
Development of a Control System and Functional Validation of a Parallel Robot for Lower Limb Rehabilitation

 ,
, 
 ,
,
Abstract
:1. Introduction
- (a)
- Stationary systems are designed to perform rehabilitation training of the human ankle and knee without the patient walking; the patients are always positioned in the same location, and only the subject limb performs training actions. The Rutgers robotic system [24] is based on Stewart platform that provide 6 DOF at the patient’s foot accompanied by virtual reality exercises. Another example is the High Performance Ankle Rehabilitation Robot designed and developed by IIT (Instituto Italiano di Tecnologia). This device performs plantar dorsiflexion and inversion/eversion using a better parallel mechanism as it takes advantage of actuation redundancy to minimize singularity and substantially improve dexterity in the workspace.
- (b)
- Active foot orthoses are wearable exoskeletons that patients wear while walking outside or on a treadmill. In the market, one currently available active foot orthoses is Anklebot, commercialized by Interactive Motion Technologies [25] and developed by MIT. This is a rehabilitation system that provides 3 DOF of the foot with respect of the shank when the patient is walking on the floor or treadmill.
2. Materials and Methods
2.1. RECOVER-Parallel Robot for Lower Limb Rehabilitation
2.1.1. Mechanical Design
- 2 active prismatic joints ( and );
- 5 passive revolute joints (, , , , and ).
- and are active prismatic joints;
- and are passive revolute joints;
- and are passive prismatic joints.
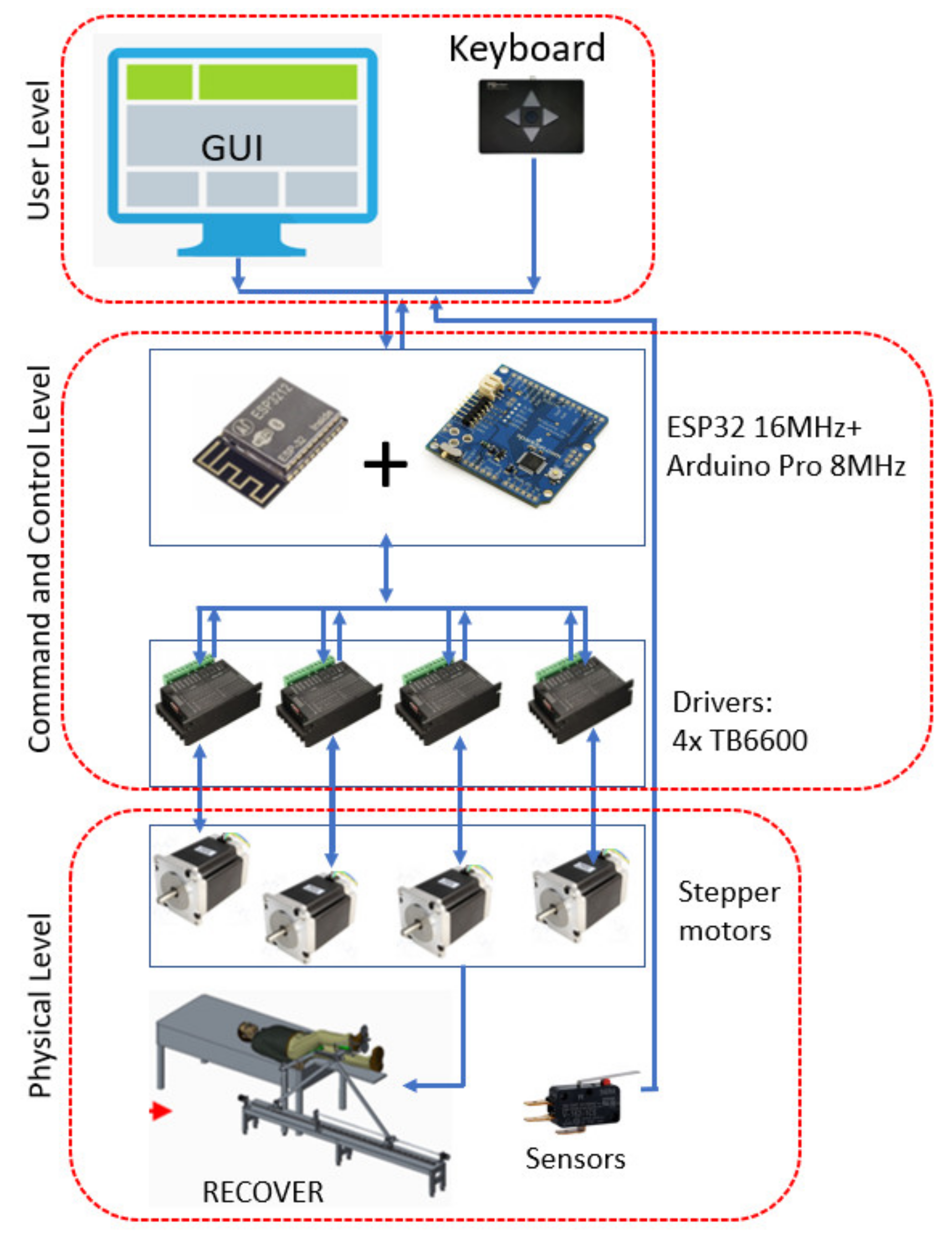
2.1.2. Robot Control System
- The number of steps (step) executed by the selected motor, if this parameter is chosen 0 then the motor will rotate until the control button (forward or backward) is active (pressed), or for a positive value it will execute the specified number of steps;
- Actuation speed given in (steps/sec), usually in the range 100–1200, the velocity sign in the expression determines the direction of rotation;
