
Education Policy and Under-Five Survival in Uganda: Evidence from the Demographic and Health Surveys

Abstract
:1. Introduction
2. Related Literature
3. Universal Primary Education in Uganda
4. Materials and Methods
4.1. Data Source
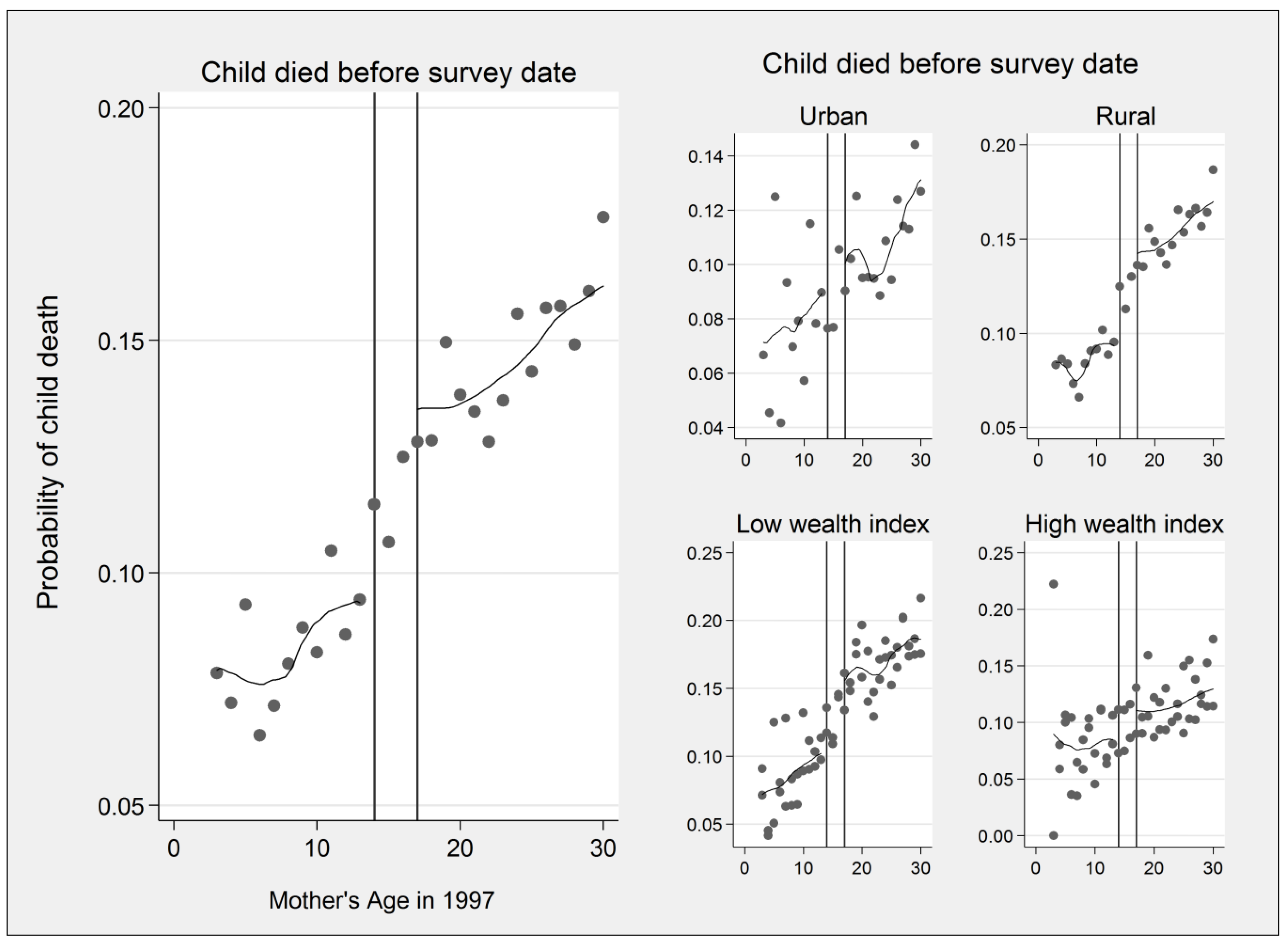
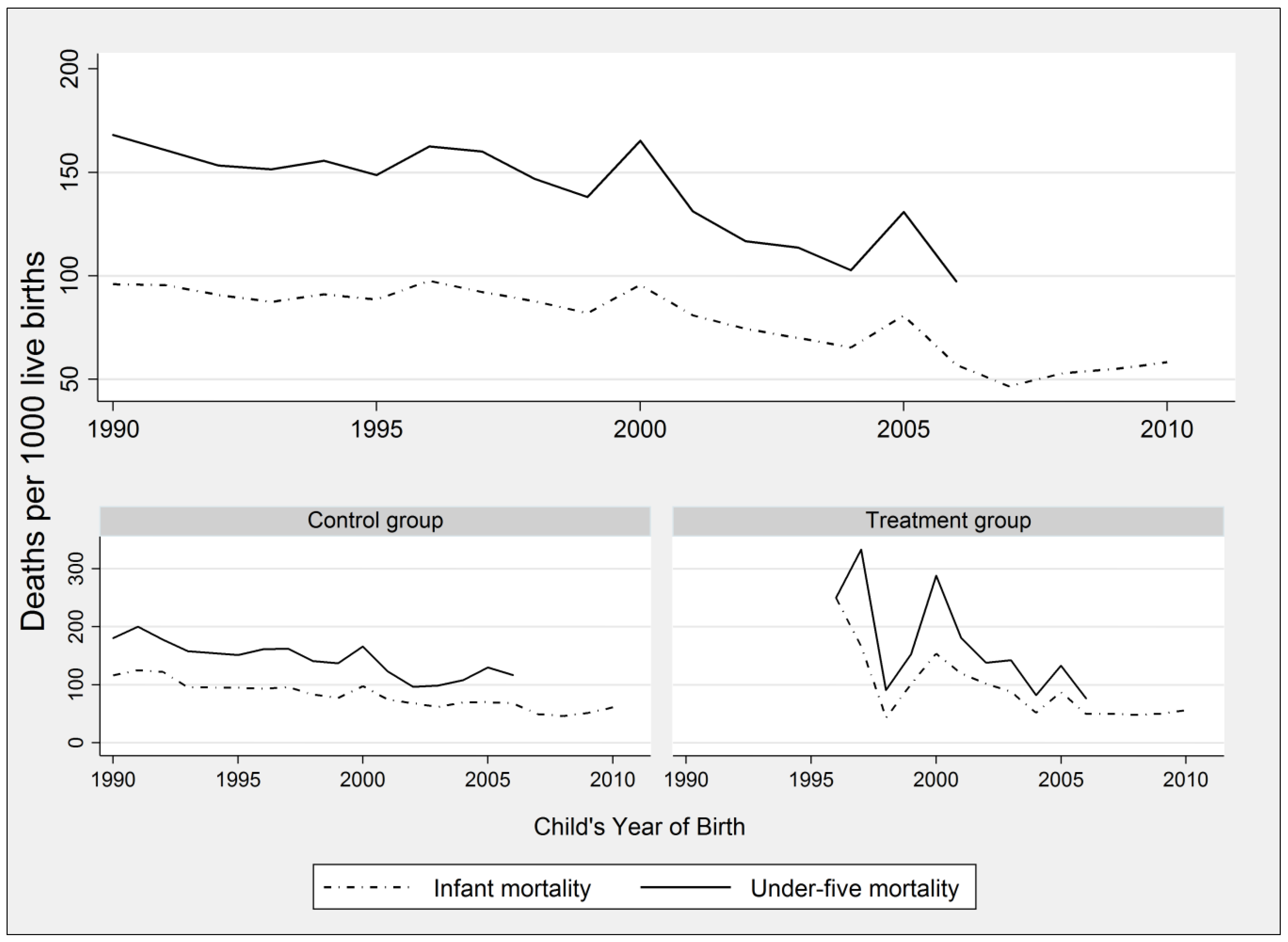
4.2. Measures of Child Mortality
4.3. Explanatory Variables
4.4. Econometric Model
4.5. Robustness Checks
5. Results
5.1. Descriptive Statistics
5.2. First Stage Results
5.3. Second Stage Results
6. Discussion and Conclusions
Acknowledgments
Conflicts of Interest
References
- Michael Grossman. “Education and nonmarket outcomes.” Handbook of the Economics of Education 1 (2006): 577–633. [Google Scholar]
- John C. Caldwell. “Education as a factor in mortality decline an examination of Nigerian data.” Population Studies 33 (1979): 395–413. [Google Scholar] [CrossRef]
- Linda G. Martin, James Trussell, Florentina Reyes Salvail, and Nasra M. Shah. “Co-variates of child mortality in the Philippines, Indonesia, and Pakistan: An analysis based on hazard models.” Population Studies 37 (1983): 417–32. [Google Scholar] [CrossRef]
- Michelle Bellessa Frost, Renata Forste, and David W. Haas. “Maternal education and child nutritional status in Bolivia: Finding the links.” Social Science & Medicine 60 (2005): 395–407. [Google Scholar] [CrossRef] [PubMed]
- John G. Cleland, and Jerome K. van Ginneken. “Maternal education and child survival in developing countries: The search for pathways of influence.” Social Science & Medicine 27 (1988): 1357–68. [Google Scholar] [CrossRef]
- George T. Bicego, and Boerma J. Ties. “Maternal education and child survival: A comparative study of survey data from 17 countries.” Social Science & Medicine 36 (1993): 1207–27. [Google Scholar] [CrossRef]
- Mary Mahy. “Childhood Mortality in the Developing World: A Review of Evidence from the Demographic and Health Surveys.” DHS Comparative Reports No. 4. Calverton, MD, USA: MEASURE DHS+, ORC Macro, December 2003, vol. 4. Available online: https://dhsprogram.com/pubs/pdf/CR4/CR4.pdf (accessed on 24 October 2016).
