Bioprinting’s Introduction within the Context of the Convention on the Rights of Persons with Disabilities and Malaysia’s Persons with Disabilities Act 2008 through the Right to Science

Abstract
:1. Introduction
2. Literature Review
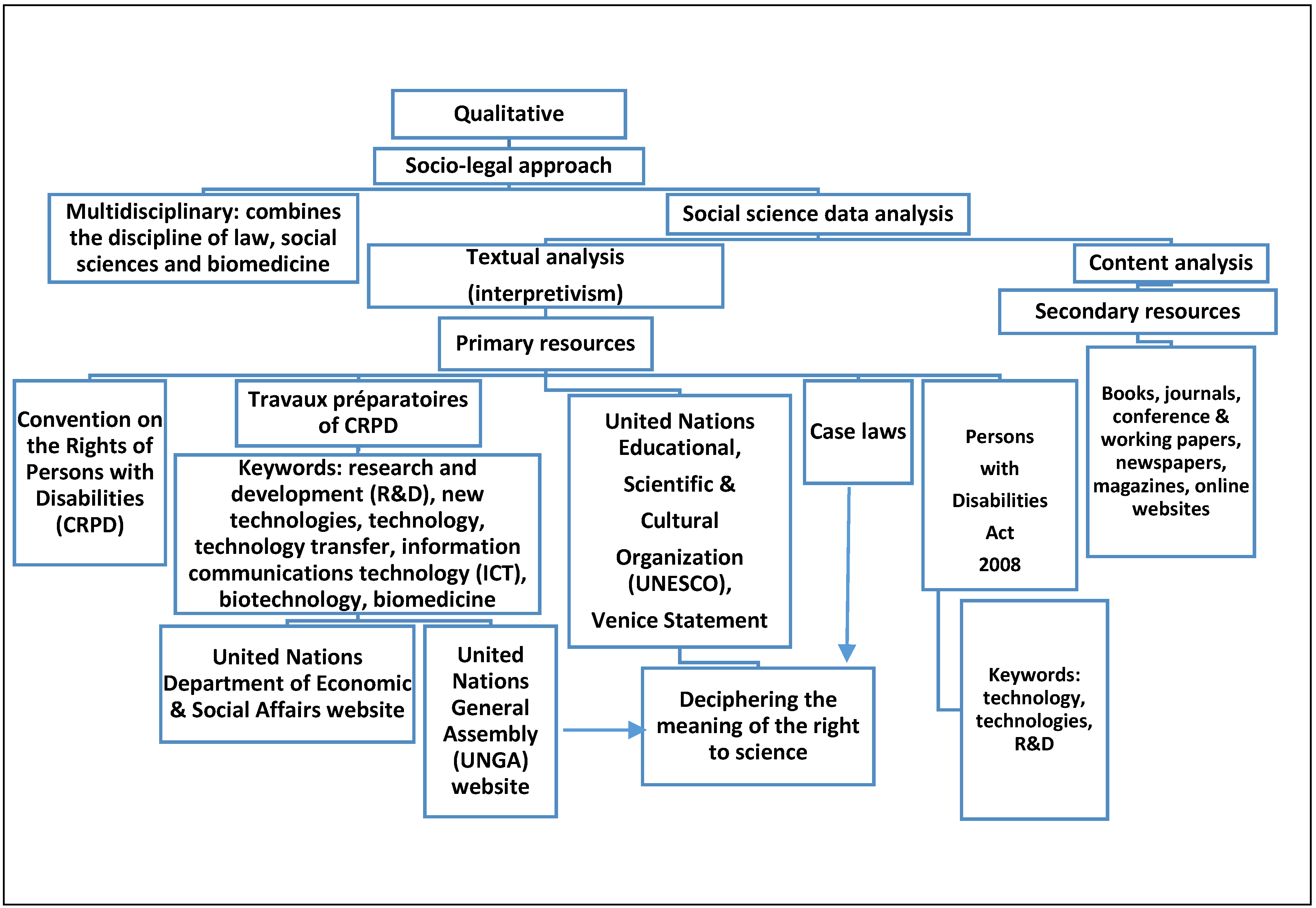
3. Methodology
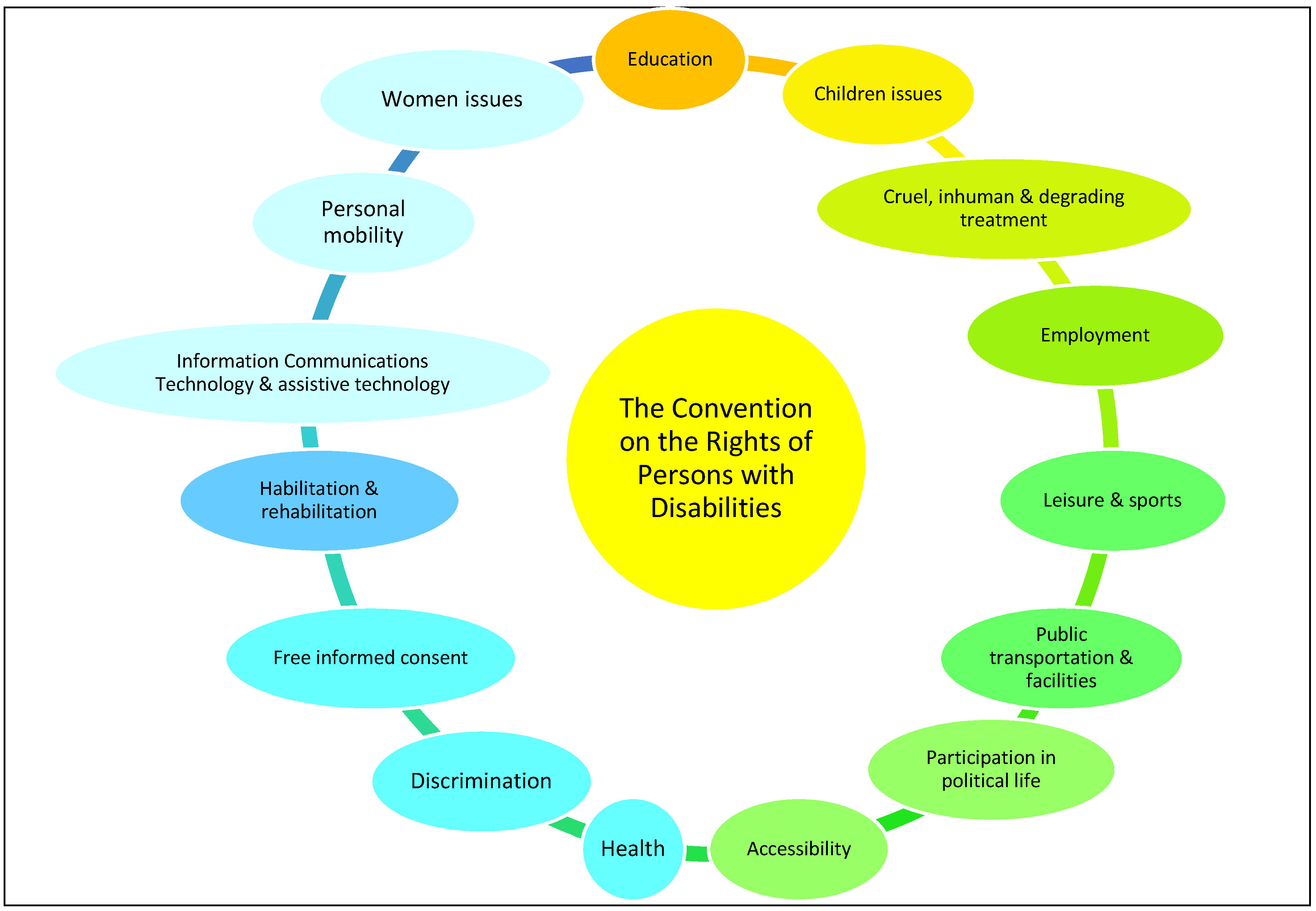
4. Overview of the United Nations Convention on the Rights of Persons with Disabilities (CRPD) and the Scope of Disability
“The purpose of the present Convention is to promote, protect and ensure the full and equal enjoyment of all human rights and fundamental freedoms by all persons with disabilities, and to promote respect for their inherent dignity.”[4]
“Views are divided as to whether it is necessary to define “Disability” and “Persons with disabilities.” I tend to think that we don’t, as this will be very difficult, and there is a risk that we will unintentionally exclude someone.”[25] (p. 3)
“Persons with disabilities include those who have long-term physical, mental, intellectual or sensory impairments which in interaction with various barriers may hinder their full and effective participation in society on an equal basis with others.”[4]
5. Results of the Study
5.1. Provisions on Research and Development (R&D) and New Technologies to Support the Right to Science and Bioprinting within the Convention on the Rights of Persons with Disabilities (CRPD)
“States Parties shall […a]dopt all measures necessary to guarantee that the medical, rehabilitation, and assistance services provided to persons with disabilities include […m]odern medical assistance and treatment that include the use of new technologies.”[30] (p. 128)
“[t]o undertake or promote the research, developments, availability and use of: (ii) New technologies, including information and communication technologies, mobility aids, devices, assistive technologies, suitable for persons with disabilities, giving priority to technologies at an affordable cost.”[32] (p. 10)
“(g) To provide accessible information to persons with disabilities about mobility aids, devices and assistive technologies, including new technologies, as well as other forms of assistance, support services and facilities.”[32] (p. 10)
