
23-Valent Pneumococcal Polysaccharide Vaccination Does Not Prevent Community-Acquired Pneumonia Hospitalizations Due to Vaccine-Type Streptococcus pneumoniae

 , ,
, ,
Abstract
1. Introduction
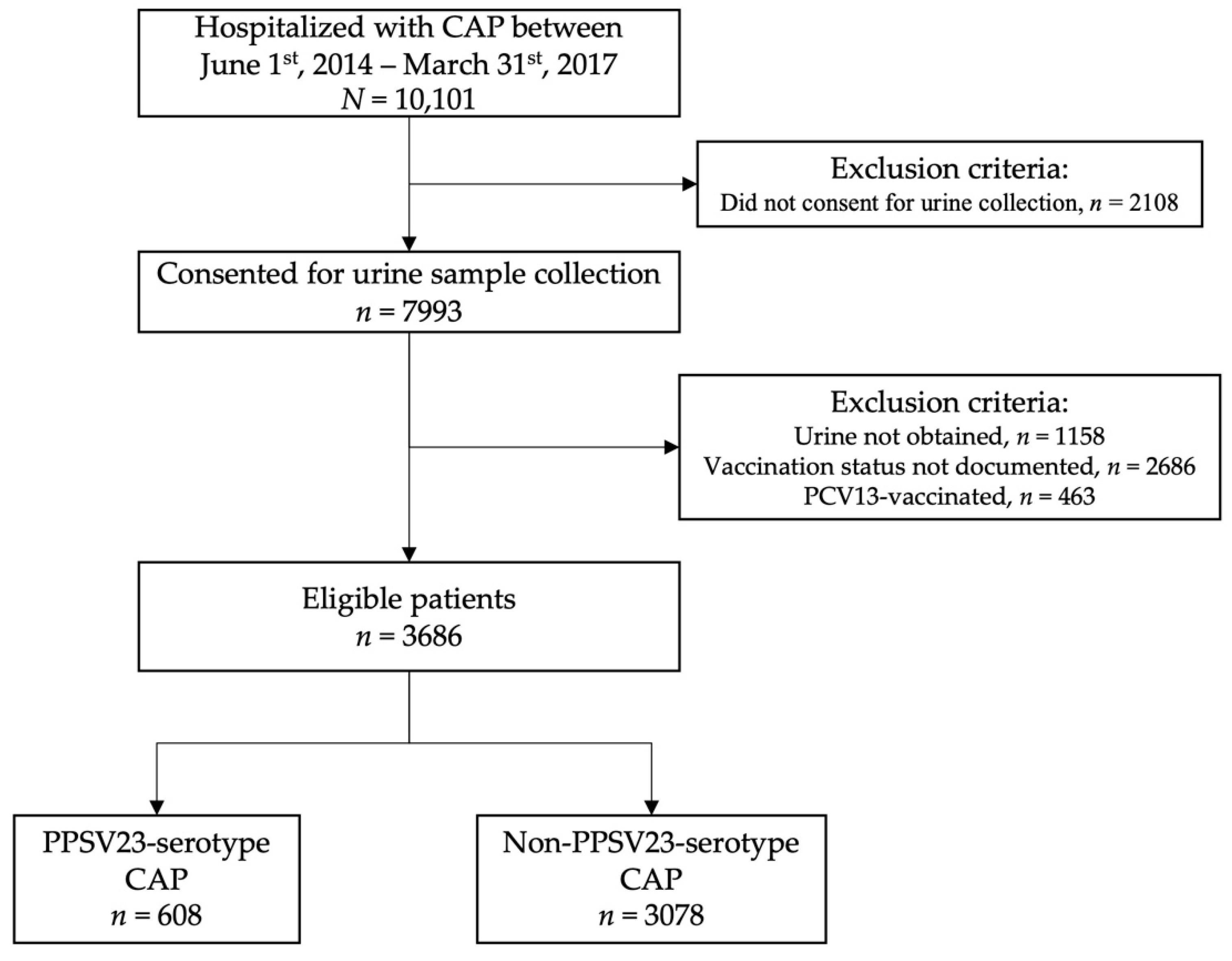
2. Materials and Methods
3. Results
3.1. Patient Characteristics by PPSV23-Vaccinated and Non-Vaccinated Patients
3.2. Patient Characteristics by PPSV23-Serotype CAP and Non-PPSV23-Serotype CAP Patients
3.3. Vaccine Effectiveness of PPSV23 in Overall Cohort
3.4. Subgroup Analyses: Vaccine Effectiveness of PPSV23
3.5. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shimbashi, R.; Suzuki, M.; Chang, B.; Watanabe, H.; Tanabe, Y.; Kuronuma, K.; Oshima, K.; Maruyama, T.; Takeda, H.; Kasahara, K.; et al. Effectiveness of 23-valent pneumococcal polysaccharide vaccine against invasive pneumococcal disease in adults, Japan, 2013–2017. Emerg. Infect. Dis. 2020, 26, 2378–2386. [Google Scholar] [CrossRef] [PubMed]
- Leventer-Roberts, M.; Feldman, B.S.; Brufman, I.; Cohen-Stavi, C.J.; Hoshen, M.; Balicer, R.D. Effectiveness of 23-valent pneumococcal polysaccharide vaccine against invasive disease and hospital-treated pneumonia among people aged ≥65 years: A retrospective case-control study. Clin. Infect. Dis. 2015, 60, 1472–1480. [Google Scholar] [CrossRef][Green Version]