- T. Akter, D. M. E. Hoque, E. K. Chowdhury, M. Rahman, M. Russell, and S. E. Arifeen. “Is there any association between parental education and child mortality? A study in a rural area of Bangladesh.” Public Health 129 (2015): 1602–9. [Google Scholar] [CrossRef] [PubMed]
- Emily Smith-Greenaway. “Maternal reading skills and child mortality in Nigeria: A reassessment of why education matters.” Demography 50 (2013): 1551–61. [Google Scholar] [CrossRef] [PubMed]
- John Hobcraft. “Women’s education, child welfare and child survival: A review of the evidence.” Health Transition Review 3 (1993): 159–175. [Google Scholar] [PubMed]
- Alaka Malwade Basu. “Maternal education, fertility and child mortality: Disentangling verbal relationships.” Health Transition Review 4 (1994): 207–15. [Google Scholar]
- Lance J. Lochner. “Nonproduction benefits of education: Crime, health, and good citizenship.” NBER Working Paper 16722. Cambridge, MA, USA: National Bureau of Economic Research, January 2011, pp. 183–282. Available online: http://www.nber.org/papers/w16722.pdf (accessed on 24 October 2016).
- Sonalde Desai, and Soumya Alva. “Maternal education and child health: Is there a strong causal relationship? ” Demography 35 (1998): 71–81. [Google Scholar] [CrossRef] [PubMed]
- Karen A. Grépin, and Prashant Bharadwaj. “Maternal education and child mortality in Zimbabwe.” Journal of Health Economics 44 (2015): 97–117. [Google Scholar] [CrossRef] [PubMed]
- Shin-Yi Chou, Jin-Tan Liu, Michael Grossman, and Theodore J. Joyce. “Parental education and child health: Evidence from a natural experiment in Taiwan.” American Economic Journal: Applied Economics 2 (2010): 33–61. [Google Scholar] [CrossRef] [PubMed]
- Jostein Gryttena, Irene Skau, and Rune J. Sørensen. “Educated mothers, healthy infants. The impact of a school reform on the birth weight of Norwegian infants 1967–2005.” Social Science & Medicine 105 (2014): 84–92. [Google Scholar] [CrossRef] [PubMed]
- Pınar Mine Gunes. “The role of maternal education in child health: Evidence from a compulsory schooling law.” Economics of Education Review 47 (2015): 1–16. [Google Scholar] [CrossRef]
- Janet Currie, and Enrico Moretti. “Mother’s education and the intergenerational transmission of human capital: Evidence from college openings.” Quarterly Journal of Economics 118 (2003): 1495–532. [Google Scholar] [CrossRef]
- Paul Glewwe. “Why does mother’s schooling raise child health in developing countries? Evidence from morocco.” The Journal of Human Resources 34 (1999): 124–59. [Google Scholar] [CrossRef]
- UNICEF, WHO, World Bank, and UN-DESA Population Division. Levels & Trends in Child Mortality. Edited by Natalie Leston. New York: United Nations Children’s Fund, 2015. [Google Scholar]
- Marshall Makate, and Clifton Makate. “The causal effect of increased primary schooling on child mortality in Malawi: Universal primary education as a natural experiment.” Social Science & Medicine 168 (2016): 72–83. [Google Scholar] [CrossRef] [PubMed]
- Ricardo Sabates, Jo Westbrook, and Jimena Hernandez-Fernandez. “The 1977 universal primary education in Tanzania: A historical base for quantitative enquiry.” International Journal of Research and Method in Education 35 (2012): 55–70. [Google Scholar] [CrossRef]
- Damien de Walque. “Does education affect smoking behaviors? Evidence using the vietnam draft as an instrument for college education.” Journal of Health Economics 26 (2007): 877–95. [Google Scholar] [CrossRef] [PubMed]
- Adriana Lleras-Muney. “The relationship between education and adult mortality in the United States.” Review of Economic Studies 72 (2005): 189–221. [Google Scholar] [CrossRef]
- T. Paul Schultz. “Returns to women’s education.” In Women’s Education in Developing Countries: Barriers, Benefits, and Policies. Baltimore: Johns Hopkins University Press, 1993, pp. 51–99. [Google Scholar]
- John Strauss, and Thomas Duncan. “Chapter 34 human resources: Empirical modeling of household and family decisions.” In Handbook of Development Economics. New York: Elsevier, 1995, vol. 3, part A; pp. 1883–2023. [Google Scholar]
- Maarten Lindeboom, Ana Llena-Nozal, and Bas van der Klaauw. “Parental education and child health: Evidence from a schooling reform.” Journal of Health Economics 28 (2009): 109–31. [Google Scholar] [CrossRef] [PubMed]
