1. Introduction
There is a shortage of nurses in many developed countries around the world, including Australia (
International Council of Nurses 2021). Understanding the effects of nurses’ perceptions is important to promote retention and attract new nurses (
Nei et al. 2015;
Gregory et al. 2007). Key outcomes that drive nurse retention are health and attitudes, especially commitment, whether being committed to the organization and/or the overall profession of nursing (
Wagner 2012). Consequently, we focus on a useful summary of the many characteristics that impact nurses’ health and attitudes, their perceptions of the state and characteristics of their employment relationship as represented in their psychological contract (
Morrison and Robinson 1997).
Psychological contracts represent the exchanges between employers and employees and are inherently perceptual (
Robinson et al. 1994). Psychological contracts can be examined through three features: promises, fulfillment and breach (
Anderson and Schalk 1998). Across the patterns of results of studies on the psychological contract, key contextual issues, such as occupation, appear to moderate the relationships between facets of the psychological contract and outcomes (
Zhao et al. 2007), although the influences of the specific contexts have yet to be delineated.
This paper has two main aims: First, investigate the relationships between the psychological contract components, with the perceptual control variable of negative affectivity, on key individual outcomes for nurses. The second aim is to design a study in consideration of contextual issues, such as occupational prestige, that may moderate the salience of the psychological contract. Therefore, this study investigates psychological contract promises, fulfillment and breach, with negative affectivity, to determine how psychological contract components may differentially affect key employee outcomes in two contexts that vary in terms of characteristics such as occupational prestige.
1.1. Psychological Contracts and Social Exchange Theory at the Level of the Individual
To better understand the nature of employees’ relationships with work, the idea of a ‘psychological contract’ was introduced by
Argyris (
1960). Some decades later, a resurgence of work on the psychological contract focused on the individual employee’s perceptions of the exchange relationship encompassing the promises and obligations between themselves and their employer (
Robinson et al. 1994).
The development, maintenance and ongoing assessment of the psychological contract can be considered foundational to the employment relationship (
Rousseau 1995). At the level of the individual, the psychological contract is often analyzed using social exchange theory, where individuals aim to balance inputs and outputs during the exchange of diffuse social obligations based on the belief contributions are likely to be returned (
P. M. Blau 1964).
The psychological contract is a contract schema, a structured mental model, about the employment relationship (
Rousseau 1995). Schemas are cognitive frameworks that guide how an individual structures the inputs from their experiences and perceptions, helping individuals make sense of circumstances (
Diehl and Coyle-Shapiro 2019). Evaluations of the employment relationship, particularly when there may be a breach of the psychological contract, are made in relation to the relevant social contract (
Morrison and Robinson 1997).
The psychological contract is often considered by analyzing three distinct components, those of promises, fulfillment and breach (
Anderson and Schalk 1998). The employee’s perceptions of promises made by the organization, and the extent to which those promises are perceived to have been fulfilled, represent the components of promises and fulfillment, respectively (
Robinson 1996). If the employee perceives that the employing organization has broken their promises in the psychological contract, they may perceive psychological contract breach (
Morrison and Robinson 1997).
The promises that are a starting point in the psychological contract may be indicative of potential future contributions to the relationship, where the expectation of fulfilled promises would influence the perception of the exchange relationship and would therefore influence an individual’s behavior (
Conway et al. 2011). Yet, the promises are often considered as just a comparison point for the related, consequent assessment of the degree to which those promises have been fulfilled.
That is, in a similar manner to the impact of realistic job previews, individuals with more realistic expectations (i.e., perceptions of promises) are more likely to have them fulfilled, leading to increased job satisfaction and commitment (
Premack and Wanous 1985). The reinforcement effect of psychological contract fulfillment (
Arnold 1996) is supported by findings across studies highlighting that fulfilling promises is likely to be more important than the promises themselves in leading to positive employee outcomes (
Conway et al. 2011).
Although making promises and fulfilling those promises appear to be at the core of a psychological contract, a large proportion of psychological contract research has been on breach. The cognitive perception of a breach can lead to an affective reaction depending on how the employee interprets and assigns meaning to the breach (
Morrison and Robinson 1997). From a social exchange perspective, when employees identify a discrepancy between the extent to which they have met their perceived obligations and the extent to which their employer has met their obligations, then the individual responds, such as by reducing their inputs (
Zhao et al. 2007).
Across these components of the psychological contract, there are few studies that examine all three constructs concurrently, so the differences are yet to be fully explored. This study therefore explores those differences to investigate how psychological contract constructs affect various employee outcomes.
