
Incidence, Persistence, and Clearance of Anal Human Papillomavirus among Men Who Have Sex with Men in China: An Observational Cohort Study

 ,
,
Abstract
1. Introduction
2. Results
2.1. Population Characteristics
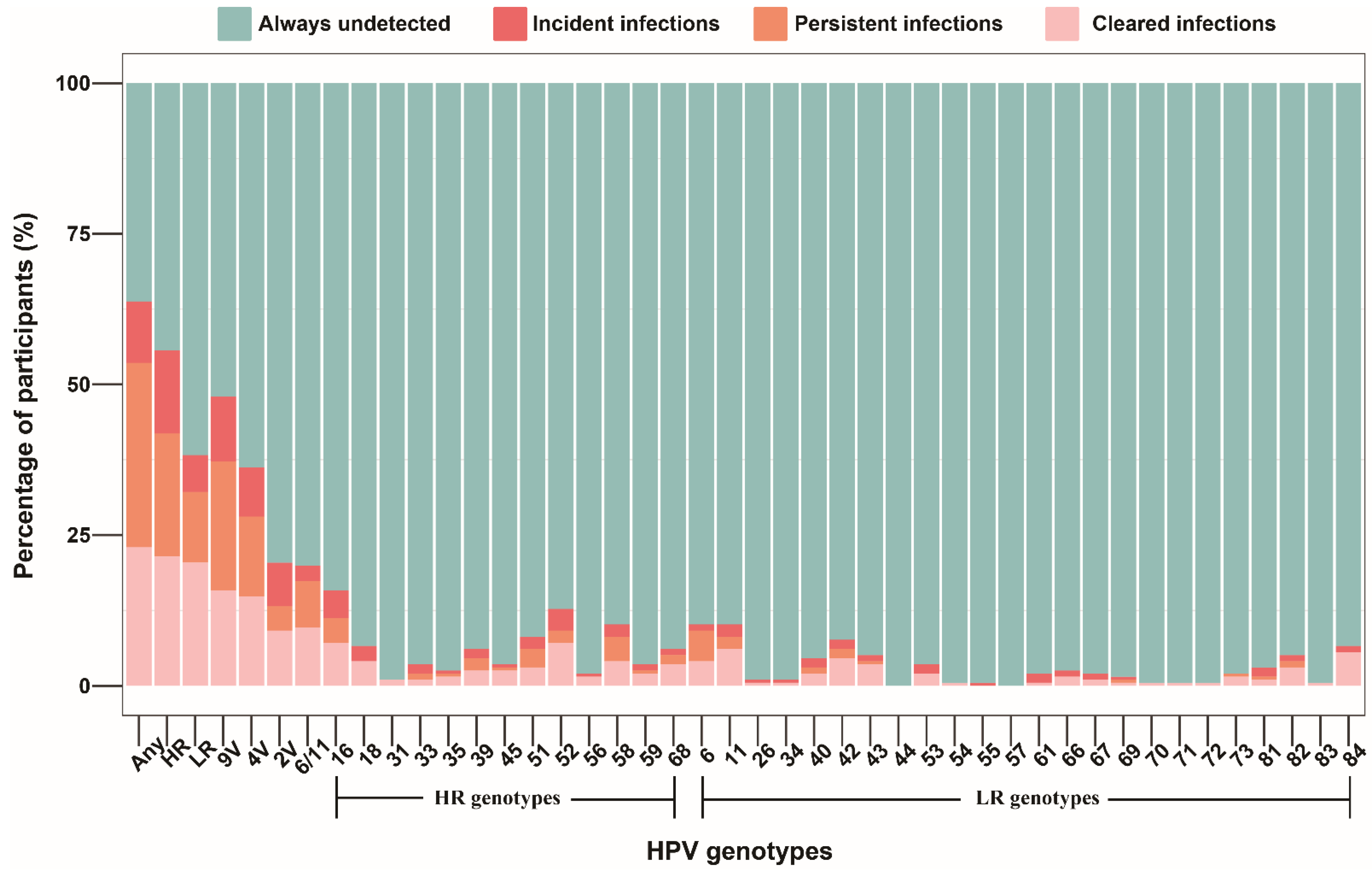
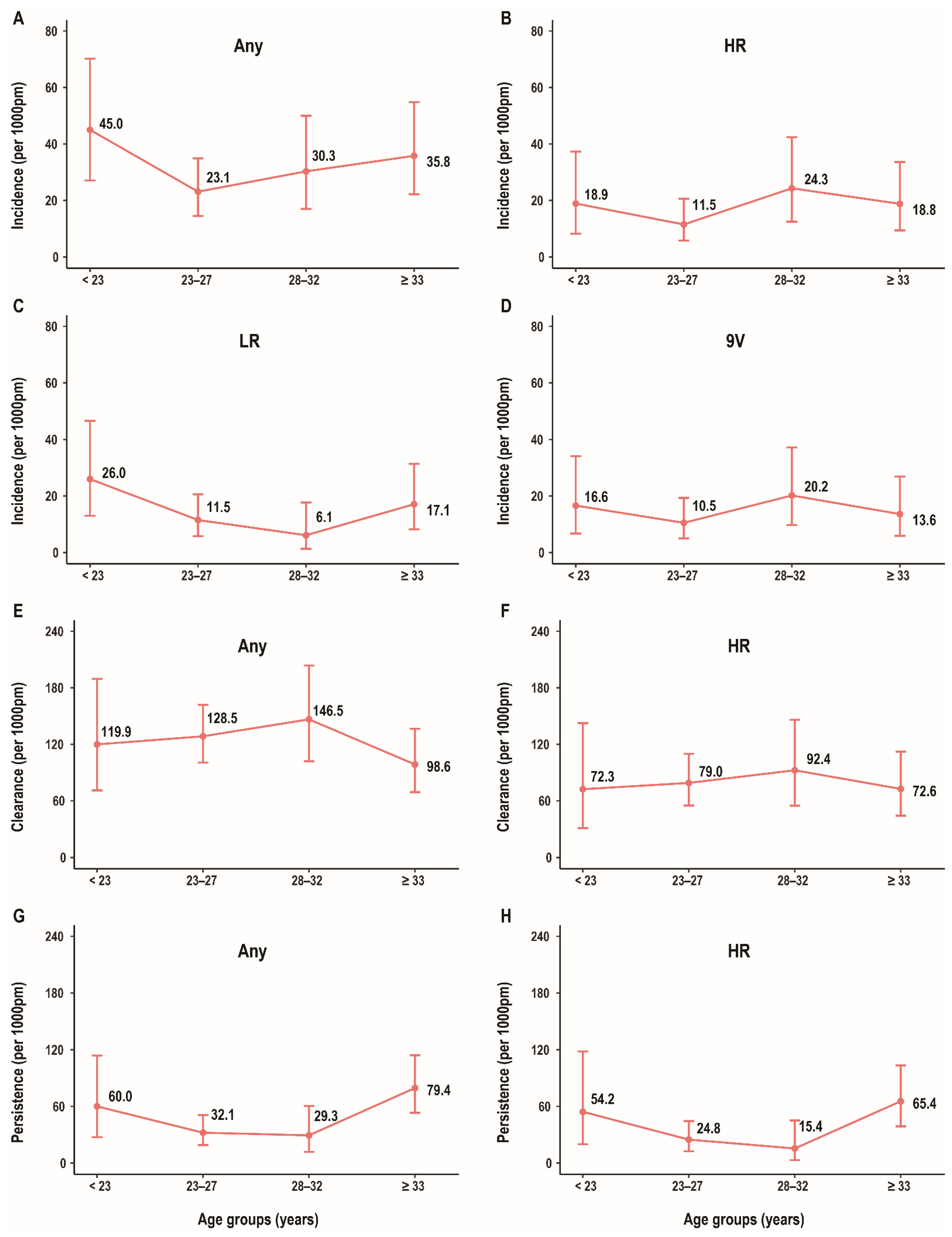
2.2. Incidence, Clearance, and Persistence of Anal HPV among MSM
2.3. Factors Associated with Anal HPV Incidence and Clearance among MSM
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Data and Specimen Collection
4.3. HPV Detection and Genotyping
4.4. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jin, F.; Vajdic, C.M.; Law, M.; Amin, J.; van Leeuwen, M.; McGregor, S.; Poynten, I.M.; Templeton, D.J.; Grulich, A.E. Incidence and time trends of anal cancer among people living with HIV in Australia. AIDS 2019, 33, 1361–1368. [Google Scholar] [CrossRef] [PubMed]
- Heer, E.; Hackl, M.; Ferlitsch, M.; Waldhoer, T.; Yang, L. Trends in incidence of anal cancer in Austria, 1983–2016. Wiener Klinische Wochenschrift 2020, 132, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Shiels, M.S.; Kreimer, A.R.; Coghill, A.E.; Darragh, T.M.; Devesa, S.S. Anal Cancer Incidence in the United States, 1977–2011: Distinct Patterns by Histology and Behavior. Cancer Epidemiol. Prev. Biomark. 2015, 24, 1548–1556. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, A.; Munk, C.; Kjaer, S.K. Trends in incidence of anal cancer and high-grade anal intraepithelial neoplasia in Denmark, 1978–2008. Int. J. Cancer 2012, 130, 1168–1173. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, J.R.; Morris, E.J.A.; Downing, A.; Finan, P.J.; Aravani, A.; Thomas, J.D.; Sebag-Montefiore, D. The rising incidence of anal cancer in England 1990–2010: A population-based study. Colorectal Dis. 2014, 16, O234–O239. [Google Scholar] [CrossRef]
- Guren, M.G.; Aagnes, B.; Nygård, M.; Dahl, O.; Møller, B. Rising Incidence and Improved Survival of Anal Squamous Cell Carcinoma in Norway, 1987–2016. Clin. Colorectal Cancer 2019, 18, e96–e103. [Google Scholar] [CrossRef]
- Lin, C.; Franceschi, S.; Clifford, G.M. Human papillomavirus types from infection to cancer in the anus, according to sex and HIV status: A systematic review and meta-analysis. Lancet Infect. Dis. 2018, 18, 198–206. [Google Scholar] [CrossRef]
- Saunders, C.L.; Meads, C.; Abel, G.A.; Lyratzopoulos, G. Associations Between Sexual Orientation and Overall and Site-Specific Diagnosis of Cancer: Evidence From Two National Patient Surveys in England. J. Clin. Oncol. 2017, 35, 3654–3661. [Google Scholar] [CrossRef]
- Frisch, M.; Biggar, I.J.; Goedert, J.J. Human papillomavirus-associated cancers in patients with human immunodeficiency virus infection and acquired immunodeficiency syndrome. J. Natl. Cancer Inst. 2000, 92, 1500–1510. [Google Scholar] [CrossRef]