- Paul Gertler. “Do conditional cash transfers improve child health? Evidence from progresa’s control randomized experiment.” The American Economic Review 94 (2004): 336–41. [Google Scholar] [CrossRef]
- Cesar Martinelli, and Susan W. Parker. “Do school subsidies promote human capital investment among the poor? ” The Scandinavian Journal of Economics 110 (2008): 261–76. [Google Scholar] [CrossRef]
- Thomas Duncan, John Strauss, and Maria-Helena Henriques. “How does mother’s education affect child height? ” Journal of Human Resources 26 (1991): 183–211. [Google Scholar]
- Nurcan Yabancı, Ibrahim Kısaç, and Suzan Şeren Karakuş. “The effects of mother’s nutritional knowledge on attitudes and behaviors of children about nutrition.” Procedia Social and Behavioral Sciences 116 (2014): 4477–81. [Google Scholar] [CrossRef]
- Jere R. Behrman, and Mark R. Rosenzweig. “Returns to birthweight.” Review of Economics and Statistics 86 (2004): 586–601. [Google Scholar] [CrossRef]
- Sandra E. Black, Paul J. Devereux, and Kjell G. Salvanes. From the Cradle to the Labor Market? The Effect of Birth Weight on Adult Outcomes. Cambridge: National Bureau of Economic Research, 2005. [Google Scholar]
- Amm Quamruzzaman, José M. Mendoza Rodríguez, Jody Heymann, Jay S. Kaufman, and Arijit Nandi. “Are tuition-free primary education policies associated with lower infant and neonatal mortality in low-and middle-income countries? ” Social Science & Medicine 120 (2014): 153–59. [Google Scholar] [CrossRef] [PubMed]
- Una Okonkwo Osili, and Bridget Terry Long. “Does female schooling reduce fertility? Evidence from Nigeria.” Journal of Development Economics 87 (2008): 57–75. [Google Scholar] [CrossRef]
- Lucia Breierova, and Esther Duflo. “The impact of education on fertility and child mortality: Do fathers really matter less than mothers? ” NBER Working Paper 10513. Cambridge, MA, USA: National Bureau of Economic Research, May 2004. Available online: http://www.nber.org/papers/w10513.pdf (accessed on 24 October 2016).
- Anne Case, Darren Lubotsky, and Christina Paxson. “Economic status and health in childhood: The origins of the gradient.” The American Economic Review 92 (2002): 1308–34. [Google Scholar] [CrossRef]
- Pınar Mine Güneş. “The impact of female education on teenage fertility: Evidence from Turkey.” The BE Journal of Economic Analysis & Policy 16 (2016): 259–88. [Google Scholar] [CrossRef]
- David M. Cutler, and Adriana Lleras-Muney. “Education and health: Evaluating theories and evidence.” In Making Americans Healthier: Social and Economic Policy as Health Policy. Edited by Robert F. Schoeni, James S. House, George A. Kaplan and Harold Pollack. New York: Russell Sage Foundation, 2008, pp. 29–60. [Google Scholar]
- Michael Grossman. “The relationship between health and schooling: What’s new? ” NBER Working Paper 21609. Cambridge, MA, USA: National Bureau of Economic Research, October 2015. Available online: http://papers.nber.org/tmp/21399-w21609.pdf (accessed on 25 October 2016).
- Harold Alderman, Jesko Hentschel, and Ricardo Sabates. “With the help of one’s neighbors: Externalities in the production of nutrition in Peru.” Social Science & Medicine 56 (2003): 2019–31. [Google Scholar] [CrossRef]
- Fred M. Ssewamala, Julia Shu-Huah Wang, Leyla Karimli, and Proscovia Nabunya. “Strengthening universal primary education in Uganda: The potential role of an asset-based development policy.” International Journal of Educational Development 31 (2011): 472–77. [Google Scholar] [CrossRef]
- Uganda Bureau of Statistics. 2015 Statistical Abstract. Kampala: Uganda Bureau of Statistics, 2015. [Google Scholar]
- Uganda Bureau of Statistics. 2004 Statistical Abstract. Kampala: Uganda Bureau of Statistics, 2004. [Google Scholar]
- Ikuko Suzuki. “Parental participation and accountability in primary schools in Uganda.” Compare 32 (2002): 243–59. [Google Scholar] [CrossRef]
- Klaus Deininger. “Does cost of schooling affect enrollment by the poor? Universal primary education in Uganda.” Economics of Education Review 22 (2003): 291–305. [Google Scholar] [CrossRef]
- Raja Bentaouet Kattan. “Implementation of free basic education policy.” The Education Working Paper. Washington, DC, USA: The World Bank, December 2006, p. 7. Available online: http://siteresources.worldbank.org/EDUCATION/Resources/EDWP_User_Fees.pdf (accessed on 25 October 2016).