“To undertake or promote research and development of, and to promote the availability and use of new technologies, including information and communications technologies, mobility aids, devices and assistive technologies, suitable for persons with disabilities, giving priority to technologies at an affordable cost.”[4]
“To provide accessible information to persons with disabilities about mobility aids, devise and assistive technologies, including new technologies, as well as other forms of assistance, support services and facilities.”[4]
5.2. Accorded Rights and Responsibilities with Regard to the Right to Science in the Convention on the Rights of Persons with Disabilities (CRPD)
“States ensure freedom of access to the Internet, promote open access to scientific knowledge and information on the Internet, and take measures to enhance access to computers and Internet connectivity.”[11] (p. 20)
“The right to have access to scientific progress in order to exercise reproductive autonomy and the possibility to found a family gives rise to the right to have access to the best health care services in assisted reproduction techniques, and, consequently, the prohibition of disproportionate and unnecessary restrictions, de iure or de facto, to exercise the reproductive decisions that correspond to each individual.”[37] (p. 46, paragraph 150)
“The relationship between human rights and science is further complicated by the fact that private and non-state actors are increasingly the principal producers of scientific progress and technological advances. It is the responsibility of States to ensure that all relevant interests are balanced, in the advance of scientific progress, in accordance with human rights.”[35] (p. 14)
“States ensure the participation of individuals, communities and peoples in decision-making relating to science in order to […] provide opportunities for all to make informed decision after considering both the possible improvements and potentially harmful side effects or dangerous usages of scientific advances.”[11] (p. 20)
“Developing countries should prioritise the development, importation and dissemination of simple and inexpensive technologies that can improve the life of marginalised populations. Industrialised states should comply with their international legal obligations by means of direct aid and the development of international collaborative models of research and development.”[11] (p. 20)
