1. Introduction
Shanghai fever is a rare sepsis-associated enteric disease caused by
P. aeruginosa, described mainly in previously immunologically healthy children. To our knowledge, only one case has been described in the literature in an adult patient with neutropenia. The disease was reported as early as 1918 and has been more recently defined by Chuang et al. with three criteria: (1) community-onset diarrhea with fever, (2) sepsis and (3) growth of
P. aeruginosa from blood or another sterile body site. Necrotizing enteritis is the major complication of Shanghai fever and mortality reported worldwide is high [
1,
2].
To date, most of the reported cases regarding Shanghai fever are restricted to East Asian countries and only very few cases are described to be from North America and Europe.
We report a case of Shanghai fever in a previously healthy Italian 7-month-old boy and analyze the medical literature to report the epidemiologic and clinical characteristics of cases of Shanghai fever from non-Asiatic countries.
2. Methods
This systematic review was performed in accordance with the PRISMA protocol (Reporting Items for Systematic Reviews and Meta-Analyses) and a systematic review registration is currently ongoing at PROSPERO.
A computerized literature search was performed on PubMed and Scopus search engines by submitting the query (Pseudomonas AND (enteritis OR diarrhea OR colitis OR enterocolitis) AND (sepsis OR septicemia OR bacteriemia) AND (children OR child OR baby OR infant)) OR Shanghai fever (title/Abstract). No filters or language restrictions were applied to the results. Furthermore, all references listed were hand-searched for other relevant articles, and a citation tracker was used to identify any other relevant literature. An article was considered eligible for inclusion if reporting cases with full clinical data consistent with Shanghai fever. The following epidemiologic and clinical variables were evaluated for each case: gender, age, clinical manifestations, intestinal involvement, antibiotic therapy, surgical procedures and clinical outcome. Outcome was considered good in patients responding to treatment and not presenting with sequelae.