- Louise Grogan. “Universal primary education and school entry in Uganda.” Journal of African Economies 18 (2009): 183–211. [Google Scholar] [CrossRef]
- Albert Byamugisha. Overall Performance of Districts and Constraints towards Attainment of Sector Targets Using the District League Table (Basing on Education Performance Index: EPI). Kampala: Government of Uganda, 2006. [Google Scholar]
- World Health Organization (WHO). World Health Statistics 2015. Geneva: WHO, 2015. [Google Scholar]
- James Fenske. “African polygamy: Past and present.” The Journal of Development Economics 117 (2015): 58–73. [Google Scholar] [CrossRef]
- Alexander C. Tsaia, and Atheendar S. Venkataramani. “The causal effect of education on HIV stigma in Uganda: Evidence from a natural experiment.” Social Science & Medicine 142 (2015): 37–46. [Google Scholar] [CrossRef] [PubMed]
- Wilbert van der Klaauw. “Estimating the effect of financial aid offers on college enrollment: A regression-discontinuity approach.” International Economic Review 43 (2002): 1249–87. [Google Scholar] [CrossRef]
- Jinyong Hahn, Petra Todd, and Wilbert van der Klaauw. “Identification and estimation of treatment effects with a regression-discontinuity design.” Econometrica 69 (2001): 201–9. [Google Scholar] [CrossRef]
- Julia Andrea Behrman. “The effect of increased primary schooling on adult women’s HIV status in Malawi and Uganda: Universal primary education as a natural experiment.” Social Science & Medicine 127 (2015): 108–15. [Google Scholar] [CrossRef] [PubMed]
- Alain de Janvry, Frederico Finan, Elisabeth Sadoulet, and Renos Vakis. “Can conditional cash transfer programs serve as safety nets in keeping children at school and from working when exposed to shocks? ” Journal of Development Economics 79 (2006): 349–73. [Google Scholar] [CrossRef]
- Dean R. Hyslop. “State dependence, serial correlation and heterogeneity in intertemporal labor force participation of married women.” Econometrica 67 (1999): 1255–94. [Google Scholar] [CrossRef]
- Jeffrey M. Wooldridge. Econometric Analysis of Cross Section and Panel Data. Cambridge: MIT Press, 2002. [Google Scholar]