1.2. Work and Health Outcomes
Fulfillment and obligations increase job satisfaction, increase organizational commitment and reduce intent to quit (
Conway et al. 2011;
Zhao et al. 2007). Importantly, from that pattern of results, the employee outcome related to all three psychological contract components is organizational commitment (e.g.,
Gakovic and Tetrick 2003). Organizational commitment can be considered to embody an ‘array of obligations’ (
Robinson et al. 1994, p. 149) and by including an additional occupational set of obligations, as represented by occupational commitment, the impacts of the psychological contract components can be investigated relative to multiple sets of obligations.
Commitment can have distinct foci, such as a focus on commitment to the organization or commitment to the occupation (
G. Blau 2003). When nurses perceive that their employer has fulfilled their promises, they can be more satisfied at work and more committed to both the organization and the profession of nursing (
Rodwell and Gulyas 2013).
Career and occupation-oriented activities are important in the psychological contract. Nurses aiming to develop their career could expect their employer to conduct appropriate career management, but if there is not appropriate development, nurses may perceive a breach of their psychological contract, which can lead to reduced organizational commitment and turnover (
Rodwell and Ellershaw 2015).
Psychological contract studies have also found relationships with more affective outcomes such as job satisfaction (
Conway et al. 2011) and psychological strain. These affective impacts may be mitigated by psychological contract indicators of predictability and control (
Gakovic and Tetrick 2003) where fulfillment may decrease uncertainty, leading to decreased strain.
However, across the above and other outcomes, there has been a variety of results. For example, meta-analyses of the impacts of psychological contract breach across a range of outcomes have often found quite large ranges for the sizes of the effects despite substantial sample sizes for some outcomes (e.g.,
Zhao et al. 2007). Some of that variation was argued to be a function of the nature of the measures, but they acknowledge that some of those moderators may have been confounded, along with other moderators that were not tested, due to an insufficient number of studies across levels of those moderators.
1.3. Investigating the Variation: Negative Affectivity and Context
So why does there remain so much variability in the nature of the relationships between components of the psychological contract and key outcomes? First, at the individual level, the perceptual basis of the psychological contract (
Rousseau 1995) suggests that individual-level perception modifiers such as negative affectivity may explain some of the variations in results (
Turnley and Feldman 1999). Second, at a broader level, the variety of contexts investigated across studies could indicate that there are characteristics of those contexts that influence the nature and impacts of psychological contracts.
Employees high in the dispositional trait of negative affectivity tend to have a pervasively negative view of the world and themselves, a negative filter on what they perceive, which can shape their appraisal of circumstances (
Watson et al. 1988). At a fundamental level, the perceptual nature of psychological contracts means that psychological contracts can be influenced by perception-modifying dispositional traits such as negative affectivity (
Raja et al. 2004;
Tallman and Bruning 2008). Negative affectivity is particularly likely to play a role in psychological contract studies when studying outcomes with an affective component.
For example, the impact of breach has sometimes been seen as primarily cognitive, resulting from a cognitive assessment of the psychological contract (
Robinson et al. 1994), but breach has been argued to also impact affect (
Morrison and Robinson 1997). Breaking the psychological contract may lead to ill health (
Robbins et al. 2012). Yet, strong affective responses to the psychological contract, especially breach, may partly be due to the individual’s affectivity, leading to calls for negative affectivity being included in psychological contract research (
Turnley and Feldman 1999).
Similarly, the inherent negative emotionality of those high in negative affectivity can also lead to greater sensitivity to psychological contract breach (
Rodwell et al. 2022;
Turnley and Feldman 1999). The greater affective sensitivity of those high in negative affectivity may especially occur with individual outcomes that have an affective component, such as job satisfaction (
Brief et al. 1995;
Spector et al. 1999) and stress-related variables (
Rodwell et al. 2015), as well as relatively cognitive outcomes such as organizational commitment (
Kickul 2001;
Rodwell 2018). Therefore, the inclusion of negative affectivity enables the separation and consideration of perceptual influences and outcome emotionality that could otherwise inflate the relationships between the facets of the psychological contract and individual-level outcomes.
At the broader level, one of the most vexing problems in organizational behavior—the variation in results across studies—is likely to be largely due to the variety of contexts investigated across studies (
Johns 2006). Furthermore, there is a strong theory basis, building upward from social exchange theory, as to the nature of the role context can play in understanding psychological contracts.
