
CRP Monitoring in Early Hospitalization: Implications for Predicting Outcomes in Patients with COVID-19

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
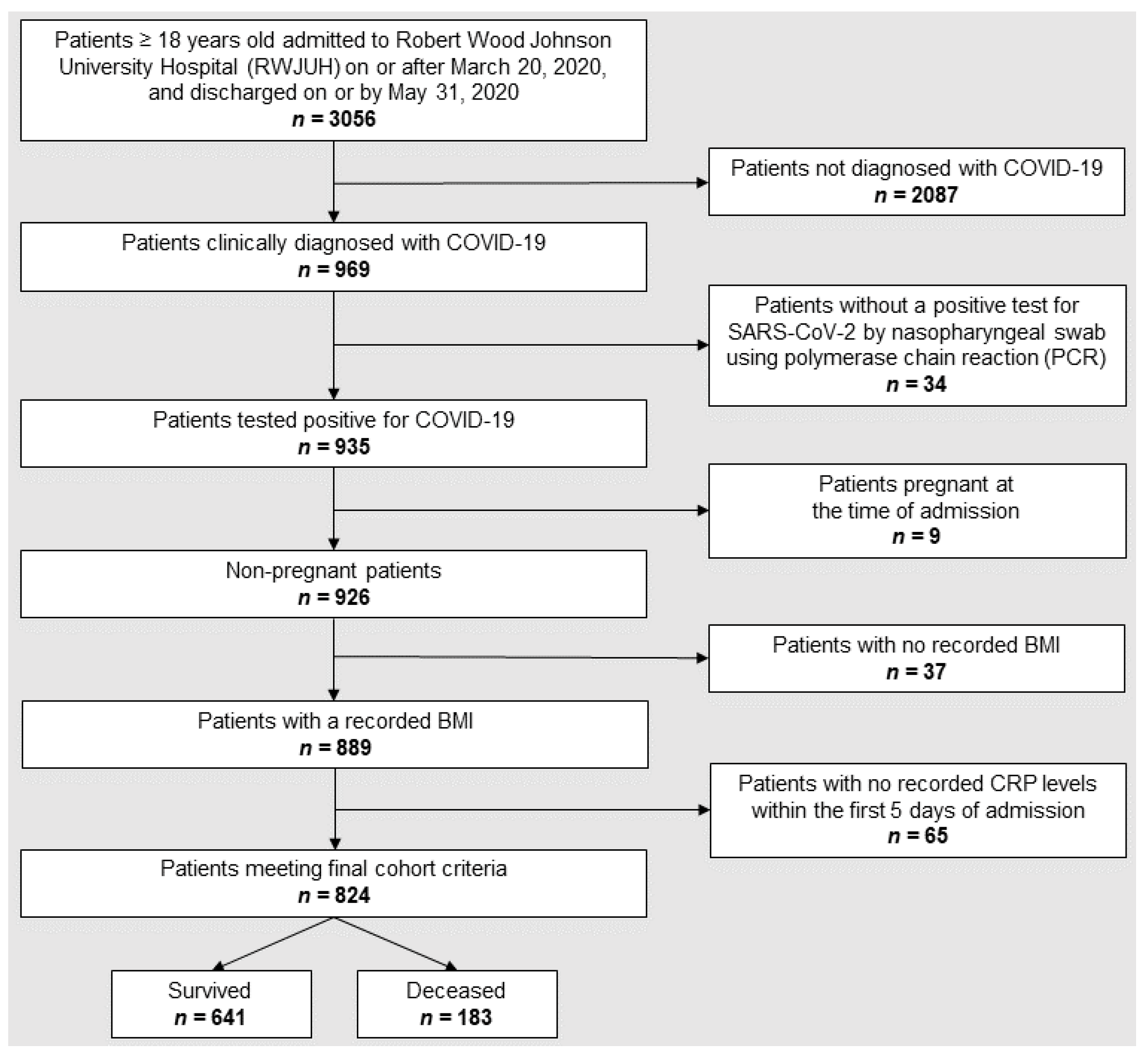
2.1. Data Collection and Patient Population
2.2. Statistical Analysis
3. Results
3.1. Characteristics of Study Population
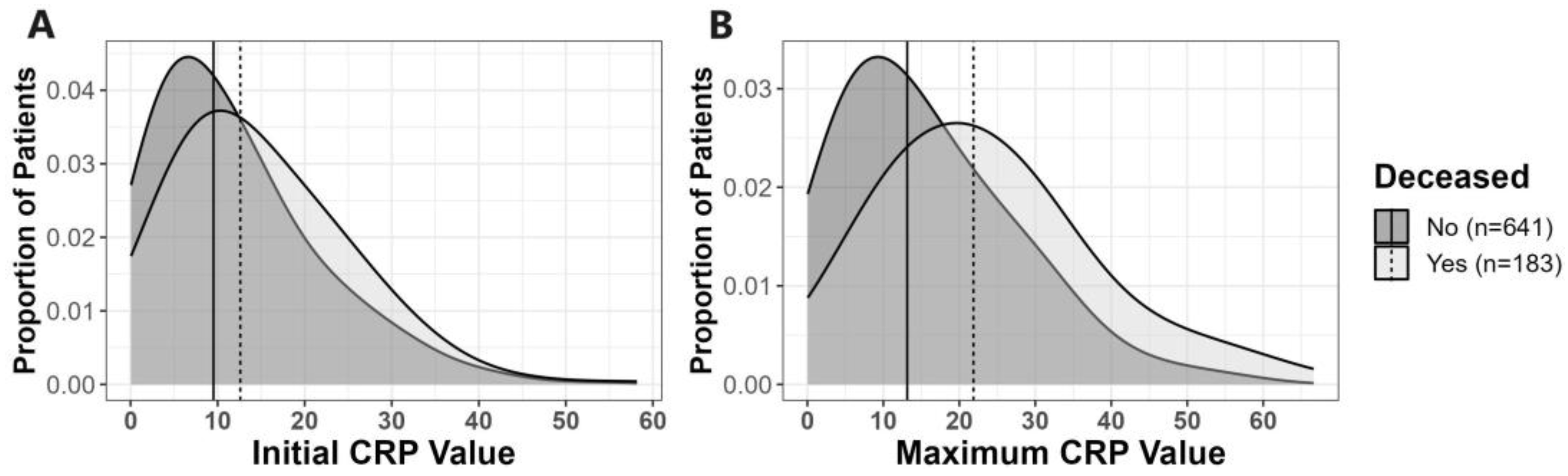
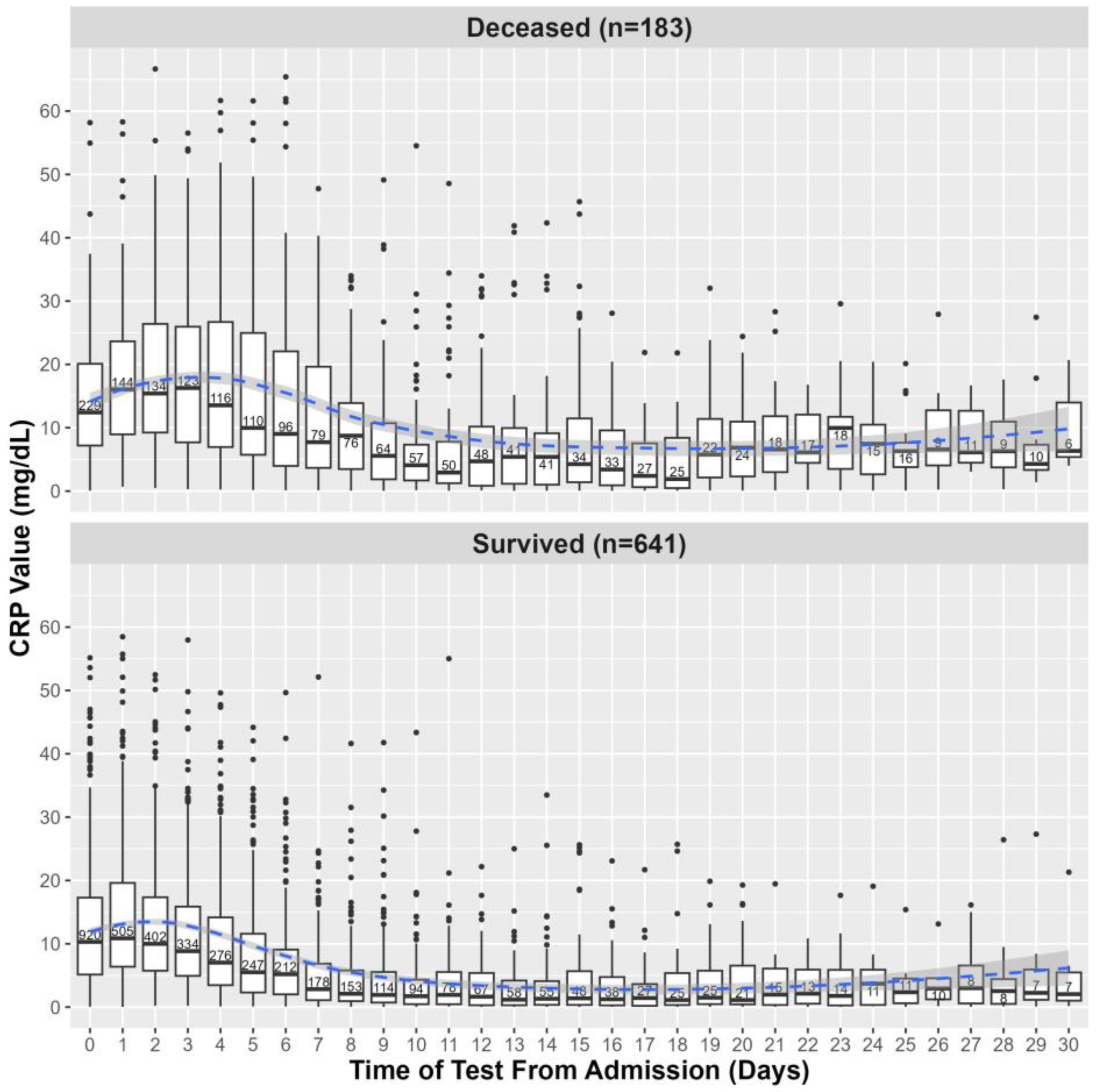
3.2. Relationship of CRP Levels to COVID-19 Patients’ Death
3.3. Relationship between MAX CRP Values with Age and COVID-19 Outcomes
3.4. Relationship between MAX CRP Values, Sex, and COVID-19 Outcomes
3.5. Relationship between MAX CRP Values, Body Mass Index, Age and COVID-19 Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Perez, L. Acute phase protein response to viral infection and vaccination. Arch. Biochem. Biophys. 2019, 671, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Vasileva, D.; Badawi, A. C-reactive protein as a biomarker of severe H1N1 influenza. Inflamm. Res. 2019, 68, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Young, B.; Gleeson, M.; Cripps, A.W. C-reactive protein: A critical review. Pathology 1991, 23, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Black, S.; Kushner, I.; Samols, D. C-reactive Protein. J. Biol. Chem. 2004, 279, 48487–48490. [Google Scholar] [CrossRef]
- Regolo, M.; Vaccaro, M.; Sorce, A.; Stancanelli, B.; Colaci, M.; Natoli, G.; Russo, M.; Alessandria, I.; Motta, M.; Santangelo, N.; et al. Neutrophil-to-Lymphocyte Ratio (NLR) Is a Promising Predictor of Mortality and Admission to Intensive Care Unit of COVID-19 Patients. J. Clin. Med. 2022, 11, 2235. [Google Scholar] [CrossRef]
- Mertens, E.; Serrien, B.; Vandromme, M.; Peñalvo, J.L. Predicting COVID-19 progression in hospitalized patients in Belgium from a multi-state model. Front. Med. 2022, 9, 1027674. [Google Scholar] [CrossRef]
- Milenkovic, M.; Hadzibegovic, A.; Kovac, M.; Jovanovic, B.; Stanisavljevic, J.; Djikic, M.; Sijan, D.; Ladjevic, N.; Palibrk, I.; Djukanovic, M.; et al. D-dimer, CRP, PCT, and IL-6 Levels at Admission to ICU Can Predict In-Hospital Mortality in Patients with COVID-19 Pneumonia. Oxid. Med. Cell. Longev. 2022, 2022, 8997709. [Google Scholar] [CrossRef]