5.3. Bioprinting Medical Applications for the Benefit of Those with Disabilities
5.4. The Development of Bioprinting in Malaysia
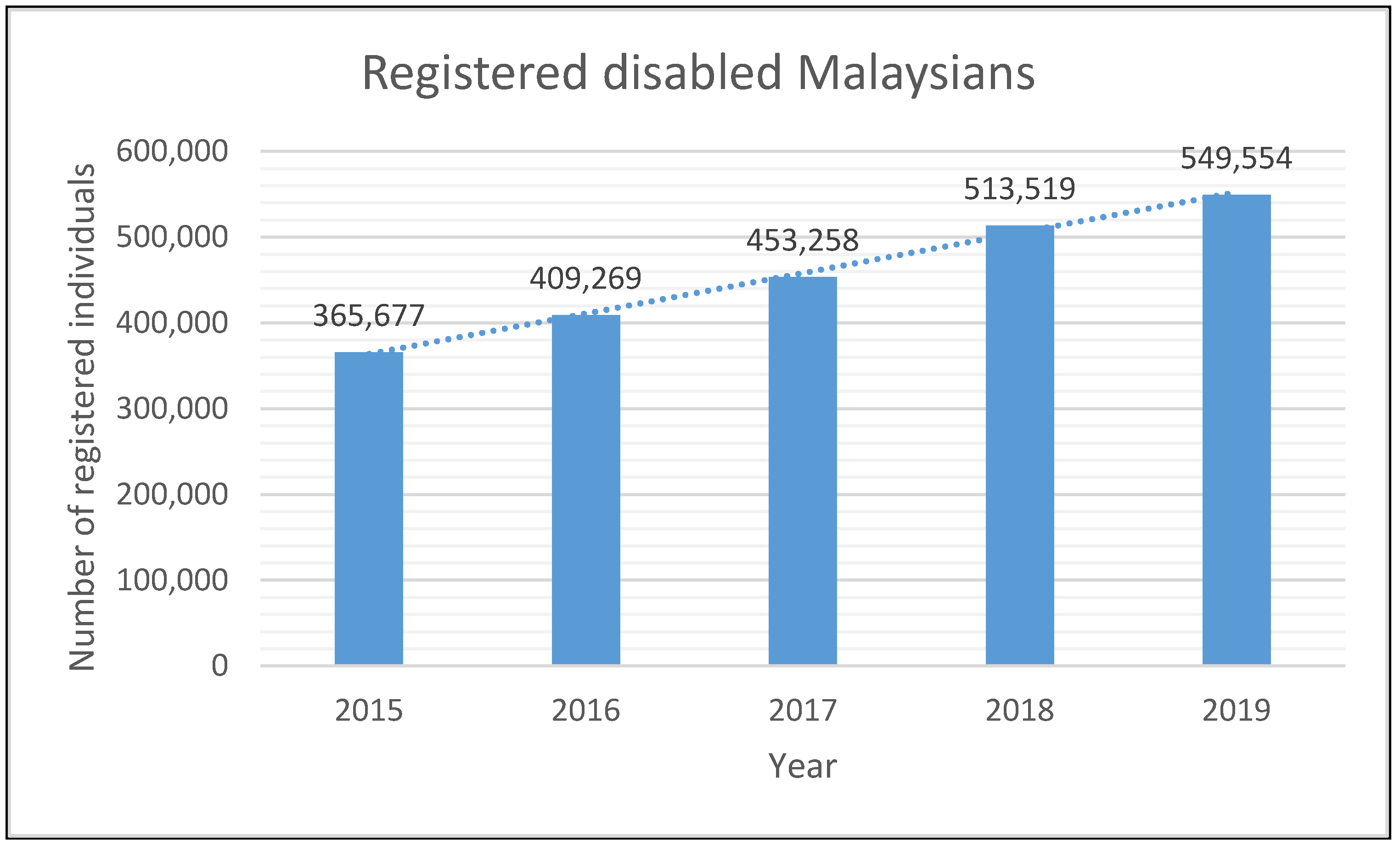
5.5. Malaysia’s Disabled Population
5.6. The Capacity of Malaysia’s Disability Law to Address Research and Development (R&D) and New Technologies
6. Discussion and Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Guillemot, F.; Mironov, V.; Nakamura, M. Bioprinting is Coming of Age: Report from the International Conference on Bioprinting and Biofabrication in Bordeaux (3B’09). Biofabrication 2010, 2, 010201. [Google Scholar] [CrossRef] [PubMed]
- Mori, A.D.; Fernandez, M.P.; Blunn, G.; Tozzi, G.; Roldo, M. 3D Printing and Electrospinning of Composite Hydrogels for Cartilage and Bone Tissue Engineering. Polymers 2018, 10, 285. [Google Scholar]
- Bauermeister, A.J.; Zuriarrain, A.; Newman, M.I. Three-Dimensional Printing in Plastic and Reconstructive Surgery: A Systematic Review. Ann. Plast. Surg. 2016, 77, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Convention on the Rights of Persons with Disabilities. Available online: https://www.un.org/disabilities/documents/convention/convoptprot-e.pdf (accessed on 3 March 2020).
- Persons with Disabilities Act 2008 (Act 685), Malaysia. Available online: http://www.ilo.org/dyn/natlex/docs/ELECTRONIC/86297/117930/F139356912/MYS86297.pdf (accessed on 3 March 2020).
- Consortium of Social Science Associations (COSSA). Science and Human Rights Coalition Focuses on Disability Rights. COSSA Wash. Update 2014, 33, 1–3. [Google Scholar]
- Wolbring, G. ‘Therapeutic’, Enhancement Enabling, Assistive Devices and the UN Convention on the Rights of Persons with Disabilities: A Missing Lens in the Enhancement Regulation Discourse. J. Int. Biotechnol. Law 2009, 6, 193–206. [Google Scholar] [CrossRef]
- Cascio, M.A.; Weiss, J.E.; Racine, E. Empowerment in Decision-Making for Autistic People in Research. Disabil. Soc. 2020, 35, 1–43. [Google Scholar] [CrossRef]
- Bryden, A.; Gran, B. Human Rights, Technology, and Disabilities: The Right to Benefit from Scientific Progress. In Proceedings of the XIX ISA World Congress on Sociology, Toronto, ON, Canada, 15–21 July 2018; International Sociological Association (ISA): Madrid, Spain, 2018; p. 168. [Google Scholar]
