
Descriptive Epidemiology of Soil-Transmitted Helminth Infections in the United States: Using Big Data to Characterize Patients and Analyze Parasitic Disease Trends




Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Temporal Trends
3.2. Case Sex Comparisons
3.3. Case Age Summary
3.4. Human Groups of Specific Ethnicity Summary
3.5. Case Hospitalization and Charges
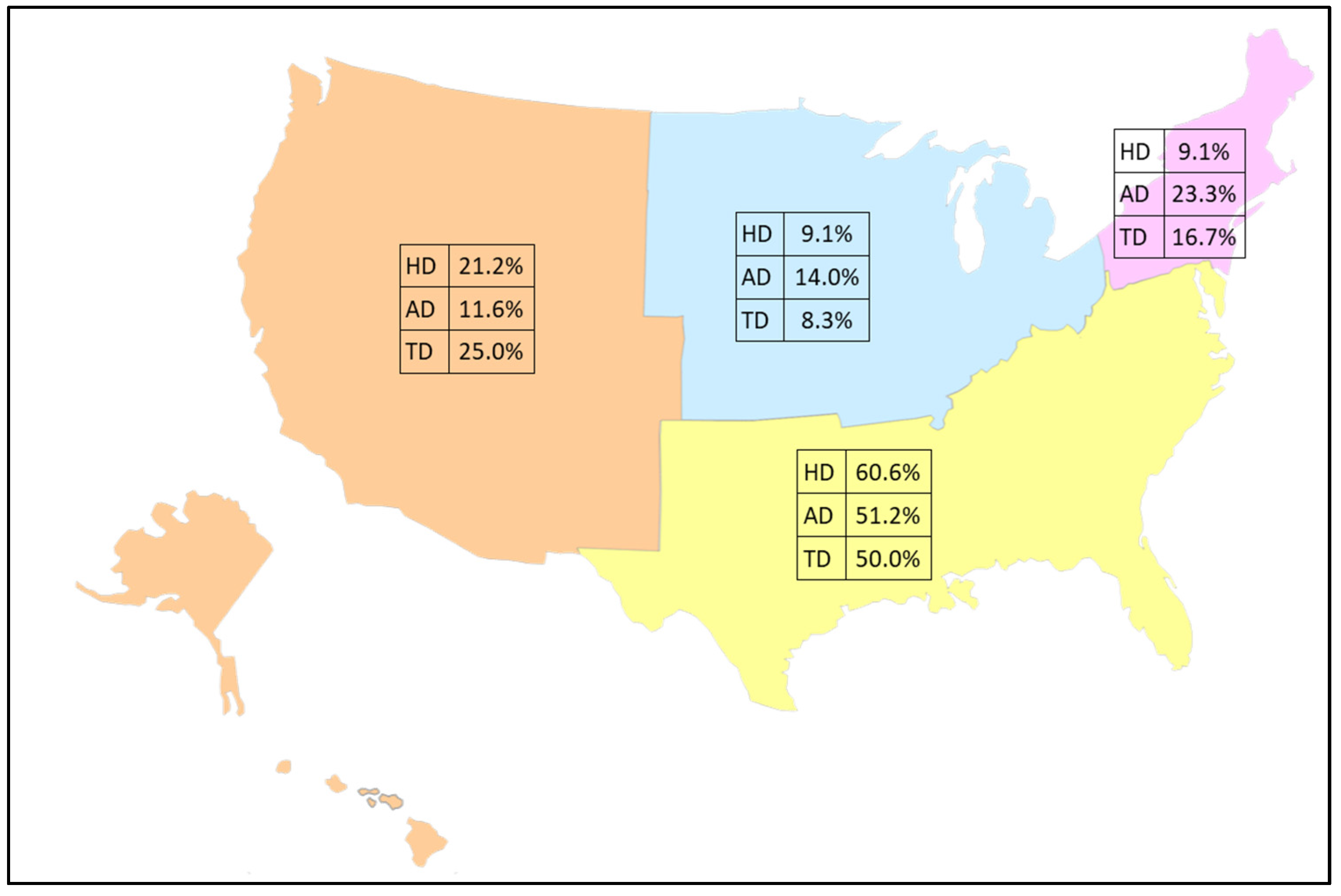
3.6. Regional Geography
3.7. Comorbid Conditions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Algorithm A1: Case Extraction and Summary Analysis Pseudocode Algorithm |
| STEP 1: Label any ICD 9/10 code as “1” if present and “0” otherwise and create a set of new temporary variables with the “0/1” indicator. RECODE Diagnostic columns IF ICD code present = 1 ELSE ICD code not present = 0 INTO temporary disease indicator columns. STEP 2: Obtain sum of all recoded variables and create a variable. COMPUTE SumVariable=sum(across temporary disease columns). STEP 3: Recode the new sum variable in “0” if the sum is 0, or “1” if the sum is anything > 0 into a disease diagnosis column. RECODE SumVariable (0 = 0) (ELSE = 1) INTO DiseaseDiag. STEP 4: Label the new "0/1" sum variable indicator. VALUE LABELS DiseaseDiag 0 = ‘Disease absent’ 1 = ‘Disease Present’. STEP 5: Give the new sum variable a descriptive label. VARIABLE LABELS DiseaseDiag ‘Disease descriptive label’. STEP 6: Delete temporary variable created in STEP 1. DELETE VARIABLES temporary disease indicator columns and sum column. STEP 7: Format new variable as a binary response column. FORMAT DiseaseDiag (F1.0). STEP 8: Export dataset containing only cases for next processing steps. SAVE Reduced dataset for DiseaseDiag = 1. STEP 9: On reduced dataset, add ICD disease labels for each disease into new disease columns. RECODE Diagnostic columns (ICD Number String = ICD Number Numeric) INTO numeric diagnostic columns. STEP 10: Add value labels to ICD numbers. VALUE LABELS numeric diagnostic columns FOR ALL VARS ICD code = ‘ICD name’. STEP 11: Use complex weighting and multiple response computations to obtain frequencies and percentages by key variables of interest. WEIGHT by discharge weight. FREQUENCIES VAR=DiseaseDiag. MULTIPLE RESPONSE VARS=numeric diagnostic columns FOR categorical vars Sex Age Race Region. |