At the level of the individual, the psychological contract is often analyzed using social exchange theory, where individuals aim to balance the exchange of inputs and outputs. However, the nature of the context can differentiate exchange relationships over time, where individuals with notable amounts of power are less reactive to social forces (
P. M. Blau 1964). That is, the schemas of the psychological contract are shaped by multiple contexts, across levels, such as law, societal beliefs and occupations (
Rousseau 2001). The possible nesting of these contextual issues requires that research try to delineate the effects of specific contextual moderators (
Zhao et al. 2007). One particularly powerful and relevant approach for understanding the impact of context on the psychological contract research is sensemaking.
The process of organizing incoming information into schemas is known as sensemaking, a theory or perspective about how individuals interpret the information they perceive (
Weick 1995). Schemas about employment relationships help individuals to structure their recall and interpretation of promises (
Diehl and Coyle-Shapiro 2019;
Morrison and Robinson 1997). Individuals actively use interpretive schemas based on experience and socialization to create sense and meaning from the reality the individual acts upon (
Weick 1995). Similarly, the sensemaking perspective can help to explain how and why the components of the psychological contract act as they do. For example, from a sensemaking perspective, the potential impact of psychological contract breach can be understood as the individual employee feeling a ‘reality shock’, which can explain the depths of reactions to breach and their affective impact (
Diehl and Coyle-Shapiro 2019).
By building upon the social exchange basis of the psychological contract, individuals using sensemaking to understand and interpret what is happening in their contexts can help to explain the roles that context may play in understanding the psychological contract. Context-driven sensemaking could particularly impact the psychological contract because members of the same social system have similar schemas (
Diehl and Coyle-Shapiro 2019), resulting in different contexts being governed by different social contracts. However, there are layers of context that apply to any given situation and each of the respective layers of context may impact the sensemaking inherent to the psychological contract.
1.4. Tightening the Contexts Considered to Delineate Possible Context Effects
To investigate the overlapping layers of context, one of the most useful research designs to illuminate the nature of the specific contexts is comparative research that intentionally contrasts situations that vary in terms of important contextual dimensions (
Johns 2006). That is, comparing the distinguishing characteristics of relevant contexts can inform understanding of the nature of the contexts.
The overlapping layers of contexts that may impact social exchange and sensemaking range from the more macro characteristics, such as, for nurses, the relatively consistently well-educated workforce, workforce supply and demand (influencing occupational power), hierarchy and prestige of the occupation, through to organizational practices, pay and conditions, and the nature of the work.
In terms of similarities, at the broad level, contexts within the same country should have similar national culture. Within the same country and state, nurses would have the same registration bodies and the same system of recognition for qualifications (including the education required for specific forms of nursing care, such as medication administration).
A high-level distinguishing characteristic among nurses is the subsector of where they work, where the two largest subsectors of nursing are general acute care in hospitals and aged care. Note though that these nursing subsectors have generally similar occupational regulations, where working as a nurse in Australia requires having completed an approved course and being registered with the Nursing and Midwifery Board of Australia (
Department of Health 2023), but vary in terms of the patients served and the related, lower-level contextual issue—the nature of work. The professional and education regulations of nurses makes the psychological contract a relevant vehicle for comparing contexts because psychological contracts are particularly relevant to services and to relatively well-educated workforces (
Rousseau 1995). Although psychological contracts appear to operate differently for ‘in demand’ employees, such as nurses, with a lower unemployment rate (
Rodwell and Ellershaw 2015).
The prototypical nurse working environment is a general acute hospital with proportionally high levels of registered nurses (RNs; nurses who have completed a bachelor’s degree or equivalent) and is where the largest proportion of the nursing workforce is employed. General hospital nurses may have more diverse and sometimes acute work demands relative to other nursing contexts such as aged care (
Rodwell and Fernando 2016).
The second largest subsector of nurse work in developed countries is in aged care nursing (i.e., residential care of the elderly). Residential care and nursing homes provide long-term personal or nursing care for those unable to properly care for themselves (
Rodríguez-Martínez et al. 2023). Aged care nursing tends to have older nurses and proportionally more enrolled nurses (nurses who have completed sub-baccalaureate certificates or diplomas and work under RNs), carrying out basic nursing care and less complex procedures (
Health Workforce Australia 2013;
Kloster et al. 2007). Nurses in residential aged care primarily care for patients suffering chronic mental and medical conditions (
Elstad and Vabø 2008).
Hospital and residential aged care nursing contexts within the same organization would have generally similar organizational and employment policies in each context. However, in terms of social organization (per
Coffey et al. 1988), general hospitals have stronger, all-pervading occupational groupings and hierarchies (e.g., relative to medical doctors) than aged care facilities (
Rodwell and Fernando 2016). The main remaining differences between hospital nurses and aged care nurses working within the same organization would then be the intertwined characteristics of the nature of the work itself and the perceptions of that work by the workers and the broader public.