- Motor selection: 1 selecting , 2 selecting , 3 selecting both motors that will rotate in the same direction, and 4 when both motors rotate but in opposite directions.
- The ratio of driving speeds ranges from 1 to 7, with 1 indicating that the motor spins 3 times faster than , 2 indicating 2 times, 3 indicating 1.5 times (3/2), 4 indicating equal speeds, and 5, 6, and 7 indicating 2/3, 1/2, and 1/3 ratios, respectively.
2.2. Experimental Validation of the RECOVER Control System
- The subject must lay on the bed’s edge, with the pelvis located at the end of the bed, so that limb movement is possible beyond the upper side of the bed.
- Human hip rotational axes and robot hip joint rotational axes must be collinear.
- The length of the robot’s femoral link must be calibrated to correspond to the anthropometric length of the thigh, so that the rotational knee joint axes of the human lower limb and the axes of knee and robotic knee joint are collinear.
- The lower limb that will not be subjected to rehabilitation training will be held by a support installed in the bed’s expansion, ensuring that it remains completely horizontal.
- The lower limb undergoing medical recovery therapy will be put on thigh support, which will be tied on with braces, and the lower leg will be placed on lower leg support, which will also be tied on with straps.
- Once the thigh and lower leg are secured to their respective supports, the foot is positioned within the ankle module, which is secured to the lower limb support. The adjustment length of connection requires the sole to be secured to the sole support, and the foot is attached to the sole support with Velcro straps.
- The rehabilitation process is started based on the advice of the physiotherapist.
- The robot performs the rehabilitation motions with the patient attached.
- When the rehabilitation process is completed, the robot returns to the start position, the lower limb will be disconnected from the sole support, lower leg support and thigh straps and the subject may end the rehabilitation process.