References
- CDC. About Soil-Transmitted Helminths. Available online: https://www.cdc.gov/sth/about/index.html (accessed on 3 October 2024).
- Neglected Tropical Diseases—GLOBAL. Available online: https://www.who.int/health-topics/neglected-tropical-diseases (accessed on 18 October 2024).
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, E.M.; Nutman, T.B. Molecular Diagnostics for Soil-Transmitted Helminths. Am. J. Trop. Med. Hyg. 2016, 95, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Athni, T.S.; Shocket, M.S.; Couper, L.I.; Nova, N.; Caldwell, I.R.; Caldwell, J.M.; Childress, J.N.; Childs, M.L.; de Leo, G.A.; Kirk, D.G.; et al. The Influence of Vector-Borne Disease on Human History: Socio-Ecological Mechanisms. Ecol. Lett. 2021, 24, 829–846. [Google Scholar] [CrossRef] [PubMed]
- Benedetto, C.; Youssef, I.; Shitabata, P.; Nami, N. An Indigenous Case of Cutaneous Larva Migrans. J. Am. Osteopath. Coll. Dermatol. 2017, 38, 2–30. [Google Scholar]
- Lynn, M.K.; Morrissey, J.A.; Conserve, D.F. Soil-Transmitted Helminths in the USA: A Review of Five Common Parasites and Future Directions for Avenues of Enhanced Epidemiologic Inquiry. Curr. Trop Med. Rep. 2021, 8, 32–42. [Google Scholar] [CrossRef]
- Bradbury, R.S.; Martin, L.; Malloch, L.; Martin, M.; Williams, J.M.; Patterson, K.; Sanders, C.; Singh, G.; Arguello, I.; Rodriguez, E.; et al. Surveillance for Soil-Transmitted Helminths in High-Risk County, Mississippi, USA. Emerg. Infect. Dis. J. CDC 2023, 29, 2533. [Google Scholar] [CrossRef]
- Bleakley, H. Disease and Development: Evidence from Hookworm Eradication in the American South. Q. J. Econ. 2007, 122, 73–117. [Google Scholar] [CrossRef]
- Healthcare Cost and Utilization Project (HCUP): 1998–2020; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2022.
