
Transgender Health between Barriers: A Scoping Review and Integrated Strategies


Abstract
1. Introduction
1.1. Transgender Health and Ecological Theory of Human Development
1.2. The Aim and the Research Questions of the Review
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Review Team
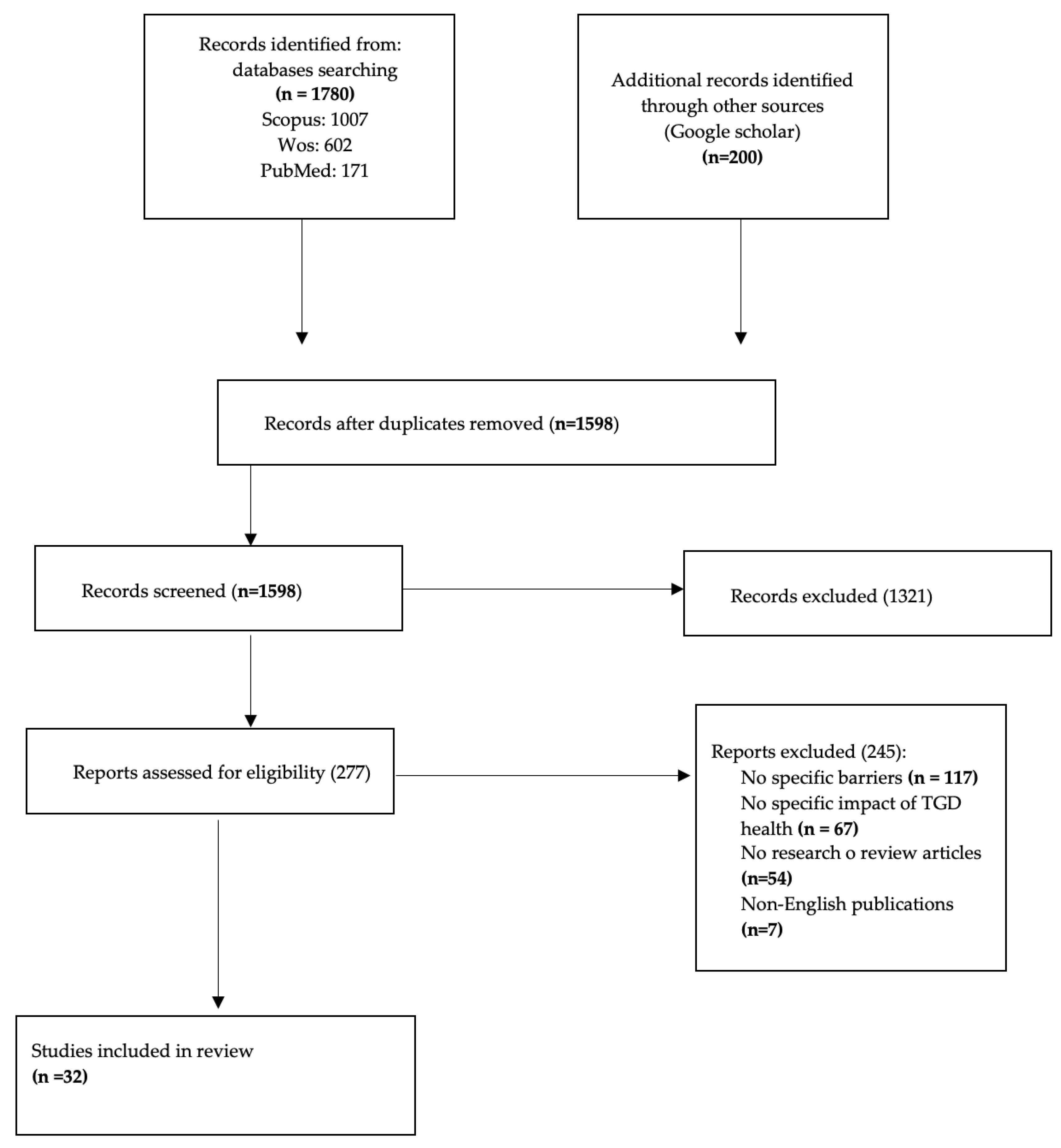
2.5. Study Selection
2.6. Data Extraction and Synthesis
2.7. Quality Assessment
3. Results
3.1. Selected Studies
3.2. General Characteristics of the Included Studies
3.3. Temporal Extension of the Included Studies
3.4. Journal Distribution of the Included Studies and Their Research Areas
3.5. Geospatial Distribution of the Included Studies
3.6. Barriers Extracted from the Included Papers
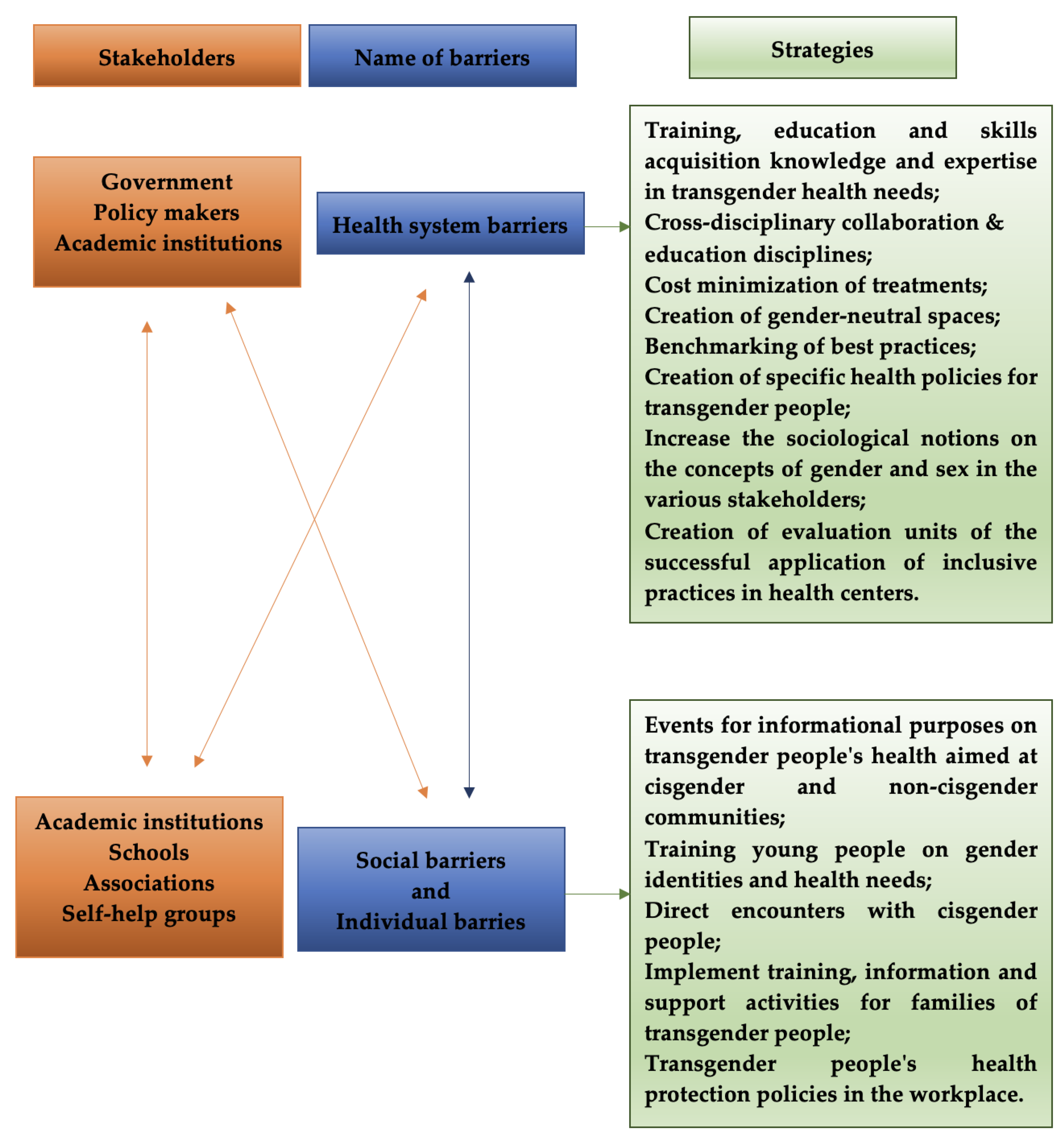
3.7. Macrolevel: Health System Barriers
Structural Barriers
3.8. Mesolevel: Social Barriers
3.9. Microlevel: Individual Barriers
3.10. The Point of View from Which the Barriers Were Detected
3.11. The Methods and the Research Instruments Used to Study the Barriers
4. Discussion
4.1. Barriers to Health Care: An Overview
4.2. The Relationships between the Different Levels of Barriers and Their Health Implications
4.3. Countries of Included Studies
4.4. Barriers, Transgender People and Public Health
4.5. Strengths and Limitations of the Research
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baqutayan, S.M.; Mahdzir, A.M.; Yusof, N.A.M.; Saimy, I.S.; Salleh, S.H. Public opinions and gender issue. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5215–5227. [Google Scholar] [PubMed]
- Meyer, I.H.; Northridge, M.E. The Health of Sexual Minorities: Public Health Perspectives on Lesbian, Gay, Bisexual and Transgender Populations; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Costa, D. The influence of social capital on health issues among transgender and gender diverse people: A rapid review. Sci. Philos. 2022, 10, 109–131. [Google Scholar]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef] [PubMed]
- HWB. Unit 1—Health, Social Services and Children Services; Access and Barriers, United Kingdom, ND. Available online: http://resources.hwb.wales.gov.uk/VTC/2012-13/22032013/hsc/eng/unit_1/u1-a-and-b/u1-a-and-b1.htm (accessed on 1 February 2023).
- Bockting, W.O.; Miner, M.H.; Swinburne Romine, R.E.; Hamilton, A.; Coleman, E. Stigma, mental health, and resilience in an online sample of the US transgender population. Am. J. Public Health 2013, 103, 943–951. [Google Scholar] [CrossRef]
- Reisner, S.L.; Poteat, T.; Keatley, J.; Cabral, M.; Mothopeng, T.; Dunham, E.; Baral, S.D. Global health burden and needs of transgender populations: A review. Lancet 2016, 388, 412–436. [Google Scholar] [CrossRef]
- Stroumsa, D. The state of transgender health care: Policy, law, and medical frameworks. Am. J. Public Health 2014, 104, e31–e38. [Google Scholar] [CrossRef]
- Douthit, N.; Kiv, S.; Dwolatzky, T.; Biswas, S. Exposing some important barriers to health care access in the rural USA. Public Health 2015, 129, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Snelgrove, J.W.; Jasudavisius, A.M.; Rowe, B.W.; Head, E.M.; Bauer, G.R. “Completely out-at-sea” with “two-gender medicine”: A qualitative analysis of physician-side barriers to providing healthcare for transgender patients. BMC Health Serv. Res. 2012, 12, 1–13. [Google Scholar] [CrossRef]
- Byne, W.; Karasic, D.H.; Coleman, E.; Eyler, A.E.; Kidd, J.D.; Meyer-Bahlburg, H.F.; Pula, J. Gender dysphoria in adults: An overview and primer for psychiatrists. Transgender Health 2018, 3, 57-A3. [Google Scholar] [CrossRef] [PubMed]
- Messinger, A.M.; Guadalupe-Diaz, X.L.; Kurdyla, V. Transgender Polyvictimization in the U.S. Transgender Survey. J. Interpers. Violence 2022, 37, NP18810–NP18836. [Google Scholar] [CrossRef]
- Carrillo, J.E.; Carrillo, V.A.; Perez, H.R.; Salas-Lopez, D.; Natale-Pereira, A.; Byron, A.T. Defining and targeting health care access barriers. J. Health Care Poor Underserved 2011, 22, 562–575. [Google Scholar] [CrossRef]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Bronfenbrenner, U. Ecology of the family as a context for human development: Research perspectives. Dev. Psychol 1986, 22, 723–742. [Google Scholar] [CrossRef]
- Lintott, L.; Beringer, R.; Do, A.; Daudt, H. A rapid review of end-of-life needs in the LGBTQ+ community and recommendations for clinicians. Palliat. Med. 2022, 36, 609–624. [Google Scholar] [CrossRef]
- Edwards, L.; Goodwin, A.; Neumann, M. An ecological framework for transgender inclusive family therapy. Contemp. Fam. Ther. 2019, 41, 258–274. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Haddaway, N.R.; Collins, A.M.; Coughlin, D.; Kirk, S. The Role of Google Scholar in Evidence Reviews and Its Applicability to Grey Literature Searching. PLoS ONE 2015, 10, e0138237. [Google Scholar] [CrossRef]