- Gambichler, T.; Schuleit, N.; Susok, L.; Becker, J.C.; Scheel, C.H.; Torres-Reyes, C.; Overheu, O.; Reinacher-Schick, A.; Schmidt, W. Prognostic Performance of Inflammatory Biomarkers Based on Complete Blood Counts in COVID-19 Patients. Viruses 2023, 15, 1920. [Google Scholar] [CrossRef]
- Hamad, D.A.; Aly, M.M.; Abdelhameid, M.A.; Ahmed, S.A.; Shaltout, A.S.; Abdel-Moniem, A.E.; Ragheb, A.M.R.; Attia, M.N.; Meshref, T.S. Combined Blood Indexes of Systemic Inflammation as a Mirror to Admission to Intensive Care Unit in COVID-19 Patients: A Multicentric Study. J. Epidemiol. Glob. Health 2022, 12, 64–73. [Google Scholar] [CrossRef]
- Fawzy, M.; Ahmed, S.; Abdelhady, S. Assessment of diagnostic and prognostic laboratory biomarkers in severe COVID-19 patients admitted to intensive care unit. Egypt J. Immunol. 2023, 30, 1–13. [Google Scholar] [CrossRef]
- Keri, V.C.; Jorwal, P.; Verma, R.; Ranjan, P.; Upadhyay, A.D.; Aggarwal, A.; Sarda, R.; Sharma, K.; Sahni, S.; Rajanna, C. Novel Scoring Systems to Predict the Need for Oxygenation and ICU Care, and Mortality in Hospitalized COVID-19 Patients: A Risk Stratification Tool. Cureus 2022, 14, e27459. [Google Scholar] [CrossRef] [PubMed]
- Mueller, A.A.; Tamura, T.; Crowley, C.P.; DeGrado, J.R.; Haider, H.; Jezmir, J.L.; Keras, G.; Penn, E.H.; Massaro, A.F.; Kim, E.Y. Inflammatory Biomarker Trends Predict Respiratory Decline in COVID-19 Patients. Cell Rep. Med. 2020, 1, 100144. [Google Scholar] [CrossRef]
- Herold, T.; Jurinovic, V.; Arnreich, C.; Lipworth, B.J.; Hellmuth, J.C.; von Bergwelt-Baildon, M.; Klein, M.; Weinberger, T. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J. Allergy Clin. Immunol. 2020, 146, 128–136.e4. [Google Scholar] [CrossRef]
- Zhang, Z.-L.; Hou, Y.-L.; Li, D.-T.; Li, F.-Z. Laboratory findings of COVID-19: A systematic review and meta-analysis. Scand. J. Clin. Lab. Investig. 2020, 80, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.; Huang, Y.; Shi, F.; Tan, K.; Ma, Q.; Chen, Y.; Jiang, X.; Li, X. C-reactive protein correlates with computed tomographic findings and predicts severe COVID-19 early. J. Med. Virol. 2020, 92, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Zhou, W.; Yan, X.; Guo, T.; Wang, B.; Xia, H.; Ye, L.; Xiong, J.; Jiang, Z.; Liu, Y.; et al. Prognostic Value of C-Reactive Protein in Patients With Coronavirus 2019. Clin. Infect. Dis. 2020, 71, 2174–2179. [Google Scholar] [CrossRef]
