
Efficacy and Safety of Fecal Microbiota Transplantation in Treatment of Clostridioides difficile Infection among Pediatric Patients: A Systematic Review and Meta-Analysis

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
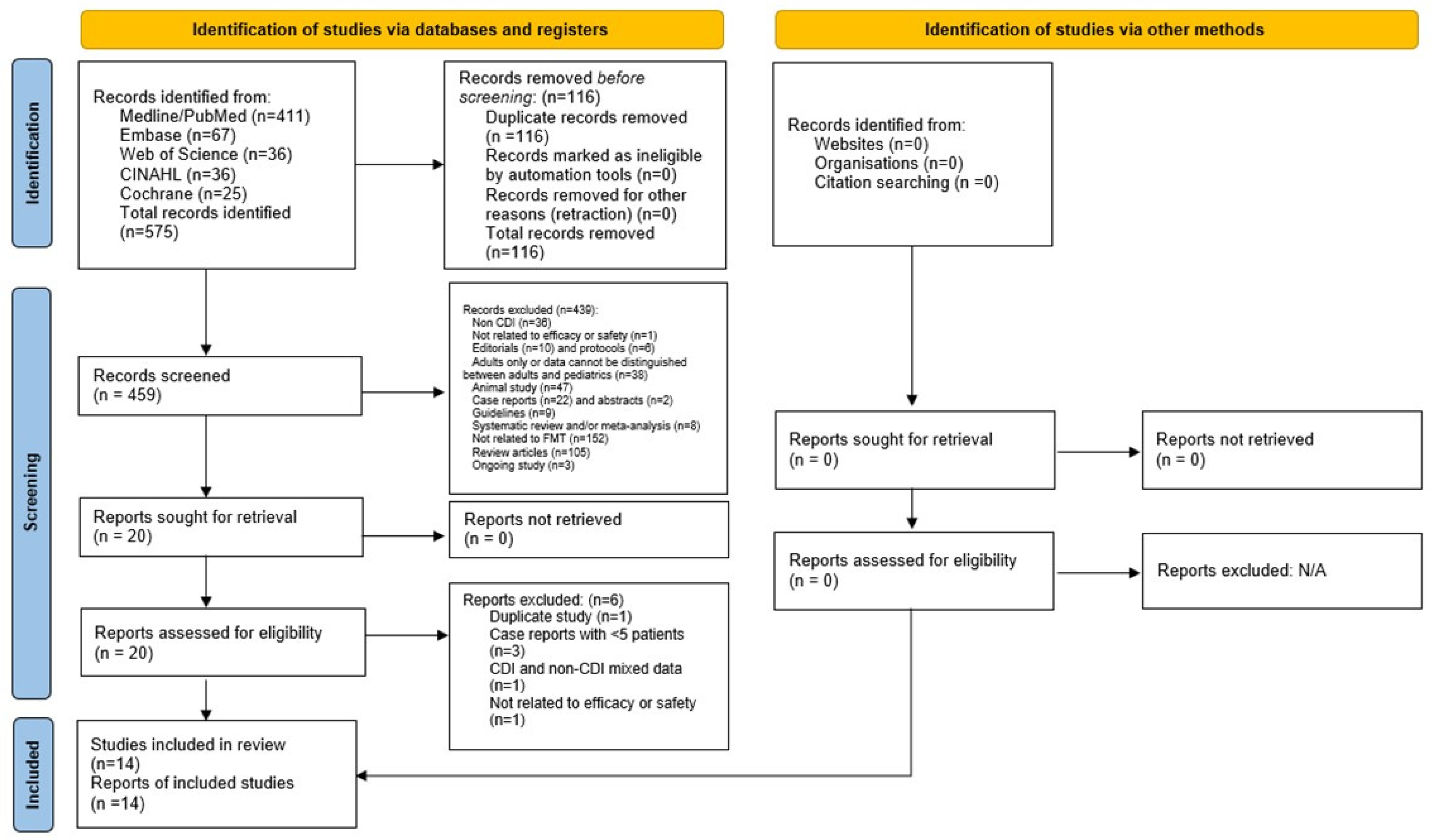
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Quality Assessment
2.4. Study Outcomes and Effect Size
2.5. Study Selection and Data Extraction
2.6. Data Analysis
3. Results
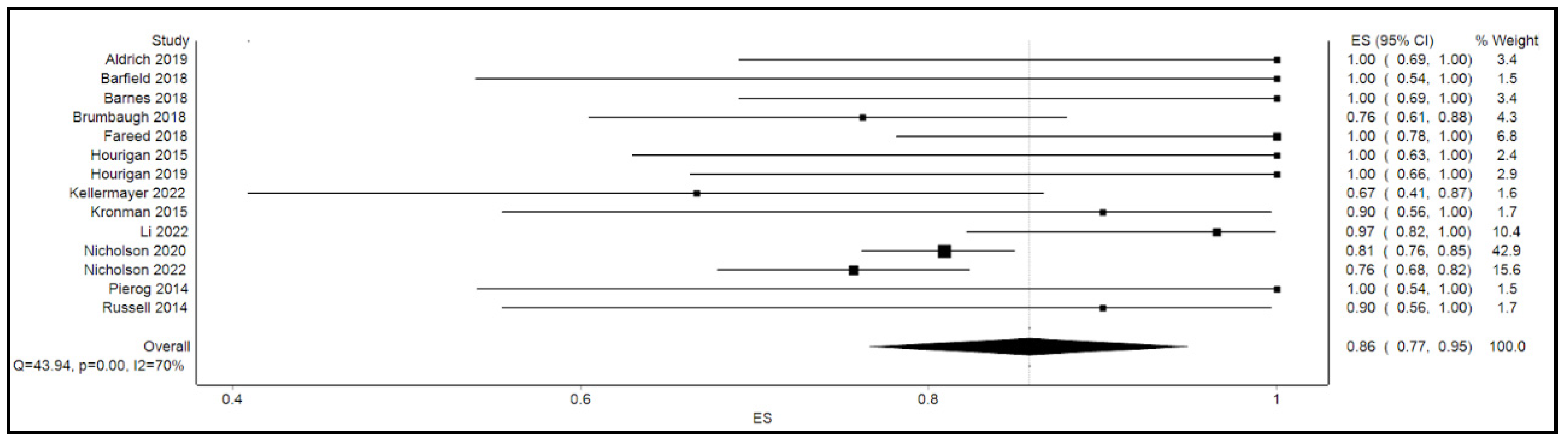
3.1. Primary Outcome
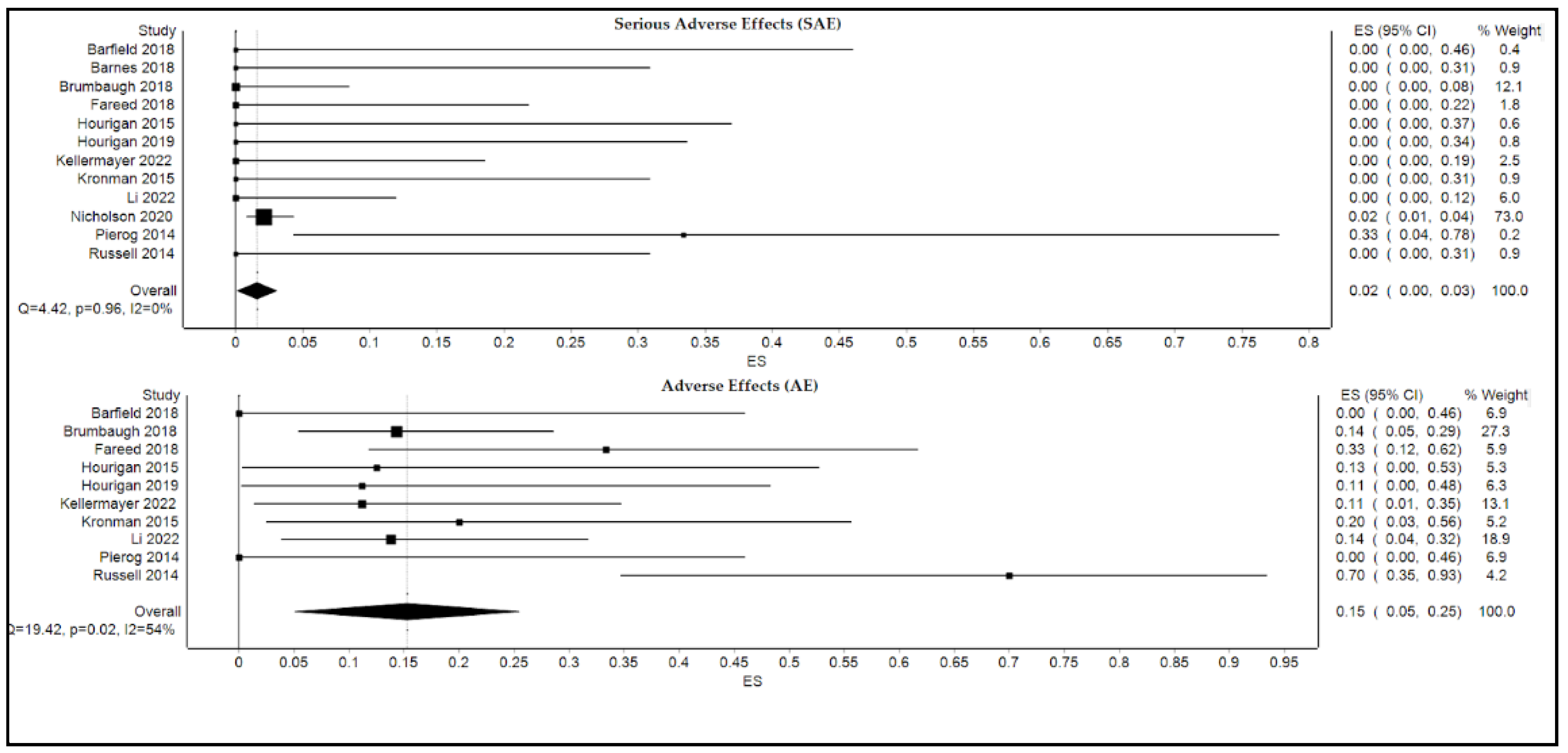
3.2. Secondary Outcome
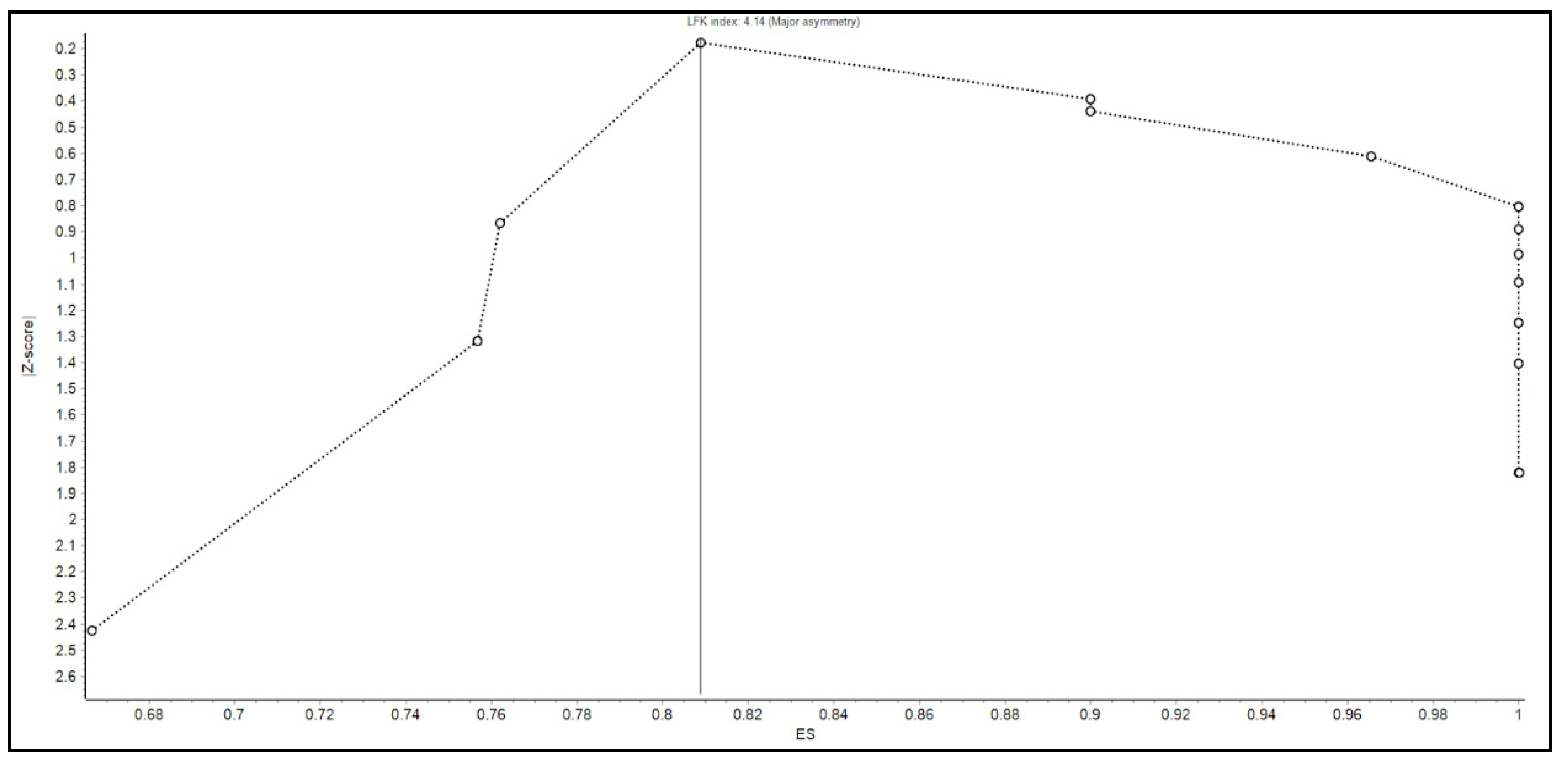
3.3. Validation Analysis (Leave-One-Out Analysis)
4. Discussion
Limitations
5. Conclusions and Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nicholson, M.R.; Alexander, E.; Ballal, S.; Davidovics, Z.; Docktor, M.; Dole, M.; Gisser, J.M.; Goyal, A.; Hourigan, S.K.; Jensen, M.K.; et al. Efficacy and Outcomes of Faecal Microbiota Transplantation for Recurrent Clostridioides difficile Infection in Children with Inflammatory Bowel Disease. J. Crohns Colitis 2022, 16, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xiao, F.; Li, Y.; Hu, H.; Xiao, Y.; Xu, Q.; Li, D.; Yu, G.; Wang, Y.; Zhang, T. Characteristics and management of children with Clostridioides difficile infection at a tertiary pediatric hospital in China. Braz. J. Infect. Dis. 2022, 26, 102380. [Google Scholar] [CrossRef] [PubMed]
- Kellermayer, R.; Wu, Q.; Nagy-Szakal, D.; Queliza, K.; Ihekweazu, F.D.; Bocchini, C.E.; Magee, A.R.; Oezguen, N.; Spinler, J.K.; Hollister, E.B.; et al. Fecal Microbiota Transplantation Commonly Failed in Children with Co-Morbidities. J. Pediatr. Gastroenterol. Nutr. 2022, 74, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Aldrich, A.M.; Argo, T.; Koehler, T.J.; Olivero, R. Analysis of Treatment Outcomes for Recurrent Clostridium difficile Infections and Fecal Microbiota Transplantation in a Pediatric Hospital. Pediatr. Infect. Dis. J. 2019, 38, 32–36. [Google Scholar] [CrossRef]
- Nicholson, M.R.; Mitchell, P.D.; Alexander, E.; Ballal, S.; Bartlett, M.; Becker, P.; Davidovics, Z.; Docktor, M.; Dole, M.; Felix, G.; et al. Efficacy of Fecal Microbiota Transplantation for Clostridium difficile Infection in Children. Clin. Gastroenterol. Hepatol. 2020, 18, 612–619.e1. [Google Scholar] [CrossRef]
- Nicholson, M.R.; Thomsen, I.P.; Slaughter, J.C.; Creech, C.B.; Edwards, K.M. Novel risk factors for recurrent Clostridium difficile infection in children. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 18–22. [Google Scholar] [CrossRef]
- Hourigan, S.K.; Ahn, M.; Gibson, K.M.; Pérez-Losada, M.; Felix, G.; Weidner, M.; Leibowitz, I.; E Niederhuber, J.; Sears, C.L.; Crandall, K.A.; et al. Fecal Transplant in Children with Clostridioides difficile Gives Sustained Reduction in Antimicrobial Resistance and Potential Pathogen Burden. Open Forum Infect. Dis. 2019, 6, ofz379. [Google Scholar] [CrossRef]