- Samson, D.; Schoelles, K.M. Medical tests guidance (2) developing the topic and structuring systematic reviews of medical tests: Utility of PICOTS, analytic frameworks, decision trees, and other frameworks. J. Gen. Intern. Med. 2012, 27, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ (Clin. Res. Ed.) 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.P.; Surratt, H.L.; Kiley, M.C.; Inciardi, J.A. Barriers to health and social services for street-based sex workers. J. Health Care Poor Underserved 2005, 16, 345–361. [Google Scholar] [CrossRef] [PubMed]
- Chakrapani, V.; Newman, P.A.; Shunmugam, M.; Dubrow, R. Barriers to free antiretroviral treatment access among kothi-identified men who have sex with men and aravanis (transgender women) in Chennai, India. AIDS Care 2011, 23, 1687–1694. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, E.; Valaitis, R.; Yost, J.; Carter, N.; Risdon, C. Primary care is primary care: Use of Normalization Process Theory to explore the implementation of primary care services for transgender individuals in Ontario. PLoS ONE 2019, 14, e0215873. [Google Scholar] [PubMed]
- Tanner, A.E.; Reboussin, B.A.; Mann, L.; Ma, A.; Song, E.; Alonzo, J.; Rhodes, S.D. Factors influencing health care access perceptions and care-seeking behaviors of immigrant Latino sexual minority men and transgender individuals: Baseline findings from the HOLA intervention study. J. Health Care Poor Underserved 2014, 25, 1679. [Google Scholar] [CrossRef] [PubMed]
- Singh, Y.; Aher, A.; Shaikh, S.; Mehta, S.; Robertson, J.; Chakrapani, V. Gender transition services for Hijras and other male-to-female transgender people in India: Availability and barriers to access and use. Int. J. Transgenderism 2014, 15, 1–15. [Google Scholar] [CrossRef]
- Roberts, T.K.; Fantz, C.R. Barriers to quality health care for the transgender population. Clin. Biochem. 2014, 47, 983–987. [Google Scholar] [CrossRef]
- Shaikh, S.; Mburu, G.; Arumugam, V.; Mattipalli, N.; Aher, A.; Mehta, S.; Robertson, J. Empowering communities and strengthening systems to improve transgender health: Outcomes from the Pehchan programme in India. J. Int. AIDS Soc. 2016, 19, 20809. [Google Scholar] [CrossRef]
- Safer, J.D.; Coleman, E.; Feldman, J.; Garofalo, R.; Hembree, W.; Radix, A.; Sevelius, J. Barriers to healthcare for transgender individuals. Curr. Opin. Endocrinol. Diabetes Obes. 2016, 23, 168–171. [Google Scholar] [CrossRef]
- Tagliamento, G.; Paiva, V. Trans-specific health care: Challenges in the context of new policies for transgender people. J. Homosex. 2016, 63, 1556–1572. [Google Scholar] [CrossRef]
- Szydlowski, M. The rights to health and health care of vulnerable populations: Reducing the existing barriers to health equity experienced by transgender people in Ireland. J. Hum. Rights Pract. 2016, 8, 239–263. [Google Scholar] [CrossRef]
- Vermeir, E.; Jackson, L.A.; Marshall, E.G. Barriers to primary and emergency healthcare for trans adults. Cult. Health Sex. 2018, 20, 232–246. [Google Scholar] [CrossRef]
- Romanelli, M.; Hudson, K.D. Individual and systemic barriers to health care: Perspectives of lesbian, gay, bisexual, and transgender adults. Am. J. Orthopsychiatry 2017, 87, 714–728. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, G.; Henning-Smith, C. Barriers to Care Among Transgender and Gender Nonconforming Adults. Milbank Q. 2017, 95, 726–748. [Google Scholar] [CrossRef]
- Valenta, T.; Shade, K.; Lieggi, M. Experiences of transgender individuals when accessing health care: A qualitative systematic review protocol. JBI Evid. Synth. 2018, 16, 628–634. [Google Scholar] [CrossRef]
- Reback, C.J.; Clark, K.; Holloway, I.W.; Fletcher, J.B. Health disparities, risk behaviors and healthcare utilization among transgender women in Los Angeles County: A comparison from 1998–1999 to 2015–2016. AIDS Behav. 2018, 22, 2524–2533. [Google Scholar] [CrossRef] [PubMed]
- Aylagas-Crespillo, M.; García-Barbero, Ó.; Rodríguez-Martín, B. Barriers in the social and healthcare assistance for transgender persons: A systematic review of qualitative studies. Enfermería Clínica (Engl. Ed.) 2018, 28, 247–259. [Google Scholar] [CrossRef]
- Philbin, M.M.; Hirsch, J.S.; Wilson, P.A.; Ly, A.T.; Giang, L.M.; Parker, R.G. Structural barriers to HIV prevention among men who have sex with men (MSM) in Vietnam: Diversity, stigma, and healthcare access. PLoS ONE 2018, 13, e0195000. [Google Scholar] [CrossRef] [PubMed]
- Luvuno, Z.P.; Ncama, B.; Mchunu, G. Transgender population’s experiences with regard to accessing reproductive health care in Kwazulu-Natal, South Africa: A qualitative study. Afr. J. Prim. Health Care Fam. Med. 2019, 11, 1–9. [Google Scholar] [CrossRef]
- Kcomt, L. Profound health-care discrimination experienced by transgender people: Rapid systematic review. Soc. Work. Health Care 2019, 58, 201–219. [Google Scholar] [CrossRef]
- Luvuno, Z.P.; Mchunu, G.; Ngidi, H.; Ncama, B.; Mashamba-Thompson, T. Evidence of interventions for improving healthcare access for lesbian, gay, bisexual and transgender people in South Africa: A scoping review. Afr. J. Prim. Health Care Fam. Med. 2019, 11, 1–10. [Google Scholar] [CrossRef]