For example, aged care nursing is seen as a less desirable career path compared to other forms of nursing by students, and students receive less placement days (on-the-job training) specific to aged care (
Kloster et al. 2007). Attracting graduate nurses to aged care over acute care is challenging, with nurses in training seeing little appeal in gerontology (
Elliott et al. 2017). Nursing students may also have a negative view of aging (
Cerqueira et al. 2023) and thus aged care. That is, aged care could be categorized as being less prestigious with the consequent lower employment expectations, resulting in a floor effect that could result in expectations having less of a role, weakening the impact of psychological contract promises.
In academic terms, occupational prestige is a form of social stratification measuring people’s relative social positions based on their occupations and a commonly used rating system was constructed by the National Opinion Research Center/NORC. The NORC study ratings are constructed by asking a sample of respondents to rate occupations based on an ‘occupational prestige ladder’ using a scale from one to nine (
Smith and Son 2014).
For the present study, different roles within the nursing occupation report varying occupational prestige ratings. For example, licensed practical nurses received an average rating of 6.5, while eldercare aides received an average of 4.9 (
Smith and Son 2014), a differential that has remained consistent for many years. There are several factors associated with the higher occupational prestige rating for registered nurses in hospitals. First, registered nurses employed in hospitals realize a wage advantage relative to nurses employed elsewhere (
Algoso et al. 2016). Second, the policies associated with residential aged care, along with views about the nature of the work, may reduce the occupational status of nurses working in residential aged care (
Thompson et al. 2016). Similarly, within the occupation of nursing, undergraduate students perceive a range of deterrents to working in aged care (
Algoso et al. 2016) that may build on a negative view of ageing (
Cerqueira et al. 2023).
People working in more powerful healthcare occupations may feel they have more career agency in reacting to challenges to their psychological contract, which can impact the nature of their performance behaviors (
Mitra et al. 2023). In effect, employees with more power may feel a greater sense of entitlement and be more likely to identify breaches of their psychological contract (
Morrison and Robinson 1997). Both the occupation and the work context (occupation-in-context) may influence the nature of the psychological contract and thereby modify the reactions of the employee. That is, comparing nursing in hospitals with aged care, in terms of how they impact the nurse’s psychological contract, may be a complex, mixed-together combination of occupational prestige, power and the nature of the work.
This study does not intend to definitively specify the components of the contextual differences at this stage but instead investigates the patterns of relationships between psychological contracts and key outcomes to see if the results suggest that more work needs to be carried out in future to delineate the key components of contexts that may influence individual-level perceptions such as the psychological contract. The social exchange differentiation that can occur by context and the role of sensemaking for differing contexts provides a rigorous theoretical basis for contextual differences changing the nature of the psychological contract.
The focus of this study is to see if the pattern of results between the components of the psychological contract and the outcomes varies by context, by investigating two distinct nursing contexts—a general hospital and residential aged care—from within the same organization. Directionality was not included because of the inconsistency of prior results and because the possible impacts of particular facets of context that remain to vary have not been investigated before. The specific hypotheses are as follows:
Psychological contract promises, fulfillment and breach, with negative affectivity, impact the individual-level outcomes of job satisfaction, psychological distress, organizational commitment and occupational commitment for nurses in a general acute hospital context;
Psychological contract promises, fulfillment and breach, with negative affectivity, impact the individual-level outcomes of job satisfaction, psychological distress, organizational commitment and occupational commitment for nurses in an aged care context.
3. Results
The analyses in SPSS/AMOS 22 used maximum likelihood estimation (MLE). Fit indices ranging from the ratio of the chi squared statistic to the degrees of freedom (χ
2/df), the standardized root mean square residual (SRMR), the root mean square error of approximation (RMSEA), to the comparative fit index (CFI) were used. The following criteria (per
Hoyle 2012) were guidelines for assessing fit: χ
2/df < 2, SRMR < 0.08, RMSEA < 0.06 and CFI > 0.95.
Data screening led to final samples of 149 hospital nurses/midwives and 197 aged care nurses. The missing data were missing completely at random. The descriptive statistics across variables for each setting are in
Table 2, showing that the Cronbach alpha reliabilities of the original scales were good.
Examining the measurement model using confirmatory factor analyses indicated that the measures were individually univariate and that there was discriminant validity between the variables. All of the variables were parceled using single-indicator latent variables (SILV) as recommended by
Rodwell and Ellershaw (
2015) and
Wang et al. (
2009).