- Bartoletti, M.; Giannella, M.; Scudeller, L.; Tedeschi, S.; Rinaldi, M.; Bussini, L.; Fornaro, G.; Pascale, R.; Pancaldi, L.; Pasquini, Z.; et al. Development and validation of a prediction model for severe respiratory failure in hospitalized patients with SARS-CoV-2 infection: A multicentre cohort study (PREDI-CO study). Clin. Microbiol. Infect. 2020, 26, 1545–1553. [Google Scholar] [CrossRef]
- Webb, B.J.; Peltan, I.D.; Jensen, P.; Hoda, D.; Hunter, B.; Silver, A.; Starr, N.; Buckel, W.; Grisel, N.; Hummel, E.; et al. Clinical criteria for COVID-19-associated hyperinflammatory syndrome: A cohort study. Lancet Rheumatol. 2020, 2, e754–e763. [Google Scholar] [CrossRef]
- Wang, G.; Wu, C.; Zhang, Q.; Wu, F.; Yu, B.; Lv, J.; Li, Y.; Li, T.; Zhang, S.; Wu, C.; et al. C-Reactive Protein Level May Predict the Risk of COVID-19 Aggravation. Open Forum Infect. Dis. 2020, 7, ofaa153. [Google Scholar] [CrossRef]
- Stringer, D.; Braude, P.; Myint, P.K.; Evans, L.; Collins, J.T.; Verduri, A.; Quinn, T.J.; Vilches-Moraga, A.; Stechman, M.J.; Pearce, L.; et al. The role of C-reactive protein as a prognostic marker in COVID-19. Int. J. Epidemiol. 2021, 50, 420–429. [Google Scholar] [CrossRef]
- Sharifpour, M.; Rangaraju, S.; Liu, M.; Alabyad, D.; Nahab, F.B.; Creel-Bulos, C.M.; Jabaley, C.S. C-Reactive protein as a prognostic indicator in hospitalized patients with COVID-19. PLoS ONE 2020, 15, e0242400. [Google Scholar] [CrossRef] [PubMed]
- Sahu, B.R.; Kampa, R.K.; Padhi, A.; Panda, A.K. C-reactive protein: A promising biomarker for poor prognosis in COVID-19 infection. Clin. Chim. Acta 2020, 509, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Wyczalkowska-Tomasik, A.; Czarkowska-Paczek, B.; Zielenkiewicz, M.; Paczek, L. Inflammatory Markers Change with Age, but do not Fall Beyond Reported Normal Ranges. Arch. Immunol. Ther. Exp. 2016, 64, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Starke, K.R.; Reissig, D.; Petereit-Haack, G.; Schmauder, S.; Nienhaus, A.; Seidler, A. The isolated effect of age on the risk of COVID-19 severe outcomes: A systematic review with meta-analysis. BMJ Glob. Health 2021, 6, e006434. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Mi, J.; Zhong, W.; Huang, C.; Zhang, W.; Tan, L.; Ding, L. Gender, age and comorbidities as the main prognostic factors in patients with COVID-19 pneumonia. Am. J. Transl. Res. 2020, 12, 6537–6548. [Google Scholar] [PubMed]
- Gao, Y.D.; Ding, M.; Dong, X.; Zhang, J.J.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Ou, M.; Zhu, J.; Ji, P.; Li, H.; Zhong, Z.; Li, B.; Pang, J.; Zhang, J.; Zheng, X. Risk factors of severe cases with COVID-19: A meta-analysis. Epidemiol. Infect. 2020, 148, e175. [Google Scholar] [CrossRef]
- Wolff, D.; Nee, S.; Hickey, N.S.; Marschollek, M. Risk factors for Covid-19 severity and fatality: A structured literature review. Infection 2021, 49, 15–28. [Google Scholar] [CrossRef]
- Zhang, J.J.; Cao, Y.Y.; Tan, G.; Dong, X.; Wang, B.C.; Lin, J.; Yan, Y.Q.; Liu, G.H.; Akdis, M.; Akdis, C.A.; et al. Clinical, radiological, and laboratory characteristics and risk factors for severity and mortality of 289 hospitalized COVID-19 patients. Allergy 2021, 76, 533–550. [Google Scholar] [CrossRef]
- Kalligeros, M.; Shehadeh, F.; Mylona, E.K.; Benitez, G.; Beckwith, C.G.; Chan, P.A.; Mylonakis, E. Association of Obesity with Disease Severity Among Patients with Coronavirus Disease 2019. Obesity 2020, 28, 1200–1204. [Google Scholar] [CrossRef] [PubMed]
- Foulkes, A.S.; Selvaggi, C.; Shinnick, D.; Lumish, H.; Kim, E.; Cao, T.; Thaweethai, T.; Qian, J.; Lu, F.; Yan, J.; et al. Understanding the Link Between Obesity and Severe COVID-19 Outcomes: Causal Mediation by Systemic Inflammatory Response. J. Clin. Endocrinol. Metab. 2022, 107, e698–e707. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Zheng, K.I.; Wang, X.-B.; Sun, Q.-F.; Pan, K.-H.; Wang, T.-Y.; Chen, Y.-P.; Targher, G.; Byrne, C.D.; George, J.; et al. Obesity Is a Risk Factor for Greater COVID-19 Severity. Diabetes Care 2020, 43, e72–e74. [Google Scholar] [CrossRef]