- International Covenant on Economic, Social and Cultural Rights. Available online: https://treaties.un.org/doc/Treaties/1976/01/19760103%2009-57%20PM/Ch_IV_03.pdf (accessed on 3 March 2020).
- United Nations General Assembly (UNGA). Report of the Special Rapporteur in the Field of Cultural Rights, Farida Shaheed: The Right to Enjoy the Benefits of Scientific Progress and Its Applications, A/HRC/20/26; UNGA: New York, NY, USA, 2012. [Google Scholar]
- Abegaz, S.T. Marching for 3D Printing: Its Potential to Promoting Access to Healthcare in Africa. In Reflections on Bioethics; Morales-Gonzalez, J.A., Nájera, E.A., Eds.; IntechOpen: London, UK, 2018; pp. 123–135. [Google Scholar]
- Gould, M.; Leblois, A.; Bianchi, F.C.; Montenegro, V. Convention on the Rights of Persons with Disabilities, Assistive Technology and Information and Communication Technology Requirements: Where Do We Stand on Implementation? Disabil. Rehabil. Assist. Technol. 2015, 10, 295–300. [Google Scholar] [CrossRef]
- Desmond, D.; Layton, N.; Bentley, J.; Boot, F.H.; Borg, J.; Dhungana, B.M.; Gallagher, P.; Gitlow, L.; Gowran, R.J.; Groce, N.; et al. Assistive Technology and People: A Position Paper from the First Global Research, Innovation and Education on Assistive Technology (GREAT) Summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 437–444. [Google Scholar] [CrossRef] [Green Version]
- Doyle-Kent, M.; Fanning, M.; O’Brien, D.; Kopacek, P. Cost Oriented Robotic Arm Optimised to Aid Independence. IFAC-PapersOnLine 2019, 52, 125–130. [Google Scholar] [CrossRef]
- Tah, I.H.M. A Need for Remedial Provision to Protect Persons with Disabilities in Malaysia. Int. J. Bus. Econ. Law 2013, 3, 1–4. [Google Scholar]
- Islam, M.R. Rights of the People with Disabilities and Social Exclusion in Malaysia. Int. J. Soc. Sci. Humanit. 2015, 5, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Tah, I.H.M.; Mokhtar, K.A. Transforming Disability Studies through Legal Perspectives in Malaysia. J. Appl. Environ. Biol. Sci. 2017, 5, 51–55. [Google Scholar]
- Talib, R.I.A.; Sunar, M.S.; Mohamed, R. Digital Society and Economy for People with Disabilities in Industry 4.0: Malaysia Perspectives. EAI Endorsed Trans. Creat. Technol. 2019, 6, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Universal Declaration of Human Rights. Available online: https://www.ohchr.org/EN/UDHR/Documents/UDHR_Translations/eng.pdf (accessed on 3 March 2020).