- Lacombe-Duncan, A.; Newman, P.A.; Bauer, G.R.; Logie, C.H.; Persad, Y.; Shokoohi, M.; O’Brien, N.; Kaida, A.; de Pokomandy, A.; Loutfy, M.R. Gender-affirming healthcare experiences and medical transition among transgender women living with HIV: A mixed-methods study. Sex. Health 2019, 16, 367–376. [Google Scholar] [CrossRef]
- Snow, A.; Cerel, J.; Loeffler, D.N.; Flaherty, C. Barriers to mental health care for transgender and gender-nonconforming adults: A systematic literature review. Health Soc. Work. 2019, 44, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Brookfield, S.; Dean, J.; Forrest, C.; Jones, J.; Fitzgerald, L. Barriers to accessing sexual health services for transgender and male sex workers: A systematic qualitative meta-summary. AIDS Behav. 2020, 24, 682–696. [Google Scholar] [CrossRef] [PubMed]
- Watson, C.W.M.; Pasipanodya, E.; Savin, M.J.; Ellorin, E.E.; Corado, K.C.; Flynn, R.P.; Opalo, C.; Lampley, E.K.; Henry, B.L.; Blumenthal, J.; et al. Barriers and facilitators to PrEP initiation and adherence among transgender and gender non-binary individuals in Southern California. AIDS Educ. Prev. 2020, 32, 472–485. [Google Scholar] [CrossRef]
- Kcomt, L.; Gorey, K.M.; Barrett, B.J.; McCabe, S.E. Healthcare avoidance due to anticipated discrimination among transgender people: A call to create trans-affirmative environments. SSM Popul. Health 2020, 11, 100608. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, E.; Valaitis, R.; Carter, N.; Risdon, C.; Yost, J. Primary care for transgender individuals: A review of the literature reflecting a Canadian perspective. SAGE Open 2020, 10, 2158244020962824. [Google Scholar] [CrossRef]
- Bakko, M.; Kattari, S.K. Transgender-Related Insurance Denials as Barriers to Transgender Healthcare: Differences in Experience by Insurance Type. J. Gen. Intern. Med. 2020, 35, 1693–1700. [Google Scholar] [CrossRef]
- Kattari, S.K.; Bakko, M.; Hecht, H.K.; Kinney, M.K. Intersecting Experiences of Healthcare Denials among Transgender and Nonbinary Patients. Am. J. Prev. Med. 2020, 58, 506–513. [Google Scholar] [CrossRef]
- Kattari, S.K.; Call, J.; Holloway, B.T.; Kattari, L.; Seelman, K.L. Exploring the Experiences of Transgender and Gender Diverse Adults in Accessing a Trans Knowledgeable Primary Care Physician. Int. J. Environ. Res. Public Health 2021, 18, 13057. [Google Scholar] [CrossRef] [PubMed]
- Kattari, S.K.; Bakko, M.; Langenderfer-Magruder, L.; Holloway, B.T. Transgender and Nonbinary Experiences of Victimization in Health care. J. Interpers. Violence 2021, 36, NP13054–NP13076. [Google Scholar] [CrossRef]
- She, R.; Mo, P.K.; Cai, Y.; Ma, T.; Liu, Y.; Lau, J.T. Mental health service utilisation among transgender women and sex workers who are at risk of mental health problems in Shenyang, China: An application of minority stress theory. Health Soc. Care Community 2022, 30, e981–e993. [Google Scholar] [CrossRef]
- Gagnon, K.W.; Bifulco, L.; Robinson, S.; Furness, B.; Lentine, D.; Anderson, D. Qualitative inquiry into barriers and facilitators to transforming primary care for lesbian, gay, bisexual and transgender people in US federally qualified health centres. BMJ Open 2022, 12, e055884. [Google Scholar] [CrossRef] [PubMed]
- Serpa, S.; Ferreira, C.M. Micro, meso and macro levels of social analysis. Int. J. Soc. Sci. Stud. 2019, 7, 120. [Google Scholar] [CrossRef]
- Koehler, A.; Strauss, B.; Briken, P.; Szuecs, D.; Nieder, T.O. Centralized and decentralized delivery of transgender health care services: A systematic review and a global expert survey in 39 countries. Front. Endocrinol. 2021, 12, 717914. [Google Scholar] [CrossRef] [PubMed]
- White Hughto, J.M.; Reisner, S.L.; Pachankis, J.E. Transgender stigma and health: A critical review of stigma determinants, mechanisms, and interventions. Soc. Sci. Med. 2015, 147, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.; Kirby, L.; Booth, A.; Klepper, M.; Sherman, A.D.; Bower, K.M.; Wright, E.M. Providing gender affirming and inclusive care to transgender men experiencing pregnancy. Midwifery 2023, 116, 103550. [Google Scholar] [CrossRef]
- Garcia, J.; Crosby, R.A. Social determinants of discrimination and access to health care among transgender women in Oregon. Transgender Health 2020, 5, 225–233. [Google Scholar] [CrossRef]
- Hill, B.J.; Crosby, R.; Bouris, A.; Brown, R.N.; Bak, T.; Rosentel, K.; VandeVusse, A.; Silverman, M.; Salazar, L.F. Exploring transgender legal name change as a potential structural intervention for mitigating social determinants of health among transgender women of color. Sex. Res. Soc. Policy 2018, 15, 25–33. [Google Scholar] [CrossRef]
- Garcia, J.; Vargas, N.; Clark, J.L.; Magaña Álvarez, M.; Nelons, D.; Parker, R.G. Social isolation and connectedness as determinants of well-being: Global evidence mapping focused on LGBTQ youth. Glob. Public Health 2020, 15, 497–519. [Google Scholar] [CrossRef]