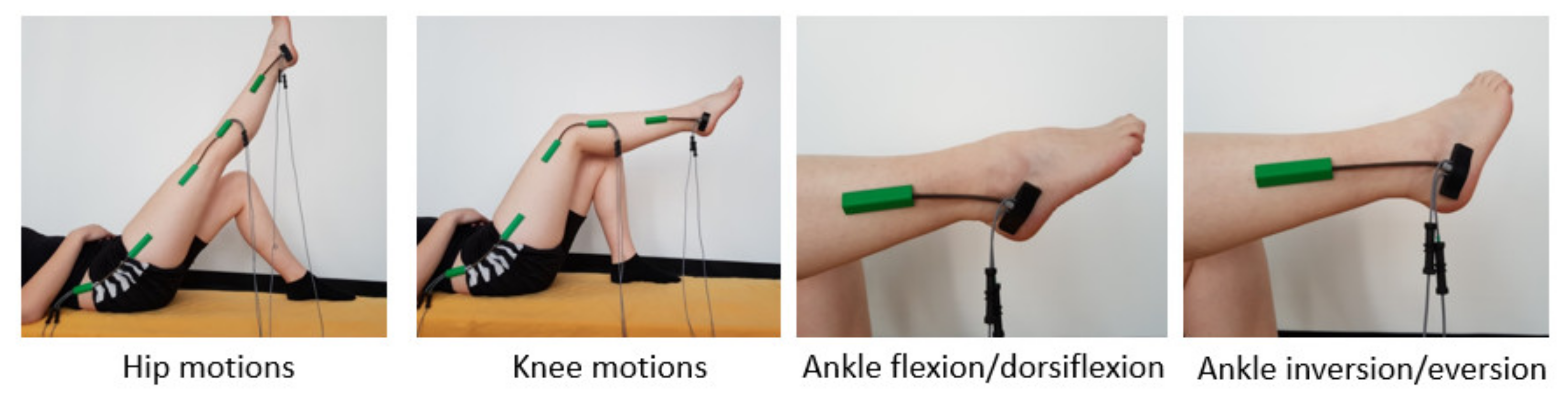
- Hip flexion/extension.
- Knee flexion/extension.
- Ankle dorsiflexion/plantar flexion.
- Ankle inversion/eversion.
- Participant is laying down on the adjustable bed, the robotic system is placed on the right side of bed; thus, the subject of test will place his right leg on the robotic device (Figure 5).
- Each subject is asked to place themselves comfortably and in a correct position on the robotic device after sterilizing the robot elements that come into direct contact with the test participant’s body;
- The subject’s foot is placed on the ankle module support composed from a lower leg support, sole support, and heel support, once the foot is positioned in the ankle module, it is secured with Velcro straps;
- Ten repetitions are performed for each rehabilitation training motion;
- First rehabilitation motion tested is hip flexion/extension; the leg is raised in sagittal plane;
- Before executing the next motion, the robot is returned to its starting position;
- The second rehabilitation motion tested is knee flexion/extension executed also in sagittal plane;
- After knee flexion/extension exercises is performed, the robot is returned again in the starting position.
- The third motion performed is dorsiflexion/plantar flexion, this motion is also in sagittal plane.
- The last motion is ankle inversion/eversion performed in the frontal plane.