- Looker, K.J.; Rönn, M.M.; Brock, P.M.; Brisson, M.; Drolet, M.; Mayaud, P.; Boily, M.C. Evidence of synergistic relationships between HIV and Human Papillomavirus (HPV): Systematic reviews and meta-analyses of longitudinal studies of HPV acquisition and clearance by HIV status, and of HIV acquisition by HPV status. J. Int. AIDS Soc. 2018, 21, e25110. [Google Scholar] [CrossRef]
- Mooij, S.H.; van Santen, D.K.; Geskus, R.B.; van der Sande, M.A.B.; Coutinho, R.A.; Stolte, I.G.; Snijders, P.J.F.; Meijer, C.J.L.M.; Speksnijder, A.G.C.L.; de Vries, H.J.C.; et al. The effect of HIV infection on anal and penile human papillomavirus incidence and clearance: A cohort study among MSM. AIDS 2016, 30, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.M.; Georges, D.; Shiels, M.S.; Engels, E.A.; Albuquerque, A.; Poynten, I.M.; de Pokomandy, A.; Easson, A.M.; Stier, E.A. A meta-analysis of anal cancer incidence by risk group: Toward a unified anal cancer risk scale. Int. J. Cancer 2021, 148, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Marra, E.; Lin, C.; Clifford, G.M. Type-Specific Anal Human Papillomavirus Prevalence Among Men, According to Sexual Preference and HIV Status: A Systematic Literature Review and Meta-Analysis. J. Infect. Dis. 2019, 219, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Wang, Q.; Ong, J.J.; Fairley, C.K.; Su, S.; Peng, P.; Jing, J.; Wang, L.; Soe, N.N.; Cheng, F.; et al. Prevalence of human papillomavirus by geographical regions, sexual orientation and HIV status in China: A systematic review and meta-analysis. Sex Transm. Infect. 2018, 94, 434–442. [Google Scholar] [CrossRef]
- Palefsky, J.M.; Giuliano, A.R.; Goldstone, S.; Moreira, E.D.; Aranda, C.; Jessen, H.; Hillman, R.; Ferris, D.; Coutlee, F.; Stoler, M.H.; et al. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. N. Engl. J. Med. 2011, 365, 1576–1585. [Google Scholar] [CrossRef]
- Petrosky, E.; Bocchini, J.A., Jr.; Hariri, S.; Chesson, H.; Curtis, C.R.; Saraiya, M.; Unger, E.R.; Markowitz, L.E. Use of 9-valent human papillomavirus (HPV) vaccine: Updated HPV vaccination recommendations of the advisory committee on immunization practices. MMWR Morb. Mortal Wkly. Rep. 2015, 64, 300–304. [Google Scholar]
- Petit, B.; Epaulard, O. Men having sex with men and the HPV vaccine in France: A low vaccine coverage that may be due to its infrequent proposal by physicians. Vaccine 2020, 38, 2160–2165. [Google Scholar] [CrossRef]
- Edelstein, M.; Iyanger, N.; Hennessy, N.; Mesher, D.; Checchi, M.; Soldan, K.; McCall, M.; Nugent, J.; Crofts, J.; Lo, J.; et al. Implementation and evaluation of the human papillomavirus (HPV) vaccination pilot for men who have sex with men (MSM), England, April 2016 to March 2017. Eurosurveillance 2019, 24, 44–50. [Google Scholar] [CrossRef]