- Suzuki, M.; Dhoubhadel, B.G.; Ishifuji, T.; Yasunami, M.; Yaegashi, M.; Asoh, N.; Ishida, M.; Hamaguchi, S.; Aoshima, M.; Ariyoshi, K.; et al. Serotype-specific effectiveness of 23-valent pneumococcal polysaccharide vaccine against pneumococcal pneumonia in adults aged 65 years or older: A multicentre, prospective, test-negative design study. Lancet Infect. Dis. 2017, 17, 313–321. [Google Scholar] [CrossRef]
- Masuda, T.; Nakatani, E.; Shirai, T.; Akamatsu, T.; Tamura, K.; Takahashi, S.; Tanaka, Y.; Watanabe, H.; Endo, Y.; Suzuki, T.; et al. Effectiveness of a 23-valent pneumococcal polysaccharide vaccine for the prevention of pneumococcal pneumonia in the elderly with chronic respiratory diseases: A case–control study of a single center. BMC Pulm. Med. 2021, 21, 123. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Chun, B.C.; Song, J.Y.; Kim, H.Y.; Bae, I.-G.; Kim, D.-M.; Choi, Y.H.; Jun, Y.H.; Choi, W.S.; Kang, S.H.; et al. Direct effectiveness of pneumococcal polysaccharide vaccine against invasive pneumococcal disease and non-bacteremic pneumococcal pneumonia in elderly population in the era of pneumococcal conjugate vaccine: A case-control study. Vaccine 2019, 37, 2797–2804. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. About Pneumococcal Vaccines. Vaccines and Preventable Diseases. 7 August 2020. Available online: https://www.cdc.gov/vaccines/vpd/pneumo/hcp/about-vaccine.html (accessed on 10 October 2021).