Item parceling entails forming agglomerate manifest variables for use in SEM and is advocated by many authors due to advantageous psychometric properties (
Meade and Kroustalis 2006). SILVs work as well as, if not slightly better than, other parceling methods (
Sass and Smith 2006). Parceling was used because the focus was on associations between variables, not their structures; parceling improves data normality, reducing estimation errors in SEM; and parceling provides more stable parameter estimates when there are smaller samples (
Bagozzi and Heatherton 1994). The formulae used to calculate the regression coefficients for each composite variable on the relevant latent variables and the composite variables’ measurement error variances are from
Munck (
1979) and are detailed in
Rodwell et al. (
2017).
The analyses investigated psychological contract promises, fulfillment and breach, with negative affectivity, on the work, occupation and distress variables (job satisfaction, psychological distress, occupational commitment and organizational commitment). Although partial invariance testing between the groups may have been possible, the value of such testing is still debated in the technical literature and, more importantly, would not be appropriate given the inability to specify any major model differences a priori (see
Byrne (
2010) for further details and introductory discussion). The delineation of the possible effects of specific contextual issues such as occupational prestige is too novel to specify the expected differences between models.
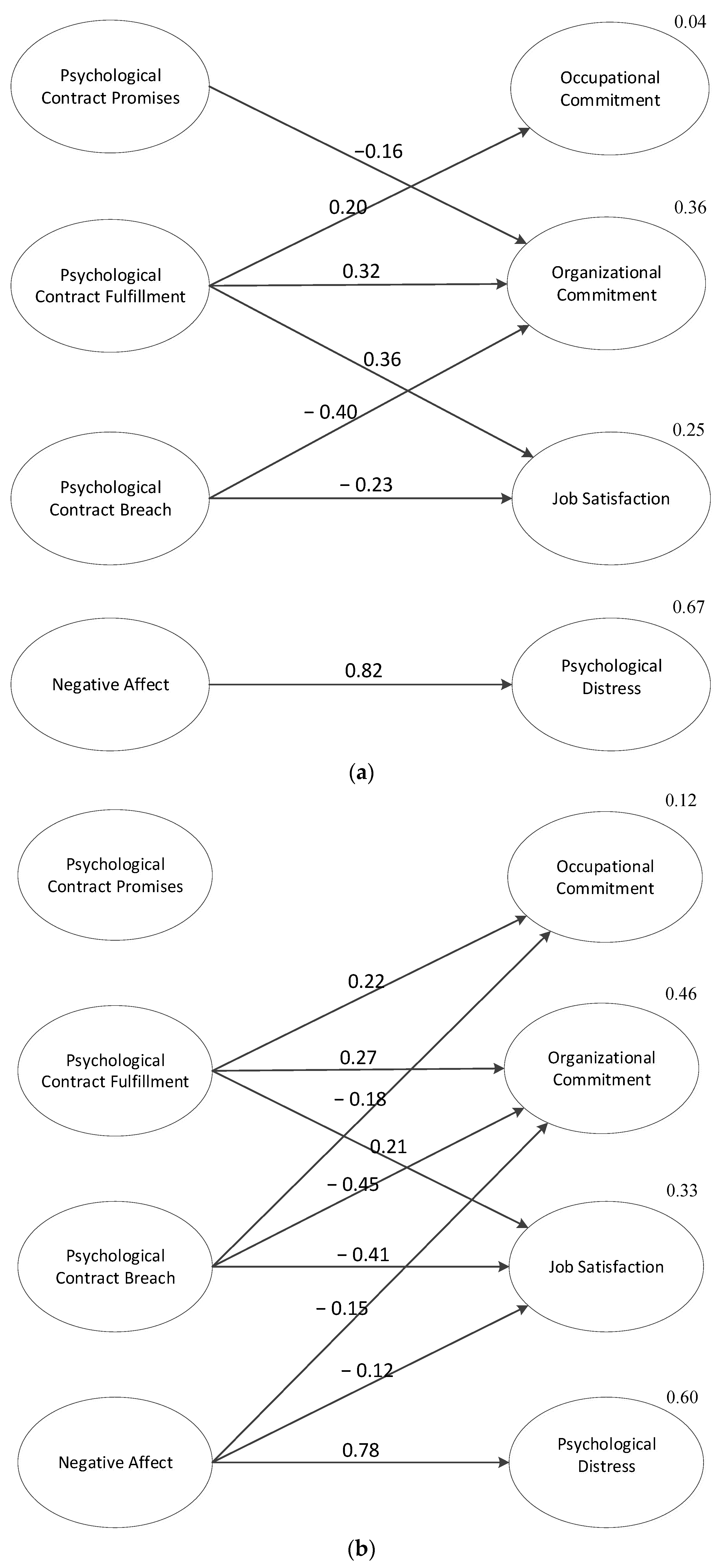
The final models showing the significant connections are in
Figure 1a,b. For the hospital nurses and midwives, the full model with all possible connections had a χ
2(df) of 27.94(6),
p < 0.001. Removing the nonsignificant paths led to χ
2(df) of 36.58(15),
p < 0.05 (Δχ
2(9) = 8.64,
p > 0.05). Correlating the outcome variables resulted in a final model having χ
2(df) of 9.71(9),
p > 0.05 (Δχ
2(6) = 26.87,
p < 0.05), indicating a significantly improved model that was not significantly different in recreating the data. The final model’s fit statistics were: χ
2/df = 1.079, SRMR = 0.036, RMSEA = 0.023 [CI90 0.000, 0.097] and CFI = 0.997.