- Chow, E.P.F.; Machalek, D.A.; Tabrizi, S.N.; Danielewski, J.A.; Fehler, G.; Bradshaw, C.S.; Garland, S.M.; Chen, M.Y.; Fairley, C.K. Quadrivalent vaccine-targeted human papillomavirus genotypes in heterosexual men after the Australian female human papillomavirus vaccination programme: A retrospective observational study. Lancet Infect. Dis. 2017, 17, 68–77. [Google Scholar] [CrossRef]
- Geskus, R.B.; González, C.; Torres, M.; Del Romero, J.; Viciana, P.; Masiá, M.; Blanco, J.R.; Iribarren, M.; De Sanjosé, S.; Hernández-Novoa, B.; et al. Incidence and clearance of anal high-risk human papillomavirus in HIV-positive men who have sex with men: Estimates and risk factors. AIDS 2016, 30, 37–44. [Google Scholar] [CrossRef]
- Hernandez, A.L.; Efird, J.T.; Holly, E.A.; Berry, J.M.; Jay, N.; Palefsky, J.M. Incidence of and risk factors for type-specific anal human papillomavirus infection among HIV-positive MSM. AIDS 2014, 28, 1341–1349. [Google Scholar] [CrossRef] [PubMed]
- Zou, H.; Tabrizi, S.N.; Grulich, A.E.; Garland, S.M.; Hocking, J.S.; Bradshaw, C.S.; Morrow, A.; Prestage, G.; Cornall, A.M.; Fairley, C.K.; et al. Early acquisition of anogenital human papillomavirus among teenage men who have sex with men. J. Infect. Dis. 2014, 209, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Yunihastuti, E.; Teeratakulpisarn, N.; Jeo, W.S.; Nilasari, H.; Rachmadi, L.; Somia, I.K.A.; Sukmawati, M.D.D.; Amijaya, K.A.T.; Yee, I.A.; Hairunisa, N.; et al. Incidence, clearance, persistence and factors related with high-risk anal HPV persistence in South-East Asian MSM and transgender women. AIDS 2020, 34, 1933–1941. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.J.; Walker, S.; Grulich, A.; Hoy, J.; Read, T.R.; Bradshaw, C.; Chen, M.; Garland, S.M.; Cornall, A.; Hillman, R. Incidence, clearance, and persistence of anal human papillomavirus in men who have sex with men living with human immunodeficiency virus: Implications for human papillomavirus vaccination. Sex. Transm. Dis. 2019, 46, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Donà, M.G.; Vescio, M.F.; Latini, A.; Giglio, A.; Moretto, D.; Frasca, M.; Benevolo, M.; Rollo, F.; Colafigli, M.; Cristaudo, A.; et al. Anal human papillomavirus in HIV-uninfected men who have sex with men: Incidence and clearance rates, duration of infection, and risk factors. Clin. Microbiol. Infect. 2016, 22, 1004.e1–1004.e7. [Google Scholar] [CrossRef]
- Cotte, L.; Veyer, D.; Charreau, I.; Péré, H.; Cua, E.; Carette, D.; Chas, J.; Capitant, C.; Chidiac, C.; Fléjou, J.F.; et al. Prevalence and incidence of HPV infection in men having sex with men enrolled in a PrEP study: A sub-study of the ANRS IPERGAY trial. Clin. Infect Dis. 2020. [Google Scholar] [CrossRef]