- Lighter, J.; Phillips, M.; Hochman, S.; Sterling, S.; Johnson, D.; Francois, F.; Stachel, A. Obesity in Patients Younger Than 60 Years Is a Risk Factor for COVID-19 Hospital Admission. Clin. Infect Dis. 2020, 71, 896–897. [Google Scholar] [CrossRef] [PubMed]
- Klang, E.; Kassim, G.; Soffer, S.; Freeman, R.; Levin, M.A.; Reich, D.L. Severe Obesity as an Independent Risk Factor for COVID-19 Mortality in Hospitalized Patients Younger than 50. Obesity 2020, 28, 1595–1599. [Google Scholar] [CrossRef]
- Choi, J.; Joseph, L.; Pilote, L. Obesity and C-reactive protein in various populations: A systematic review and meta-analysis. Obes. Rev. 2013, 14, 232–244. [Google Scholar] [CrossRef]
- Park, H.S.; Park, J.Y.; Yu, R. Relationship of obesity and visceral adiposity with serum concentrations of CRP, TNF-alpha and IL-6. Diabetes Res. Clin. Pract. 2005, 69, 29–35. [Google Scholar] [CrossRef]
- Wee, C.C.; Mukamal, K.J.; Huang, A.; Davis, R.B.; McCarthy, E.P.; Mittleman, M.A. Obesity and C-reactive protein levels among white, black, and hispanic US adults. Obesity 2008, 16, 875–880. [Google Scholar] [CrossRef]
- McNeill, J.N.; Lau, E.S.; Paniagua, S.M.; Liu, E.E.; Wang, J.K.; Bassett, I.V.; Selvaggi, C.A.; Lubitz, S.A.; Foulkes, A.S.; Ho, J.E. The role of obesity in inflammatory markers in COVID-19 patients. Obes. Res. Clin. Pract. 2021, 15, 96–99. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef]
- Natanov, D.; Avihai, B.; McDonnell, E.; Lee, E.; Cook, B.; Altomare, N.; Ko, T.; Chaia, A.; Munoz, C.; Ouellette, S.; et al. Predicting COVID-19 prognosis in hospitalized patients based on early status. mBio 2023, 14, e0150823. [Google Scholar] [CrossRef]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir Crit. Care Med. 2019, 200, e45–e67. [Google Scholar]
- National Center for Health Statistics (U.S.). Guidance for Certifying Deaths Due to Coronavirus Disease 2019 (COVID–19): Expanded in February 2023 to Include Guidance for Certifying Deaths Due to Post-acute Sequelae of COVID-19. Available online: https://stacks.cdc.gov/view/cdc/124588 (accessed on 31 October 2023).