For aged care nurses, the full model with all appropriate direct relationships was tested and had χ2(df) of 83.37(6), p < 0.001. Removing the nonsignificant paths led to χ2(df) of 93.65(13), p < 0.001 (Δχ2(7) = 10.28, p > 0.05). Correlating the outcome variables resulted in a final model having χ2(df) of 6.83(7), p > 0.05 (Δχ2(6) = 86.82, p < 0.05), a significantly improved model that was not significantly different in recreating the data. The final model’s fit statistics were χ2/df = 0.975, SRMR = 0.032, RMSEA = 0.000 [CI90 0.000, 0.086] and CFI = 1.000.
4. Discussion
Psychological contract breach and fulfillment had similar, but separate and distinct, relationships with the outcomes, specifically, job satisfaction, occupational commitment and organizational commitment, yet promises on their own had little effect in the hospital sample and none in the aged care group. Nurses’ perceptions of their employer’s promises were only significant for one outcome across the two contexts, where promises were negatively related to organizational commitment in hospital nurses. The negative relationship between promises and organizational commitment for hospital nurses may be due to the hospital nurses having unrealistic expectations, perceiving that the organization owes them more, which results in reduced commitment, a mechanism akin to having not had realistic job previews (
Premack and Wanous 1985).
In contrast, when employers were seen to have fulfilled their promises, the nurses had increased occupational commitment, job satisfaction and organizational commitment for both samples. These results highlight the importance of fulfillment and confirm previous results for other samples (e.g.,
Conway et al. 2011;
Zhao et al. 2007) that the fulfillment of obligations is often important for nurses’ job satisfaction and organizational commitment. The consistent links between fulfillment and both organizational and occupational commitment in this study appear to confirm that the various sets of obligations (comprising the two foci of commitment) are exchanged by the employee in return for the perceived work and organization-specific promises being fulfilled. This pattern of results extends
Robinson et al.’s (
1994) findings to occupational commitment and confirms the connection between career activities and the psychological contract. That is, the promises by the employer in the psychological contract may indicate a debt that is incurred by the organization, but the debt incurred by the employee when the organization fulfills their obligations is far more powerful.
Fulfillment was related to both forms of commitment and job satisfaction, supporting and extending previous research on nurses (e.g.,
Gregory et al. 2007). The relationship between fulfillment and job satisfaction may be because satisfaction is more proximal to the met expectations of the employees (
Rodwell and Gulyas 2013). These findings emphasize the importance of the fulfillment of promises and suggest that the primary mechanism for employees is the amount of reinforcement received (
Arnold 1996).
The effects of psychological contract breach were similar across the two nursing groups. Specifically, breach reduced job satisfaction and organizational commitment in both groups of nurses, and with increased occupational commitment for aged care nurses. This pattern of results supports previous research on job satisfaction and organizational commitment in nurses and other professional groups (
Zhao et al. 2007). Again, the consistent relationships between breach and both organizational and occupational commitment further confirms that the sets of obligations comprising commitment are exchanged. The study results indicate that commitment is withdrawn or not provided by the employee when faced with breach. That is, the relationships between fulfillment and the two forms of commitment are driven by the discrepancy between the perceptions of what was delivered and what was promised (
Turnley and Feldman 1999), which leads to the employee adjusting their commitment, especially their obligations to the organization.