- Zhou, Y.; Lin, Y.-F.; Meng, X.; Duan, Q.; Wang, Z.; Yang, B.; Zheng, H.; Li, P.; Li, M.; Lu, Y.; et al. Anal human papillomavirus among men who have sex with men in three metropolitan cities in southern China: Implications for HPV vaccination. Vaccine 2020, 38, 2849–2858. [Google Scholar] [CrossRef]
- Wei, F.; Guo, M.; Huang, S.; Li, M.; Cui, X.; Su, Y.; Wu, X.; Ma, X.; Zheng, Y.; Huang, Y.; et al. Sex Differences in the Incidence and Clearance of Anogenital Human Papillomavirus Infection in Liuzhou, China: An Observational Cohort Study. Clin. Infect. Dis. 2020, 70, 82–89. [Google Scholar] [CrossRef]
- Zhang, C.; Liu, F.; Pan, Y.; Deng, Q.; Li, X.; He, Z.; Liu, M.; Ning, T.; Guo, C.; Liang, Y.; et al. Incidence and clearance of oral human papillomavirus infection: A population-based cohort study in rural China. Oncotarget 2017, 8, 59831–59844. [Google Scholar] [CrossRef][Green Version]
- Marra, E.; Kovaleva, A.; Bruisten, S.M.; Vermeulen, W.; Boyd, A.; Schim van der Loeff, M.F. Incidence and Clearance of Anal High-risk Human Papillomavirus Infections and Their Determinants Over 5 Years Among Human Immunodeficiency Virus-negative Men Who Have Sex With Men. Clin. Infect. Dis. 2019, 68, 1556–1565. [Google Scholar] [CrossRef]
- Alberts, C.J.; Heard, I.; Canestri, A.; Marchand, L.; Fléjou, J.-F.; Piroth, L.; Ferry, T.; Didelot, J.-M.; Siproudhis, L.; Henno, S.; et al. Incidence and Clearance of Anal Human Papillomavirus (HPV)-16 and HPV-18 Infection, and Their Determinants, Among Human Immunodeficiency Virus-Infected Men Who Have Sex With Men in France. J. Infect. Dis. 2020, 221, 1488–1493. [Google Scholar] [CrossRef] [PubMed]
- Phanuphak, N.; Teeratakulpisarn, N.; Pankam, T.; Kerr, S.J.; Barisri, J.; Deesua, A.; Rodbamrung, P.; Hongchookiat, P.; Chomchey, N.; Phanuphak, P. Anal human papillomavirus infection among Thai men who have sex with men with and without HIV infection: Prevalence, incidence, and persistence. J. Acquir. Immune Defic. Syndr. 2013, 63, 472. [Google Scholar] [CrossRef]
- Wei, F.; Su, Y.; Yao, X.; Cui, X.; Bian, L.; Yin, K.; Yu, X.; Zhuang, C.; Bi, Z.; Huang, S.; et al. Sex differences in the incidence and clearance of anal human papillomavirus infection among heterosexual men and women in Liuzhou, China: An observational cohort study. Int. J. Cancer 2019, 145, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Lin, Y.-F.; Gao, L.; Dai, J.; Luo, G.; Li, L.; Yuan, T.; Li, P.; Zhan, Y.; Gao, Y.; et al. Human papillomavirus prevalence among men who have sex with men in China: A systematic review and meta-analysis. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1357–1367. [Google Scholar] [CrossRef] [PubMed]
