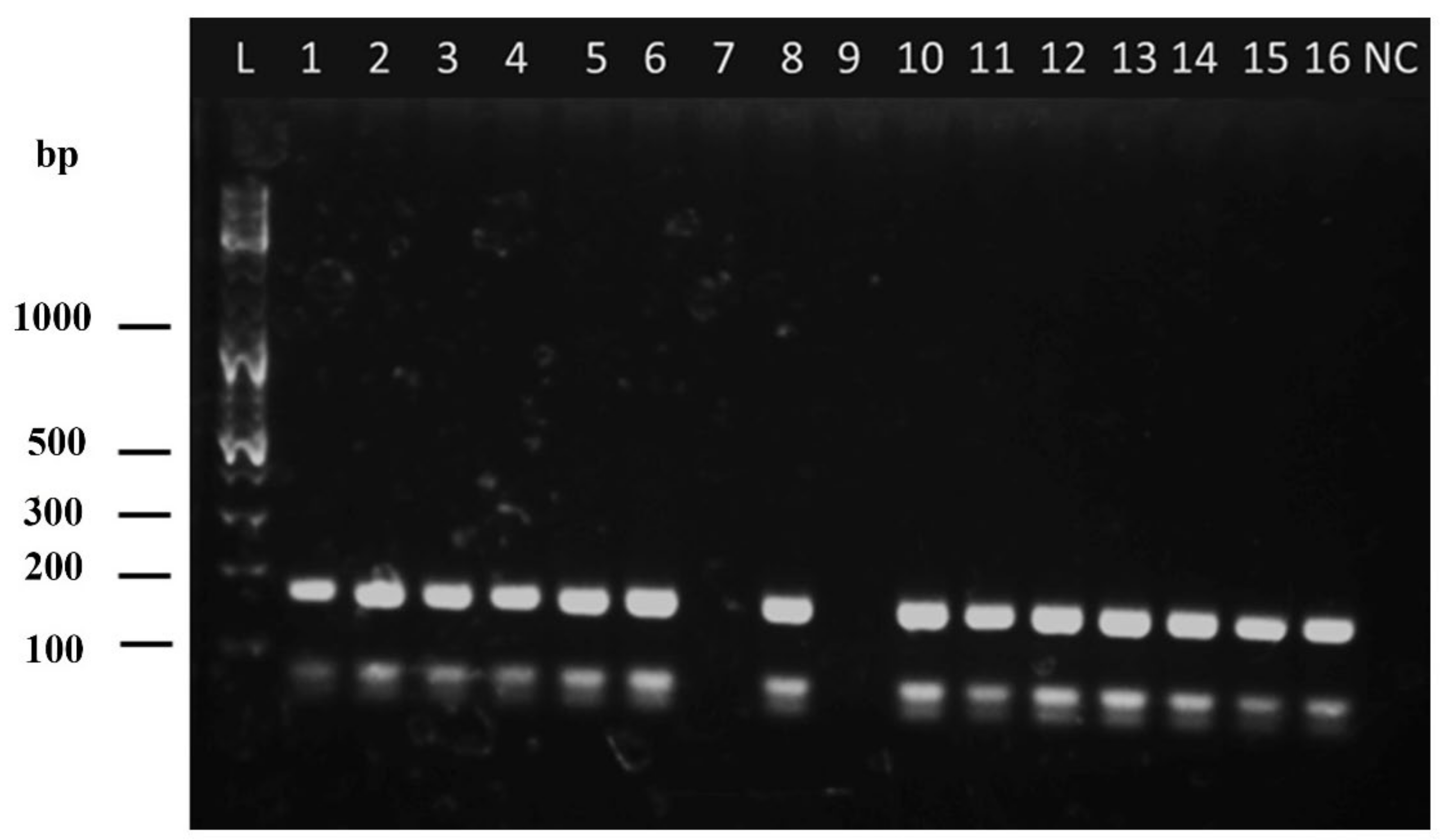
3.3. Analysis of the Cohort of Cutaneous Leishmaniasis Cases by the Nested ITS1 PCR-RFLP (n = 194)
3.4. Diagnostic Accuracy of SSS against Nested ITS1 PCR
3.5. Comparison of the Diagnostic Ability of Clinically Diagnosed Cases of CL in the Hospital Setting by Slit Skin Smear (SSS) and Modified Nested ITS1 PCR