- For the hip joint, a dual axis goniometer (for the measurement of the hip motion amplitudes in two perpendicular planes), positioned laterally (SG150);
- For the knee joint, a similar goniometer was used even though the motion is performed in a single plane, thus only the signal from one axis will be interpreted (SG150);
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Robots Association. Multi Annual Roadmap for Robotics in Europe; Robots Association: Préverenges, Switzerland, 2017. [Google Scholar]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global Burden of Stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Wafa, H.A.; Wolfe, C.D.A.; Emmett, E.; Roth, G.A.; Johnson, C.O.Y.; Wang, Y. Burden of Stroke in Europe. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef] [PubMed]
- Gorelick, P.B. The global burden of stroke: Persistent and disabling. Lancet Neurol. 2019, 18, 417–418. [Google Scholar] [CrossRef] [Green Version]
- Lloyd-Jones, D.; Adams, R.J.; Brown, T.M.; Carnethon, M.; Dai, S.; de Simone, G.; Ferguson, T.B.; Ford, E.; Furie, K.; Gillespie, C.; et al. Heart disease and stroke statistics—2010 update: A report from the American heart association. Circulation 2010, 121, e46–e215. [Google Scholar] [PubMed]
- Díaz, I.; Gil, J.J.; Sánchez, E. Lower-Limb Robotic Rehabilitation: Literature Review and Challenges. J. Robot. 2011, 2011, e759764. [Google Scholar] [CrossRef]
- Esquenazi, A.; Packel, A. Robotic-assisted gait training and resto ration. Am. J. Phys. Med. Rehabil. 2012, 91, S228–S231. [Google Scholar] [CrossRef] [PubMed]
- Banala, S.K.; Kim, S.H.; Agrawal, S.K.; Scholz, J.P. Robot assisted gait training with active leg exoskeleton (ALEX). IEEE Trans. Neural Syst. Rehabil. Eng. 2009, 17, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, R.; Rodrigues, L. Development of nonmotorized mechanisms for lower limb rehabilitation. Robotica 2021, 1–18. [Google Scholar] [CrossRef]
- Wang, L.; Chang, Y.; Zhu, H. Internal Model Control and Experimental Study of Ankle Rehabilitation Robot. Robotica 2020, 38, 940–956. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, K.; Chai, Y.; Mo, Z.; Wang, K. Research on mechanical optimization methods of cable-driven lower limb rehabilitation robot. Robotica 2021, 1–16. [Google Scholar] [CrossRef]
- Colombo, G.; Joerg, M.; Schreier, R.; Dietz, V. Treadmill training of paraplegic patients using a robotic orthosis. J. Rehabil. Res. Dev. 2000, 37, 693–700. [Google Scholar] [PubMed]
- Freivogel, S.; Mehrholz, J.; Husak-Sotomayor, T.; Schmalohr, D. Gait training with the newly developed “LokoHelp”-system is feasible for non-ambulatory patients after stroke, spinal cord and brain injury. A feasibility study. Brain Inj. 2008, 22, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Freivogel, S.; Schmalohr, D.; Mehrholz, J. Improved walking ability and reduced therapeutic stress with an electromechanical gait device. J. Rehabil. Med. 2009, 41, 734–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banala, K.; Agrawal, S.K.; Scholz, J.P. Active Leg Exoskeleton (ALEX) for gait rehabilitation of motor-impaired patients. In Proceedings of the 10th IEEE International Conference on Rehabilitation Robotics (ICORR ’07), Noordwijk, The Netherlands, 12–15 June 2007; pp. 401–407. [Google Scholar]
- Hesse, S.; Uhlenbrock, D. A mechanized gait trainer for restoration of gait. J. Rehabil. Res. Dev. 2000, 37, 701–708. [Google Scholar] [PubMed]