- Merezhko, O. Legal Hermeneutics and Methodology of Law. Eur. Polit. Law Discourse 2014, 1, 4–10. [Google Scholar]
- Cowney, F.; Bradney, A. Socio-legal Studies: A Challenge to the Doctrinal Approach. In Research Methods in Law; Watkins, D., Burton, M., Eds.; Routledge: New York, NY, USA, 2013; pp. 34–54. [Google Scholar]
- United Nations Department of Economic and Social Affairs (UNDESA). Convention on the Rights of Persons with Disabilities (CRPD): Entry into Force. Available online: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities/entry-into-force.html (accessed on 3 March 2020).
- United Nations Department of Economic and Social Affairs (UNDESA). Convention on the Rights of Persons with Disabilities (CRPD): Ratifications/Accessions, Signatories. Available online: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html (accessed on 3 March 2020).
- United Nations General Assembly (UNGA). Letter Dated 7 October 2005 from the Chairman to All Members of the Committee, A/AC.265/2006/1; UNGA: New York, NY, USA, 2005. [Google Scholar]
- Kanter, A.S. The United Nations Convention on the Rights of Persons with Disabilities and its Implications for the Rights of Elderly People under International Law. Ga. State Univ. Law Rev. 2009, 25, 527–573. [Google Scholar]
- Kayess, R.; Fogarty, B. The Rights and Dignity of Persons with Disabilities: A United Nations Convention. Altern. Law J. 2007, 32, 22–30. [Google Scholar] [CrossRef]
- United Nations Department of Economic and Social Affairs (UNDESA). Compilation of Proposals for a Comprehensive and Integral International Convention to Promote and Protect the Rights and Dignity of Persons with Disabilities. Ad Hoc Committee on a Comprehensive and Integral International Convention on Protection and Promotion of the Rights and Dignity of Persons with Disabilities; United Nations: New York, NY, USA, 2003. [Google Scholar]
- United Nations Department of Economic and Social Affairs (UNDESA). Bangkok Draft: Proposed Elements of a Comprehensive and Integral International Convention to Promote and Protect the Rights of Persons with Disabilities. Regional Workshop towards a Comprehensive and Integral International Convention on Protection and Promotion of the Rights and Dignity of Persons with Disabilities; Ad Hoc Committee on an International Convention, United Nations Department of Economic and Social Affairs (UNDESA); United Nations: New York, NY, USA, 2003. [Google Scholar]
- United Nations Department of Economic and Social Affairs (UNDESA). Compilation of Proposals for Elements of a Convention; Working Group of the Ad Hoc Committee on a Comprehensive and Integral International Convention on Protection and Promotion of the Rights and Dignity of Persons with Disabilities; United Nations: New York, NY, USA, 2004. [Google Scholar]
- United Nations General Assembly (UNGA). Report of the Third Session of the Ad Hoc Committee on a Comprehensive and Integral International Convention on the Protection and Promotion of the Rights and Dignity of Persons with Disabilities, A/AC.265/2004/5; UNGA: New York, NY, USA, 2004. [Google Scholar]
- United Nations General Assembly (UNGA). Report of the Ad Hoc Committee on a Comprehensive and Integral International Convention on the Protection and Promotion of the Rights and Dignity of Persons with Disabilities on Its Seventh Session, A/AC.265/2006/2; UNGA: New York, NY, USA, 2006. [Google Scholar]
- Borg, J.; Lindström, A.; Larsson, S. Assistive Technology in Developing Countries: National and International Responsibilities to Implement the Convention on the Rights of Persons with Disabilities. Lancet 2009, 374, 1863–1865. [Google Scholar] [CrossRef]
- Scanlon, M.L.; MacNaughton, G.; Sprague, C. Neglected Population, Neglected Right: Children Living with HIV and the Right to Science. Heal. Hum. Rights J. 2017, 19, 169–180. [Google Scholar]
- United Nations Educational, Scientific and Cultural Organization (UNESCO). The Right to Enjoy the Benefits of Scientific Progress and its Applications; United Nations Educational, Scientific and Cultural Organization: Paris, France, 2009. [Google Scholar]
- World Health Organization (WHO). Medical Device–Full Definition. Available online: https://www.who.int/medical_devices/full_deffinition/en/ (accessed on 3 March 2020).