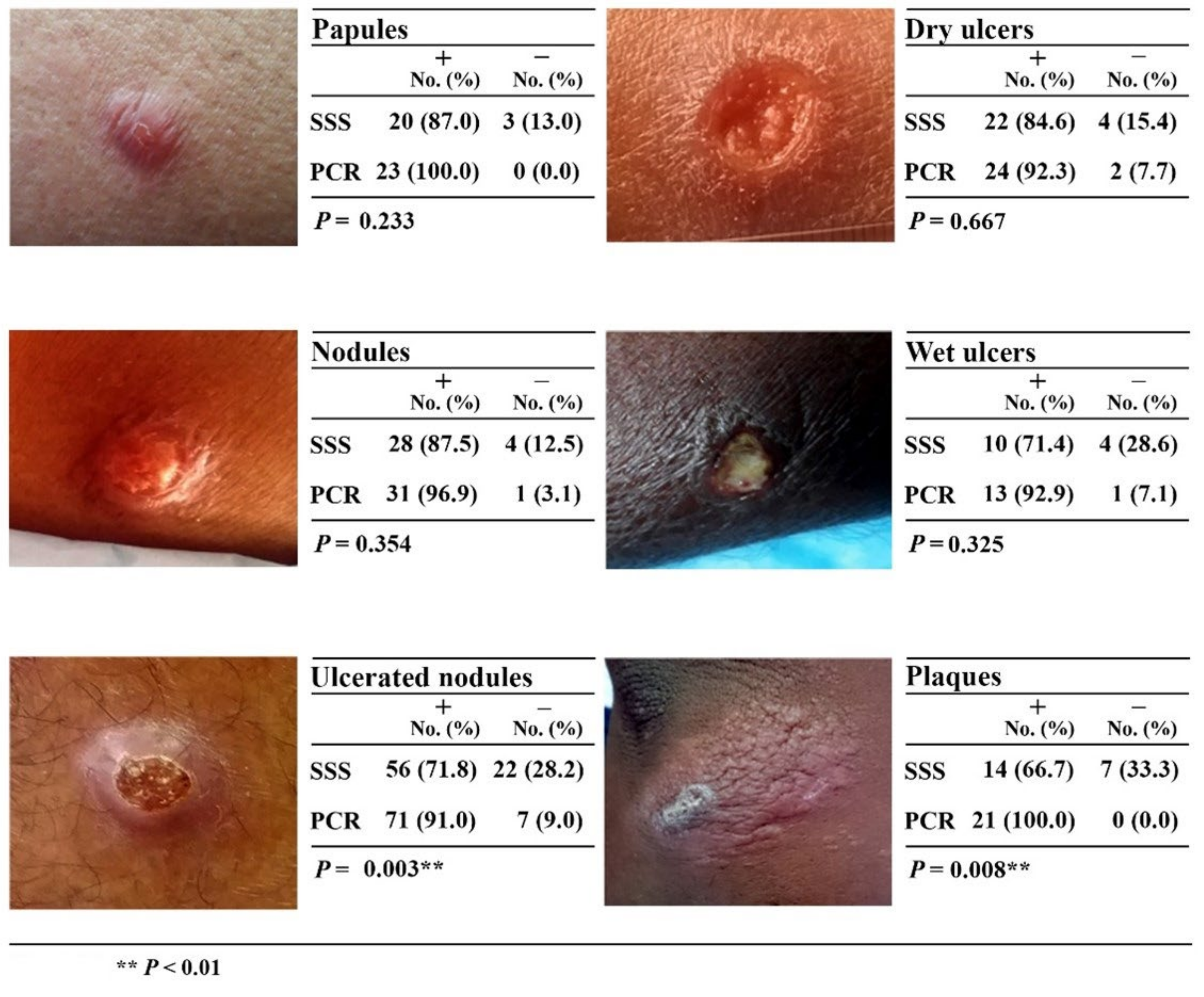
3.6. Comparison of the Diagnostic Ability of Different Types of CL Lesions by Slit Skin Smear (SSS) and Modified Nested ITS1 PCR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Leishmaniasis. Available online: https://www.who.int/news-room/fact-sheets/detail/leishmaniasis (accessed on 6 August 2020).