- Schilt, K.; Lagos, D. The development of transgender studies in sociology. Annu. Rev. Sociol. 2017, 43, 425–443. [Google Scholar] [CrossRef]
- Kidd, S.A.; Veltman, A.; Gately, C.; Chan, K.J.; Cohen, J.N. Lesbian, gay, and transgender persons with severe mental illness: Negotiating wellness in the context of multiple sources of stigma. Am. J. Psychiatr. Rehabil. 2011, 14, 13–39. [Google Scholar] [CrossRef]
- Latorre, R.A.; Endman, M.; Gossmann, I. Androgyny and need achievement in male and female psychiatric inpatients. J. Clin. Psychol. 1976, 32, 233–235. [Google Scholar] [CrossRef]
- Crenshaw, K. Demarginalizing the intersection of race and sex: A black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. Univ. Chicago Legal Forum 1989, 140, 139–167. [Google Scholar]
- Moradi, B. (Re)focusing intersectionality: From social identities back to systems of oppression and privilege. In Handbook of Sexual Orientation & Gender Diversity in Counseling and Psychotherapy; DeBord, K.A., Fischer, A.R., Bieschke, K.J., Perez, R.M., Eds.; APA: Seattle, WA, USA, 2017; pp. 105–127. [Google Scholar]
- Blumer, M.L.C.; Ansara, Y.G.; Watson, C.M. Cisgenderism in family Therapy: How everyday clinical practices can delegitimize people’s gender self-designations. J. Fam. Psychother. 2013, 24, 267–285. [Google Scholar] [CrossRef]
- Radix, A.E.; Lelutiu-Weinberger, C.; Gamarel, K.E. Satisfaction and healthcare utilization of transgender and gender nonconforming individuals in NYC: A community-based participatory study. LGBT Health 2014, 1, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Sperber, J.; Landers, S.; Lawrence, S. Access to health care for transgendered persons: Results of a needs assessment in Boston. Int. J. Transgenderism 2005, 8, 75–91. [Google Scholar] [CrossRef]
- Roller, C.G.; Sedlak, C.; Draucker, C.B. Navigating the system: How transgender individuals engage in health care services. J. Nurs. Scholarsh. 2015, 47, 417–424. [Google Scholar] [CrossRef]
- deHaan, G.; Santos, G.; Arayasirikul, S.; Raymond, H.F. Non-prescribed hormone use and barriers to care for transgender women in San Francisco. LGBT Health 2015, 2, 313–323. [Google Scholar] [CrossRef]
- Khobzi Rotondi, N.; Bauer, G.R.; Scanlon, K.; Kaay, M.; Travers, R.; Travers, A. Nonprescribed hormone use and self-performed surgeries: ‘Do-it-yourself’ transitions in transgender communities in Ontario, Canada. Am. J. Public Health 2013, 103, 1830–1836. [Google Scholar] [CrossRef]
- Aguirre-Sánchez-Beato, S. Trans Terminology and Definitions in Research on Transphobia: A conceptual review. Quad. Psicologia 2018, 20, 295–305. [Google Scholar] [CrossRef]
- Fiorilli, O.; Ruocco, A. Psychosocial issues in transgender health and barriers to healthcare. Ital. J. Gend. Specif. Med. 2019, 5, 123–130. [Google Scholar]
- McGowan, E.; Sanders, S.; Iwatsubo, T.; Takeuchi, A.; Saido, T.; Zehr, C.; Yu, X.; Uljon, S.; Wang, R.; Mann, D.M.; et al. Amyloid phenotype characterization of transgenic mice overexpressing both mutant amyloid precursor protein and mutant presenilin 1 transgenes. Neurobiol. Dis. 1999, 6, 231–244. [Google Scholar] [CrossRef]
- Scandurra, C.; Amodeo, A.L.; Valerio, P.; Bochicchio, V.; Frost, D.M. Minority stress, resilience, and mental health: A study of Italian transgender people. J. Soc. Issues 2017, 73, 563–585. [Google Scholar] [CrossRef]
- Kattari, S.K.; Bakko, M.; Hecht, H.K.; Kattari, L. Correlations between healthcare provider interactions and mental health among transgender and nonbinary adults. SSM Popul. Health 2019, 10, 100525. [Google Scholar] [CrossRef]
- Lindroth, M. Competent persons who can treat you with competence, as simple as that’—An interview study with transgender people on their experiences of meeting healthcare professionals. J. Clin. Nurs. 2016, 25, 3511–3521. [Google Scholar] [CrossRef]
- Baldwin, A.; Dodge, B.; Schick, V.R.; Light, B.; Scharrs, P.W.; Herbenick, D. Transgender and genderqueer individuals’ experiences with healthcare providers: What’s working, what’s not, and where do we go from here? J. Health Care Poor Underserved 2018, 29, 1300–1318. [Google Scholar] [CrossRef] [PubMed]
- Waldman, R.A.; Waldman, S.D.; Grant-Kels, J.M. The ethics of performing noninvasive, reversible gender-affirming procedures on transgender adolescents. J. Am. Acad. Dermatol. 2018, 79, 1166–1168. [Google Scholar] [CrossRef]
- Plemons, E. A capable surgeon and a willing electrologist: Challenges to the expansion of transgender surgical care in the United States. Med. Anthropol. Anthropol. Q. 2019, 33, 282–301. [Google Scholar] [CrossRef] [PubMed]
- Pandya, A.K.; Redcay, A. Access to health services: Barriers faced by the transgender population in India. J. Gay Lesbian Ment. Health 2021, 25, 132–154. [Google Scholar] [CrossRef]
- Available online: https://www.pewresearch.org/short-reads/2022/06/07/about-5-of-young-adults-in-the-u-s-say-their-gender-is-different-from-their-sex-assigned-at-birth/ft_2022-06-07_transandnbadults_01/ (accessed on 10 May 2023).