- CDC. Defining Adult Overweight & Obesity. Available online: https://www.cdc.gov/obesity/basics/adult-defining.html (accessed on 19 September 2023).
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Shrout, E.; Bolger, N. Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychol. Methods 2002, 7, 422–445. [Google Scholar] [CrossRef] [PubMed]
- Rees, E.M.; Nightingale, E.S.; Jafari, Y.; Waterlow, N.R.; Clifford, S.; Pearson, C.A.B.; CMMID Working Group; Jombart, T.; Procter, S.R.; Knight, G.M. COVID-19 length of hospital stay: A systematic review and data synthesis. BMC Med. 2020, 18, 270. [Google Scholar] [CrossRef]
- Lakoski, S.G.; Cushman, M.; Criqui, M.; Rundek, T.; Blumenthal, R.S.; D’Agostino, R.B., Jr.; Herrington, D.M. Gender and C-reactive protein: Data from the Multiethnic Study of Atherosclerosis (MESA) cohort. Am. Heart J. 2006, 152, 593–598. [Google Scholar] [CrossRef]
- Khera, A.; McGuire, D.K.; Murphy, S.A.; Stanek, H.G.; Das, S.R.; Vongpatanasin, W.; Wians, F.H.; Grundy, S.M.; de Lemos, J.A. Race and gender differences in C-reactive protein levels. J. Am. Coll. Cardiol. 2005, 46, 464–469. [Google Scholar] [CrossRef]
- Aronson, D.; Bartha, P.; Zinder, O.; Kerner, A.; Markiewicz, W.; Avizohar, O.; Brook, G.J.; Levy, Y. Obesity is the major determinant of elevated C-reactive protein in subjects with the metabolic syndrome. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 674–679. [Google Scholar] [CrossRef]
- Gudowska-Sawczuk, M.; Wrona, A.; Gruszewska, E.; Cylwik, B.; Panasiuk, A.; Flisiak, R.; Chrostek, L. Serum level of interleukin-6 (IL-6) and N-terminal propeptide of procollagen type I (PINP) in patients with liver diseases. Scand. J. Clin. Lab. Investig. 2018, 78, 125–130. [Google Scholar] [CrossRef]
- Han, M.S.; White, A.; Perry, R.J.; Camporez, J.-P.; Hidalgo, J.; Shulman, G.I.; Davis, R.J. Regulation of adipose tissue inflammation by interleukin 6. Proc. Natl. Acad. Sci. USA 2020, 117, 2751–2760. [Google Scholar] [CrossRef]
- Ziegler, L.; Lundström, A.; Havervall, S.; Thålin, C.; Gigante, B. IL-6 signalling biomarkers in hospitalised patients with moderate to severe SARS-CoV-2 infection in a single centre study in Sweden. Cytokine 2022, 159, 156020. [Google Scholar] [CrossRef] [PubMed]
- Fakhouri, T.H.; Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of obesity among older adults in the United States, 2007–2010. NCHS Data Brief 2012, 106, 1–8. [Google Scholar]
- Lapice, E.; Maione, S.; Patti, L.; Cipriano, P.; Rivellese, A.A.; Riccardi, G.; Vaccaro, O. Abdominal adiposity is associated with elevated C-reactive protein independent of BMI in healthy nonobese people. Diabetes Care 2009, 32, 1734–1736. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Zhao, H.; Yin, C.; Lan, X.; Wu, L.; Du, X.; Griffiths, H.R.; Gao, D. Hepatokines and Myokines: Focus on Their Role and Molecular Mechanisms in Adipose Tissue Inflammation. Front. Endocrinol. 2022, 13, 873699. [Google Scholar] [CrossRef]