- Mcgwire, B.S.; Satoskar, A.J. Leishmaniasis: Clinical syndromes and treatment. QJM-Int. J. Med. 2014, 107, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Anon. General Circular no. 02/102/2008; Ministry of Health and Indigenous Medical Services: Colombo, Sri Lanka, 23 September 2008. [Google Scholar]
- Karunaweera, N.D.; Ginige, S.; Senanayake, S.; Silva, H.; Manamperi, N.; Samaranayake, N.; Siriwardana, Y.; Gamage, D.; Senerath, U.; Zhou, G. Spatial Epidemiologic Trends and Hotspots of Leishmaniasis, Sri Lanka, 2001–2018. Emerg. Infect. Dis. 2020, 26, 1. [Google Scholar] [CrossRef] [PubMed]
- Nawaratna, S.S.; Weilgama, D.J.; Rajapaksha, K. Cutaneous leishmaniasis in Sri Lanka: A study of possible animal reservoirs. Int. J. Infect. Dis. 2009, 13, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Rosypal, A.; Tripp, S.; Kinlaw, C.; Hailemariam, S.; Tidwell, R.; Lindsay, D.; Rajapakse, R.; Sreekumar, C.; Dubey, J. Surveillance for antibodies to Leishmania spp. in dogs from Sri Lanka. J. Parasitol. 2010, 96, 230–231. [Google Scholar] [CrossRef]
- Abayaweera, C.A.; Siriwardana, Y.; Abeywardana, T.; Rathnayaka, R.; Kumarasinghe, H.; Karunaweera, N.D. Dogs as a possible animal reservoir for leishmaniasis in Dickwella, Sri Lanka. In Proceedings of the Annual Research Procedings University of Colombo, Colombo, Sri Lanka, 12–13 May 2010. [Google Scholar]
- Iddawela, D.; Vithana, S.M.P.; Atapattu, D.; Wijekoon, L. Clinical and epidemiological characteristics of cutaneous leishmaniasis in Sri Lanka. BMC Infect. Dis. 2018, 18, 108. [Google Scholar] [CrossRef]
- Rajakaruna, R.S.; Jayathilake, P.; Wijerathna, H.; Fernando, A.; Ginarathne, K.; Naullage, N.; Silva, S.; Thananjayan, K.; Amarasiri, L.; Jayasundara, N. Canine Vector-Borne Diseases of Working Dogs of the Sri Lanka Air Force, Free-Roaming, and Privately-Owned Dogs. Res. Square 2021. [Google Scholar] [CrossRef]
- Siriwardana, H.; Chandrawansa, P.; Sirimanna, G.; Karunaweera, N. Leishmaniasis in Sri Lanka: A decade old story. Sri Lankan J. Infect. Dis. 2012, 2, 2–12. [Google Scholar] [CrossRef]
- Amarasinghe, A.; Wickramasinghe, S.J.A.P. A comprehensive review of cutaneous leishmaniasis in Sri Lanka and identification of existing knowledge gaps. Acta Parasitol. 2020, 65, 300–309. [Google Scholar] [CrossRef]
- Karunaweera, N.; Pratlong, F.; Siriwardane, H.; Ihalamulla, R.; Dedet, J. Sri Lankan cutaneous leishmaniasis is caused by Leishmania donovani zymodeme MON-37. Trans. R. Soc. Trop. Med. Hyg. 2003, 97, 380–381. [Google Scholar] [CrossRef]
- Lypaczewski, P.; Matlashewski, G.J.T.L.M. Leishmania donovani hybridisation and introgression in nature: A comparative genomic investigation. Lancet Microbe 2021, 2, e250–e258. [Google Scholar] [CrossRef]
- Rajapaksa, U.; Ihalamulla, R.; Karunaweera, N. First report of mucosal tissue localisation of leishmaniasis in Sri Lanka. Ceylon Med. J. 2005, 50, 90. [Google Scholar]
- Ranasinghe, S.; Zhang, W.-W.; Wickremasinghe, R.; Abeygunasekera, P.; Chandrasekharan, V.; Athauda, S.; Mendis, S.; Hulangamuwa, S.; Matlashewski, G.; Pratlong, F.J.P.; et al. Leishmania donovani zymodeme MON-37 isolated from an autochthonous visceral leishmaniasis patient in Sri Lanka. Pathog. Glob. Health 2012, 106, 421–424. [Google Scholar] [CrossRef]