- Davidovics, Z.H.; Michail, S.; Nicholson, M.R.; Kociolek, L.; Pai, N.; Hansen, R.; Schwerd, T.; Maspons, A.; Shamir, R.; Szajewska, H.; et al. Fecal Microbiota Transplantation for Recurrent Clostridium difficile Infection and Other Conditions in Children: A Joint Position Paper from the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 130–143. [Google Scholar] [CrossRef]
- Barnes, D.; Ng, K.; Smits, S.; Sonnenburg, J.; Kassam, Z.; Park, K.T. Competitively Selected Donor Fecal Microbiota Transplantation: Butyrate Concentration and Diversity as Measures of Donor Quality. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 185–187. [Google Scholar] [CrossRef]
- Fareed, S.; Sarode, N.; Stewart, F.J.; Malik, A.; Laghaie, E.; Khizer, S.; Yan, F.; Pratte, Z.; Lewis, J.; Immergluck, L.C. Applying fecal microbiota transplantation (FMT) to treat recurrent Clostridium difficile infections (rCDI) in children. PeerJ 2018, 6, e4663. [Google Scholar] [CrossRef]
- Hardin, A.P.; Hackell, J.M.; Simon, G.R.; Boudreau, A.D.A.; Baker, C.N.; Barden, G.A. Committee on Practice And Ambulatory Medicine. Age limit of pediatrics. Pediatrics 2017, 140, e20172151. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.Y.; Popov, J.; Pai, N. Fecal microbial transplant for the treatment of pediatric inflammatory bowel disease. World J. Gastroenterol. 2016, 22, 10304–10315. [Google Scholar] [CrossRef] [PubMed]
- Abu-Zidan, F.M.; Abbas, A.K.; Hefny, A.F. Clinical “case series”: A concept analysis. Afr. Health Sci. 2012, 12, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel Members; Jensen, M.D.; Ryan, D.H.; Donato, K.A.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; et al. Executive summary: Guidelines (2013) for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society published by the Obesity Society and American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Based on a systematic review from the The Obesity Expert Panel, 2013. Obesity 2014, 22, S5–S39. [Google Scholar] [CrossRef]
- Mullish, B.H.; Quraishi, M.N.; Segal, J.P.; McCune, V.L.; Baxter, M.; Marsden, G.L.; Moore, D.J.; Colville, A.; Bhala, N.; Iqbal, T.H.; et al. The use of faecal microbiota transplant as treatment for recurrent or refractory Clostridium difficile infection and other potential indications: Joint British Society of Gastroenterology (BSG) and Healthcare Infection Society (HIS) guidelines. Gut 2018, 67, 1920–1941. [Google Scholar] [CrossRef]
- Doi, S.A.R.; Furuya-Kanamori, L. Selecting the best meta-analytic estimator for evidence-based practice: A simulation study. Int. J. Evid. Based Healthc. 2020, 18, 86–94. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Kanwal, F.; White, D. “Systematic Reviews and Meta-analyses” in Clinical Gastroenterology and Hepatology. Clin. Gastroenterol. Hepatol. 2012, 10, 1184–1186. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence—Inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef]