- Uganda Bureau of Statistics (UBOS), and Macro International Inc. Uganda Demographic and Health Survey 2006. Calverton: UBOS and Macro International Inc., 2007. [Google Scholar]
- Uganda Bureau of Statistics (UBOS), and Macro International Inc. Uganda: Demographic and Health Survey 2000–2001. Calverton: UBOS and Macro International Inc., 2001. [Google Scholar]
- Uganda Bureau of Statistics (UBOS), and ICF International Inc. Uganda Demographic and Health Survey 2011. Kampala: UBOS. Calverton: ICF International Inc., 2012. [Google Scholar]
- Douglas Staiger, and James H. Stock. “Instrumental variables regression with weak instruments.” Econometrica 65 (1997): 557–86. [Google Scholar] [CrossRef]
- Joshua D. Angrist, Guido W. Imbens, and Donald B. Rubin. “Identification of causal effects using instrumental variables.” Journal of the American Statistical Association 91 (1996): 444–55. [Google Scholar] [CrossRef]
- Alcott Benjamin, and Pauline Rose. “Does private schooling narrow wealth inequalities in learning outcomes? ” Oxford Review of Education 42 (2016): 495–510. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Group (Age 5–13 in 1997) | Control Group (Age 17–25 in 1997) | Pairwise t-Test Absolute Difference ((2)–(1)) | Overall Group (Age 5–25 in 1997) | |
|---|---|---|---|---|
| Variables | (1) | (2) | (3) | (4) |
| Maternal-Related Variables | ||||
| Years of education | 5.856 | 4.762 | −1.094 *** | 4.547 |
| Age in 1997 | 9.973 | 20.870 | 10.898 *** | 22.405 |
| Age at first birth | 18.209 | 18.805 | 0.596 *** | 18.611 |
| Terminated pregnancy | 0.147 | 0.234 | 0.086 *** | 0.247 |
| Births in last five years | 1.518 | 1.511 | −0.007 | 1.306 |
| Low wealth (quintiles 1 & 2) | 0.428 | 0.372 | −0.057 *** | 0.400 |
| High wealth (quintiles 4 & 5) | 0.402 | 0.464 | 0.062 *** | 0.407 |
| Urban resident | 0.249 | 0.245 | −0.004 | 0.157 |
| Total number of women (mothers) | 3356 | 6440 | 9957 | |
| Child-Level Variables | ||||
| Child’s year of birth | 2006.356 | 1998.985 | −7.371 *** | 2002.265 |
| Child is female | 0.500 | 0.494 | −0.006 | 0.494 |
| Child is one of multiple | 0.024 | 0.026 | 0.003 | 0.018 |