- Schmidt, H. Hapticwalker—a novel haptic device for walking simulation. In Proceedings of the EuroHaptics Conference, Munich, Germany, 5–7 June 2004; pp. 60–67. [Google Scholar]
- Chen, S.; Wang, Y.; Li, S.; Wang, G.; Huang, Y.; Mao, X. Lower limb rehabilitation robot. In Proceedings of the ASME/IFToMMInternational Conference on Reconfigurable Mechanisms and Robots (ReMAR ’09), London, UK, 22–24 June 2009; pp. 439–443. [Google Scholar]
- Yoon, J.; Novandy, B.; Yoon, C.H.; Park, K.J. A 6-DOF gait rehabilitation robot with upper and lower limb connections that allows walking velocity updates on various terrains. IEEE/ASME Trans. Mechatron. 2010, 15, 201–215. [Google Scholar] [CrossRef]
- Peshkin, M.; Brown, D.A.; Santos-Munne, J.J.; Makhlin, A.; Lewis, E.; Colgate, J.E.; Patton, J.; Schwandt, D. KineAssist: A robotic overground gait and balance training device. In Proceedings of the 9th IEEE International Conference on Rehabilitation Robotics (ICORR ’05), Evanston, IL, USA, 28 June–1 July 2005; pp. 241–246. [Google Scholar]
- Goffer, A. Gait-Locomotor Apparatus. U.S. Patent Number 7,153,242, 26 December 2006. [Google Scholar]
- Kawamoto, H.Y.; Sankai, H. Power assist system hal-3 for gait disorder person. In Proceedings of the 8th International Conference on Computers Helping People with Special Needs, London, UK, 15–20 July 2002; pp. 196–203. [Google Scholar]
- Schmitt, C.; M’etrailler, P.; Al-Khodairy, A.; Brodard, R.; Fournier, J.; Bouri, M.; Clavel, R. The motion maker: A rehabilitation system combining an orthosis with closed-loop electrical muscle stimulation. In Proceedings of the 8th Vienna International Workshop on Functional Electrical Stimulation, Vienna, Austria, 10–13 September 2004; pp. 117–120. [Google Scholar]
- Girone, M.; Burdea, G.; Bouzit, M.; Popescu, V.; Deutsch, J.E. Stewart platform-based system for ankle telerehabilitation. Auton. Robot. 2001, 10, 203–212. [Google Scholar] [CrossRef]
- Roy, A.; Krebs, H.I.; Patterson, S.L.; Judkins, T.N.; Khanna, I.; Forrester, L.W.; Macko, R.M.; Hogan, N. Measurement of human ankle stiffness using the anklebot. In Proceedings of the 10th IEEE International Conference on Rehabilitation Robotics, (ICORR ’07), Noordwijk, The Netherlands, 12–15 June 2007; pp. 356–363. [Google Scholar]
- Melo, N.; Dórea, C.; Alsina, P.; Araújo, M. Joint trajectory generator for powered orthosis based on gait modelling using PCA and FFT. Robotica 2018, 36, 395–407. [Google Scholar] [CrossRef]
- Huo, W.; Arnez-Paniagua, V.; Ding, G.; Amirat, Y.; Mohammed, S. Adaptive Proxy-Based Controller of an Active Ankle Foot Orthosis to Assist Lower Limb Movements of Paretic Patients. Robotica 2019, 37, 2147–2164. [Google Scholar] [CrossRef]
- Zhou, X.; Liu, G.; Han, B.; Li, H.; Zhang, L.; Liu, X. Different Prevention and Treatment Strategies for Knee Osteoarthritis (KOA) with Various Lower Limb Exoskeletons—A Comprehensive Review. Robotica 2021, 39, 1345–1367. [Google Scholar] [CrossRef]
- Vaida, C.; Birlescu, I.; Pisla, A.; Ulinici, I.; Tarnita, D.; Carbone, G.; Pisla, D. Systematic Design of a Parallel Robotic System for Lower Limb Rehabilitation. IEEE Access 2020, 8, 34522–34537. [Google Scholar] [CrossRef]
- Gherman, B.; Birlescu, I.; Nicolae, P.; Carbone, G.; Tarnita, D.; Pisla, D. On the singularity-free workspace of a parallel robot for lower-limb rehabilitation. Proc. Rom. Acad. 2019, 20, 383–391. [Google Scholar]