- Nyitray, A.G.; Carvalho da Silva, R.J.; Baggio, M.L.; Smith, D.E.; Abrahamsen, M.; Papenfuss, M.; Lin, H.-Y.; Quiterio, M.; Salmerón, J.; Lazcano-Ponce, E.; et al. Six-month incidence, persistence, and factors associated with persistence of anal human papillomavirus in men: The HPV in men study. J. Infect. Dis. 2011, 204, 1711–1722. [Google Scholar] [CrossRef] [PubMed]
- Zou, H.; Xu, J.; Hu, Q.; Yu, Y.; Fu, G.; Wang, Z.; Lu, L.; Zhuang, M.; Chen, X.; Fu, J.; et al. Decreasing age at first anal intercourse among men who have sex with men in China: A multicentre cross-sectional survey. J. Int. AIDS Soc. 2016, 19, 20792. [Google Scholar] [CrossRef]
- Zou, H.; Meng, X.; Grulich, A.; Huang, S.; Jia, T.; Zhang, X.; Luo, Z.; Ding, Y.; Yang, L.; Huang, J.; et al. A randomised controlled trial to evaluate the impact of sexual health clinic based automated text message reminders on testing of HIV and other sexually transmitted infections in men who have sex with men in China: Protocol for the T2T Study. BMJ Open 2017, 7, e015787. [Google Scholar] [CrossRef]
- World Health Organization. Human Papillomaviruses. Available online: https://monographs.iarc.who.int/wp-content/uploads/2018/06/mono100B-11.pdf (accessed on 9 January 2022).



{kind=link}
{kind=link}
| HPV Genotypes | Incident Infections | Person Months | Incidence/1000 Person Months (95% CI) | Persistent Infections | Person Months | Persistence/1000 Person Months (95% CI) | Cleared Infections | Person Months | Clearance/1000 Person Months (95% CI) |
|---|---|---|---|---|---|---|---|---|---|
| Any genotype a | 77 | 2457 | 31.3 (24.7–39.2) | 63 | 1314 | 47.9 (36.8–61.3) | 161 | 1314 | 122.5 (104.3–143.0) |
| HR genotypes | |||||||||
| Any HR genotype | 42 | 2457 | 17.1 (12.3–23.1) | 38 | 922 | 41.2 (29.2–56.6) | 81 | 922 | 87.9 (69.8–109.2) |
| HPV 16 | 9 | 2187 | 4.1 (1.9–7.8) | 8 | 271 | 29.5 (12.7–58.2) | 14 | 271 | 51.7 (28.2–86.7) |
| HPV 18 | 5 | 2353 | 2.1 (0.7–5.0) | 0 | 104 | 0.0 (0.0–35.5) | 8 | 104 | 76.9 (33.2–151.6) |
| HPV 31 | 0 | 2434 | 0.0 (0.0–1.5) | 0 | 23 | 0.0 (0.0–160.4) | 2 | 23 | 87.0 (10.5–314.1) |
| HPV 33 | 3 | 2409 | 1.2 (0.3–3.6) | 2 | 48 | 41.7 (5.0–150.5) | 2 | 48 | 41.7 (5.0–150.5) |
| HPV 35 | 1 | 2409 | 0.4 (0.0–2.3) | 1 | 48 | 20.8 (0.5–116.1) | 3 | 48 | 62.5 (12.9–182.7) |
| HPV 39 | 3 | 2364 | 1.3 (0.3–3.7) | 4 | 93 | 43.0 (11.7–110.1) | 5 | 93 | 53.8 (17.5–125.5) |
| HPV 45 | 1 | 2380 | 0.4 (0.0–2.3) | 1 | 77 | 13.0 (0.3–72.4) | 5 | 77 | 64.9 (21.1–151.5) |
| HPV 51 | 4 | 2296 | 1.7 (0.5–4.5) | 6 | 161 | 37.3 (13.7–81.1) | 6 | 161 | 37.3 (13.7–81.1) |
| HPV 52 | 7 | 2223 | 3.1 (1.3–6.5) | 4 | 234 | 17.1 (4.7–43.8) | 14 | 234 | 59.8 (32.7–100.4) |
| HPV 56 | 1 | 2417 | 0.4 (0.0–2.3) | 0 | 40 | 0.0 (0.0–92.2) | 3 | 40 | 75.0 (15.5–219.2) |
| HPV 58 | 4 | 2271 | 1.8 (0.5–4.5) | 8 | 186 | 43.0 (18.6–84.7) | 8 | 186 | 43.0 (18.6–84.7) |