- Case of Artavia Murillo Et Al. (“In Vitro Fertilization”) v. Costa Rica. Judgment of 28 November 2012, Inter-American Court of Human Rights. Available online: https://www.corteidh.or.cr/docs/casos/articulos/seriec_257_ing.pdf (accessed on 31 March 2020).
- López, Glenda y otros c. Instituto Venezolano de los Seguros Sociales (IVSS) s/ Acción de Amparo. Expediente 00-1343. Sentencia N° 487. 1997. Available online: https://www.globalhealthrights.org/wp-content/uploads/2013/08/Lopez-v.-IVSS-English-Translation.pdf (accessed on 31 March 2020).
- Lovászy, L.G. Innovation has Changed the Meaning of (Re) Habilitation. EuroScientist. Available online: http://21ax0w3am0j23cz0qd1q1n3u-wpengine.netdna-ssl.com/wp-content/uploads/2016/02/Innovation-has-chnaged-the-meaning-of-rehabilityation-FINAL.pdf (accessed on 3 March 2020).
- Zhou, G.; Jiang, H.; Yin, Z.; Liu, Y.; Zhang, Q.; Pan, B.; Zhou, J.; Zhou, X.; Sun, H. In Vitro Regeneration of Patient-Specific Ear-Shaped Cartilage and Its First Clinical Application for Auricular Reconstruction. EBioMedicine 2018, 28, 287–302. [Google Scholar] [CrossRef] [Green Version]
- Freier, A. Researchers 3D Bioprint the First Ears Made from Children’s Own Cells. Available online: https://all3dp.com/researchers-3d-bioprint-first-ears-made-childens-cells/ (accessed on 25 February 2020).
- Horizon. 3D-Printed Living Tissues Could Spell the End of Arthritis. Horizon: The EU Research & Innovation Magazine. Available online: https://horizon-magazine.eu/article/3d-printed-living-tissues-could-spell-end-arthritis.html (accessed on 3 March 2020).
- Schlaefli, S. Nose Made by Bioprinters. Globe Magazine. Available online: https://ethz.ch/en/news-and-events/eth-news/news/2015/03/nose-made-by-bioprinters.html (accessed on 3 March 2020).
- Augustine, R. Skin Bioprinting: A Novel Approach for Creating Artificial Skin from Synthetic and Natural Building Blocks. Prog. Biomater. 2018, 7, 77–92. [Google Scholar] [CrossRef] [Green Version]
- Wake Forest Baptist Medical Center. Mobile Bedside Bioprinter Can Heal Wounds. Science Daily. 28 February 2019. Available online: https://www.sciencedaily.com/releases/2019/02/190228134229.htm (accessed on 4 May 2020).
- Supriyanto, I.E. Cardiovascular and Biomedical Research at Universiti Teknologi Malaysia. Available online: https://mrc.ukri.org/documents/pdf/universiti-teknologi-malaysia/ (accessed on 28 January 2019).
- Hakam, M.S.; Imani, R.; Abolfathi, N.; Fakhrzadeh, H.; Sharifi, A.M. Evaluation of Fibrin-Gelatin Hydrogel as Biopaper for Application in Skin Bioprinting: An In-Vitro Study. Biomed. Mater. Eng. 2016, 27, 669–682. [Google Scholar] [CrossRef] [PubMed]
- Kian, S.T.; Low, E.; Ramilan, M.F.; Rahim, R.A.; Saim, H.; Zakaria, W.N.W.; Khialdin, S.M.; Isa, H.; Chin, F.S. A Development of a 3D Bio-Printer. J. Tomogr. Syst. Sens. Appl. 2019, 2, 1–10. [Google Scholar]
- Park, R. 3D Printed Surgical Guides Make Their Malaysian Debut. 3D Printing Industry. 20 June 2013. Available online: https://3dprintingindustry.com/news/3d-printed-surgical-guides-make-their-malaysian-debut-13222/ (accessed on 15 June 2017).
- Kumar, A. Malaysian Biomedical Centre’s “Major Breakthrough” Using Stratasys 3D Printing. CIO Asia. 14 November 2013. Available online: https://www.cio-asia.com/tech/imaging-and-printing/malaysian-biomedical-centres-major-breakthrough-using-stratasys-3d-printing/ (accessed on 16 June 2017).
- Lee, M.L. 3D Printing May Save Your Life If You Need Risky Surgery. Star Online. 25 October 2015. Available online: https://www.star2.com/health/wellness/2015/10/25/3d-printing-may-save-your-life-if-you-need-risky-surgery/ (accessed on 19 January 2017).
- Muda, A.S.; Mohammed, Y. Medical Grade 3D Print (MeG3rD). Available online: https://sciencepark.upm.edu.my/article/medical_grade_3d_print_meg3rd-40793?L=en (accessed on 14 March 2020).