- Di Natali, C.; Poliero, T.; Sposito, M.; Graf, E.; Bauer, C.; Pauli, C.; Ortiz, J. Design and Evaluation of a Soft Assistive Lower Limb Exoskeleton. Robotica 2019, 37, 2014–2034. [Google Scholar] [CrossRef] [Green Version]
- Nadas, I.; Gherman, B.; Birlescu, I.; Bogateanu, R.; Banica, A.; Carbone, G.; Pisla, D. Dynamic balancing of RECOVER robotic system. IOP Conf. Ser. Mater. Sci. Eng. 2020, 997, 12083. [Google Scholar] [CrossRef]
- Gherman, B.; Nadas, I.; Tucan, P.; Carbone, G.; Pisla, D. Design and Simulation of Gait Rehabilitation Parallel Robotic System. In New Advances in Mechanisms, Mechanical Transmissions and Robotics; Lovasz, E.C., Maniu, I., Doroftei, I., Ivanescu, M., Gruescu, C.M., Eds.; MTM&Robotics, Mechanisms and Machine Science; Springer: Cham, Switzerland, 2020; Volume 88. [Google Scholar] [CrossRef]
- Gherman, B.; Birlescu, I.; Tucan, P.; Vaida, C.; Pisla, A.; Pisla, D. Modelling and simulation of a robotic system for lower limb rehabilitation. In Proceedings of the ASME 2018 International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, Volume 5B: 42nd Mechanisms and Robotics Conference (V05BT07A083), Quebec City, QC, Canada, 26–29 August 2018; ASME: New York, NY, USA. [Google Scholar] [CrossRef]
- Nadas, I.; Gherman, B.; Albert, S.; Surducan, V.; Pop, N.; Carbone, G.; Banica, A.; Pisla, D. Design and control of Recover Rehabilitation Parallel Robot. In Proceedings of the 1st International Conference on Advanced Research in Engineering, CARE 2020, Tokyo, Japan, 10–30 November 2020; Tarnita, D., Dumitru, N., Paraschiv, G., Dumitru, I., Eds.; Universitaria Craiova: Craiova, Romania, 2020; pp. 3–10. [Google Scholar]
- Gherman, B.; Birlescu, I.; Puskas, F.; Pisla, A.; Carbone, G.; Tucan, P.; Banica, A.; Pisla, D. A Kinematic Characterization of a Parallel Robotic System for Lower Limb Rehabilitation. In Mechanisms and Machine Science; Corves, B., Wenger, P., Hüsing, M., Eds.; EuCoMeS 2018; Springer: Cham, Switzerland, 2019; Volume 59. [Google Scholar] [CrossRef]
- Nadas, I.; Gherman, B.; Albert, S.; Surducan, V.; Pop, N.; Carbone, G.; Banica, A.; Pisla, D. Innovative Development of a Parallel Robotic System for Lower Limb Rehabilitation; Series: Applied Mathematics, Mechanics, and Engineering; Acta Technica Napocensis: Cluj-Napoca, Romania, 2021; Volume 64, pp. S1–S2. ISSN 2393–2988. Available online: https://atna-mam.utcluj.ro/index.php/Acta/article/view/1537 (accessed on 15 September 2021).
- Pisla, D.; Gherman, B.; Nadas, I.; Pop, N.; Craciun, F.; Tucan, P.; Vaida, C.; Carbone, G.; Birlescu, I.; Plitea, N. Innovative Parallel Robot for Medical Recovery of the Lower Limbs. Patent Numbers: RO133815-A0; RO133815-A3, 30 December 2020. [Google Scholar]
- Vaida, C.; Pisla, D.; Schadlbauer, J.; Husty, M.; Plitea, N. Kinematic Analysis of an Innovative Medical Parallel Robot Using Study Parameters. In New Trends in Medical and Service Robots; Wenger, P., Chevallereau, C., Pisla, D., Bleuler, H., Rodić, A., Eds.; Mechanisms and Machine Science; Springer: Cham, Switzerland, 2016; Volume 39. [Google Scholar] [CrossRef]
- Gherman, B.; Vaida, C.; Pisla, D.; Plitea, N.; Gyurka, B.; Lese, D.; Glogoveanu, M. Singularities and workspace analysis for a parallel robot for minimally invasive surgery. In Proceedings of the 2010 IEEE International Conference on Automation, Quality and Testing, Robotics (AQTR), Cluj-Napoca, Romania, 28–30 May 2010; pp. 1–6. [Google Scholar] [CrossRef]