3. Results
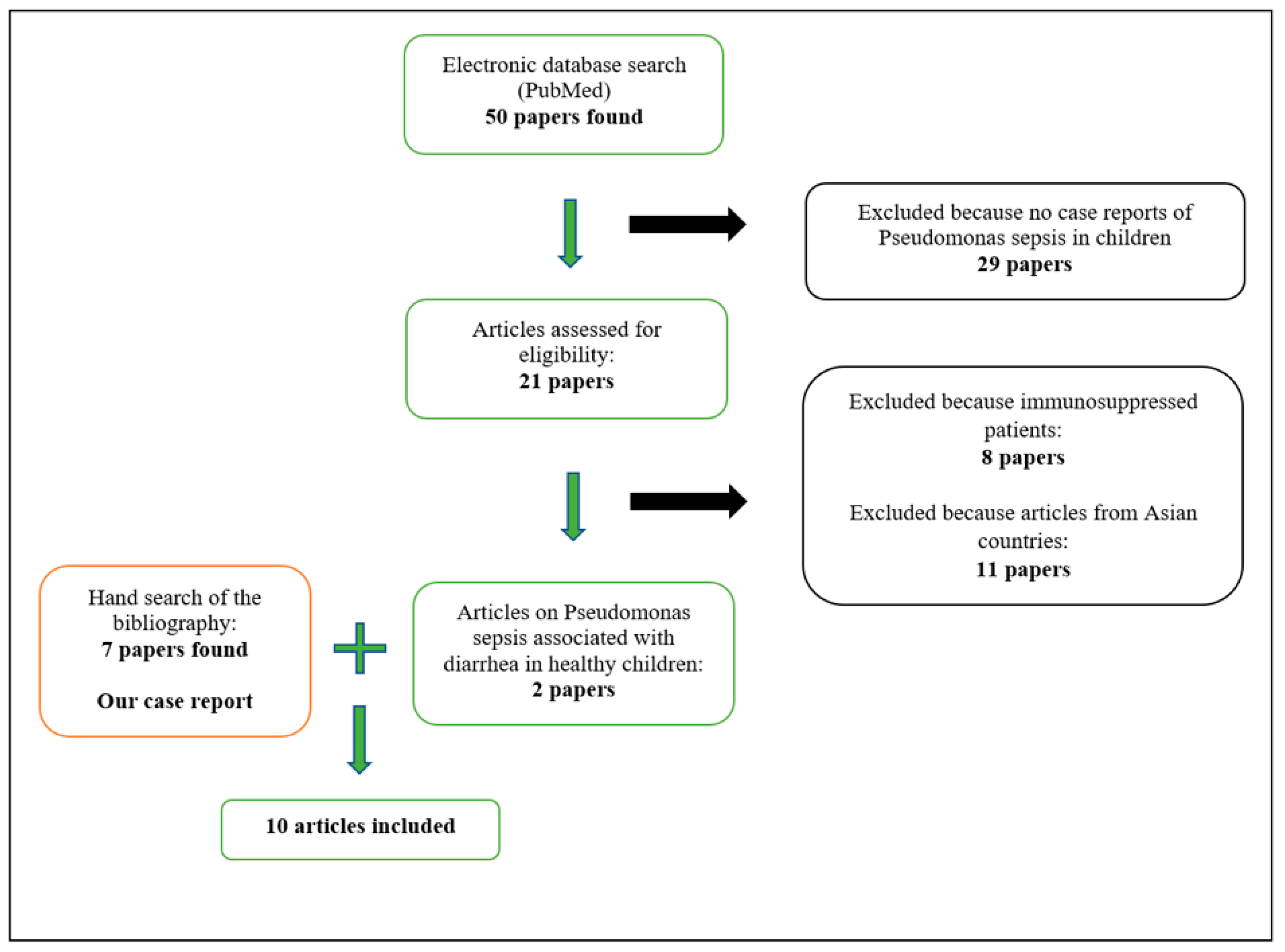
From the literature search carried out we retrieved 50 papers, of which only 2 were eligible [
3,
4]. In particular, we excluded from the analysis eleven papers because they were describing cases related to Asian countries and eight because they involved immunosuppressed patients. Other papers were not relevant. In a manual search of the bibliography, we found seven relevant articles (
Figure 1).
Nine articles, each reporting single cases of Shanghai fever, were eventually included, dating from 1980 to 2022 [
3,
4,
5,
6,
7,
8,
9,
10,
11]. All cases in our review meet the criteria of Shanghai fever [
2]. Our review reports cases from non-Asiatic countries and, in particular, four cases from Europe, four cases from North America, one case from South America and one case from South Africa. The median age of the patients was 7 months and 80% were aged <1 year. The male-to-female ratio was 6:4. The most common clinical manifestations were fever (100%), diarrhea (100%) and ecthyma gangrenosum (90%). All patients with ecthyma gangrenosum had multiple sites affected. One patient had meningitis [
9]. The median time from onset of the first symptom to sepsis was four days (range: three to six days). Three had bowel perforation requiring immediate surgical intervention [
5,
10]. Intraoperative findings showed widespread patchy necrosis with fibrin coating of the small intestine or colon. No patients had short bowel syndrome after surgery.
Leukopenia, thrombocytopenia, high C-reactive protein (CRP) levels, coagulopathy and hypoalbuminemia were the characteristic laboratory findings. Leukopenia and thrombocytopenia were found in six cases (60%), and leukocytosis in 2 cases (20%). Mild to moderate anemia was found in eight cases (80%) described in our review.
Blood was the most common site of isolation for P. aeruginosa (70%). P. aeruginosa was also isolated from skin lesions (60%), stool (50%), peritoneal fluid (30%), tracheal or bronchial secretions (30%), urine samples (20%), oropharyngeal exudate (20%), cerebrospinal fluid (10%) and pleural effusion (10%).