- Lee, J. “Future of Malaysia, Korea Lies in ASEAN”: International Trade Minister. Korea Herald. 24 October 2018. Available online: http://www.koreaherald.com/view.php?ud=20181022000796 (accessed on 26 December 2018).
- Tan, L.F.; Ong, C.W. Big Need for Biomed Engineers. Star Online. 26 July 2015. Available online: https://www.thestar.com.my/news/education/2015/07/26/big-need-for-biomed-engineers (accessed on 2 February 2020).
- Ong, H.S. Wan Azizah: Govt Committed to Welfare of OKU Community. Star Online. 13 April 2019. Available online: https://www.thestar.com.my/news/nation/2019/04/13/wan-azizah-govt-committed-to-welfare-of-oku-community/ (accessed on 14 May 2020).
- Social Welfare Department, Malaysia. Statistical Registration of People with Disabilities According to State. 2018. Available online: https://ydata.iyres.gov.my/iyresbankdataV2/www/index.php?r=pub/home/readcontent4&id=110 (accessed on 10 May 2020).
- Asyraf, F. Disabled Children Not Registered with Social Welfare Dept Because Parents Embarrassed. Malaysiakini. 22 September 2019. Available online: https://www.malaysiakini.com/news/492865 (accessed on 15 May 2020).
- Ministry of Human Resources, Malaysia. Percentage of Registration of Persons with Disabilities (PWD) by Category of Disabilities Malaysia 2018. Available online: https://www.myforesight.my/2019/06/26/disability-inclusion/ (accessed on 4 May 2020).
- Social Welfare Department, Malaysia. Information on Registration for People with Disabilities and Disabled Category; Social Welfare Department: Putrajaya, Malaysia, 2019.
- Ministry of Health, Malaysia. Assistance for Heart Disease’s Patients. Available online: http://www.myhealth.gov.my/en/assistance-heart-diseases-patient/ (accessed on 14 May 2020).
- Ministry of Health, Malaysia. The Annual Report National ORL Registry: Hearing and Otology Related Disease/Cochlear Implant; Ministry of Health, Malaysia: Kuala Lumpur, Malaysia, 2013; ISSN 2289-4379.
- Hassan, E.; Goh, B.S. The Prevalence and Characteristics of Microtia: A Cross Sectional Study in Universiti Kebangsaan Malaysia Medical Center. In Proceedings of the MSOHNS Annual Scientific Meeting & 9th Malaysia-Singapore Joint ENT Meeting 2014, Genting Highlands, Malaysia, 20 April 2014; Malaysian Society of Otorhinolaryngologists Head & Neck Surgeons (MSO-HNS): Kuala Lumpur, Malaysia, 2014; p. 15. [Google Scholar]
- Majid, M.A. Combating Malaysia’s Involvement in Worldwide Organ Trafficking by Tapping into the Potential of Bioprinting. Glob. J. Bus. Soc. Sci. Rev. 2019, 7, 61–74. [Google Scholar] [CrossRef]
- Hassandarvish, M. On Dialysis for Nine Years, KL Man Counts Himself Lucky to Receive Kidney from Brother. Malay Mail Online. 28 November 2019. Available online: https://www.malaymail.com/news/life/2019/11/28/on-dialysis-for-nine-years-kl-man-counts-himself-lucky-to-receive-kidney-fr/1814196 (accessed on 4 May 2020).
- Ministry of Health, Malaysia. General Disabilities. Available online: http://www.myhealth.gov.my/en/general-disabilities/ (accessed on 14 May 2020).
- Fire and Rescue Department of Malaysia. Death and Injury Statistics from Fire. 2018. Available online: http://www.data.gov.my/data/dataset/6e4096cf-8e08-4b47-94ed-21bb312b5149/resource/6fe56128-4f19-4036-918d-642d23869c3c/download/statistik-kematian-dan-kecederaan-akibat-kebakaran-2018.xlsx (accessed on 6 May 2020).
- Ministry of Housing and Local Government, Malaysia. KPKT Selected Statistics Until 30th June 2019; Ministry of Housing and Local Government: Putrajaya, Malaysia, 2019.
- Foo, C.N.; Arumugam, M.; Rampal, L.; Munn, S.L.; Sidik, S.M.; Osman, Z.J. Knee Pain and Functional Disability of Knee Osteoarthritis Patients Seen at Malaysian Government Hospitals. Malays. J. Med. Health Sci. 2017, 13, 7–15. [Google Scholar]
- Ringgit Plus.com. Ringgit Plus Team Price Difference between a Government vs Private Hospital in Malaysia. Available online: https://ringgitplus.com/en/blog/insurance/government-and-private-hospitals-in-malaysia-how-much-do-they-really-cost.html (accessed on 10 May 2020).
- Health Tourism.com. Ear Plastic Surgery in Malaysia. Available online: https://www.health-tourism.com/ear-plastic-surgery/malaysia/ (accessed on 6 May 2020).