- HCUP Partners. Available online: https://hcup-us.ahrq.gov/partners.jsp?NIS (accessed on 24 October 2024).
- HCUP-US NIS Overview. Available online: https://hcup-us.ahrq.gov/nisoverview.jsp (accessed on 3 October 2024).
- Cross, C.L.; Rivera, B.; Sy, F. Descriptive Epidemiological Analysis of Cestode Infections in Nevada: Characterizing Patients and Analyzing Trends Using Patient Utilization Records, 2013–2019. N. J Publ.Health 2023, 20, 1–7. [Google Scholar]
- Producing National HCUP Estimates—Accessible Version. Available online: https://hcup-us.ahrq.gov/tech_assist/nationalestimates/508_course/508course_2018.jsp (accessed on 3 October 2024).
- Healthcare Cost and Utilization Project (HCUP). NIS Notes. Available online: https://hcup-us.ahrq.gov/db/vars/race/nisnote.jsp#general (accessed on 20 November 2024).
- Agrawal, R.; Pattnaik, S.; Kshatri, J.S.; Kanungo, S.; Mandal, N.; Palo, S.K.; Pati, S. Prevalence and Correlates of Soil-Transmitted Helminths in Schoolchildren Aged 5 to 18 Years in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Front. Public Health 2024, 12, 1283054. [Google Scholar] [CrossRef]
- Dunn, J.C.; Turner, H.C.; Tun, A.; Anderson, R.M. Epidemiological Surveys of, and Research on, Soil-Transmitted Helminths in Southeast Asia: A Systematic Review. Parasites Vectors 2016, 9, 31. [Google Scholar] [CrossRef]
- Strunz, E.C.; Addiss, D.G.; Stocks, M.E.; Ogden, S.; Utzinger, J.; Freeman, M.C. Water, Sanitation, Hygiene, and Soil-Transmitted Helminth Infection: A Systematic Review and Meta-Analysis. PLoS Med. 2014, 11, e1001620. [Google Scholar] [CrossRef] [PubMed]
- Starr, M.C.; Montgomery, S.P. Soil-Transmitted Helminthiasis in the United States: A Systematic Review—1940–2010. Am. Soc. Trop. Med. Hyg. 2011, 85, 680–684. [Google Scholar] [CrossRef] [PubMed]
- McKenna, M.L.; McAtee, S.; Bryan, P.E.; Jeun, R.; Ward, T.; Kraus, J.; Bottazzi, M.E.; Hotez, P.J.; Flowers, C.C.; Mejia, R. Human Intestinal Parasite Burden and Poor Sanitation in Rural Alabama. Am. J. Trop. Med. Hyg. 2017, 97, 1623. [Google Scholar] [CrossRef] [PubMed]
- Elman, C.; McGuire, R.A.; Wittman, B. Extending Public Health: The Rockefeller Sanitary Commission and Hookworm in the American South. Am. J. Public Health 2014, 104, 47–58. [Google Scholar] [CrossRef]
- Hotez, P.J.; Brooker, S.; Bethony, J.M.; Bottazzi, M.E.; Loukas, A.; Xiao, S. Hookworm Infection. N. Engl. J. Med. 2004, 351, 799–807. [Google Scholar] [CrossRef]
- Tolera, A.; Dufera, M. The Prevalence of Soil-Transmitted Helminths and Associated Risk Factors among School Children at Sekela Primary School, Western Ethiopia. J. Parasitol. Res. 2020, 2020, 8885734. [Google Scholar] [CrossRef]