| HPV 59 | 2 | 2382 | 0.8 (0.1–3.0) | 1 | 76 | 13.2 (0.3–73.3) | 4 | 76 | 52.6 (14.3–134.8) |
| HPV 68 | 2 | 2339 | 0.9 (0.1–3.1) | 3 | 118 | 25.4 (5.2–74.3) | 7 | 118 | 59.3 (23.9–122.2) |
| LR genotypes | |||||||||
| Any LR genotype | 35 | 2457 | 14.2 (9.9–19.8) | 25 | 902 | 27.7 (17.9–40.9) | 80 | 902 | 88.7 (70.3–110.4) |
| HPV 6 | 2 | 2246 | 0.9 (0.1–3.2) | 10 | 211 | 47.4 (22.7–87.2) | 8 | 211 | 37.9 (16.4–74.7) |
| HPV 11 | 4 | 2239 | 1.8 (0.5–4.6) | 4 | 218 | 18.3 (5.0–47.0) | 12 | 218 | 55.0 (28.4–96.2) |
| HPV 26 | 1 | 2447 | 0.4 (0.0–2.3) | 0 | 11 | 0.0 (0.0–335.4) | 1 | 11 | 90.9 (2.3–506.5) |
| HPV 34 | 1 | 2443 | 0.4 (0.0–2.3) | 0 | 14 | 0.0 (0.0–263.5) | 1 | 14 | 71.4 (1.8–398.0) |
| HPV 40 | 3 | 2375 | 1.3 (0.3–3.7) | 2 | 82 | 24.4 (3.0–88.1) | 4 | 82 | 48.8 (13.3–124.9) |
| HPV 42 | 3 | 2339 | 1.3 (0.3–3.7) | 3 | 118 | 25.4 (5.2–74.3) | 9 | 118 | 76.3 (34.9–144.8) |
| HPV 43 | 2 | 2356 | 0.8 (0.1–3.1) | 1 | 101 | 9.9 (0.3–55.2) | 7 | 101 | 69.3 (27.9–142.8) |
| HPV 44 | 0 | 2457 | 0.0 (0.0–1.5) | 0 | 0 | NA | 0 | 0 | NA |
| HPV 53 | 3 | 2405 | 1.2 (0.3–3.6) | 0 | 53 | 0.0 (0.0–69.6) | 4 | 53 | 75.5 (20.6–193.2) |
| HPV 54 | 0 | 2446 | 0.0 (0.0–1.5) | 0 | 11 | 0.0 (0.0–335.4) | 1 | 11 | 90.9 (2.3–506.5) |
| HPV 55 | 1 | 2457 | 0.4 (0.0–2.3) | 0 | 0 | NA | 0 | 0 | NA |
| HPV 57 | 0 | 2457 | 0.0 (0.0–1.5) | 0 | 0 | NA | 0 | 0 | NA |
| HPV 61 | 3 | 2444 | 1.2 (0.3–3.6) | 0 | 13 | 0.0 (0.0–283.8) | 1 | 13 | 76.9 (1.9–428.6) |
| HPV 66 | 2 | 2424 | 0.8 (0.1–3.0) | 0 | 34 | 0.0 (0.0–108.5) | 3 | 34 | 88.2 (18.2–257.9) |
| HPV 67 | 2 | 2435 | 0.8 (0.1–3.0) | 0 | 22 | 0.0 (0.0–167.7) | 2 | 22 | 90.9 (11.0–328.4) |
| HPV 69 | 1 | 2428 | 0.4 (0.0–2.3) | 1 | 29 | 34.5 (0.9–192.1) | 1 | 29 | 34.5 (0.9–192.1) |
| HPV 70 | 0 | 2443 | 0.0 (0.0–1.5) | 0 | 14 | 0.0 (0.0–263.5) | 1 | 14 | 71.4 (1.8–398.0) |
| HPV 71 | 0 | 2443 | 0.0 (0.0–1.5) | 0 | 14 | 0.0 (0.0–263.5) | 1 | 14 | 71.4 (1.8–398.0) |
| HPV 72 | 0 | 2443 | 0.0 (0.0–1.5) | 0 | 15 | 0.0 (0.0–245.9) | 1 | 15 | 66.7 (1.7–371.4) |
| HPV 73 | 0 | 2421 | 0.0 (0.0–1.5) | 1 | 36 | 27.8 (0.7–154.8) | 3 | 36 | 83.3 (17.2–243.5) |
| HPV 81 | 3 | 2429 | 1.2 (0.3–3.6) | 1 | 28 | 35.7 (0.9–199.0) | 2 | 28 | 71.4 (8.7–258.0) |
| HPV 82 | 2 | 2348 | 0.9 (0.1–3.1) | 2 | 110 | 18.2 (2.2–65.7) | 6 | 110 | 54.5 (20.0–118.7) |
| HPV 83 | 0 | 2445 | 0.0 (0.0–1.5) | 0 | 12 | 0.0 (0.0–307.4) | 1 | 12 | 83.3 (2.1–464.3) |
| HPV 84 | 2 | 2318 | 0.9 (0.1–3.1) | 0 | 139 | 0.0 (0.0–26.5) | 11 | 139 | 79.1 (39.5–141.6) |
| Vaccine-preventable genotypes | |||||||||
| 9V genotypes b | 35 | 2457 | 14.2 (9.9–19.8) | 37 | 902 | 41.0 (28.9–56.5) | 73 | 902 | 80.9 (63.4–101.8) |
| 4V genotypes c | 20 | 2457 | 8.1 (5.0–12.6) | 22 | 687 | 32.0 (20.1–48.5) | 42 | 687 | 61.1 (44.1–82.6) |
| 2V genotypes d | 14 | 2408 | 5.8 (3.2–9.8) | 8 | 325 | 24.6 (10.6–48.5) | 22 | 325 | 67.7 (42.4–102.5) |