- Furuya-Kanamori, L.; Barendregt, J.J.; Doi, S.A.R. A new improved graphical and quantitative method for detecting bias in meta-analysis. Int. J. Evid. Based Healthc. 2018, 16, 195–203. [Google Scholar] [CrossRef]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Fagan, T. Exact 95% confidence intervals for differences in binomial proportions. Comput. Biol. Med. 1999, 29, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Lin, L. Use of Prediction Intervals in Network Meta-analysis. JAMA Netw. Open 2019, 2, e199735. [Google Scholar] [CrossRef] [PubMed]
- Barfield, E.; Small, L.; Navallo, L.; Solomon, A. Going to the Bank: Fecal Microbiota Transplantation in Pediatrics. Clin. Pediatr. 2018, 57, 481–483. [Google Scholar] [CrossRef] [PubMed]
- Brumbaugh, D.E.; De Zoeten, E.F.; Pyo-Twist, A.; Fidanza, S.; Hughes, S.; Dolan, S.A.; Child, J.; Dominguez, S.R. An Intragastric Fecal Microbiota Transplantation Program for Treatment of Recurrent Clostridium difficile in Children is Efficacious, Safe, and Inexpensive. J. Pediatr. 2018, 194, 123–127.e1. [Google Scholar] [CrossRef] [PubMed]
- Hourigan, S.K.; Chen, L.A.; Grigoryan, Z.; Laroche, G.; Weidner, M.; Sears, C.L.; Oliva-Hemker, M. Microbiome changes associated with sustained eradication of Clostridium difficile after single faecal microbiota transplantation in children with and without inflammatory bowel disease. Aliment. Pharmacol. Ther. 2015, 42, 741–752. [Google Scholar] [CrossRef]
- Pierog, A.; Mencin, A.; Reilly, N.R. Fecal microbiota transplantation in children with recurrent Clostridium difficile infection. Pediatr. Infect. Dis. J. 2014, 33, 1198–1200. [Google Scholar] [CrossRef]
- Kronman, M.P.; Nielson, H.J.; Adler, A.L.; Giefer, M.J.; Wahbeh, G.; Singh, N.; Zerr, D.M.; Suskind, D.L. Fecal microbiota transplantation via nasogastric tube for recurrent Clostridioides difficile infection in pediatric patients. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 23–26. [Google Scholar] [CrossRef]
- Russell, G.H.; Kaplan, J.L.; Youngster, I.; Baril-Dore, M.; Schindelar, L.; Hohmann, E.; Winter, H.S. Fecal transplant for recurrent Clostridium difficile infection in children with and without inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 588–592. [Google Scholar] [CrossRef]
- Iqbal, U.; Anwar, H.; Karim, M.A. Safety and efficacy of encapsulated fecal microbiota transplantation for recurrent Clostridium difficile infection: A systematic review. Eur. J. Gastroenterol. Hepatol. 2018, 30, 730–734. [Google Scholar] [CrossRef]
- Youngster, I.; Russell, G.H.; Pindar, C.; Ziv-Baran, T.; Sauk, J.; Hohmann, E.L. Oral, capsulized, frozen fecal microbiota transplantation for relapsing Clostridium difficile infection. JAMA 2014, 312, 1772–1778, Erratum in JAMA 2015, 313, 729. [Google Scholar] [CrossRef] [PubMed]