- Soares Magalhães, R.J.; Salamat, M.S.; Leonardo, L.; Gray, D.J.; Carabin, H.; Halton, K.; McManus, D.P.; Williams, G.M.; Rivera, P.; Saniel, O.; et al. Mapping the Risk of Soil-Transmitted Helminthic Infections in the Philippines. PLoS Negl. Trop Dis. 2015, 9, e0003915. [Google Scholar] [CrossRef]
- Andargie, Y.; Alelign, A.; Tekeste, Z. Prevalence and Associated Risk Factors of Soil-Transmitted Helminth Infections among Schoolchildren in Mekan Eyesus Town, Northwestern Ethiopia. Parasite Epidemiol. Control. 2024, 27, e00379. [Google Scholar] [CrossRef]
- Muluneh, C.; Hailu, T.; Alemu, G. Prevalence and Associated Factors of Soil-Transmitted Helminth Infections among Children Living with and without Open Defecation Practices in Northwest Ethiopia: A Comparative Cross-Sectional Study. Am. J. Trop. Med. Hyg. 2020, 103, 266–272. [Google Scholar] [CrossRef]
- Kache, R.; Phasuk, N.; Viriyavejakul, P.; Punsawad, C. Prevalence of Soil-Transmitted Helminth Infections and Associated Risk Factors among Elderly Individuals Living in Rural Areas of Southern Thailand. BMC Public Health 2020, 20, 1882. [Google Scholar] [CrossRef]
- McDermott, K.W.; Sun, R. Trends in Hospital Inpatient Stays in the United States, 2005–2014: HCUP Statistics Briefs #225. Available online: https://hcup-us.ahrq.gov/reports/statbriefs/sb225-Inpatient-US-Stays-Trends.pdf (accessed on 24 October 2024).
- Pancreatic-Biliary Ascariasis: Experience of 300 Cases. Available online: https://read.qxmd.com/read/9399767/pancreatic-biliary-ascariasis-experience-of-300-cases (accessed on 24 October 2024).
- Pediatric Ascariasis: Practice Essentials, Background, Pathophysiology. 2024. Available online: https://emedicine.medscape.com/article/996482-overview?form=fpf#a6 (accessed on 24 October 2024).
- Sellau, J.; Hansen, C.S.; Gálvez, R.I.; Linnemann, L.; Honecker, B.; Lotter, H. Immunological Clues to Sex Differences in Parasitic Diseases. Trends Parasitol. 2024, 40, 1029–1041. [Google Scholar] [CrossRef] [PubMed]
- Weatherhead, J.E.; Hotez, P.J.; Mejia, R. The Global State of Helminth Control and Elimination in Children. Pediatr. Clin. N. Am. 2017, 64, 867–877. [Google Scholar] [CrossRef] [PubMed]
- R Lindrose, A.; Mitra, I.; Fraser, J.; Mitre, E.; Hickey, P.W. Helminth Infections in the US Military: From Strongyloidiasis to Schistosomiasis. J. Travel Med. 2021, 28, taab004. [Google Scholar] [CrossRef] [PubMed]
- Coelho, P.R.P.; McGuire, R.A. Racial Differences in Disease Susceptibilities: Intestinal Worm Infections in the Early Twentieth-Century American South. Soc. Hist. Med. 2006, 19, 461–482. [Google Scholar] [CrossRef]
- FastStats. Available online: https://www.cdc.gov/nchs/fastats/hospital.htm (accessed on 22 November 2024).