None of the patients received antipseudomonal antibiotics within 24 h of admission. In all cases, antipseudomonal therapy was started after a positive cultures result. Only one patient died due to multiple organ failure from
Pseudomonas sepsis. In this case, the baby was hospitalized on the fifth day of her illness in poor condition (distributive shock and pancolonic necrosis) [
5].
Taken together, no definitive common primary immune deficiency was identified in these patients based upon both laboratory and clinical evaluations. Extremely young age (<1 year) was the only identified host factor predisposing to Shanghai fever.
4. Case Report
A previously healthy 7-month-old male child was admitted with three days of high graded fever, hyporexia and diarrhea associated with perianal erythema. On admission, his body temperature was 37.7 °C, respiratory rate was normal and heart rate was 140 beats/min. An examination revealed pharyngeal hyperemia without exudate, two small erythematosus lesions on the legs initially interpretated as insect bites, de-epithelialization and erythema of the perianal skin. The abdomen was soft and painless and no signs of meningeal irritations could be detected during the inspection. The first laboratory workup revealed leukopenia (white blood cells 2.8 × 10
3/μL, neutrophils 1.38 × 10
3/μL and lymphocyte count 1.2 × 10
3/μL), mild anemia (Hb 10.7 g/dL), platelets 63 × 10
3/μL, high inflammatory markers (CRP 27.3 mg/dL, procalcitonin 70 μg/L), hypoalbuminemia, hyponatremia and hypokalemia. Liver enzymes, renal function tests, prothrombin time and activated thromboplastin time were always normal with a subsequent increase of D-dimer. The suspicion of sepsis led to the decision of performing a blood culture and to start an intravenous antibiotic therapy with Ceftriaxone. On the second day of hospitalization, we observed a worsening of clinical conditions. The patient presented signs of meningeal irritation such as neck stiffness and photophobia, in addition to continuous and mournful crying. He had developed whitish tonsillar exudate, foul-smelling breath and multiple hyperemic and infiltrated skin lesions over the legs and buttocks, which were rapidly becoming ulcerative-necrotizing skin lesions suggestive of ecthyma gangrenosum (
Figure 2).