- Vaida, C.; Plitea, N.; Gherman, B.; Szilaghyi, A.; Galdau, B.; Cocorean, D.; Covaciu, F.; Pisla, D. Structural Analysis and Synthesis of Parallel Robots for Brachytherapy. In New Trends in Medical and Service Robots; Mechanisms and Machine Science; Pisla, D., Bleuler, H., Rodic, A., Vaida, C., Pisla, A., Eds.; Springer: Cham, Switzerland, 2014; Volume 16. [Google Scholar] [CrossRef]
- Schonstein, C. Kinematic Control Functions for a Serial Robot Structure Based on the Time Derivative Jacobian Matrix; Series: Applied Mathematics and Mechanics; Acta Technica Napocensis: Cluj-Napoca, Romania, 2018; ISSN 1221-5872. [Google Scholar]
- Vaida, C.; Carbone, G.; Major, K.; Major, Z.; Plitea, N.; Pisla, D. On Human Robot Interaction Modalities in the Upper Limb Rehabilitation after Stroke; Series: Applied Mathematics Mechanics and Engineering; Acta Technica Napocensis: Cluj-Napoca, Romania, 2017; Volume 60, pp. 91–102. [Google Scholar]
- Vaida, C.; Pisla, D.; Plitea, N.; Gherman, B.; Gyurka, B.; Stancel, E.; Hesselbach, J.; Raatz, A.; Vlad, L.; Graur, F. Development of a control system for a parallel robot used in minimally invasive surgery. IFMBE Proc. 2009, 26, 171–176. [Google Scholar]
- Husty, M.; Birlescu, I.; Tucan, P.; Vaida, C.; Pisla, D. An algebraic parameterization approach for parallel robots analysis. Mech. Mach. Theory 2019, 140, 245–257. [Google Scholar] [CrossRef]
- Biometrics Ltd. Available online: https://www.biometricsltd.com/ (accessed on 18 September 2021).
- Centers for Disease Control and Prevention. Normal Joint Range of Motion Study. Available online: https://www.cdc.gov/ncbddd/jointrom/index.html (accessed on 8 October 2021).














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject No. | Gender | Age (Years) | Weight (kg) | Height (cm) |
|---|---|---|---|---|
| 1 | Female | 44 | 53 | 162 |
| 2 | Female | 36 | 55 | 172 |
| 3 | Female | 35 | 53 | 163 |
| 4 | Male | 30 | 68 | 173 |
| 5 | Male | 34 | 70 | 178 |
| 6 | Male | 40 | 76 | 175 |
| 7 | Male | 31 | 89 | 184 |
| 8 | Male | 42 | 80 | 184 |
| Hip Motion | Knee Motion | Ankle Flex/Ext Motion | Ankle Inv/Ev. Motion |
|---|---|---|---|
| 0.0539 ± 0.0296 | 0.0517 ± 0.0294 | 0.0494 ± 0.281 | 0.0481 ± 0.0297 |
| Rehabilitation Motions | (°) |
|---|---|
| Hip flexion | 85° |
| Hip extension | −25° |
| Knee flexion | 118° |
| Knee extension | 0° |
| Ankle dorsiflexion | −25° |
| Ankle plantar flexion | 41° |
| Ankle inversion | −25° |
| Ankle eversion | 25° |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pisla, D.; Nadas, I.; Tucan, P.; Albert, S.; Carbone, G.; Antal, T.; Banica, A.; Gherman, B. Development of a Control System and Functional Validation of a Parallel Robot for Lower Limb Rehabilitation. Actuators 2021, 10, 277. https://doi.org/10.3390/act10100277
Pisla D, Nadas I, Tucan P, Albert S, Carbone G, Antal T, Banica A, Gherman B. Development of a Control System and Functional Validation of a Parallel Robot for Lower Limb Rehabilitation. Actuators. 2021; 10(10):277. https://doi.org/10.3390/act10100277
Chicago/Turabian StylePisla, Doina, Iuliu Nadas, Paul Tucan, Stefan Albert, Giuseppe Carbone, Tiberiu Antal, Alexandru Banica, and Bogdan Gherman. 2021. "Development of a Control System and Functional Validation of a Parallel Robot for Lower Limb Rehabilitation" Actuators 10, no. 10: 277. https://doi.org/10.3390/act10100277