- Visser, M.; Bouter, L.M.; McQuillan, G.M.; Wener, M.H.; Harris, T.B. Elevated C-reactive protein levels in overweight and obese adults. JAMA 1999, 282, 2131–2135. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Demographics | Overall (n = 824) | Survived (n = 641, 77.8%) | Deceased (n = 183, 22.2%) | p-Value + |
|---|---|---|---|---|
| Age on Admission | 63 (IQR: 51–75) * | 60 (IQR: 49–72) | 72 (IQR: 63.5–83.5) | <0.001 |
| LOS (days) | 8 (IQR: 4–12) | 7 (IQR: 4–11) | 10 (IQR: 6–17) | <0.001 |
| Number of patients with LOS ≥ 5 days | 587 (71.2%) ** | 433 (67.6%) | 154 (84.2) | <0.001 |
| Sex | 0.573 | |||
| Female | 314 (38.1%) | 241 (37.6%) | 73 (39.9%) | |
| Male | 510 (61.9%) | 400 (62.4%) | 110 (60.1%) | |
| Ethnicity | <0.001 | |||
| African American | 115 (14.0%) | 95 (14.8%) | 20 (10.9%) | |
| Asian | 57 (6.8%) | 43 (6.7%) | 14 (7.7%) | |
| Hispanic | 276 (33.5%) | 235 (36.7%) | 41 (22.4%) | |
| Other | 26 (3.2%) | 20 (3.1%) | 6 (3.3%) | |
| South Asian | 46 (5.6%) | 38 (5.9%) | 8 (4.4%) | |
| White | 304 (36.9%) | 210 (32.8%) | 84 (51.4%) | |
| BMI Group | 0.463 | |||
| Underweight or Normal | 262 (31.8%) | 197 (30.7%) | 65 (35.6%) | |
| Overweight | 276 (33.5%) | 219 (34.2%) | 57 (31.1%) | |
| Obese | 286 (34.7%) | 225 (35.1%) | 61 (33.3%) | |
| Comorbidity | ||||
| Obesity | 288 (35.0%) | 226 (35.3%) | 62 (33.9%) | 0.730 |
| Hypertension | 523 (63.5%) | 389 (60.7%) | 134 (73.2%) | 0.002 |
| CAD or MI | 161 (19.5%) | 108 (16.8%) | 53 (29.0%) | <0.001 |
| Diabetes | 330 (40.0%) | 252 (39.3%) | 78 (42.6%) | 0.420 |
| Chronic Kidney Disease | 91 (11.0%) | 61 (9.5%) | 30 (16.4%) | 0.009 |
| Chronic Liver Disease | 23 (2.8%) | 15 (2.3%) | 8 (4.4%) | 0.141 |
| Autoimmune Condition | 41 (5.0%) | 30 (4.7%) | 11 (6.0%) | 0.465 |
| Asthma | 69 (8.4%) | 59 (9.2%) | 10 (5.5%) | 0.107 |
| COPD | 71 (8.6%) | 48 (7.5%) | 23 (12.6%) | 0.031 |
| Pulmonary—Other | 55 (6.7%) | 41 (6.4%) | 14 (7.7%) | 0.549 |
| Malignancy (history of) | 110 (13.3%) | 70 (10.9%) | 40 (21.9%) | <0.001 |
| ATSG Category | <0.001 | |||
| Non-Severe | 545 (66.1%) | 545 (85.0%) | 0 (0%) | |
| Severe | 279 (33.9%) | 96 (15.0%) | 183 (100%) |
| Laboratory Values [Median (IQR)] | Overall (n = 824) | Survived (n = 641, 77.8%) | Deceased (n = 183, 22.2%) | p-Value * | Reference Range |
|---|---|---|---|---|---|
| C-Reactive Protein | |||||
| Max CRP | 15.02 (7.71–25.24) | 13.14 (6.58–22.65) | 21.86 (13.16–30.79) | <0.001 | <0.07 mg/dL |
| On Admission | 10.32 (5.26–17.63) | 9.52 (4.82–16.43) | 12.60 (7.46–21.24) | <0.001 | <0.07 mg/dL |
| Admission values | |||||
| [Eosinophil] | 0.00 (0.00–0.03) | 0.01 (0.00–0.03) | 0.00 (0.00–0.01) | <0.001 | 0.03–0.27 × 103/μL |
| [Lymphocyte] | 0.83 (0.59–1.21) | 0.87 (0.64–1.25) | 0.73 (0.51–1.06) | <0.001 | 1.16–3.18 × 103/μL |
| [Neutrophil] | 6.10 (4.34–8.83) | 5.99 (4.23–8.33) | 6.84 (4.74–9.82) | 0.009 | 2.00–7.15 × 103/μL |
| BUN | 18 (11–32) | 15 (11–26) | 30 (20–49) | <0.001 | 6–23 mg/dL |