- Siriwardana, Y.; Deepachandi, B.; Gunasekara, C.; Warnasooriya, W.; Karunaweera, N.D. Leishmania donovani Induced Cutaneous Leishmaniasis: An Insight into Atypical Clinical Variants in Sri Lanka. J. Trop. Med. 2019, 2019, 4538597. [Google Scholar] [CrossRef]
- Silva, H.; Liyanage, A.; Deerasinghe, T.; Chandrasekara, V.; Chellappan, K.; Karunaweera, N.D. Treatment failure to sodium stibogluconate in cutaneous leishmaniasis: A challenge to infection control and disease elimination. PLoS ONE 2021, 16, e0259009. [Google Scholar] [CrossRef]
- Giantsis, I.A.; Chaskopoulou, A.; Claude Bon, M.J. Direct multiplex PCR (dmPCR) for the identification of six phlebotomine sand fly species (Diptera: Psychodidae), including major Leishmania vectors of the Mediterranean. J. Econ. Entomol. 2017, 110, 245–249. [Google Scholar] [CrossRef]
- Ranasinghe, S.; Wickremasinghe, R.; Hulangamuwa, S.; Sirimanna, G.; Opathella, N.; Maingon, R.D.; Chandrasekharan, V. Polymerase chain reaction detection of LeishmaniaDNA in skin biopsy samples in Sri Lanka where the causative agent of cutaneous leishmaniasis is Leishmania donovani. Mem. Inst. Oswaldo Cruz 2015, 110, 1017–1023. [Google Scholar] [CrossRef]
- Deepachandi, B.; Weerasinghe, S.; Soysa, P.; Karunaweera, N.; Siriwardana, Y. A highly sensitive modified nested PCR to enhance case detection in leishmaniasis. BMC Infect. Dis. 2019, 19, 623. [Google Scholar] [CrossRef]
- Kothalawala, H.; Karunaweera, N. Loop-mediated isothermal amplification assay as a sensitive diagnostic tool for Leishmania donovani infections in Sri Lanka. Ceylon Med. J. 2016, 61, 68–70. [Google Scholar] [CrossRef]
- Cupolillo, E.; Grimaldi Jr., G.; Momen, H.; Beverley, S.M. Intergenic region typing (IRT): A rapid molecular approach to the characterization and evolution of Leishmania. Mol. Biochem. Parasitol. 1995, 73, 145–155. [Google Scholar] [CrossRef]
- Schönian, G.; Schnur, L.; El Fari, M.; Oskam, L.; Kolesnikov, A.A.; Sokolowska-Köhler, W.; Presber, W. Genetic heterogeneity in the species Leishmania tropica revealed by different PCR-based methods. Trans. R. Soc. Trop. Med. Hyg. 2001, 95, 217–224. [Google Scholar] [CrossRef]
- Koarashi, Y.; Cáceres, A.G.; Saca, F.M.Z.; Flores, E.E.P.; Trujillo, A.C.; Alvares, J.L.A.; Yoshimatsu, K.; Arikawa, J.; Katakura, K.; Hashiguchi, Y. Identification of causative Leishmania species in Giemsa-stained smears prepared from patients with cutaneous leishmaniasis in Peru using PCR-RFLP. Acta Trop. 2016, 158, 83–87. [Google Scholar] [CrossRef] [PubMed]
- El Tai, N.; Osman, O.; El Fari, M.; Presber, W.; Schönian, G. Genetic heterogeneity of ribosomal internal transcribed spacer in clinical samples of Leishmania donovani spotted on filter paper as revealed by single-strand conformation polymorphisms and sequencing. Trans. R. Soc. Trop. Med. Hyg. 2000, 94, 575–579. [Google Scholar] [CrossRef]
- Schönian, G.; Nasereddin, A.; Dinse, N.; Schweynoch, C.; Schallig, H.D.; Presber, W.; Jaffe, C.L. PCR diagnosis and characterization of Leishmania in local and imported clinical samples. Diagn. Microbiol. Infect. Dis. 2003, 47, 349–358. [Google Scholar] [CrossRef]