- Hecker, M.T.; Obrenovich, M.E.; Cadnum, J.L.; Jencson, A.L.; Jain, A.K.; Ho, E.; Donskey, C.J. Fecal Microbiota Transplantation by Freeze-Dried Oral Capsules for Recurrent Clostridium difficile Infection. Open Forum Infect. Dis. 2016, 3, ofw091. [Google Scholar] [CrossRef] [PubMed]
- Staley, C.; Hamilton, M.J.; Vaughn, B.P.; Graiziger, C.T.; Newman, K.M.; Kabage, A.J.; Sadowsky, M.J.; Khoruts, A. Successful Resolution of Recurrent Clostridium difficile Infection using Freeze-Dried, Encapsulated Fecal Microbiota; Pragmatic Cohort Study. Am. J. Gastroenterol. 2017, 112, 940–947. [Google Scholar] [CrossRef] [PubMed]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. 2018, 66, e1–e48. [Google Scholar] [CrossRef]
- Hourigan, S.K.; Nicholson, M.R.; Kahn, S.A.; Kellermayer, R. Updates and Challenges in Fecal Microbiota Transplantation for Clostridioides difficile Infection in Children. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 430–432. [Google Scholar] [CrossRef]
- Xiao, F.; Sun, J.; Xu, Y.; Li, F.; Huang, X.; Li, H.; Zhao, J.; Huang, J.; Zhao, J. Infectious SARS-CoV-2 in Feces of Patient with Severe COVID-19. Emerg. Infect. Dis. 2020, 26, 1920–1922. [Google Scholar] [CrossRef]
- Chen, C.C.; Chiu, C.H. Current and future applications of fecal microbiota transplantation for children. Biomed. J. 2022, 45, 11–18. [Google Scholar] [CrossRef]
- Nicholson, M.R.; Hourigan, S.K.; Conrad, M.; Goyal, A.; Jensen, K.; Kelsen, J.; Kennedy, M.; Weatherly, M.; Kahn, S.A. Current Challenges in Fecal Microbiota Transplantation for Clostridioides difficile Infection in Children. Am. J. Gastroenterol. 2021, 116, 1954–1956. [Google Scholar] [CrossRef]
- Kellermayer, R. Fecal microbiota transplantation: Great potential with many challenges. Transl. Gastroenterol. Hepatol. 2019, 4, 40. [Google Scholar] [CrossRef]
- Tariq, R.; Syed, T.; Yadav, D.; Prokop, L.J.; Singh, S.; Loftus, E.V., Jr.; Pardi, D.S.; Khanna, S. Outcomes of Fecal Microbiota Transplantation for, C. difficile Infection in Inflammatory Bowel Disease: A Systematic Review and Meta-analysis. J. Clin. Gastroenterol. 2021; Online ahead of print. [Google Scholar] [CrossRef]
- Cho, S.; Spencer, E.; Hirten, R.; Grinspan, A.; Dubinsky, M.C. Fecal Microbiota Transplant for Recurrent Clostridium difficile Infection in Pediatric Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 343–347. [Google Scholar] [CrossRef]
- Zhang, X.-Y.; Wang, Y.-Z.; Li, X.-L.; Hu, H.; Liu, H.-F.; Li, D.; Xiao, Y.-M.; Zhang, T. Safety of fecal microbiota transplantation in Chinese children: A single-center retrospective study. World J. Clin. Cases 2018, 6, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Gao, X.; Hu, H.; Xiao, Y.; Li, D.; Yu, G.; Yu, D.; Zhang, T.; Wang, Y. Clinical Efficacy and Microbiome Changes Following Fecal Microbiota Transplantation in Children with Recurrent Clostridium difficile Infection. Front. Microbiol. 2018, 9, 2622. [Google Scholar] [CrossRef] [PubMed]