Breach has been argued to have more severe consequences than unmet obligations because breaches may cause employees to feel wronged due to the broken promise and breach has usually been found to have more of an impact than fulfillment (
Anderson and Schalk 1998). However, the effect of relationships between breach and fulfillment on job satisfaction and the two forms of commitment were often significant in a similar pattern, rather than only breach being significant. One possible explanation for this consistent pattern of results is that the perception-based nature of negative affectivity alters the potential relationships with the employee outcomes, such that the strength of the negative effects of breach were reduced, yet the apparently more cognitively oriented positive effects of fulfillment remained strong. This change in strength of effects may suggest that negative affectivity plays or role in the interpretation process of breach. That is, the extent to which the perception of breach leads to an affective reaction depends on the interpretation process by which the employee generates meaning (
Morrison and Robinson 1997), and that interpretation process is strongly influenced by negative affectivity.
Another novel contribution of this study comes from investigating the relationships between the psychological contract and distress, with few psychological contract studies having explored impacts on mental health (
Robbins et al. 2012). In this study, strain is only predicted by negative affectivity in both samples, suggesting that the links from the psychological contract to strain found in previous studies may have been spurious, and were possibly a product of negative affectivity, a variable not measured in those studies. That is, the inclusion of negative affectivity in psychological contract research could begin to clarify the character of the relationships between the psychological contract components and affect-oriented outcomes.
Higher levels of negative affectivity were linked to increased psychological distress for both samples of nurses and to reduced job satisfaction and organizational commitment for the aged care setting. Strong effects of negative affectivity in both nursing samples strengthens the case for negative affectivity to be included in future psychological contract research, particularly given the inherently perceptual nature of the psychological contract. Negative affectivity has a more diffuse set of relationships for the aged care nurses, impacting three of the four outcomes. The more diffuse set of relationships with negative affectivity may also reflect self-selection effects where those in aged care have a wider range of negative affectivity, making it more likely that negative affectivity could be significantly related to more outcomes. The effects of negative affectivity may be due to more vigilant monitoring of their psychological contract (
Morrison and Robinson 1997), a process that could be investigated in future research.
Overall, the similarity in the patterns of results from fulfillment and breach may indicate that both discrepancy and shock mechanisms apply. That is, assessments of relatively continuous discrepancies reflect fulfillment, which involves nurses making homeostatic adjustments, a running mental tally, increasing commitment and satisfaction. In contrast, psychological contract breach is discontinuous, on the fulfillment continuum, which leads to a ‘reality shock’ (
Diehl and Coyle-Shapiro 2019) and reduced satisfaction. That is, there may be two forms of discrepancy mechanism underpinning the assessment of the psychological contract: assessment of continuous discrepancy, by fulfillment, and assessment of discontinuous discrepancy, in terms of breach.
Promises, in their own right, only had one significant relationship, where the negative effects of promises appear in the hospital context but do not appear in the aged care context. The lack of relationships from promises to any of the outcomes suggests that aged care nurses do not hold the organization to its promises or feel that they cannot hold the organization to account for its promises. The lower employment expectations could lead to a floor effect where expectations have less of a role, weakening the impact of psychological contract promises. Similarly, the other distinct relationship was from breach to occupational commitment for the aged care nurses. That is, the aged care nurses having less power are more reactive to social forces, where the nature of the context can differentiate exchange relationships over time (per
P. M. Blau 1964).
Together, these distinct relationships suggest that employees with more prestige and perhaps power may have more of a sense of entitlement than those with little power (
Morrison and Robinson 1997). The employment schemas help individuals interpret and track the promises that exist in an employment relationship (
Morrison and Robinson 1997;
Diehl and Coyle-Shapiro 2019), but those schemas vary by the power and prestige of the occupation by context. The apparently lower levels of agency for the aged care nurses could have wide-ranging impacts, especially if breach may lead to them leaving the profession, because nursing home staff impact the quality of life perceived by residents and their family (
Rodríguez-Martínez et al. 2023). The occupation-in-context effects suggest that those aged care nurses make more transactional career decisions to regain control they have lost in their work environment (in a similar manner to that found by
Mitra et al. (
2023) for medical doctors in a primary care context).
The schemas of the psychological contract are shaped by multiple contexts, across levels, such as law, societal beliefs and occupations (
Rousseau 2001). By focusing on the same broad occupation in the same organization, in the same country, with the same licensing regulations and educational requirements, but in different types of work contexts, this study begins to clarify the potential role of context that may help to clarify the inconsistent findings across psychological contract studies. More attention may be needed with regard to delineating the particular drivers of differences by context, such as occupational prestige, because a range of other issues can also be relevant in impacting the social schema that informs the sensemaking behind the psychological contract.
Future research may particularly wish to tease out the influences of prestige and power as part of the sensemaking and psychological contract processes for a wider variety of combinations of occupations and contexts. For aged care nursing, what are the drivers of graduate nurses seeing little appeal in gerontology (
Elliott et al. 2017) and are nurses’ perceptions influenced by a negative view of ageing (
Cerqueira et al. 2023) or are there specific elements of the nature of aged care work that reduce the occupational status of nurses working in residential aged care (
Thompson et al. 2016)?