- Pride, M.W.; Huijts, S.M.; Wu, K.; Souza, V.; Passador, S.; Tinder, C.; Song, E.; Elfassy, A.; McNeil, L.; Menton, R.; et al. Validation of an immunodiagnostic assay for detection of 13 streptococcus pneumoniae serotype-specific polysaccharides in human urine. Clin. Vaccine Immunol. 2012, 19, 1131–1141. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, J.A.; Wiemken, T.L.; Peyrani, P.; Arnold, F.W.; Kelley, R.; Mattingly, W.A.; Nakamatsu, R.; Pena, S.; Guinn, B.E.; Furmanek, S.P.; et al. Adults hospitalized with pneumonia in the United States: Incidence, epidemiology, and mortality. Clin. Infect. Dis. 2017, 61, 1806–1812. [Google Scholar] [CrossRef]
- Kalina, W.V.; Souza, V.; Wu, K.; Giardina, P.; McKeen, A.; Jiang, Q.; Tan, C.; French, R.; Ren, Y.; Belanger, K.; et al. Qualification and clinical validation of an immunodiagnostic assay for detecting 11 additional streptococcus pneumoniae serotype–specific polysaccharides in human urine. Clin. Infect. Dis. 2020, 71, e430–e438. [Google Scholar] [CrossRef]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A prediction rule to identify low-risk patients with community-acquired pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef]
- Lim, W.S.; Van der Eerden, M.M.; Laing, R.; Boersma, W.G.; Karalus, N.; Town, G.I.; Lewis, S.A.; Macfarlane, J. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef]
- Lahariya, C. Vaccine epidemiology: A review. J. Fam. Med. Prim. Care 2016, 5, 7–15. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Pneumococcal Vaccination: Summary of Who and When to Vaccinate. Vaccines and Preventable Diseases. 7 August 2020. Available online: https://www.cdc.gov/vaccines/vpd/pneumo/hcp/who-when-to-vaccinate.html (accessed on 10 October 2021).
- Lawrence, H.; Pick, H.; Baskaran, V.; Daniel, P.; Rodrigo, C.; Ashton, D.; Edwards-Pritchard, R.C.; Sheppard, C.; Eletu, S.D.; Litt, D.; et al. Effectiveness of the 23-valent pneumococcal polysaccharide vaccine against vaccine serotype pneumococcal pneumonia in adults: A case-control test-negative design study. PLoS Med. 2020, 17, e1003326. [Google Scholar] [CrossRef]
- Heo, J.Y.; Seo, Y.B.; Choi, W.S.; Kim, E.J.; Jeong, H.W.; Lee, J.; Yoon, J.G.; Noh, J.Y.; Cheong, H.J.; Kim, W.J.; et al. Effectiveness of pneumococcal vaccination against pneumococcal pneumonia hospitalization in older adults: A prospective, test-negative study. J. Infect. Dis. 2022, 225, 836–845. [Google Scholar] [CrossRef]
- Domínguez, A.; Soldevila, N.; Toledo, D.; Torner, N.; Force, L.; Pérez, M.J.; Martí, M.C.; Rodríguez-Rojas, L.; Astray, J.; Egurrola, M.; et al. Effectiveness of 23-valent pneumococcal polysaccharide vaccination in preventing community-acquired pneumonia hospitalization and severe outcomes in the elderly in Spain. PLoS ONE 2017, 12, e0171943. [Google Scholar] [CrossRef] [PubMed]
- Van Heiden, S.; Carrico, R.; Wiemken, T.L.; Alexander, R.; McLaughlin, J.M.; Jiang, Q.; Peyrani, P.; Mattingly, W.A.; Furmanek, S.P.; English, C.L.; et al. Level of recall bias regarding pneumococcal vaccination history among adults hospitalized with community-acquired pneumonia: Results from the University of Louisville Pneumonia Study. J. Respir. Infect. 2017, 1, 3. [Google Scholar] [CrossRef]