- Herrick, J.A.; Nordstrom, M.; Maloney, P.; Rodriguez, M.; Naceanceno, K.; Gallo, G.; Mejia, R.; Hershow, R. Parasitic Infections Represent a Significant Health Threat among Recent Immigrants in Chicago. Parasitol. Res. 2020, 119, 1139–1148. [Google Scholar] [CrossRef]
- Okulewicz, A. The Impact of Global Climate Change on the Spread of Parasitic Nematodes. Ann. Parasitol. 2017, 63, 15–20. [Google Scholar] [CrossRef]
- Brooker, S.; Bethony, J.; Hotez, P.J. Human Hookworm Infection in the 21st Century. Adv. Parasitol. 2004, 58, 197. [Google Scholar] [CrossRef]
- Mignatti, A.; Boag, B.; Cattadori, I.M. Host Immunity Shapes the Impact of Climate Changes on the Dynamics of Parasite Infections. Proc. Natl. Acad. Sci. USA 2016, 113, 2970–2975. [Google Scholar] [CrossRef]
- Fox, N.J.; Marion, G.; Davidson, R.S.; White, P.C.L.; Hutchings, M.R. Livestock Helminths in a Changing Climate: Approaches and Restrictions to Meaningful Predictions. Animals 2012, 2, 93. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Disease Condition | ICD 9 (Through 30 September 2015) | ICD 10 (Beginning 1 October 2015) |
|---|---|---|
| Hookworm Disease | ||
| Ancylostomiasis | 126.0, 126.2, 126.3, 126.8 | B76.0 |
| Necatoriasis | 126.1 | B76.1 |
| Other hookworm diseases | 126.9 | B76.8 |
| Hookworm disease, unspecified | 126.9 | B76.9 |
| Ascariasis | ||
| Ascariasis with intestinal complications | 127.0 | B77.0 |
| Ascariasis with other complications | B77.8 | |
| Ascariasis pneumonia | 127.0 with 484.8 | B77.81 |
| Ascariasis with other complications | 127.0 | B77.89 |
| Ascariasis, unspecified | 127.0 | B77.9 |
| Trichuriasis | ||
| Trichuriasis | 127.3 | B79 |
| Statistic | Hookworm Disease | Ascariasis | Trichuriasis | |||
|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |
| Total Cases | 1044 | 759 | 1163 | 1336 | 415 | 297 |
| Mean (Annual) | 45.4 | 33.0 | 50.6 | 58.1 | 18.0 | 12.9 |
| SD | 19.62 | 18.51 | 26.73 | 20.69 | 12.19 | 8.50 |
| LCL (95%) | 36.91 | 25.00 | 39.00 | 49.14 | 12.77 | 9.24 |
| UCL (05%) | 53.88 | 41.00 | 62.13 | 67.03 | 23.31 | 16.59 |
| Median | 38 | 25 | 40 | 57 | 15 | 10 |
| Minimum | 15 | 10 | 10 | 18 | <10 * | <10 |
| Maximum | 91 | 81 | 119 | 93 | 47 | 29 |
| Statistic | Age Group (Years) | ||||||
|---|---|---|---|---|---|---|---|
| <1 | 1–4 | 5–14 | 15–24 | 25–39 | 40–64 | 65+ | |
| Hookworm Disease | |||||||
| Total Cases | 15 | 90 | 181 | 184 | 354 | 565 | 422 |
| % | 0.83% | 4.97% | 9.99% | 10.16% | 19.55% | 31.20% | 23.30% |
| Mean (Annual) | 0.7 | 3.9 | 7.9 | 8.0 | 15.4 | 24.6 | 18.3 |
| SD | 1.72 | 4.04 | 9.26 | 6.93 | 7.20 | 15.92 | 13.12 |