- Cruz, I.; Canavate, C.; Rubio, J.; Morales, M.; Chicharro, C.; Laguna, F.; Jimenez-Mejias, M.; Sirera, G.; Videla, S.; Alvar, J.; et al. A nested polymerase chain reaction (Ln-PCR) for diagnosing and monitoring Leishmania infantum infection in patients co-infected with human immunodeficiency virus. Trans. R. Soc. 2002, 96, S185–S189. [Google Scholar] [CrossRef]
- da Silva, M.A.L.; Soares, C.R.P.; Medeiros, R.A.; Medeiros, Z.; de Melo, F.L. Optimization of single-tube nested PCR for the diagnosis of visceral leishmaniasis. Exp. Parasitol. 2013, 134, 206–210. [Google Scholar] [CrossRef]
- Akhoundi, M.; Downing, T.; Votýpka, J.; Kuhls, K.; Lukeš, J.; Cannet, A.; Ravel, C.; Marty, P.; Delaunay, P.; Kasbari, M. Leishmania infections: Molecular targets and diagnosis. Mol. Asp. Med. 2017, 57, 1–29. [Google Scholar] [CrossRef]
- Franssen, S.U.; Durrant, C.; Stark, O.; Moser, B.; Downing, T.; Imamura, H.; Dujardin, J.-C.; Sanders, M.J.; Mauricio, I.; Miles, M.A.J.E. Global genome diversity of the Leishmania donovani complex. eLife 2020, 9, e51243. [Google Scholar] [CrossRef]
- Siriwardana, Y.; Deepachandi, B.; Weerasinghe, S.; Karunaweera, N.; Udagedara, C.; Warnasuriya, W.; Ranawaka, R.R.; Kahawita, I. First Evidence from Sri Lanka for Subphenotypic Diversity within L. donovani-Induced Classical Cutaneous Leishmaniasis. Biomed Res. Int. 2021, 2021, 3537968. [Google Scholar] [CrossRef]
- Kariyawasam, U.L.; Selvapandiyan, A.; Rai, K.; Wani, T.H.; Ahuja, K.; Beg, M.A.; Premathilake, H.U.; Bhattarai, N.R.; Siriwardena, Y.D.; Zhong, D. Genetic diversity of Leishmania donovani that causes cutaneous leishmaniasis in Sri Lanka: A cross sectional study with regional comparisons. BMC Infect. Dis. 2017, 17, 791. [Google Scholar] [CrossRef]
- Refai, F.W.; Madarasingha, N.P.; Fernandopulle, R.; Karunaweera, N. Nonresponsiveness to standard treatment in cutaneous leishmaniasis: A case series from Sri Lanka. Trop. Parasitol. 2016, 6, 155. [Google Scholar]
- Vergnes, B.; Gourbal, B.; Girard, I.; Sundar, S.; Drummelsmith, J.; Ouellette, M.J.M.; Proteomics, C. A proteomics screen implicates HSP83 and a small kinetoplastid calpain-related protein in drug resistance in Leishmania donovani clinical field isolates by modulating drug-induced programmed cell death. Mol. Cell. Proteom. 2007, 6, 88–101. [Google Scholar] [CrossRef]
- Kato, H.; Gomez, E.A.; Seki, C.; Furumoto, H.; Martini-Robles, L.; Muzzio, J.; Calvopiña, M.; Velez, L.; Kubo, M.; Tabbabi, A. PCR-RFLP analyses of Leishmania species causing cutaneous and mucocutaneous leishmaniasis revealed distribution of genetically complex strains with hybrid and mito-nuclear discordance in Ecuador. PLoS Negl. Trop. Dis. 2019, 13, e0007403. [Google Scholar] [CrossRef]
- Naotunne, T.; Rajakulendran, S.; Abeywickreme, W.; Kulasiri, C.; Perera, J.; Premaratne, U.; Attygalle, D.; Mendis, K. Cutaneous leishmaniasis in Sri Lanka. An imported disease linked to the Middle East and African employment boom. Trop. Geogr. Med. 1990, 42, 72–74. [Google Scholar]
- Fotakis, E.A.; Giantsis, I.A.; Avgerinou, A.; Kourtidis, S.; Agathaggelidou, E.; Kapoula, C.; Dadakou, G.; Vontas, J.; Chaskopoulou, A. Identification of Leishmania species in naturally infected sand flies from refugee camps, Greece. Emerg. Infect. Dis. 2019, 25, 361. [Google Scholar] [CrossRef]