Perianal lesions became worse with the loss of substance covered in greenish secretions. A lumbar puncture and microbiological analysis of cerebrospinal fluid were performed. Escherichia coli and P. aeruginosa were isolated from blood cultures. Pseudomonas colonies were also isolated from skin lesions, oropharyngeal exudate, stool sample and bronchial aspirate culture. The results from the urine culture and the microbiological analysis of cerebrospinal fluid were within the normal range. The treatment was switched to antipseudomonal antibiotic by starting a therapy with Meropenem. A substantial decrease of CRP and procalcitonin levels, as well as an increase in the number of leukocytes, were registered in the patient since then.
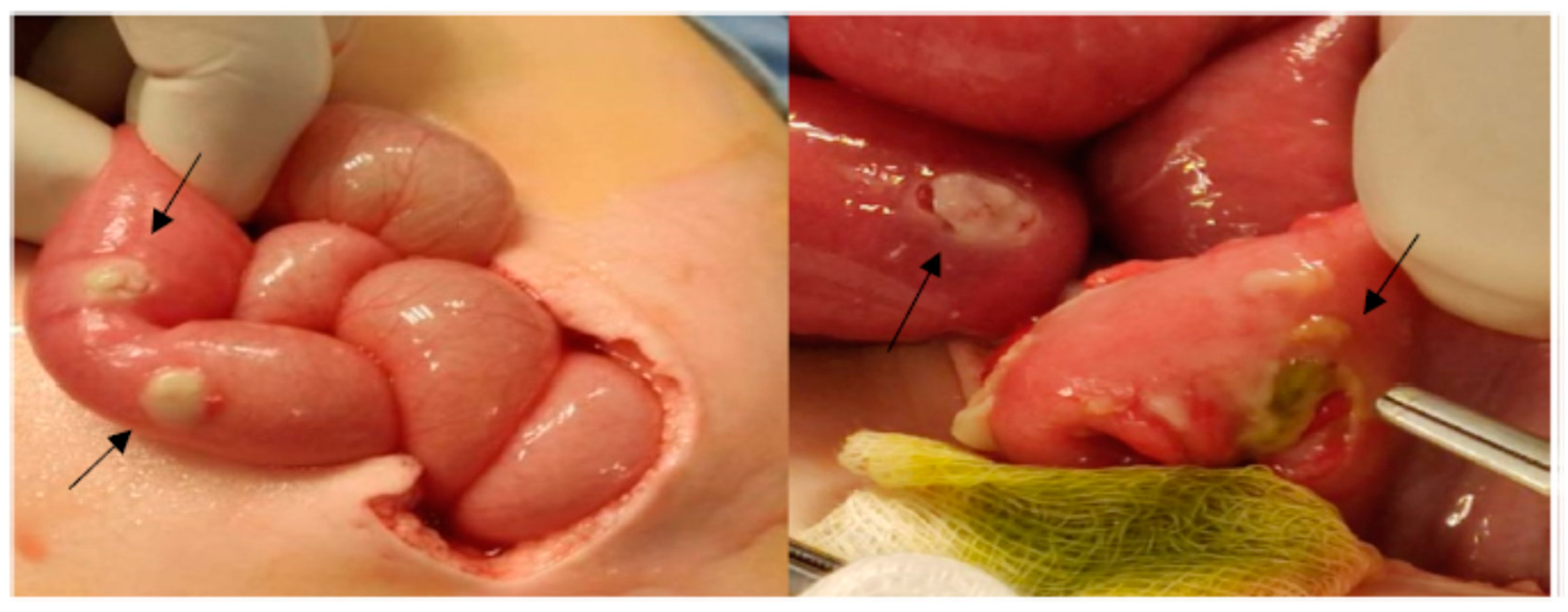
On the fifth day of admission, the patient presented fever associated with bilious vomiting, severe abdominal distension and peritonism. An abdominal X-ray showed signs of hollow organ perforation.
Laparotomy revealed two bowel perforations and widespread patchy necrosis with fibrin coating across the entire small intestine (
Figure 3).
An intestine tract of about 7 cm was resected and an ileostomy was performed. P. aeruginosa was also isolated from peritoneal fluid.
During an extensive immunological study performed to the aim of excluding any primary immune deficiency disease, the immunological evaluation of the patient showed normal lymphocyte subset counts and CD11/CD18 expression, normal complement and immunoglobulin (Ig) levels (IgG 591 mg/dL, IgA 45.2 mg/dL, IgM 61.9 mg/dL), negative HIV test and normal oxidative burst in the dihydrorhodamine test (DHR123).
Over about a month after the admission, the patient showed an improvement of clinical conditions and skin lesions, which led to his discharge from the hospital. Negative blood culture, skin lesions culture and stool culture were obtained before the patient left the hospital.
Nineteen days after his discharge, the baby was hospitalized again because of bilious vomiting caused by two intestinal obstructions secondary to adhesion formations. He was operated upon again and dismissed from hospital five days after the intervention.
5. Discussion
P. aeruginosa is an opportunistic, aerobic Gram-negative bacterial pathogen responsible for a variety of genitourinary, pulmonary, skin and soft tissue infections in hospitalized pediatric patients, often in association with significant morbidity [
12,
13,
14,
15]. Rarely,
P. aeruginosa can lead to severe and life-threatening infections among previously healthy children [
16,
17,
18,
19]. Skin lesions such as subcutaneous nodules and ecthyma gangrenosum may be the first manifestation of
Pseudomonas sepsis that have rarely been reported even in healthy children [
5,
20,
21,
22,
23].