- Drewes, J.L.; Corona, A.; Sanchez, U.; Fan, Y.; Hourigan, S.K.; Weidner, M.; Sidhu, S.D.; Simner, P.J.; Wang, H.; Timp, W.; et al. Transmission and clearance of potential procarcinogenic bacteria during fecal microbiota transplantation for recurrent Clostridioides difficile. JCI Insight 2019, 4, e130848. [Google Scholar] [CrossRef] [PubMed]
- Bluestone, H.; Kronman, M.P.; Suskind, D.L. Fecal Microbiota Transplantation for Recurrent Clostridium difficile Infections in Pediatric Hematopoietic Stem Cell Transplant Recipients. J Pediatr. Infect. Dis. Soc. 2018, 7, e6–e8. [Google Scholar] [CrossRef]
- Walia, R.; Garg, S.; Song, Y.; Girotra, M.; Cuffari, C.; Fricke, W.F.; Dutta, S.K. Efficacy of fecal microbiota transplantation in 2 children with recurrent Clostridium difficile infection and its impact on their growth and gut microbiome. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 565–570. [Google Scholar] [CrossRef]
- Ooijevaar, R.E.; van Rossen, T.M.; Vandenbroucke-Grauls, C.M.J.E.; Budding, A.E.; Kneepkens, C.M.F.; de Meij, T.G.J. Fecestransplantatie voor kinderen met recidiverende C. difficile-infecties [Faecal transplants for children with recurrent infections]. Ned. Tijdschr. Geneeskd. 2019, 163, D3739. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Study Design | Quality Assessment | Score | Data Collection Period | Follow-Up Period (Months) | Number of Patients Who Received FMT | Single or Multi-Center | Condition Treated with FMT | FMT Method |
|---|---|---|---|---|---|---|---|---|---|
| Nicholson 2022 [1] | Retrospective | NOS | 8 | 03/2012–03/2020 | 3 | 396 | Multi-center | rCDI | Sigmoidoscopy/Colonoscopy Upper Gastrointestinal Delivery * Capsule |
| Li 2022 [2] | Retrospective | NOS | 8 | 09/2014–09/2020 | 3 | 29 | Single | rCDI | Naso-intestinal tube Enema Capsule |
| Kellermayer 2022 [3] | Prospective | NOS | 7 | 02/2013–12/2015 | 2 | 18 | Single | rCDI | Colonoscopy Enema Nasogastric tube |
| Aldrich 2019 [4] | Retrospective | NOS | 9 | 01/2010–12/2014 | 2 | 10 | Single | rCDI | Colonoscopy EGD Nasojejunal Gastric |
| Nicholson 2020 [5] | Retrospective | NOS | 8 | 02/2004–02/2017 | 3 | 335 | Multi-center | Both CDI and rCDI | Colonoscopy Enteral routes ** |
| Hourigan 2019 [7] | Prospective | NOS | 7 | Not reported | 6 | 9 | Multi-center | rCDI | Colonoscopy |
| Barnes 2018 [9] | Prospective | NOS | 8 | 06/2014–06/2016 | 2.5 | 10 | Single | rCDI | Colonoscopy Upper Gastrointestinal Delivery & |
| Fareed 2018 [10] | Prospective | NOS | 8 | Not reported | 15 | 15 | Multi-center | rCDI | Colonoscopy Nasojejunal |
| Barfield 2018 [25] | Case series | NIH scale | 9 | 10/2013–11/2016 | 3 | 6 | Single | Both CDI and rCDI | Colonoscopy |