| HPV 6/11 | 6 | 2457 | 2.4 (0.9–5.3) | 14 | 429 | 32.6 (17.8–54.8) | 20 | 429 | 46.6 (28.5–72.0) |
| Factors | Incidence (N = 196) | Clearance (N = 105) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n a | % b | Crude | Adjusted | n a | % b | Crude | Adjusted | |||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |||||
| Age at recruitment (years) | ||||||||||||
| <23 | 14 | 41.2 | Ref. | Ref. | Ref. | Ref. | 12 | 92.3 | Ref. | Ref. | Ref. | Ref. |
| 23–27 | 15 | 20.8 | 0.45 (0.22–0.92) | 0.028 | 0.52 (0.24–1.12) | 0.095 | 38 | 90.5 | 0.96 (0.68–1.36) | 0.833 | 1.01 (0.53–1.92) | 0.977 |
| 28–32 | 9 | 21.4 | 0.46 (0.20–1.06) | 0.067 | 0.74 (0.28–1.94) | 0.543 | 18 | 94.7 | 1.05 (0.74–1.50) | 0.788 | 1.06 (0.56–2.02) | 0.858 |
| ≥33 | 17 | 35.4 | 0.83 (0.42–1.65) | 0.596 | 0.69 (0.26–1.81) | 0.453 | 20 | 64.5 | 0.56 (0.34–0.90) | 0.018 | 0.45 (0.23–0.91) | 0.026 |
| Site of enrollment | ||||||||||||
| Guangzhou | 32 | 30.5 | Ref. | Ref. | 45 | 76.3 | Ref. | Ref. | Ref. | Ref. | ||
| Wuxi | 8 | 27.6 | 0.89 (0.41–1.91) | 0.766 | 18 | 94.7 | 1.46 (1.07–1.99) | 0.016 | 1.67 (1.04–2.68) | 0.034 | ||
| Shenzhen | 15 | 24.2 | 0.77 (0.42–1.41) | 0.389 | 25 | 92.6 | 1.40 (1.03–1.90) | 0.031 | 1.27 (0.92–1.74) | 0.142 | ||
| Marriage | ||||||||||||
| Unmarried | 44 | 27.9 | Ref. | Ref. | Ref. | Ref. | 70 | 86.4 | Ref. | Ref. | Ref. | Ref. |
| In marriage/cohabitation or engagement with female | 10 | 35.7 | 1.34 (0.69–2.64) | 0.390 | 1.25 (0.62–2.53) | 0.527 | 13 | 68.4 | 0.68 (0.42–1.12) | 0.129 | 0.98 (0.53–1.80) | 0.937 |
| Educational level | ||||||||||||
| High school and below | 23 | 44.2 | Ref. | Ref. | Ref. | Ref. | 23 | 79.3 | Ref. | Ref. | ||
| University and above | 32 | 22.2 | 0.44 (0.26–0.74) | 0.002 | 0.36 (0.20–0.64) | 0.001 | 65 | 85.5 | 1.14 (0.80–1.61) | 0.472 | ||
| Salary (yuan/month) | ||||||||||||
| <5000 | 26 | 30.2 | Ref. | Ref. | 40 | 81.6 | Ref. | Ref. | ||||
| ≥5000 | 29 | 26.4 | 0.85 (0.51–1.44) | 0.550 | 48 | 85.7 | 1.09 (0.81–1.46) | 0.575 | ||||
| Profession | ||||||||||||
| White collar worker | 22 | 22.5 | Ref. | Ref. | Ref. | Ref. | 41 | 83.7 | Ref. | Ref. | Ref. | Ref. |
| Service industry/worker | 10 | 27.0 | 1.24 (0.59–2.59) | 0.576 | 0.77 (0.34–1.76) | 0.535 | 20 | 87.0 | 1.07 (0.75–1.52) | 0.710 | 1.37 (0.92–2.03) | 0.124 |
| Unemployed/self-employed | 8 | 53.3 | 2.88 (1.33–6.21) | 0.007 | 2.31 (0.96–5.55) | 0.061 | 4 | 57.1 | 0.56 (0.22–1.41) | 0.215 | 0.92 (0.32–2.63) | 0.871 |
| Teacher/institution staff | 3 | 25.0 | 1.13 (0.34–3.74) | 0.842 | 1.57 (0.43–5.81) | 0.497 | 6 | 100.0 | 1.39 (1.12–1.72) | 0.003 | 2.20 (1.30–3.72) | 0.003 |
| Student | 7 | 33.3 | 1.58 (0.68–3.66) | 0.283 | 1.61 (0.68–3.82) | 0.282 | 10 | 90.9 | 1.16 (0.77–1.74) | 0.477 | 1.01 (0.55–1.86) | 0.981 |