- Jobson, G.A.; Theron, L.B.; Kaggwa, J.K.; Kim, H.J. Transgender in Africa: Invisible, inaccessible, or ignored? SAHARA-J. J. Soc. Asp. HIV/AIDS 2012, 9, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Scheim, A.I.; Baker, K.E.; Restar, A.J.; Sell, R.L. Health and health care among transgender adults in the United States. Annu. Rev. Public Health 2022, 43, 503–523. [Google Scholar] [CrossRef]
- Turner, C.M.; Arayasirikul, S.; Wilson, E.C. Disparities in HIV-related risk and socio-economic outcomes among trans women in the sex trade and effects of a targeted, anti-sex-trafficking policy. Soc. Sci. Med. 2021, 270, 113664. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, V.; Verster, A.; Mello, M.B.; Blondeel, K.; Amin, A.; Luhmann, N.; Baggaley, R.; Doherty, M. The World Health Organization’s work and recommendations for improving the health of trans and gender diverse people. J. Int. AIDS Soc. 2022, 25 (Suppl. S5), e26004. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, G.; Tran, N.M.; Bennett, M.A. State Policies and Health Disparities between Transgender and Cisgender Adults: Considerations and Challenges Using Population-Based Survey Data. J. Health Politics Policy Law 2022, 47, 555–581. [Google Scholar] [CrossRef]
- Carpenter, L.F.; Marshall, R.B. Walking while trans: Profiling of transgender women by law enforcement, and the problem of proof. Wm. Mary J. Women Law 2017, 24, 5. [Google Scholar]
- Sirufo, M.M.; Magnanimi, L.M.; Ginaldi, L.; De Martinis, M. Barriers to inclusive healthcare for transgender people. Eur. J. Radiol. 2022, 153, 110367. [Google Scholar] [CrossRef]
- Divan, V.; Cortez, C.; Smelyanskaya, M.; Keatley, J. Transgender social inclusion and equality: A pivotal path to development. J. Int. AIDS Soc. 2016, 19 (Suppl. S2), 20803. [Google Scholar] [CrossRef]
- Asadi, M.; Tabari, F.; Haghani, S.; Heidari, M.E. The impact of empowerment model-based education on quality of life of transgender people under hormone therapy: A randomized clinical trial. J. Fam. Med. Prim. Care 2020, 9, 2794–2800. [Google Scholar]
- Shin, S.; Park, H. Effect of empowerment on the quality of life of the survivors of breast cancer: The moderating effect of self-help group participation. Jpn. J. Nurs. Sci. 2017, 14, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Castro-Peraza, M.E.; García-Acosta, J.M.; Delgado, N.; Perdomo-Hernández, A.M.; Sosa-Alvarez, M.I.; Llabrés-Solé, R.; Lorenzo-Rocha, N.D. Gender Identity: The Human Right of Depathologization. Int. J. Environ. Res. Public Health 2019, 16, 978. [Google Scholar]
- Costa, D. Diversity and Health: Two Sides of the Same Coin. Ital. Sociol. Rev. 2023, 13, 69–90. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Keywords | Scopus | Web Of Science | PubMed |
|---|---|---|---|
| Transgender AND barrier * AND health * | 1298 | 1802 | 1168 |
| Transgender AND health service * | 3156 | 3353 | 3934 |
| Transgender AND accessibility AND health service * | 630 | 85 | 1377 |
| Transgender AND disparity AND health service * | 565 | 559 | 667 |
| Transgender AND health system * | 1427 | 1688 | 1323 |
| Parameter | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Source | Studies that investigated the barriers to health care for transgender people | Studies not focused on the barriers to health for transgender people |
| Intervention | Explores the presence of barriers classified in specific and nongeneric typologies. Explores the presence of a specific nomenclature of barriers. | Only whether barriers are mentioned in a generic way without any categorization. |
| Comparator | None | None |
| Outcomes | Provides a punctual and specific definition of the barriers in order to be able to propose a specific framework and/or any suggestions. | Models, papers or tools not focused on barriers or in any case devoid of practical effects on the health of transgender people |
| Timeframe | Unrestricted (final extraction: February 2023) | Unrestricted (final extraction: February 2023) |
| Study Type | Research articles and review articles published in peer-reviewed journals | Book chapters, book reviews, vignette studies, supplements, study protocols, commentaries, guidelines, editorials, book, meeting abstract, letter to editors |
| Language | English | Non-English |
| Authors | Title | Year | Country | Methods/Study Design | Population | Study Content | Types of Barriers |
|---|---|---|---|---|---|---|---|
| 1. Kurtz P.S. et al. [24] | Barriers to Health and Social Services for Street-Based Sex Workers | 2005 | United States | Qualitative study using an interview and focus group | Sex workers Transgender, women, etc. (n = 611) | To examine the service needs and associated barriers to access among sex workers | Structural barriers; Individual barriers |
| 2.Chakrapani V. et al. [25] | Barriers to free antiretroviral treatment access among kothi-identified men who have sex with men and aravanis (transgender women) in Chennai, India | 2011 | India | Qualitative study using an interview and focus group | Kothi (n = 17) | To identify and understand barriers faced by these marginalized groups in accessing free antiretroviral treatment in government treatment centers | Family/ social-level barriers; Health care system barriers; Individual level barriers |
| 3. Snelgrove J.W. et al. [26] | “Completely out-at-sea” with “two-gender medicine”: A qualitative analysis of physician-side barriers to providing healthcare for transgender patients | 2012 | United States | Qualitative study using semi- structured interviews | Physician (n = 13) | To examine physician perceptions of barriers to health care provision for transgender patients | Health care barriers |
| 4. Tanner A.E. et al. [27] | Factors influencing health care access perceptions and care-seeking behaviors of immigrant Latino sexual minority men and transgender individuals: Baseline findings from the HOLA intervention study | 2014 | United States | Quantitative study using a survey | Latino sexual minority men and transgender individuals (n = 180) | To examine factors associated with perceptions of access and actual care behaviors among this population in North Carolina | Macrostructural barriers; Mesostructural barriers; Microstructural barriers |
| 5. Singh Y. et al. [28] | Gender Transition Services for Hijras and Other Male-to-Female Transgender People in India: Availability and Barriers to Access and Use | 2014 | India | Qualitative study using using a focus group, in-depth interviews and informant interviews | Hijras/ Transgender people and service providers (n = 94) | To explore access to and use of gender transition services by hijras and other male-to-female transgender people in the public and private hospitals in seven Indian cities | Systemic barriers; Community barriers; Personal barriers |
| 6. Roberts T.K. and Fantz C.R. [29] | Barriers to quality health care for the transgender population | 2014 | United States | Review | NA | To explore the literature on barriers | Structural barriers; Financial barriers |
| 7. Shaikh S. et al. [30] | Empowering communities and strengthening systems to improve transgender health: outcomes from the Pehchan programme in India | 2016 | India | Quantitative study using a cross- sectional survey | Transgender people (n = 268) | To strengthen community systems and provide HIV, health, legal and social services to transgender communities across 18 Indian states through a rights-based empowerment approach | Structural barriers; Social barriers |
| 8. Safer J.D. et al. [31] | Barriers to healthcare for transgender individuals | 2016 | United States | Review | NA | To briefly review the literature characterizing barriers to health care for transgender individuals and to propose research priorities to understand the mechanisms of those barriers and interventions to overcome them | Direct barriers; Indirect barriers; Health care barriers; Financial barriers; Structural barriers; Social barriers. |