- UniMed Travels. Rhinoplasty in Malaysia. Available online: http://www.unimedtravels.com/rhinoplasty/malaysia (accessed on 6 May 2020).
- Sun Daily. There Are 7055 New Patients Every Year, Says Report. Sun Daily. 5 September 2016. Available online: https://www.thesundaily.my/archive/1960044-ISARCH392427 (accessed on 10 May 2020).
- Kamaruddin, S.P. Normothermic Donor Heart Perfusion Device, TechScan 003/2017; Ministry of Health: Putrajaya, Malaysia, 2017.
- Osman, O.M.; Diah, N.M. Empowering People with Disabilities (PWDs) via Information Communication Technology (ICT): The Case of Malaysia. Int. J. Stud. Child. Women Elder. Disabl. 2017, 2, 86–93. [Google Scholar]
- Academy of Sciences Malaysia. Science & Technology Foresight Malaysia 2050; Academy of Sciences Malaysia: Kuala Lumpur, Malaysia, 2017.
- Academy of Sciences Malaysia. Advisory Report on Stem Cells Ageing and Regenerative Medicine. Kuala Lumpur, Malaysia; 2013. Available online: https://www.akademisains.gov.my/asmpub/?smd_process_download=1&download_id=210 (accessed on 3 March 2020).
- Rahim, A.A.; Samad, N.A.A.; Said, I.; Seman, W.; Amin, W.M. Malaysian Plan of Action for People with Disabilities 2016–2022: Way Forward. In Proceedings of the UIA 2017 Seoul World Architects Congress, International Union of Architects (UIA), Seoul, Korea, 3–7 September 2017; International Union of Architects: Seoul, Korea, 2017; pp. 1–6. [Google Scholar]
- Ibrahim, M.; Ahmad, M.S.; Abdullah, I.; Omar, M.H.; Ariff, A.F.; Yusoff, S.A.T. UniSZA as the National Centre of Design for Disability in Malaysia. In Proceedings of the IOP Conference Series: Materials Science and Engineering, Kuala Terengganu, Malaysia, 27–28 August 2019; Institute of Physics (IOP): London, UK, 2019; Volume 697, pp. 1–6. [Google Scholar]
- Human Rights Commission of Malaysia (SUHAKAM). Persons with Disabilities (PWD). Available online: https://www.suhakam.org.my/areas-of-work/pendidikan/orang-kurang-upaya-oku/ (accessed on 3 March 2020).

{kind=link}
{kind=link}
{kind=link}
| CRPD | Interpretation of the Right to Science in Art. 27 of the UDHR and Art. 15(1) (b) of the ICESCR |
|---|---|
| Art. 4(1) (g) of the CRPD stresses that research and development (R&D) be conducted and new technologies be promoted for persons with disabilities who are marginalised. | The relevant Articles address the need for scientific research to be conducted for marginalised communities without discrimination. |
| Art. 4(1) (g) of the CRPD refers to Information Communications Technology (ICT) for the benefit of the disabled. | The right to science includes ensuring freedom of access, the promotion of information on the internet and its connectivity. |
| Art. 4(1) (h) of the CRPD stresses the need for accessible information to improve the life of disabled people. | The right to science has been interpreted as including the right to be informed of new scientific discoveries and their applications in order to improve the life of marginalised communities. |
| Art 4(1) (g) of the CRPD stresses that new technologies must be made available at an affordable price. | The right to science has also been interpreted as meaning that new technologies must be made available at an affordable price. |
| Art. 32(1) (b)–(c) of the CRPD emphasises international collaboration which covers capacity building, namely in the sharing of information, experiences, training programmes and best practices, for the benefit of disabled people. Cooperation in R&D and access to scientific knowledge are also stressed. | The right to science has been understood to include international cooperation and assistance in science and technology which may cover direct aid, financial and material assistance, and collaborative models of R&D for the benefit of developing countries. |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdul Majid, M. Bioprinting’s Introduction within the Context of the Convention on the Rights of Persons with Disabilities and Malaysia’s Persons with Disabilities Act 2008 through the Right to Science. Societies 2020, 10, 40. https://doi.org/10.3390/soc10020040
Abdul Majid M. Bioprinting’s Introduction within the Context of the Convention on the Rights of Persons with Disabilities and Malaysia’s Persons with Disabilities Act 2008 through the Right to Science. Societies. 2020; 10(2):40. https://doi.org/10.3390/soc10020040
Chicago/Turabian StyleAbdul Majid, Marina. 2020. "Bioprinting’s Introduction within the Context of the Convention on the Rights of Persons with Disabilities and Malaysia’s Persons with Disabilities Act 2008 through the Right to Science" Societies 10, no. 2: 40. https://doi.org/10.3390/soc10020040
APA StyleAbdul Majid, M. (2020). Bioprinting’s Introduction within the Context of the Convention on the Rights of Persons with Disabilities and Malaysia’s Persons with Disabilities Act 2008 through the Right to Science. Societies, 10(2), 40. https://doi.org/10.3390/soc10020040