| LCL (95%) | 0 | 2.16 | 3.87 | 5.00 | 12.28 | 17.68 | 12.68 |
| UCL (05%) | 1.40 | 5.66 | 11.87 | 11.00 | 18.51 | 31.45 | 24.02 |
| Median | 0 | 5 | 5 | 5 | 18 | 20 | 15 |
| Minimum | <10 * | <10 | <10 | <10 | <10 | <10 | <10 |
| Maximum | <10 | 11 | 40 | 22 | 29 | 79 | 56 |
| Total Cases | 15 | 90 | 181 | 184 | 354 | 565 | 422 |
| Ascariasis Disease | |||||||
| Total Cases | 23 | 283 | 308 | 322 | 509 | 586 | 497 |
| % | 0.91% | 11.19% | 12.18% | 12.74% | 20.13% | 23.18% | 19.66% |
| Mean (Annual) | 1.0 | 8.5 | 16.0 | 17.2 | 32.0 | 55.7 | 40.5 |
| SD | 2.37 | 11.45 | 11.37 | 11.10 | 11.57 | 12.18 | 10.02 |
| LCL (95%) | 0.00 | 3.52 | 11.04 | 12.38 | 26.99 | 50.43 | 36.18 |
| UCL (05%) | 2.05 | 13.42 | 20.87 | 21.98 | 36.99 | 60.96 | 44.85 |
| Median | 0 | 10 | 10 | 10 | 20 | 25 | 20 |
| Minimum | <10 | <10 | <10 | <10 | <10 | <10 | <10 |
| Maximum | <10 | 57 | 48 | 36 | 50 | 48 | 39 |
| Trichuriasis Disease | |||||||
| Total Cases | <10 | 18 | 102 | 131 | 98 | 203 | 137 |
| % | 0.00% | 2.61% | 14.80% | 19.01% | 14.22% | 29.46% | 19.88% |
| Mean (Annual) | <10 | <10 | <10 | <10 | <10 | <10 | <10 |
| SD | <10 | <10 | <10 | <10 | <10 | <10 | <10 |
| LCL (95%) | <10 | <10 | <10 | <10 | <10 | <10 | <10 |
| UCL (05%) | <10 | <10 | <10 | <10 | <10 | 12.28 | <10 |
| Median | 0 | 0 | 5 | 5 | 0 | 0 | 5 |
| Minimum | <10 | <10 | <10 | <10 | <10 | <10 | <10 |
| Maximum | <10 | <10 | 10 | 19 | 17 | 26 | 21 |
| Total Cases | <10 | 18 | 102 | 131 | 98 | 203 | 137 |
| Statistic | Human Group of Specific Ethnicity | |||||
|---|---|---|---|---|---|---|
| White | Black | Hispanic | Asian or PI | Native American | Other | |
| Hookworm Disease | ||||||
| Total Cases | 895 | 155 | 297 | 121 | 20 | 165 |
| % | 54.14 | 9.38 | 17.97 | 7.32 | 1.21 | 9.98 |
| Mean (Annual) | 38.9 | 6.7 | 12.9 | 5.3 | 0.9 | 7.2 |
| SD | 16.53 | 5.40 | 7.80 | 5.40 | 3.40 | 10.46 |
| LCL (95%) | 31.76 | 4.41 | 9.54 | 2.92 | −0.60 | 2.65 |
| UCL (05%) | 46.06 | 9.07 | 16.29 | 7.60 | 2.34 | 11.70 |
| Median | 35 | 5 | 10 | 5 | 0 | 5 |
| Minimum | 20 | <10 * | <10 | <10 | <10 | <10 |
| Maximum | 89 | 22 | 26 | 22 | 16 | 40 |
| Total Cases | 895 | 155 | 297 | 121 | 20 | 165 |
| Ascariasis Disease | ||||||
| Total Cases | 632 | 405 | 634 | 176 | 45 | 198 |
| % | 30.24 | 19.38 | 30.33 | 8.42 | 2.15 | 9.47 |
| Mean (Annual) | 27.5 | 17.6 | 27.6 | 7.7 | 2.0 | 8.6 |
| SD | 9.82 | 19.79 | 18.76 | 5.73 | 4.47 | 7.56 |
| LCL (95%) | 23.23 | 9.05 | 19.45 | 5.17 | 0.02 | 5.34 |
| UCL (05%) | 31.73 | 26.17 | 35.68 | 10.13 | 3.89 | 11.88 |
| Median | 25 | 15 | 25 | 8 | 0 | 6 |
| Minimum | 10 | <10 | <10 | <10 | <10 | <10 |
| Maximum | 50 | 99 | 99 | 19 | 20 | 26 |