{kind=link}
| Variable | PPSV23-Vaccinated (n = 608) | Non-Vaccinated (n = 3078) | p-Value |
|---|---|---|---|
| Age, median (IQR) | 68 (59, 76) | 65 (53, 77) | 0.001 |
| Male sex, n (%) | 301 (50) | 1461 (47) | 0.381 |
| Black or African American race, n (%) | 114 (19) | 622 (20) | 0.444 |
| Nursing home resident, n (%) | 59 (10) | 256 (8) | 0.299 |
| Current or former smoker, n (%) | 450 (74) | 2170 (71) | 0.090 |
| Obesity (BMI > 30), n (%) | 235 (39) | 1170 (38) | 0.815 |
| COPD, n (%) | 350 (58) | 1442 (47) | <0.001 |
| Diabetes, n (%) | 227 (37) | 969 (31) | 0.006 |
| Renal disease, n (%) | 198 (33) | 787 (26) | <0.001 |
| Heart failure, n (%) | 218 (36) | 852 (28) | <0.001 |
| Coronary artery disease, n (%) | 223 (37) | 867 (28) | <0.001 |
| Cerebrovascular disease, n (%) | 78 (13) | 373 (12) | 0.674 |
| Neoplastic disease (active or within past year), n (%) | 80 (13) | 405 (13) | >0.999 |
| Liver disease (non-cirrhotic), n (%) | 53 (9) | 212 (7) | 0.131 |
| Cirrhosis, n (%) | 9 (1) | 48 (2) | >0.999 |
| Essential arterial hypertension, n (%) | 469 (77) | 2047 (67) | <0.001 |
| Hyperlipidemia, n (%) | 324 (53) | 1250 (41) | <0.001 |
| Prior myocardial infarction, n (%) | 108 (18) | 377 (12) | <0.001 |
| Atrial fibrillation, n (%) | 135 (22) | 572 (19) | 0.044 |
| HIV, n (%) | 8 (1) | 52 (2) | 0.624 |
| Direct ICU admission, n (%) | 103 (17) | 511 (17) | 0.884 |
| PSI risk class IV–V, n (%) | 381 (63) | 1676 (54) | <0.001 |
| CURB-65 score 4 or 5, n (%) | 63 (10) | 288 (9) | 0.486 |
| Variable | PPSV23 Serotype CAP (n = 336) | Non-PPSV23 Serotype CAP (n = 3350) | p-Value |
|---|---|---|---|
| Age, median (IQR) | 62 (55, 72) | 66 (55, 77) | 0.006 |
| Male sex, n (%) | 156 (46) | 1606 (48) | 0.637 |
| Black or African American race, n (%) | 60 (18) | 676 (20) | 0.345 |
| Nursing home resident, n (%) | 23 (7) | 292 (9) | 0.286 |
| Current or former smoker, n (%) | 260 (77) | 2360 (70) | 0.009 |
| Obesity (BMI > 30), n (%) | 121 (36) | 1284 (38) | 0.431 |
| COPD, n (%) | 180 (54) | 1612 (48) | 0.064 |
| Diabetes, n (%) | 95 (28) | 1101 (33) | 0.098 |
| Renal disease, n (%) | 79 (24) | 906 (27) | 0.183 |
| Heart failure, n (%) | 80 (24) | 990 (30) | 0.032 |
| Coronary artery disease, n (%) | 74 (22) | 1016 (30) | 0.002 |
| Cerebrovascular disease, n (%) | 33 (10) | 418 (12) | 0.184 |
| Neoplastic disease (active or within past year), n (%) | 38 (11) | 447 (13) | 0.334 |
| Liver disease (non-cirrhotic), n (%) | 35 (10) | 230 (7) | 0.022 |
| Cirrhosis, n (%) | 9 (3) | 48 (1) | 0.125 |
| Essential arterial hypertension, n (%) | 219 (65) | 2297 (69) | 0.226 |
| Hyperlipidemia, n (%) | 125 (37) | 1449 (43) | 0.038 |
| Prior myocardial infarction, n (%) | 36 (11) | 449 (13) | 0.192 |
| Atrial fibrillation, n (%) | 47 (14) | 660 (20) | 0.014 |
| HIV, n (%) | 10 (3) | 50 (1) | 0.068 |
| Direct ICU admission, n (%) | 75 (22) | 539 (16) | 0.005 |
| PSI risk class IV–V, n (%) | 189 (56) | 1868 (56) | 0.909 |
| CURB-65 score 4 or 5, n (%) | 26 (8) | 325 (10) | 0.284 |