P. aeruginosa can also affect the entire gastrointestinal tract. Hundreds of cases of Shanghai fever have been reported in literature, mostly from East Asia, and with very few exceptions from North America and Europe. All the cases reported in this review meet the criteria of Shanghai fever, although they were registered outside East Asian countries. Chuang et al. described the biggest case series of Shanghai fever in 27 patients in Taiwan [
2]. The clinical manifestations of
P. aeruginosa sepsis among patients from Eastern countries appear to be different from the ones reported in Western countries. Fever and diarrhea are the most common presentations in East Asia, whereas fever and skin lesions are more common in cases reported from North America and Europe [
2]. Ecthyma gangrenosum was reported in 90% of the cases studied in our review, but only in 63% of the patients described by Chuang. The identification of ecthyma gangrenosum lesions could be useful to the earliest possible introduction of the antipseudomonal therapy, since empiric antibiotic treatment commonly used in sepsis in the immunocompetent child are not effective for Pseudomonas infections [
18].
In cases of Shanghai fever in East Asia, most patients have necrotizing enteritis, while bowel perforation is reported in 30% of cases. In our review of cases from complementary regions, three of the patients (30%) have undergone surgery for intestinal perforation.
Necrotizing-ulcerative lesions can also involve the oral cavity and these lesions may lead to perforation of the hard and soft palate, as in one of the cases reported in our review in which the debridement of palatal necrotic tissues and closure of soft palate defect was necessary. In the same case, ecthyma gangrenosum evolved into leg gangrene [
24].
Seizures are frequently associated with Shanghai fever and meningitis is the most serious complication of the central nervous system [
2]. The patient in our case study had signs of meningeal irritation, such as neck stiffness, photophobia and drowsiness, but the cerebrospinal fluid analysis resulted negative. Only in one of the cases reported in our review
P. aeruginosa was isolated in cerebrospinal fluid [
9], while CNS depression and neck stiffness were described in two other cases [
4,
6].
We reported the most important symptoms of Shanghai fever in non-Asiatic countries in
Table 1.
Furthermore, our study seems to confirm existing observations on Shanghai fever, stating that infants account for >80% of reported cases [
2].
Neutropenia is one of the main risk factors for the development of ecthyma gangrenosum and severe
Pseudomonas infections. It has been suggested that infection with
Pseudomonas in healthy children can cause a transient neutropenia by producing a toxin that decreases the number of neutrophils in circulation, such as in patients with Shanghai fever and no immune deficiency disease [
18,
23]. Five patients (50%) in our review had transient neutropenia on admission and the young age appears to be the only risk factor identified in the host. None of the patients in our review presented a primary or acquired immune deficiency disease.
As shown by Chuang et al., Shanghai fever is not associated with hospital-acquired colonization but is caused by more virulent community strains of
P. aeruginosa, demonstrating a higher cytotoxic and invasive profiles [
2].
P. aeruginosa can present various antibiotic resistant mechanism, including the formation of biofilms, the production of virulence toxins and enzymes, low membrane permeability and the expression of antibiotic efflux pumps [
24,
25]. Unfortunately, we were unable to perform molecular analysis or virulence assays in our isolate, but the
P. aeruginosa we isolated was a biofilm producer microorganism. Environmental inspections were performed by the family and
P. aeruginosa was isolated in their domestic water supply. In one case considered by this review,
P. aeruginosa was isolated in samples of bottled water used to prepare baby formulas [
7].
Our case study is compatible with Shanghai fever syndrome despite the epidemiological profile of the latter. Since the patient had no history of traveling outside Italy during his life, it is possible to affirm that more virulent strains of P. aeruginosa are not restricted to Asian countries and may cause Shanghai fever in Italy.
In conclusion, we believe it is important to shed light on this syndrome in non-Asiatic countries and to take into account that it can also affect healthy children. Its clinical features are younger age, especially infancy, with a bloody, mucoid or greenish stool pattern. Diagnosis should be rapid in order to begin a timely treatment with antipseudomonal antibiotics.