| Geographic Regions | ||||
| Kampala | 0.094 | 0.141 | 0.046 *** | 0.168 |
| Central 1 | 0.085 | 0.135 | 0.051 *** | 0.164 |
| Central 2 | 0.102 | 0.093 | −0.010 * | 0.115 |
| East central | 0.119 | 0.160 | 0.041 *** | 0.150 |
| Eastern | 0.130 | 0.084 | −0.046 *** | 0.097 |
| North | 0.128 | 0.114 | −0.014 *** | 0.082 |
| Karamoja | 0.084 | 0.063 | −0.021 *** | 0.029 |
| West-Nile | 0.090 | 0.084 | −0.006 | 0.067 |
| Western | 0.104 | 0.083 | −0.021 *** | 0.089 |
| Southwest | 0.064 | 0.044 | −0.020 *** | 0.040 |
| Number of children | 7115 | 26,987 | 34,102 | |
| Specification | Overall (Age 5–25 in 1997) | Age 8–22 in 1997 | Include Age 14–16 in 1997 | Age 6–24 in 1997 | ||||
|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | |||||
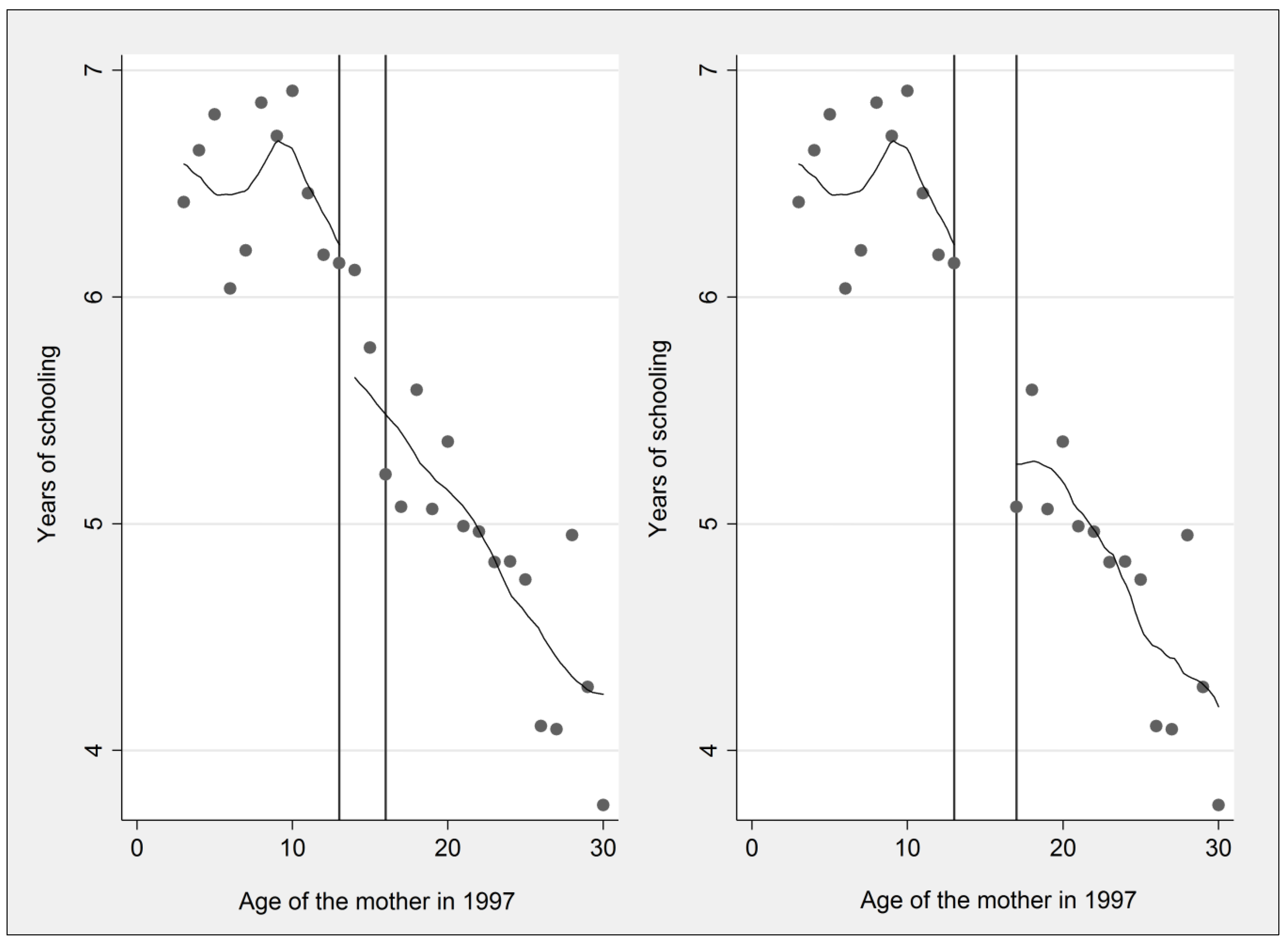
| Years of schooling | ||||||||
| Age less than 13 in 1997 | 0.682 *** | (0.181) | 0.490 * | (0.221) | 0.417 ** | (0.141) | 0.675 *** | (0.195) |
| Urban resident | 0.839 *** | (0.099) | 0.734 *** | (0.117) | 0.757 *** | (0.090) | 0.848 *** | (0.104) |
| Mean of the dependent variable | 5.733 | 5.828 | 5.734 | 5.755 | ||||
| Observations | 13,529 | 9594 | 16,370 | 12,390 | ||||
| Probability of Attending Primary School | ||||||||
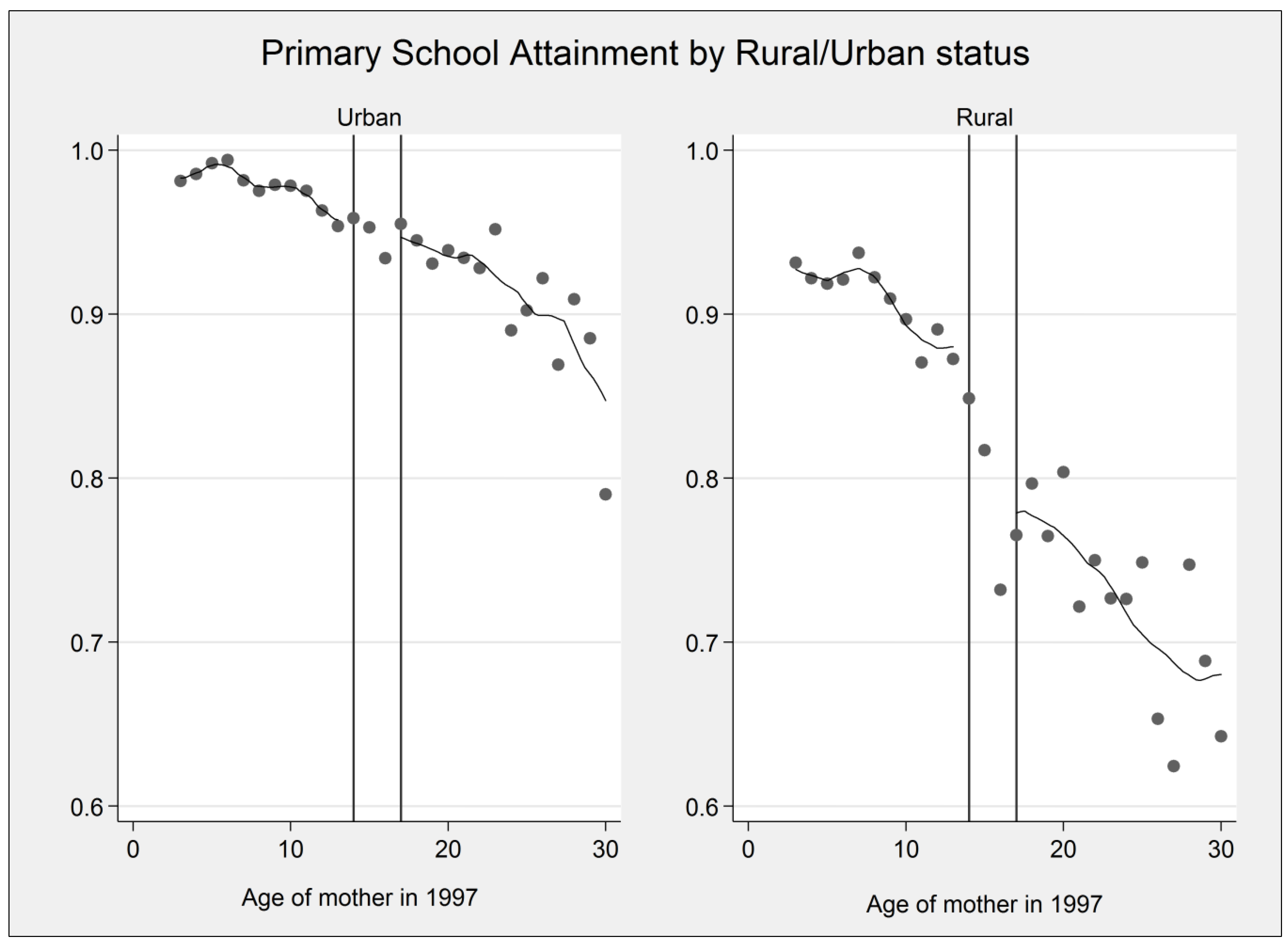
| Age less than 13 in 1997 | 0.263 ** | (0.083) | 0.243 * | (0.105) | 0.190 ** | (0.065) | 0.238 * | (0.097) |
| Urban resident | 0.037 | (0.057) | 0.034 | (0.069) | 0.044 | (0.050) | 0.040 | (0.060) |
| Mean of the dependent variable | 0.862 | 0.864 | 0.859 | 0.863 | ||||
| Observations | 13,530 | 9595 | 16,372 | 12,391 | ||||
| OLS Estimates | Child Dead by Survey Date | Child Dead by Age 1 | Child Dead by Age 5 | |||
| Years of schooling | −0.0043 *** | (0.0007) | −0.0025 *** | (0.0004) | −0.0060 *** | (0.0008) |
| Attended some primary school | −0.0163 ** | (0.0058) | −0.0145 *** | (0.0032) | −0.0228 ** | (0.0087) |
| Observations | 34,102 | 30,895 | 19,279 | |||
| IV Estimates | Child Dead by Survey Date | Child Dead by Age 1 | Child Dead by Age 5 | |||
| Years of schooling | −0.0224 *** | (0.0052) | −0.0158 * | (0.0072) | −0.0306 | (0.0171) |