| D-Dimer | 1091 (636–1932) | 1023 (570–1813) | 1207 (861–3342) | <0.001 | 0–500 ng/mL |
| Ferritin | 779 (410–1475) | 735 (396–1376) | 1037 (453–1786) | 0.004 | 20–335 ng/mL |
| INR | 1.17 (1.08–1.29) | 1.16 (1.08–1.28) | 1.19 (1.08–1.34) | 0.035 | 0.8–1.1 |
| [WBC] | 7.9 (5.9–10.7) | 7.7 (5.8–10.3) | 8.4 (6.1–11.4) | 0.026 | 4.0–10.0 × 103/μL |
| Regression Models | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| CRP | ||
| Initial CRP (continuous) → Death | 1.005 (1.002, 1.008) | <0.001 |
| Initial CRP (>10 mg/dL) → Death | 1.62 (1.17, 2.23) | 0.004 |
| MAX CRP (continuous) → Death | 1.009 (1.006, 1.011) | <0.001 |
| MAX CRP (>10 mg/dL) → Death | 3.99 (2.59, 6.39) | <0.001 |
| Age | ||
| Age (≥60 years old) → Death | 4.20 (2.83, 6.41) | <0.001 |
| Age (≥60 years old) → MAX CRP (>10 mg/dL) | 0.93 (0.70, 1.25) | 0.65 |
| Age (≥60 years old) × MAX CRP (>10 mg/dL) → Death * | 0.48 (0.07, 1.82) | 0.35 |
| Sex | ||
| Sex (M vs. F) → Death | 0.91 (0.65, 1.27) | 0.57 |
| Sex (M vs. F) → MAX CRP (>10 mg/dL) | 1.44 (1.07, 1.94) | 0.015 |
| Sex (M vs. F) × MAX CRP (>10 mg/dL) → Death | 1.21 (0.48, 3.02) | 0.67 |
| Sex (M vs. F) × Age (≥60 years old) → Death | 0.60 (0.20, 1.55) | 0.32 |
| BMI | ||
| BMI (≥25 kg/m2) → Death | 0.81 (0.57, 1.14) | 0.22 |
| BMI (≥25 kg/m2) → MAX CRP (>10 mg/dL) | 1.65 (1.21, 2.24) | 0.0014 |
| BMI (≥25 kg/m2) × MAX CRP (> 10 mg/dL) → Death | 1.03 (0.41, 2.59) | 0.95 |
| BMI (≥25 kg/m2) × Age (≥60 years old) → Death | 0.16 (0.02, 0.59) | 0.017 |
| Among Age < 60 years old: BMI (≥25 kg/m2) → Death | 4.99 (1.46, 31.27) | 0.030 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avihai, B.; Sundel, E.P.; Lee, E.; Greenberg, P.J.; Cook, B.P.; Altomare, N.J.; Ko, T.M.; Chaia, A.I.; Parikh, P.D.; Blaser, M.J. CRP Monitoring in Early Hospitalization: Implications for Predicting Outcomes in Patients with COVID-19. Pathogens 2023, 12, 1315. https://doi.org/10.3390/pathogens12111315
Avihai B, Sundel EP, Lee E, Greenberg PJ, Cook BP, Altomare NJ, Ko TM, Chaia AI, Parikh PD, Blaser MJ. CRP Monitoring in Early Hospitalization: Implications for Predicting Outcomes in Patients with COVID-19. Pathogens. 2023; 12(11):1315. https://doi.org/10.3390/pathogens12111315
Chicago/Turabian StyleAvihai, Byron, Erin P. Sundel, Eileen Lee, Patricia J. Greenberg, Brennan P. Cook, Nicole J. Altomare, Tomohiro M. Ko, Angelo I. Chaia, Payal D. Parikh, and Martin J. Blaser. 2023. "CRP Monitoring in Early Hospitalization: Implications for Predicting Outcomes in Patients with COVID-19" Pathogens 12, no. 11: 1315. https://doi.org/10.3390/pathogens12111315
APA StyleAvihai, B., Sundel, E. P., Lee, E., Greenberg, P. J., Cook, B. P., Altomare, N. J., Ko, T. M., Chaia, A. I., Parikh, P. D., & Blaser, M. J. (2023). CRP Monitoring in Early Hospitalization: Implications for Predicting Outcomes in Patients with COVID-19. Pathogens, 12(11), 1315. https://doi.org/10.3390/pathogens12111315