Author Contributions
Conceptualization C.C., M.S., C.A., S.G., M.M. and A.C.; Methodology: C.C., S.B. (Sebastiano Billone) and A.C.; Software: L.A.C. and A.C.; Validation: C.C. and A.C.; Formal Analysis: C.C., M.S., S.G. and A.C.; Investigation: C.C., V.C. and M.G.; Resources: C.C., S.B. (Sara Bagarello) and S.A.; Data Curation: C.C. and C.A.; Writing—Original Draft Preparation: C.C., V.C. and C.A.; Writing—Review and Editing: M.S., S.G. and M.M.; Visualization: C.C. and L.A.C.; Supervision: C.C. and A.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the absence of sensitive data, according to the legal framework in which our Institute operates.
Informed Consent Statement
Written informed consent for publication was obtained from parents.
Data Availability Statement
All data used and/or analyzed during this study are included in this article.
Conflicts of Interest
The authors declared no conflict of interest.
Abbreviations
| P. aeruginosa | Pseudomonas aeruginosa |
| CRP | C-reactive protein |
| Ig | Immunoglobulin |
References
- Dold, H. On pyocyaneus sepsis and intestinal infections in Shanghai due to Bacillus pyocyaneus. Chin. Med. J. 1918, 32, 435. [Google Scholar]
- Chuang, C.-H.; Wang, Y.-H.; Chang, H.-J.; Chen, H.-L.; Huang, Y.-C.; Lin, T.-Y.; Ozer, E.; Allen, J.P.; Hauser, A.; Chiu, C. Shanghai fever: A distinct Pseudomonas aeruginosa enteric disease. Gut 2014, 63, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Goolamali, S.I.; Fogo, A.; Killian, L.; Shaikh, H.; Brathwaite, N.; Ford-Adams, M.; Macfarlane, S. Ecthyma gangrenosum: An important feature of pseudomonal sepsis in a previously well child. Clin. Exp. Dermatol. 2009, 34, e180–e182. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, M.K.; Senekal, M. Community-acquired Pseudomonas aeruginosa infection in an infant. Ann. Trop. Paediatr. 1996, 16, 203–206. [Google Scholar] [CrossRef]
- Mull, C.C.; Scarfone, R.J.; Conway, D. Ecthyma gangrenosum as a manifestation of Pseudomonas sepsis in a previously healthy child. Ann. Emerg. Med. 2000, 36, 383–387. [Google Scholar] [CrossRef]
- Schuster, D.I. Palatopharyngeal and lower extremity soft tissue loss in an infant secondary to Pseudomonas gangrenous cellulitis. Ann. Plast. Surg. 1981, 6, 138–141. [Google Scholar] [CrossRef]
- Ortí, A.; Escrig, R.; Pérez-Tamarit, D.; del Otero, M.C.; Diosdado, N.; Muro, M.D.; Asensi, F. Pseudomonas aeruginosa infection in a previously healthy infant. Clin. Pediatr. 2002, 41, 525–528. [Google Scholar] [CrossRef]
- Morales, C.E.A.; Salorio, S.G.F. Ectima gangrenoso como primera manifestación de choque séptico por Pseudomonas aeruginosa en un niño sano. Med. Asoc. Med. Hosp. ABC 2016, 61, 271–274. [Google Scholar]
- Viola, L.; Langer, A.; Pulitano, S.; Chiaretti, A.; Piastra, M.; Polidori, G. Serious Pseudomonas Aeruginosa Infection in Healthy Children: Case Report and Review of the Literature. Pediatr. Int. 2006, 48, 330–333. [Google Scholar] [CrossRef]
- Penteado, F.D.; Bain, V.; Durigon, G.S.; Litvinov, N.; Pereira, M.F.B.; de Sousa Marques, H.H. Shanghai Fever in a Healthy Infant: First Report in South America. Pediatr. Infect. Dis. J. 2018, 37, e278–e279. [Google Scholar] [CrossRef]