| First stage F-statistic | 19.608 | 17.670 | 11.866 | |||
| Attended some primary school | −0.4050 * | (0.1605) | −0.3113 | (0.1624) | −0.5948 | (0.5043) |
| Observations | 34,102 | 30,895 | 19,279 | |||
| Mean of the dependent variable | 0.128 | 0.082 | 0.149 | |||
| IV Estimates | Child Dead at Survey Date | Infant Mortality | Under-Five Mortality | |||
|---|---|---|---|---|---|---|
| Age Cohort 19-27 in 2000 and 2011 | ||||||
| Years of schooling | −0.0111 ** | (0.0042) | −0.0225 ** | (0.0086) | −0.0330 | (0.0294) |
| Observations | 8350 | 7084 | 2919 | |||
| First stage F-statistic | 20.291 | 21.313 | 11.945 | |||
| Mean of the dependent variable | 0.098 | 0.070 | 0.132 | |||
| Maternal Age 8–22 in 1997 | ||||||
| Years of schooling | −0.0373 *** | (0.0065) | −0.0165 *** | (0.0047) | −0.0426 | (0.0329) |
| Observations | 23,049 | 20,636 | 11,900 | |||
| First stage F-statistic | 8.378 | 6.873 | 3.551 | |||
| Mean of the dependent variable | 0.123 | 0.081 | 0.148 | |||
| Maternal Age 10–20 in 1997 | ||||||
| Years of schooling | −0.0228 * | (0.0095) | −0.0490 | (0.0296) | −0.2391 | (0.9837) |
| Observations | 15,247 | 13,547 | 7394 | |||
| First stage F-statistic | 2.002 | 1.391 | 0.082 | |||
| Mean of the dependent variable | 0.123 | 0.079 | 0.148 | |||
© 2016 by the author; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makate, M. Education Policy and Under-Five Survival in Uganda: Evidence from the Demographic and Health Surveys. Soc. Sci. 2016, 5, 70. https://doi.org/10.3390/socsci5040070
Makate M. Education Policy and Under-Five Survival in Uganda: Evidence from the Demographic and Health Surveys. Social Sciences. 2016; 5(4):70. https://doi.org/10.3390/socsci5040070
Chicago/Turabian StyleMakate, Marshall. 2016. "Education Policy and Under-Five Survival in Uganda: Evidence from the Demographic and Health Surveys" Social Sciences 5, no. 4: 70. https://doi.org/10.3390/socsci5040070
APA StyleMakate, M. (2016). Education Policy and Under-Five Survival in Uganda: Evidence from the Demographic and Health Surveys. Social Sciences, 5(4), 70. https://doi.org/10.3390/socsci5040070