| 9. Tagliamento G. and Paiva, V. [32] | Trans-Specific Healthcare: Challenges in the Context of New Policies for Transgender People | 2016 | Brazil | Qualitative study using an interview and direct participant observation | 23 transgender people | To understand transgender peoples’ access to the Brazilian public health care system in light of the new public policies for this group in Brazil | Programmatic barriers |
| 10. Szydlowski M. [33] | The Rights to Health and Health Care of Vulnerable Populations: Reducing the Existing Barriers to Health Equity Experienced by Transgender People in Ireland | 2016 | Ireland | Review | NA | To explore the existing barriers that Irish transgender people encounter while accessing medical care and to identify potential measures to minimize their negative impact | Direct barriers; Indirect barriers |
| 11. Vermeir E. et al. [34] | Barriers to primary and emergency healthcare for trans adults | 2017 | United States | Qualitative study using an interview | Adult transgender people (n = 8) | To explore the barriers trans adults encounter when pursuing primary and emergency care in Nova Scotia | Interpersonal barriers; Physical barriers; Environment barriers |
| 12. Romanelli M. et al. [35] | Individual and systemic barriers to health care: Perspectives of lesbian, gay, bisexual, and transgender adults. | 2017 | United States | Qualitative study using an interview | Transgender People (40) | To explore the systematic and individual barriers to health care | Individual barriers; Systematic barriers |
| 13. Gonzales G. et al. [36] | Barriers to Care Among Transgender and Gender Nonconforming Adults | 2017 | United Stated | Quantitative study using a survey | Transgender people (1173) | To compared barriers to care among cisgender, transgender and gender nonconforming (GNC) adults using data from a large, multistate sample | Health care barriers |
| 14. Valenta T. et al. [37] | Experiences of transgender individuals when accessing health care: a qualitative systematic review protocol | 2018 | United States | Review | NA | To synthesize existing qualitative literature examining the experiences of transgender individuals when accessing health care | Structural barriers |
| 15. Reback C.J. et al. [38] | Health Disparities, Risk Behaviors and Healthcare Utilization Among Transgender Women in Los Angeles County: A Comparison from 1998–1999 to 2015–2016 | 2018 | United States | Quantitative study using a survey | Transgender women (n = 515) | To compare how structural determinants of health, HIV prevalence, HIV risk behaviors, substance use, gender confirmation procedures and perceived discrimination and harassment/abuse differed across a 17-year period | Structural barriers |
| 16. Aylagas-Crespillo M. et al. [39] | Barriers to social and healthcare assistance for transgender persons: A systematic review of qualitative studies | 2018 | Spain | Review | NA | To explore the barriers to requesting social and health care assistance perceived by transgender persons and professionals involved in the assistance | Individual barriers; Organizational barriers; Barriers at the community level; Barriers at the political level |
| 17. Philbin M.M. et al. [40] | Structural barriers to HIV prevention among men who have sex with men (MSM) in Vietnam: Diversity, stigma, and healthcare access | 2018 | Thailand | Qualitative study using an in-depth interview and focus group | Transgender people (n = 63) | To explore three key structural issues, i.e., diversity, stigma and access to health care services, in order to lay the groundwork for raising questions that are crucial to consider for the successful implementation of HIV prevention among transgender people in Vietnam and elsewhere in the region | Structural barriers |
| 18. Luvuno Z.P. et al. [41] | Transgender population’s experiences with regard to Accessing reproductive health care in Kwazulu-Natal, South Africa: A qualitative study | 2019 | Africa | Qualitative study using an interview | Transgender people (n = 9) | To examine the experiences of the transgender population in accessing health care facilities for sexual and reproductive needs | Structural barriers; Systemic barriers |
| 19. Kcomt L. [42] | Profound health-care discrimination experienced by transgender people: rapid systematic review | 2019 | United States | Review | NA | To explore the prevalence of health care discrimination among transgender people in the U.S. and draw comparisons with sexual minority samples and the general U.S. population | Health care barriers |
| 20. Luvuno Z.P. et al. [43] | Evidence of interventions for improving healthcare access for lesbian, gay, bisexual, and transgender people in South Africa: A scoping review | 2019 | Africa | Review | NA | To provide an overview of documented evidence on South African interventions aimed at improving health care access for LGBT individuals using a systematic scoping review | Structural barriers; Systemic barriers |
| 21. Lacombe-Duncan A. et al. [44] | Gender-affirmed healthcare experiences and medical transition among transgender women living with HIV: a mixed-methods study | 2019 | United States | Mixed methods using a cross- sectional survey and semi- structured interview | Transgender people (n = 59) | To describe barriers and facilitators to access to medical transition among transgender people | Structural barriers; Interpersonal barriers; Institutional barriers |
| 22. Snow A. et al. [45] | Barriers to Mental Health Care for Transgender and Gender-Nonconforming Adults: A Systematic Literature Review | 2019 | United States | Review | NA | To explore obstacles to transgender people mental health care | Psychotherapeutic barriers |
| 23. Brookfield S. et al. [46] | Barriers to Accessing Sexual Health Services for Transgender and Male Sex Workers: A Systematic Qualitative Meta-summary | 2020 | Australia | Review | NA | To appraise and summarize the qualitative literature regarding barriers to health care for transgender people | Structural barriers |
| 24. Watson C.W.M. et al. [47] | Barriers and facilitators to prep initiation and adherence among transgender and gender non-binary individuals in southern California | 2020 | United States | Qualitative study using a focus group | Transgender and nonbinary people (n = 37) | To explore pre-exposure prophylaxis awareness and identify trans-specific perceived barriers and facilitators of pre-exposure prophylaxis uptake | Structural barriers |
| 25. Kcomt L. et al. [48] | Healthcare avoidance due to anticipated discrimination among transgender people: A call to create trans-affirmative environments | 2020 | United States | Quantitative study using a survey | Transgender people (n= 19,157) | To explore avoidance of health care due to anticipated discrimination among transgender adults | Interpersonal barriers; Structural barriers |
| 26. Ziegler E. et al. [49] | Primary Care for Transgender Individuals: A Review of the Literature Reflecting a Canadian Perspective | 2020 | United States | Review | NA | To understand the primary-care needs and access to health care services for transgender adults in Canada | Organizational barriers |
| 27. Bakko M. et al. [50] | Transgender-Related Insurance Denials as Barriers to Transgender Healthcare: Differences in Experience by Insurance Type. | 2020 | United States | Quantitative study using a survey | Transgender and nonbinary people (11,320) | To investigates the association between transgender and nonbinary individuals’ experiences of different forms of transgender-related insurance denial and insurance types | Financial barriers |