| Brumbaugh 2018 [26] | Retrospective | NOS | 7 | 03/2015–09/2016 | 3 | 42 | Single | rCDI | Nasogastric or gastrostomy tube |
| Hourigan 2015 [27] | Prospective | NOS | 7 | Not reported | 6 | 8 | Multi-center | rCDI | Colonoscopy |
| Pierog 2014 [28] | Case series | NIH scale | 7 | Not reported | 3 | 6 | Single | rCDI | Colonoscopy |
| Kronman 2015 [29] | Case series | NIH scale | 8 | 08/2011–05/2014 | 6 | 10 | Single | rCDI | Nasogastric, nasojejunal or nasoduodenal tuve |
| Russell 2014 [30] | Case series | NIH scale | 7 | 2009–2013 | 1 month to 48 months | 10 | Single | rCDI | Nasogastric tube Colonoscopy |
| Route of FMT Administration | Number of Times FMT Administered (n = 725) |
|---|---|
| Nasogastric tube | 85 (11.72%) |
| Naso-intestinal tube | 36 (4.97%) |
| Nasoduodenal | 1 (0.14%) |
| Nasojejunal tube | 6 (0.83%) |
| Gastric tube | 1 (0.14%) |
| Capsule | 31 (4.28%) |
| Enema | 20 (2.76%) |
| Both esophagogastroduodenoscopy and colonoscopy | 1 (0.14%) |
| Sigmoidoscopy | 2 (0.28%) |
| Colonoscopy | 361 (49.79%) |
| Unspecified route via upper gastrointestinal tract | 63 (8.69%) |
| Unspecified route via lower gastrointestinal tract | 105 (14.48%) |
| Unspecified upper or lower gastrointestinal tract | 13 (1.79%) |
| Comorbidities | Number of Patients |
|---|---|
| Inflammatory bowel disease (unspecified) | 178 |
| Ulcerative colitis | 83 |
| Crohn’s disease | 76 |
| Gastrointestinal diseases | 49 |
| Immunodeficient and/or transplant status | 153 |
| Malignancy | 17 |
| Neuromuscular disorders or impairment | 8 |
| Autism spectrum disorder | 2 |
| Genetic disorders | 3 |
| Author/Year | Number of Patients Who Received FMT | Number of Patients with FMT Success (Percentage) | Number of Patients with FMT Failure (Percentage) |
|---|---|---|---|
| Nicholson, 2022 [1] | 396 | 315 (79.55%) | 81 (20.46%) |
| Li, 2022 [2] | 29 | 28 (96.55%) | 1 (3.45%) |
| Kellermayer, 2022 [3] | 18 | 12 (66.67%) | 6 (33.33%) |
| Aldrich, 2019 [4] | 10 | 10 (100%) | 0 (0.00%) |
| Nicholson, 2020 [5] | 335 | 271 (80.90%) | 64 (19.10%) |
| Hourigan, 2019 [7] | 9 | 9 (100%) | 0 (0.00%) |
| Barnes, 2018 [9] | 10 | 10 (100%) | 0 (0.00%) |
| Fareed, 2018 [10] | 15 | 15 (100%) | 0 (0.00%) |
| Barfield, 2018 [25] | 6 | 6 (100%) | 0 (0.00%) |
| Brumbaugh, 2018 [26] | 42 | 32 (76.19%) | 10 (23.81%) |
| Hourigan, 2015 [27] | 8 | 8 (100%) | 0 (0.00%) |
| Pierog, 2014 [28] | 6 | 6 (100%) | 0 (0.00%) |
| Kronman, 2015 [29] | 10 | 9 (90%) | 1 (10.00%) |
| Russell, 2014 [30] | 10 | 9 (90%) | 1 (10.00%) |
| Total | 904 | 740 (81.86%) | 164 (18.14%) |
| Author/Year | Number of Male Patients with FMT Success | Number of Female Patients with FMT Success | Number of Male Patients with FMT Failure | Number of Female Patients with FMT Failure |
|---|---|---|---|---|
| Nicholson, 2022 [1] ** | 63 | 49 | 21 | 15 |
| Li, 2022 [2] | NR | NR | NR | NR |
| Kellermayer, 2022 [3] | 6 | 6 | 4 | 2 |
| Aldrich, 2019 [4] | NR | NR | 0 * | 0 * |