- Orchard, P.; Moffet, H.L.; Hafez, G.; Sondel, P. Pseudomonas sepsis simulating acute promyelocytic leukemia. Pediatr. Infect. Dis. J. 1988, 7, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Bodey, G.P.; Jadeja, L.; Elting, L. Pseudomonas bacteremia. Retrospective analysis of 410 episodes. Arch. Intern. Med. 1985, 145, 1621–1629. [Google Scholar] [CrossRef] [PubMed]
- Grisaru-Soen, G.; Lerner-Geva, L.; Keller, N.; Berger, H.; Passwell, J.H.; Barzilai, A. Pseudomonas aeruginosa bacteremia in children: Analysis of trends in prevalence, antibiotic resistance and prognostic factors. Pediatr. Infect. Dis. J. 2000, 19, 959–963. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Smith, J.C.; Zhu, Q.; Guo, Z.; MacDonald, N.E. A five-year review of Pseudomonas aeruginosa bacteremia in children hospitalized at a single center in southern China. Int. J. Infect. Dis. 2012, 16, e628–e632. [Google Scholar] [CrossRef]
- Wang, T.M.; Chen, S.C.; Shian, W.J.; Chen, C.H.; Chi, C.S. Pseudomonas septicemia in infants and children: A retrospective analysis of 49 cases. Zhonghua Yi Xue Za Zhi 1993, 52, 378–384. [Google Scholar]
- Martín-Ancel, A.; Borque, C.; del Castillo, F. Pseudomonas sepsis in children without previous medical problems. Pediatr. Infect. Dis. J. 1993, 12, 258–260. [Google Scholar] [CrossRef]
- Huang, Y.-C.; Lin, T.-Y.; Wang, C.-H. Community-acquired Pseudomonas aeruginosa sepsis in previously healthy infants and children: Analysis of forty-three episodes. Pediatr. Infect. Dis. J. 2002, 21, 1049–1052. [Google Scholar] [CrossRef]
- Chusid, M.J.; Hillmann, S.M. Community-acquired Pseudomonas sepsis in previously healthy infants. Pediatr. Infect. Dis. J. 1987, 6, 681–684. [Google Scholar] [CrossRef]
- Wong, S.N.; Tam, A.Y.; Yung, R.W.; Kwan, E.Y.; Tsoi, N.N. Pseudomonas septicaemia in apparently healthy children. Acta Paediatr. Scand. 1991, 80, 515–520. [Google Scholar] [CrossRef]
- Secord, E.; Mills, C.; Shah, B.; Tunnessen, W.W. Picture of the month. Ecthyma gangrenosum secondary to Pseudomonas aeruginosa. Am. J. Dis. Child. 1993, 147, 795–796. [Google Scholar]
- Duman, M.; Ozdemir, D.; Yiş, U.; Köroğlu, T.F.; Oren, O.; Berktaş, S. Multiple erythematous nodules and ecthyma gangrenosum as a manifestation of Pseudomonas aeruginosa sepsis in a previously healthy infant. Pediatr. Dermatol. 2006, 23, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Bourelly, P.E.; Grossman, M.E. Subcutaneous nodule as a manifestation of Pseudomonas sepsis in an immunocompromised host. Clin. Infect. Dis. 1998, 26, 188–189. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zomorrodi, A.; Wald, E.R. Ecthyma gangrenosum: Considerations in a previously healthy child. Pediatr. Infect. Dis. J. 2002, 21, 1161–1164. [Google Scholar] [CrossRef] [PubMed]
- Biscaye, S.; Demonchy, D.; Afanetti, M.; Dupont, A.; Haas, H.; Tran, A. Ecthyma gangrenosum, a skin manifestation of Pseudomonas aeruginosa sepsis in a previously healthy child. Medicine 2017, 96, e5507. [Google Scholar] [CrossRef]
- Russomanno, K.; Cardis, M.; Kirkorian, A.Y. Ecthyma gangrenosum: The critical role of biofilms and other mechanisms of antibiotic resistance and implications for management. Pediatr. Dermatol. 2021, 38, 458–460. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 




{kind=link}
{kind=link}
{kind=link}