| 28. Kattari S.K. et al. [51] | Intersecting Experiences of Healthcare Denial Among Transgender and Nonbinary Patients | 2020 | United States | Quantitative study using a survey | Transgender people (27,715) | To explore lack of evidence on how health care denials vary by gender identity and other intersecting identity characteristics in transgender and nonbinary populations | Health care barriers; Structural barriers; Policy barriers |
| 29. Kattari S.K. et al. [52] | Exploring the Experiences of Transgender and Gender Diverse Adults in Accessing a Trans Knowledgeable Primary Care Physician | 2021 | United States | Quantitative study using a survey | Transgender people (27,715) | To understand differences within the transgender population regarding having seen a doctor, having a primary care provider and having a primary care provider who is knowledgeable about trans health | Health care barriers; Financial barriers |
| 30. Kattari S.K. et al. [53] | Transgender and Nonbinary Experiences of Victimization in Health care. | 2021 | United States | Quantitative study using a survey | Transgender and nonbinary people | To explore the experience high rates of myriad types of victimization, including in health care settings | Health care barriers |
| 31. She R. et al. [54] | Mental health service utilisation among transgender women and sex workers who are at risk of mental health problems in Shenyang, China: An application of minority stress theory | 2022 | China | Quantitative study using a cross-sectional survey | Transgender people (n = 235) | To explore the factors of mental health service utilization behavior and related behavioral intention among TGSWs who were at risk of mental health problems in the past year | Internal barriers; External barriers |
| 32. Gagnon K. et al. [55] | Qualitative inquiry into barriers and facilitators to transform primary care for lesbian, gay, bisexual, and transgender people in US federally qualified health centres | 2022 | United States | Cross-sectional qualitative content analysis | Service providers (n = 40) | To explore barriers and facilitators that arose during an initiative to improve care for transgender patients in federally qualified health centers from the perspectives of staff | Institutional barriers |
| Name of Journal | Number of Articles | Research Areas |
|---|---|---|
| African journal of primary health care & family medicine | 2 | Good health and well-being; Goal Gender equality; Reduced Inequalities; Health Policy/legislation and jurisprudence; Health Services Accessibility; Sexual and Gender Minorities |
| Aids and behavior | 2 | Public, Environmental and Occupational Health; Biomedical Social Sciences |
| Aids care | 1 | Health Care Sciences and Services; Public, Environmental and Occupational Health; Psychology; Respiratory System; Biomedical Social Sciences |
| American Journal of Orthopsychiatry | 1 | Psychiatry; Social Work |
| American Journal of Preventive Medicine | 1 | Public, Environmental and Occupational Health; General and Internal Medicine |
| Aids education and prevention | 1 | Education and Educational Research; Public, Environmental and Occupational Health |
| BMC health services research | 1 | Health Care Sciences and Services |
| BMJ Open | 1 | Health Care Sciences and Services |
| Clinical biochemistry | 1 | Medical Laboratory Technology |
| Culture health & sexuality | 1 | Family Studies; Biomedical Social Sciences |
| Current Opinion in Endocrinology, Diabetes and Obesity | 1 | Gender and Sexuality Studies |
| Enfermeria clinica | 1 | Nursing |
| Health & social care in the community | 1 | Public, Environmental and Occupational Health; Social Work |
| Health & social work | 1 | Social Work |
| International Journal of Environmental Research and Public Health | 1 | Environmental Sciences and Ecology; Public, Environmental and Occupational Health |
| International journal of transgenderism | 1 | Sexuality and Health |
| JBI database of systematic reviews and implementation reports | 1 | Health Services Accessibility; Psychology |
| Journal of General Internal Medicine | 1 | Health Care Sciences and Services; General and Internal Medicine |
| Journal of health care for the poor and underserved | 2 | Health Services Accessibility; Sex Work; Social work; Health Care Sciences and Services; Public, Environmental and Occupational Health |
| Journal of homosexuality | 1 | Psychology; Social Sciences—Other Topics |
| Journal of human rights practice | 1 | International Relations; Government and Law |
| Journal of interpesonal violence | 1 | Criminology and Penology; Family Studies; Psychology |
| Journal of the international aids society | 1 | Immunology; Infectious Diseases |
| Milbank Quarterly | 1 | Health Care Sciences and Services |
| Plos one | 1 | Science and Technology—Other Topics |
| Sage Open | 1 | Social Sciences—Other Topics |
| Sexual health | 1 | Public, Environmental and Occupational Health; Infectious Diseases |
| Social science & Medicine-Population Health | 1 | Public, Environmental and Occupational Health |
| Public, Environmental & Occupational Health | 1 | Social Work |
| Authors | Definition |
|---|---|
| Internal barriers concern for confidentiality; fear of discrimination; feeling that the treatment is useless; thinking that the symptoms will go away; fear of treatment. External barriers: cost concern; lack of access to qualified doctors; lack of time; negative experience of mental health services. |
| Structural barriers concern discrimination from health care providers; lack of trans-inclusive services; mental health; struggles that limit the ability to access health services and concerns about the potential side of effects of drug interactions with hormone therapy and lack of services; protection from sexually transmitted diseases. | |
| Organizational barriers concern of a lack of transgender-friendly spaces; gender-neutral spaces and toilets; gender documentation in electronic health records, and inappropriate reference ranges for laboratory systems; the lack of policies for welcoming transgender individuals and lack of training of health professionals in this regard. |
| Structural barriers failure of the health care system to provide an inclusive environment, such as unisex bathrooms and appropriate arrangements for inpatient transgender patients. Systemic barriers include erasure through a failure to acknowledge the existence of the transgender population as patients within the health system. This erasure can be passive, through lack of knowledge, data, policies and practice guidelines relating to the transgender population, resulting in a paucity of programmers that cater for transgender patients; however, this erasure can also be active exclusion in the form of hostility and verbal abuse intended to cause discomfort and harm to transgender patients, thereby alienating the transgender population and, eventually, resulting in their avoidance of health care facilities. | |
| Structural access barriers to medical transition generally described among transgender people consist of costs, lack of service availability, stigma, difficulties with the supply of drugs from female hormones to antiretroviral therapy and the lack of information on drug interactions. Interpersonal barriers: transphobia, stigma and nonacceptance. Institutional barriers: lack of knowledge about transgender health. | |
| Individual barriers: health status: being affected by HIV; age: youth in transgender people; perception of refusal declared by transgender people; perception of the lack of rights declared by transgender people; lack of training and skills of professionals. Organizational barriers: lack of information from transgender people about available resources; poor computerized assistance programs. Community barriers: the taboo of being transgender. Barriers at the political level: lack of legal standards, concrete policies, etc. toward the protection and safeguarding of transgender health. |