| Trichuriasis Disease | ||||||
| Total Cases | 115 | 114 | 199 | 86 | <10 | 61 |
| % | 20.00 | 19.83 | 34.61 | 14.96 | <10 | 10.61 |
| Mean (Annual) | 5.0 | 5.0 | 8.7 | 3.7 | <10 | 2.7 |
| SD | 5.04 | 7.53 | 7.53 | 4.51 | <10 | 3.46 |
| LCL (95%) | 2.82 | 1.70 | 5.40 | 1.79 | <10 | 1.16 |
| UCL (05%) | 7.18 | 8.21 | 11.91 | 5.69 | <10 | 4.15 |
| Median | 5 | 4 | 10 | 0 | <10 | 0 |
| Minimum | <10 | <10 | <10 | <10 | <10 | <10 |
| Maximum | 21 | 32 | 24 | 11 | <10 | 12 |
| Total Cases | 115 | 114 | 199 | 86 | <10 | 61 |
| CONDITION (STH) | COMORBIDITY |
|---|---|
| Hookworm Disease (HD) | Cellulitis/abscess of foot (9.4%) Hypopotassemia (9.2%) Cellulitis/abscess of leg (7.6%) Trichuriasis (5.9%) Congestive heart failure (5.3%) |
| Ascariasis Disease (AD) | Volume depletion (6.9%) Urinary tract infection (6.0%) Hookworm disease (5.1%) Acute pancreatitis (4.7%) Hypopotassemia (4.5%) |
| Trichuriasis Disease (TD) | Ascariasis (7.9%) Hemorrhoids (6.0%) Volume depletion (5.9%) Acid/base balance disorder (5.6%) Shigella boydii infection (5.3%) |
| Shared Conditions among HD, AD, TD | Essential hypertension (11.9%) Type II diabetes mellitus (5.0%) Anemia, unspecified (5.0%) Iron deficiency anemia (4.9%) Tobacco use disorder (4.6%) Acute kidney failure (4.3%) Congestive heart failure (4.0%) Hyposmolality/Hyponatremia (3.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cross, C.L.; Carrier, B.; Alcala, M.A.A.; Messenger, L.A. Descriptive Epidemiology of Soil-Transmitted Helminth Infections in the United States: Using Big Data to Characterize Patients and Analyze Parasitic Disease Trends. Pathogens 2024, 13, 1091. https://doi.org/10.3390/pathogens13121091
Cross CL, Carrier B, Alcala MAA, Messenger LA. Descriptive Epidemiology of Soil-Transmitted Helminth Infections in the United States: Using Big Data to Characterize Patients and Analyze Parasitic Disease Trends. Pathogens. 2024; 13(12):1091. https://doi.org/10.3390/pathogens13121091
Chicago/Turabian StyleCross, Chad L., Bryson Carrier, Miklo A. A. Alcala, and Louisa A. Messenger. 2024. "Descriptive Epidemiology of Soil-Transmitted Helminth Infections in the United States: Using Big Data to Characterize Patients and Analyze Parasitic Disease Trends" Pathogens 13, no. 12: 1091. https://doi.org/10.3390/pathogens13121091
APA StyleCross, C. L., Carrier, B., Alcala, M. A. A., & Messenger, L. A. (2024). Descriptive Epidemiology of Soil-Transmitted Helminth Infections in the United States: Using Big Data to Characterize Patients and Analyze Parasitic Disease Trends. Pathogens, 13(12), 1091. https://doi.org/10.3390/pathogens13121091