| Other | 5 | 38.5 | 1.88 (0.73–4.87) | 0.191 | 2.02 (0.83–4.92) | 0.121 | 7 | 77.8 | 0.88 (0.48–1.63) | 0.695 | 1.34 (0.74–2.44) | 0.337 |
| No. of sexual partners during follow-up | ||||||||||||
| <6 | 30 | 31.6 | Ref. | Ref. | Ref. | Ref. | 41 | 78.9 | Ref. | Ref. | Ref. | Ref. |
| ≥6 | 23 | 29.1 | 0.91 (0.53–1.55) | 0.726 | 0.94 (0.55–1.64) | 0.839 | 36 | 87.8 | 1.20 (0.88–1.64) | 0.244 | 1.12 (0.81–1.55) | 0.481 |
| Time since first anal sex (years) | ||||||||||||
| <5 | 26 | 28.9 | Ref. | Ref. | Ref. | Ref. | 33 | 89.2 | Ref. | Ref. | Ref. | Ref. |
| ≥5 | 29 | 27.4 | 0.94 (0.56–1.58) | 0.813 | 1.33 (0.67–2.62) | 0.416 | 55 | 80.9 | 0.84 (0.64–1.12) | 0.237 | 1.07 (0.78–1.48) | 0.673 |
| Role in anal sex with males | ||||||||||||
| Insertive c | 15 | 26.3 | Ref. | Ref. | Ref. | Ref. | 20 | 76.9 | Ref. | Ref. | Ref. | Ref. |
| Receptive d | 31 | 31.3 | 1.23 (0.67–2.25) | 0.514 | 2.12 (1.10–4.09) | 0.024 | 50 | 87.7 | 1.25 (0.85–1.84) | 0.256 | 1.25 (0.71–2.19) | 0.438 |
| Receptive and insertive | 9 | 22.5 | 0.84 (0.37–1.90) | 0.670 | 1.37 (0.58–3.23) | 0.473 | 18 | 81.8 | 1.11 (0.69–1.79) | 0.676 | 1.04 (0.56–1.93) | 0.902 |
| HIV status | ||||||||||||
| Negative | 50 | 27.5 | Ref. | Ref. | Ref. | Ref. | 77 | 82.8 | Ref. | Ref. | Ref. | Ref. |
| Positive | 5 | 35.7 | 1.37 (0.55–3.36) | 0.498 | 0.85 (0.28–2.60) | 0.620 | 11 | 91.7 | 1.20 (0.84–1.71) | 0.318 | 0.92 (0.60–1.41) | 0.692 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, Y.; Zhou, X.; Lin, Y.-F.; Luo, G.; Lu, Y.; Wang, Z.; Li, P.; Luo, Z.; Meng, X.; Tian, T.; et al. Incidence, Persistence, and Clearance of Anal Human Papillomavirus among Men Who Have Sex with Men in China: An Observational Cohort Study. Pathogens 2022, 11, 314. https://doi.org/10.3390/pathogens11030314
Zhou Y, Zhou X, Lin Y-F, Luo G, Lu Y, Wang Z, Li P, Luo Z, Meng X, Tian T, et al. Incidence, Persistence, and Clearance of Anal Human Papillomavirus among Men Who Have Sex with Men in China: An Observational Cohort Study. Pathogens. 2022; 11(3):314. https://doi.org/10.3390/pathogens11030314
Chicago/Turabian StyleZhou, Yiguo, Xinyi Zhou, Yi-Fan Lin, Ganfeng Luo, Yong Lu, Zhenyu Wang, Peiyang Li, Zhenzhou Luo, Xiaojun Meng, Tian Tian, and et al. 2022. "Incidence, Persistence, and Clearance of Anal Human Papillomavirus among Men Who Have Sex with Men in China: An Observational Cohort Study" Pathogens 11, no. 3: 314. https://doi.org/10.3390/pathogens11030314
APA StyleZhou, Y., Zhou, X., Lin, Y.-F., Luo, G., Lu, Y., Wang, Z., Li, P., Luo, Z., Meng, X., Tian, T., Fu, L., Dai, J., & Zou, H. (2022). Incidence, Persistence, and Clearance of Anal Human Papillomavirus among Men Who Have Sex with Men in China: An Observational Cohort Study. Pathogens, 11(3), 314. https://doi.org/10.3390/pathogens11030314