| Nicholson, 2020 [5] | 136 | 135 | 36 | 28 |
| Hourigan, 2019 [7] | NR | NR | 0 * | 0 * |
| Barnes, 2018 [9] | 7 | 3 | 0 | 0 |
| Fareed, 2018 [10] | 6 | 9 | 0 | 0 |
| Barfield, 2018 [25] | 3 | 3 | 0 | 0 |
| Brumbaugh, 2018 [26] | NR | NR | NR | NR |
| Hourigan, 2015 [27] | NR | NR | 0 * | 0 * |
| Pierog, 2014 [28] | 4 | 2 | 0 | 0 |
| Kronman, 2015 [29] | 3 | 6 | 0 | 1 |
| Russell, 2014 [30] | 5 | 4 | 1 | 0 |
| Total | 233 (78.98%; 233/295) | 217 (82.51%; 217/263) | 62 (21.02%; 62/295) | 46 (17.49%; 46/263) |
| Author/Year | Total Number of IBD Patients Who Received FMT | Number of IBD Patients with FMT Success | Number of IBD Patients with FMT Failure |
|---|---|---|---|
| Nicholson, 2022 [1] | 148 | 112 | 36 |
| Li, 2022 [2] | 16 | NR | NR |
| Kellermayer, 2022 [3] | 5 | 1 | 4 |
| Aldrich, 2019 [4] | 25 | NR | NR |
| Nicholson, 2020 [5] | 120 ** | 85 | 26 |
| Hourigan, 2019 [7] | 0 | N/A | N/A |
| Barnes, 2018 [9] | 0 | N/A | N/A |
| Fareed, 2018 [10] | 5 | 5 | 0 |
| Barfield, 2018 [25] | 2 | 2 | 0 |
| Brumbaugh, 2018 [26] | 13 | 7 | 6 |
| Hourigan, 2015 [27] | 5 | 5 | 0 |
| Pierog, 2014 [28] | 1 | 1 | 0 |
| Kronman, 2015 [29] | 3 | 3 | 0 |
| Russell, 2014 [30] | 3 | 2 | 1 |
| Total | 346 | 223 (75.33%; 223/296) * | 73 (24.66%; 73/296) * |
| Author/Year | Number of SAEs Related to FMT | Description of SAE | Number of Patients with SAE | Number of AE Related to FMT | Description of AE | Number of Patients with AE |
|---|---|---|---|---|---|---|
| Nicholson, 2022 [1] | 29 | 19 IBD-related hospitalization; 1 pancreatitis-related hospitalization; 9 IBD-related surgeries | 27 | NR | NR | NR |
| Li 2022 [2] | 0 | N/A | 0 | 4 | 1 fever; 1 transient diarrhea, 1 transient abdominal pain; 1 vomit | 4 |
| Kellermayer, 2022 [3] | 0 | N/A | 0 | 2 | 1 paradoxical diarrhea 1 intermittent diarrhea and abdominal pain | 2 |
| Aldrich, 2019 [4] | NR | NR | NR | NR | NR | NR |
| Nicholson, 2020 [5] | 7 | 1 aspiration pneumonia; 3 IBD flare; 2 colectomy; 1 vomiting and dehydration | 7 | 19 * | Diarrhea Abdominal pain Vomiting | 19 |
| Hourigan, 2019 [7] | 0 | N/A | 0 | 1 | Chronic diarrhea and fecal urgency of non-infectious etiology | 1 |
| Barnes, 2018 [9] | 0 | N/A | 0 | NR | NR | NR |
| Fareed, 2018 [10] | 0 | N/A | 0 | 5 | 5 abdominal pain | 5 |
| Barfield, 2018 [25] | 0 | N/A | 0 | 0 | N/A | 0 |
| Brumbaugh, 2018 [26] | 0 | N/A | 0 | 6 | 6 vomiting | 6 |
| Hourigan, 2015 [27] | 0 | N/A | 0 | 1 | Diarrhea of non-infectious etiology | 1 |
| Pierog, 2014 [28] | 2 | 1 appendicitis 1 infection unrelated to gastrointestinal tract | 2 | 0 | N/A | 0 |
| Kronman, 2015 [29] | 0 | N/A | 0 | 2 | 1 vomiting 1 mucoid stools | 1 |
| Russell, 2014 [30] | 0 | N/A | 0 | 7 | 1 mucoid stools; 3 abdominal pain and diarrhea; 1 diarrhea with abdominal pain; 2 bloody stools with bloating and abdominal pain | 6 |
| Total | 38 | N/A | 36 | 47 | N/A | 45 |