If occupational prestige and power need to be enhanced, how is that implemented? Changing the notable wage differential across nursing contexts (
Algoso et al. 2016) may be a start, but improving the nature of aged care work may also require more developmental training opportunities (
Elliott et al. 2017) and (extending
Mitra et al. 2023) improved workloads, job rotation and job sharing options, structured time off, and flexible work benefits that improve expectations. Once those changes have occurred, disseminating the changed nature of aged care nursing may involve increasing aged care placement days (addressing
Kloster et al. 2007).
This study’s limitations include its cross-sectional design, preventing claims of causality, but that is expected, as it is one of the first to surface the potential role of occupational prestige and power for nurses’ psychological contracts. A further limitation is that the data were self-report measures, which may cause issues with common method variance (CMV). Several steps were taken during the design of this study to reduce the chance of CMV. For example, prior to completing the questionnaire, detailed information was presented to participants outlining that the data would be confidential and anonymous, which should have lessened any social desirability threats. Further, the other main likely response bias was explicitly surfaced by including negative affectivity in the analyses, which would account for much of any potential inflationary variance (following
Spector 2006).
Note that the comparator approach used in this study was particularly focused on nurses and was in a developed country, Australia. Therefore, the elements of context being proposed for delineation may be more applicable to nurses in developed countries and would need to be tested for their applicability to other occupations and/or countries.
This study also investigated only one side of the exchange relationship, through employees’ perceptions of the variables, although this is consistent with the dominant approach to psychological contracts (following
Rousseau 1995). Future research may wish to use longitudinal designs and data from multiple sources, such as employees and employers, enabling in-depth study.
5. Conclusions
The fulfillment of promises appears to be a key driver of the psychological contract reflecting the amount of reinforcement received (
Arnold 1996). Employees therefore appear to be driven by reinforcement, indicating that organizations should make promises to employees that they are sure they can fulfil. The effect of fulfillment on improving employee outcomes combines with the detrimental impacts of any breaches to the psychological contract. The results also highlight the need to include negative affectivity in future psychological contract research, particularly with negative affectivity as the only predictor of employee strain. Future research could clarify whether promises are quite weak as a driver and/or the negative effects of promises only appear in contexts where the employees have less occupational prestige and/or power, where they cannot afford to be cynical about the promises.
More broadly, the results suggest that fulfillment occurs in a relatively continuous manner, while breach creates a shock and a discontinuity. That is, two of the psychological contract components reflect two forms of discrepancy mechanism, one where fulfillment assesses the relatively continuous extent to which promises are fulfilled and the other where breach indicates a discontinuous discrepancy.
The pattern of relationships between fulfillment and breach, with multiple commitment foci, highlight the importance of career management activities, which in turn may also help in keeping these employees in the profession. Raising the profile of career management activities, especially in aged care, may also be of interest to broader bodies, such as governments, seeking to keep professionals in healthcare occupations to avoid or minimize staffing shortfalls.
In terms of context-oriented theory, sensemaking of the specific context, occupation and nature of work reflected by differences in terms of occupational prestige and power modified the impact of promises and widened the impact of breach to include reducing the aged care nurses’ commitment to the profession. Future research can begin to delineate which of the possible key influences on the psychological contract such as task power, occupational power, task discretion, career pathways, salary importance, variety of work, stimulation, and impacts of training are the most important.
In terms of improving the prestige and nature of aged care work, little is known about how that could be achieved. If a starting point is increasing the wages of aged care nurses, then there may be some areas for interesting contextual comparisons. For example, in most OECD countries, aged care workers have lower salaries than average (
Elliott et al. 2017). Yet, there are exceptions. For example, studies have begun exploring the impact of aged care employees earning more in Luxemburg relative to Belgium (
Fujisawa and Colombo 2009). Future detailed comparisons of contexts and characteristics of contexts may provide opportunities for future research to investigate which of the contextual differences impact organizational behavior such as psychological contracts. Contexts such as aged care urgently need more nurses, and a better understanding of what attracts and retains nurses in aged care could help.
With shortages of nurses and, in particular, dramatic shortages of aged care nurses, managers can also set realistic expectations, conduct realistic job previews and, once the nurses are on staff, fulfil the organization’s promises. More broadly, healthcare organizations and other bodies may also want to put more effort in to enhancing the occupational prestige of aged care nursing.





{kind=link}