| Programmatic barriers are due to cultural standards that are difficult to modify; negative stereotypes and stigmas associated with transgender identity, which may lead to discontinuation of ongoing clinical activity treatment. They are related to AIDS and stigmatization and discrimination of transgender people. |
| Direct barriers systematically limit access to certain services through eligibility requirements, medical necessity criteria, prohibitive costs, and restrictions on gender-specific medical services. Indirect barriers, such as stigma and discrimination, can hinder or delay the delivery of care or compromise its quality. |
| Social barriers: experience of high levels of both perceived and internalized social stigma, social isolation, discrimination, and victimization. Extreme social exclusion and lack of acceptance of transgender populations in different settings diminishes their self-esteem and ability to participate in social events. Structural barriers are factors that contribute to poor health and HIV risk among transgender populations. For example, medical training often excludes transgender health and, as a result, health professionals lack the appropriate skills and competencies to provide tailored services to transgender populations |
| Macrolevel barriers: barriers at the health care level, distance from the nearest clinic, lack of transportation and state immigration. Mesolevel barrier: barriers at social level, availability/hours, language, time to get an appointment, too long, previous visit and high cost. Microlevel barriers: barriers at personal level, health insurance status, inability to get permission to work, lack of knowledge on where to get services, concerns about being badly treated, perception of suitability for service health and privacy issues |
| Barriers from the health system: lack of availability of free sex reassignment surgery and hormone therapy in public hospitals; lack of experience among health professionals regarding gender transition services. Policy barriers: lack of national policy/practice guidelines for gender transition; lack of clarity on the legal status of sex reassignment surgery by qualified surgeons. Community level barriers: preference for traditional surgery among some sections of the transgender community; relative nonacceptance of surgeon-performed sex reassignment surgery (involving vagina creation) among some senior transgender gurus, as they disagree with the need for transgender identification by people with a vagina. Personal Barriers: lack of awareness among transgender people about sex reassignment surgery offered by qualified surgeons; inadequate resources to pay for gender transition services, sex reassignment surgery, breast increase and hormone therapy available in private hospitals. |
| Psychotherapeutic barriers compounded by an incongruous financial burden: having to pay to educate their therapist. |
| Family/social-level barriers: lack of family support; discrimination and lack of support within other communities; unmet basic needs. Health care system barriers: negative experiences with health care providers; lack of transgender-friendly registration and admission procedures; inadequate counseling services and lack of confidentiality; perceived lack of focus on antiretroviral treatment in HIV/AIDS interventions. Individual-level barriers: delay in HIV testing; fatalism; insufficient knowledge about antiretroviral treatment and beliefs in alternative cures; alcohol use. |
| Structural barriers such as restroom access; uncomfortable with public restrooms; electronic health records, billing/coding systems and laboratory information systems have implemented a binary male/female identification system; failure to be identified by a preferred name or pronoun can cause discomfort, leading to a poor rapport with providers and impacting quality of care. Financial barriers: insurance issues; disproportionate levels of unemployment within the trans community; individual insurance market, trans identity has long been considered a preexisting condition disqualifying trans persons for coverage; “transition-related care” is excluded by insurance companies. | |
| Health care barriers are grouped into five themes: accessing resources, medical knowledge deficits, ethics of transition-related medical care, diagnosing vs. pathologizing trans patients and health system determinants. | |
| Interpersonal barriers: health care providers with low knowledge and health care providers and their low sensitivity and appropriateness attitudes. Physical environment barriers, such as a lack of gender-neutral washrooms; exclusion of trans-related information in health care settings; feeling that the physical environment within the health care setting was not conducive to privacy; feeling uncomfortable when filling out gender-binary medical forms and identifying these forms as a physical barrier to care. Social environmental barriers: ignoring or being blind to trans identity; barriers to pursuing hormone replacement therapy and mental health care; lack of trans-friendly clinics and resources and incessant experiences of ‘discrimination’ throughout that are simply untrue; fallacious social discourses incorporated into the social environments of health care settings. |
| Structural barriers: availability, information, accessibility; transportation; legal status requirements; social stigma, program staff communication skills; program target population; program structure. Individual barriers: awareness of service, drug seeking and use, street life, distractions/sense of time, mental/emotional stability, fear of arrest, generalized fear, negative attitude, low frustration and tolerance. | |
| Financial barriers: lack of insurance and lack of income); Health care barriers: discrimination, lack of cultural competence by health care providers; Structural barriers: inappropriate electronic records, forms, lab references and clinic facilities; social barriers: transportation, housing and mental health; Direct barriers: lack of insurance coverage along with those that are indirect, such as unfriendly office environments and perceived stigma for both the patients themselves and the providers of transgender health care; Indirect barriers: environment and stigma. |
| Social barriers: forms of victimization, such as 1) the doctor/health care provider used harsh or abusive language, 2) the doctor/health care provider was physically rough or abusive, 3) the patient was verbally harassed in the health care setting and 4) patient experienced unwanted sexual contact in a health care setting; Policy barriers: lack of policy protections against denial of transgender patients; Health care barriers: transphobic discrimination results in elevated rates of denial of care, receipt of substandard care (e.g., rough exams); forced care (e.g., being forced to undergo procedures); Structural barriers: lack of legal documentation discourages transgender patients from seeking appropriate and adequate care. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, D. Transgender Health between Barriers: A Scoping Review and Integrated Strategies. Societies 2023, 13, 125. https://doi.org/10.3390/soc13050125
Costa D. Transgender Health between Barriers: A Scoping Review and Integrated Strategies. Societies. 2023; 13(5):125. https://doi.org/10.3390/soc13050125
Chicago/Turabian StyleCosta, Davide. 2023. "Transgender Health between Barriers: A Scoping Review and Integrated Strategies" Societies 13, no. 5: 125. https://doi.org/10.3390/soc13050125
APA StyleCosta, D. (2023). Transgender Health between Barriers: A Scoping Review and Integrated Strategies. Societies, 13(5), 125. https://doi.org/10.3390/soc13050125