| Studies | Pooled ES | LCI 95% | UCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 UCI 95% |
|---|---|---|---|---|---|---|---|---|
| Nicholson, 2022 [1] | 0.876 | 0.777 | 0.976 | 34.999 | 0.000 | 65.713 | 38.297 | 80.947 |
| Li, 2022 [2] | 0.845 | 0.747 | 0.943 | 37.581 | 0.000 | 68.069 | 43.107 | 82.079 |
| Kellermayer, 2022 [3] | 0.861 | 0.769 | 0.952 | 41.218 | 0.000 | 70.887 | 48.797 | 83.447 |
| Aldrich, 2019 [4] | 0.853 | 0.760 | 0.946 | 40.570 | 0.000 | 70.422 | 47.863 | 83.220 |
| Nicholson, 2020 [5] | 0.894 | 0.811 | 0.978 | 35.512 | 0.000 | 66.208 | 39.312 | 81.184 |
| Hourigan, 2019 [7] | 0.853 | 0.760 | 0.947 | 41.123 | 0.000 | 70.820 | 48.662 | 83.414 |
| Barnes, 2018 [9] | 0.853 | 0.760 | 0.946 | 40.570 | 0.000 | 70.422 | 47.863 | 83.220 |
| Fareed, 2018 [10] | 0.847 | 0.755 | 0.939 | 36.915 | 0.000 | 67.493 | 41.935 | 81.801 |
| Barfield, 2018 [25] | 0.855 | 0.763 | 0.948 | 42.451 | 0.000 | 71.732 | 50.490 | 83.860 |
| Brumbaugh, 2018 [26] | 0.862 | 0.766 | 0.958 | 41.983 | 0.000 | 71.417 | 49.860 | 83.706 |
| Hourigan, 2015 [27] | 0.854 | 0.761 | 0.947 | 41.616 | 0.000 | 71.165 | 49.355 | 83.583 |
| Pierog, 2014 [28] | 0.855 | 0.763 | 0.948 | 42.444 | 0.000 | 71.728 | 50.481 | 83.858 |
| Kronman, 2015 [29] | 0.857 | 0.762 | 0.952 | 43.802 | 0.000 | 72.604 | 52.227 | 84.289 |
| Russell, 2014 [30] | 0.857 | 0.762 | 0.952 | 43.802 | 0.000 | 72.604 | 52.227 | 84.289 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tun, K.M.; Hsu, M.; Batra, K.; Lo, C.-H.; Laeeq, T.; Vongsavath, T.; Mohammed, S.; Hong, A.S. Efficacy and Safety of Fecal Microbiota Transplantation in Treatment of Clostridioides difficile Infection among Pediatric Patients: A Systematic Review and Meta-Analysis. Microorganisms 2022, 10, 2450. https://doi.org/10.3390/microorganisms10122450
Tun KM, Hsu M, Batra K, Lo C-H, Laeeq T, Vongsavath T, Mohammed S, Hong AS. Efficacy and Safety of Fecal Microbiota Transplantation in Treatment of Clostridioides difficile Infection among Pediatric Patients: A Systematic Review and Meta-Analysis. Microorganisms. 2022; 10(12):2450. https://doi.org/10.3390/microorganisms10122450
Chicago/Turabian StyleTun, Kyaw Min, Mark Hsu, Kavita Batra, Chun-Han Lo, Tooba Laeeq, Tahne Vongsavath, Salman Mohammed, and Annie S. Hong. 2022. "Efficacy and Safety of Fecal Microbiota Transplantation in Treatment of Clostridioides difficile Infection among Pediatric Patients: A Systematic Review and Meta-Analysis" Microorganisms 10, no. 12: 2450. https://doi.org/10.3390/microorganisms10122450
APA StyleTun, K. M., Hsu, M., Batra, K., Lo, C.-H., Laeeq, T., Vongsavath, T., Mohammed, S., & Hong, A. S. (2022). Efficacy and Safety of Fecal Microbiota Transplantation in Treatment of Clostridioides difficile Infection among Pediatric Patients: A Systematic Review and Meta-Analysis. Microorganisms, 10(12), 2450. https://doi.org/10.3390/microorganisms10122450