- Hide, M.; Banuls, A.-L. Species-specific PCR assay for L. infantum/L. donovani discrimination. Acta Trop. 2006, 100, 241–245. [Google Scholar] [CrossRef]
- Ramírez, J.R.; Agudelo, S.; Muskus, C.; Alzate, J.F.; Berberich, C.; Barker, D.; Velez, I.D. Diagnosis of cutaneous leishmaniasis in Colombia: The sampling site within lesions influences the sensitivity of parasitologic diagnosis. J. Clin. Microbiol. 2000, 38, 3768–3773. [Google Scholar] [CrossRef]
- Sharquie, K.E.; Hassen, A.S.; Hassan, S.A.; Al-Hamami, I.A. Evaluation of diagnosis of cutaneous leishmaniasis by direct smear, culture and histopathology. Saudi Med. J. 2002, 23, 925–928. [Google Scholar]
- Kato, H.; Watanabe, J.; Nieto, I.M.; Korenaga, M.; Hashiguchi, Y. Leishmania species identification using FTA card sampling directly from patients’ cutaneous lesions in the state of Lara, Venezuela. Trans. R. Soc. Trop. Med. Hyg. 2011, 105, 561–567. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primer * | Sequence |
|---|---|
| Outer primers | |
| LITSR | 5′-CTGGATCATTTTCCGATG-3′ |
| L5.8S | 5′-TGATACCACTTATCGCACTT-3′ |
| Inner primers | |
| LITSR inner | 5′-CATTTTCCGATGATTACACC-3′ |
| L5.8S inner | 5′-TACTGCGTTCTTCAACGA-3′ |
| Leishmania Species and Strain | GenBank Accession Number | PCR Product Size (bp) | Restriction Fragment Sizes (bp) |
|---|---|---|---|
| L. major—5ASKH | KU680845 | 312 | 124, 188 |
| L. tropica—OD | EU326226 | 291 | 20, 48, 55, 168 |
| L. donovani—DD8 | MH202977 | 293 | 55, 69, 169 |
| Clinical Diagnosis | |||||
|---|---|---|---|---|---|
| Confirmed | Doubtful | ||||
| Positive (%) | Negative (%) | Positive (%) | Negative (%) | p | |
| Nested PCR | 166 (94.9) | 9 (5.1) | 17 (89.5) | 2 (10.5) | 0.605 |
| SSS | 139 (79.4) | 36 (20.6) | 11 (57.9) | 8 (42.1) | 0.044 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Silva, N.L.; De Silva, V.N.H.; Deerasinghe, A.T.H.; Rathnapala, U.L.; Itoh, M.; Takagi, H.; Weerasooriya, M.V.; Kato, H.; Yahathugoda, T.C. Development of a Highly Sensitive Nested PCR and Its Application for the Diagnosis of Cutaneous Leishmaniasis in Sri Lanka. Microorganisms 2022, 10, 990. https://doi.org/10.3390/microorganisms10050990
De Silva NL, De Silva VNH, Deerasinghe ATH, Rathnapala UL, Itoh M, Takagi H, Weerasooriya MV, Kato H, Yahathugoda TC. Development of a Highly Sensitive Nested PCR and Its Application for the Diagnosis of Cutaneous Leishmaniasis in Sri Lanka. Microorganisms. 2022; 10(5):990. https://doi.org/10.3390/microorganisms10050990
Chicago/Turabian StyleDe Silva, Nirmitha Lalindi, Viraji Nefertiti Hiromel De Silva, Arachchige Theja Hemapala Deerasinghe, Upeksha Lakmini Rathnapala, Makoto Itoh, Hidekazu Takagi, Mirani Vasanthamala Weerasooriya, Hirotomo Kato, and Thishan Channa Yahathugoda. 2022. "Development of a Highly Sensitive Nested PCR and Its Application for the Diagnosis of Cutaneous Leishmaniasis in Sri Lanka" Microorganisms 10, no. 5: 990. https://doi.org/10.3390/microorganisms10050990
APA StyleDe Silva, N. L., De Silva, V. N. H., Deerasinghe, A. T. H., Rathnapala, U. L., Itoh, M., Takagi, H., Weerasooriya, M. V., Kato, H., & Yahathugoda, T. C. (2022). Development of a Highly Sensitive Nested PCR and Its Application for the Diagnosis of Cutaneous Leishmaniasis in Sri Lanka. Microorganisms, 10(5), 990. https://doi.org/10.3390/microorganisms10050990