| Cases n (%) | Controls n (%) | Unadjusted VE % (95% CI) | Adjusted VE % (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Overall Cohort, n = 3866 | |||||
| Number | 336 | 3350 | 17% (−13 to 40%) | 14% (−17% to 39%) | 0.350 |
| PPSV23 vaccinated | 48 (8) | 560 (92) | |||
| Non-vaccinated | 288 (9) | 2790 (91) | |||
| Cases n (%) | Controls n (%) | Unadjusted VE % (95% CI) | Adjusted VE % (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Patients aged 65 and older, n = 1922 | |||||
| Number | 144 | 1778 | −1% (−54% to 36%) | 2% (−50% to 38%) | 0.938 |
| PPSV23 vaccinated | 27 (8) | 331 (92) | |||
| Non-vaccinated | 117 (7) | 1447 (93) | |||
| Admitted directly to the Ward, n = 3072 | |||||
| Number | 261 | 2811 | 12% (−25% to 39%) | 7% (−31% to 36%) | 0.685 |
| PPSV23 vaccinated | 39 (9) | 466 (92) | |||
| Non-vaccinated | 222 (9) | 2345 (91) | |||
| Admitted directly to the ICU, n = 614 | |||||
| Number | 75 | 539 | 35% (−28% to 71%) | 36% (−27% to 71%) | 0.232 |
| PPSV23 vaccinated | 9 (9) | 94 (91) | |||
| Non-vaccinated | 66 (13) | 445 (87) | |||
| PSI Risk Class I–III, n = 1629 | |||||
| Number | 147 | 1482 | 9% (−47% to 47%) | 8% (−50% to 46%) | 0.756 |
| PPSV23 vaccinated | 19 (8) | 208 (92) | |||
| Non-vaccinated | 128 (9) | 1274 (91) | |||
| PSI Risk Class IV–V, n = 2057 | |||||
| Number | 189 | 1868 | 22% (−16% to 49%) | 21% (−19% to 49%) | 0.276 |
| PPSV23 vaccinated | 29 (8) | 352 (92) | |||
| Non-vaccinated | 160 (10) | 1516 (90) | |||
| CURB-65 Score 0–3, n = 3335 | |||||
| Number | 310 | 3025 | 12% (−21% to 37%) | 9% (−26% to 35%) | 0.587 |
| PPSV23 vaccinated | 46 (8) | 499 (92) | |||
| Non-vaccinated | 264 (9) | 2526 (91) | |||
| CURB-65 Score 4–5, n = 351 | |||||
| Number | 26 | 325 | 64% (−26% to 94%) | 64% (−30% to 94%) | 0.182 |
| PPSV23 vaccinated | 2 (3) | 61 (97) | |||
| Non-vaccinated | 24 (8) | 264 (91) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandler, T.; Furmanek, S.; Carrico, R.; Balcom, D.; Arnold, F.; Ramirez, J. 23-Valent Pneumococcal Polysaccharide Vaccination Does Not Prevent Community-Acquired Pneumonia Hospitalizations Due to Vaccine-Type Streptococcus pneumoniae. Microorganisms 2022, 10, 560. https://doi.org/10.3390/microorganisms10030560
Chandler T, Furmanek S, Carrico R, Balcom D, Arnold F, Ramirez J. 23-Valent Pneumococcal Polysaccharide Vaccination Does Not Prevent Community-Acquired Pneumonia Hospitalizations Due to Vaccine-Type Streptococcus pneumoniae. Microorganisms. 2022; 10(3):560. https://doi.org/10.3390/microorganisms10030560
Chicago/Turabian StyleChandler, Thomas, Stephen Furmanek, Ruth Carrico, Dawn Balcom, Forest Arnold, and Julio Ramirez. 2022. "23-Valent Pneumococcal Polysaccharide Vaccination Does Not Prevent Community-Acquired Pneumonia Hospitalizations Due to Vaccine-Type Streptococcus pneumoniae" Microorganisms 10, no. 3: 560. https://doi.org/10.3390/microorganisms10030560
APA StyleChandler, T., Furmanek, S., Carrico, R., Balcom, D., Arnold, F., & Ramirez, J. (2022). 23-Valent Pneumococcal Polysaccharide Vaccination Does Not Prevent Community-Acquired Pneumonia Hospitalizations Due to Vaccine-Type Streptococcus pneumoniae. Microorganisms, 10(3), 560. https://doi.org/10.3390/microorganisms10030560