
The Reliability of Common Functional Performance Tests within an Experimental Test Battery for the Lower Extremities



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Subjects
2.3. Procedures
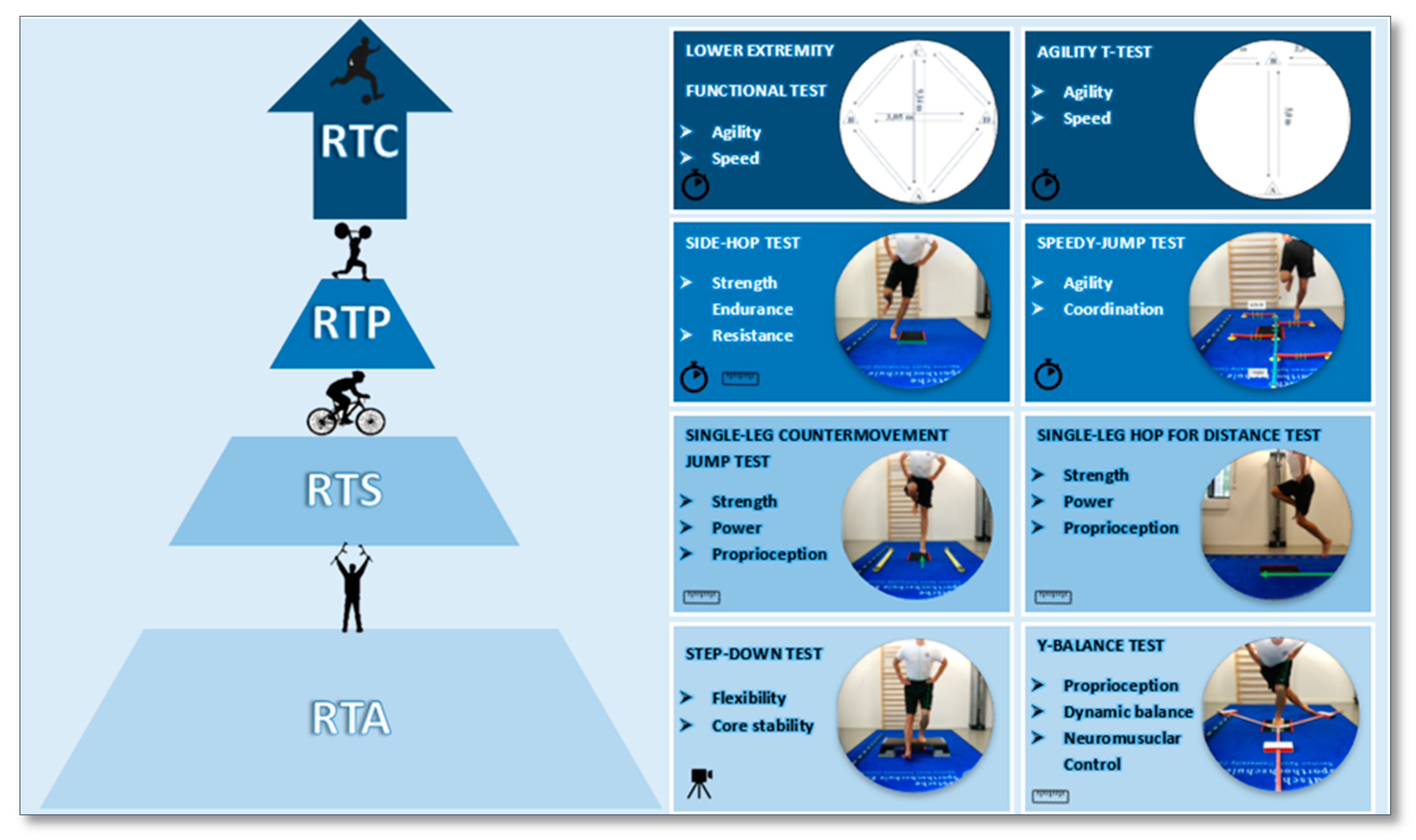
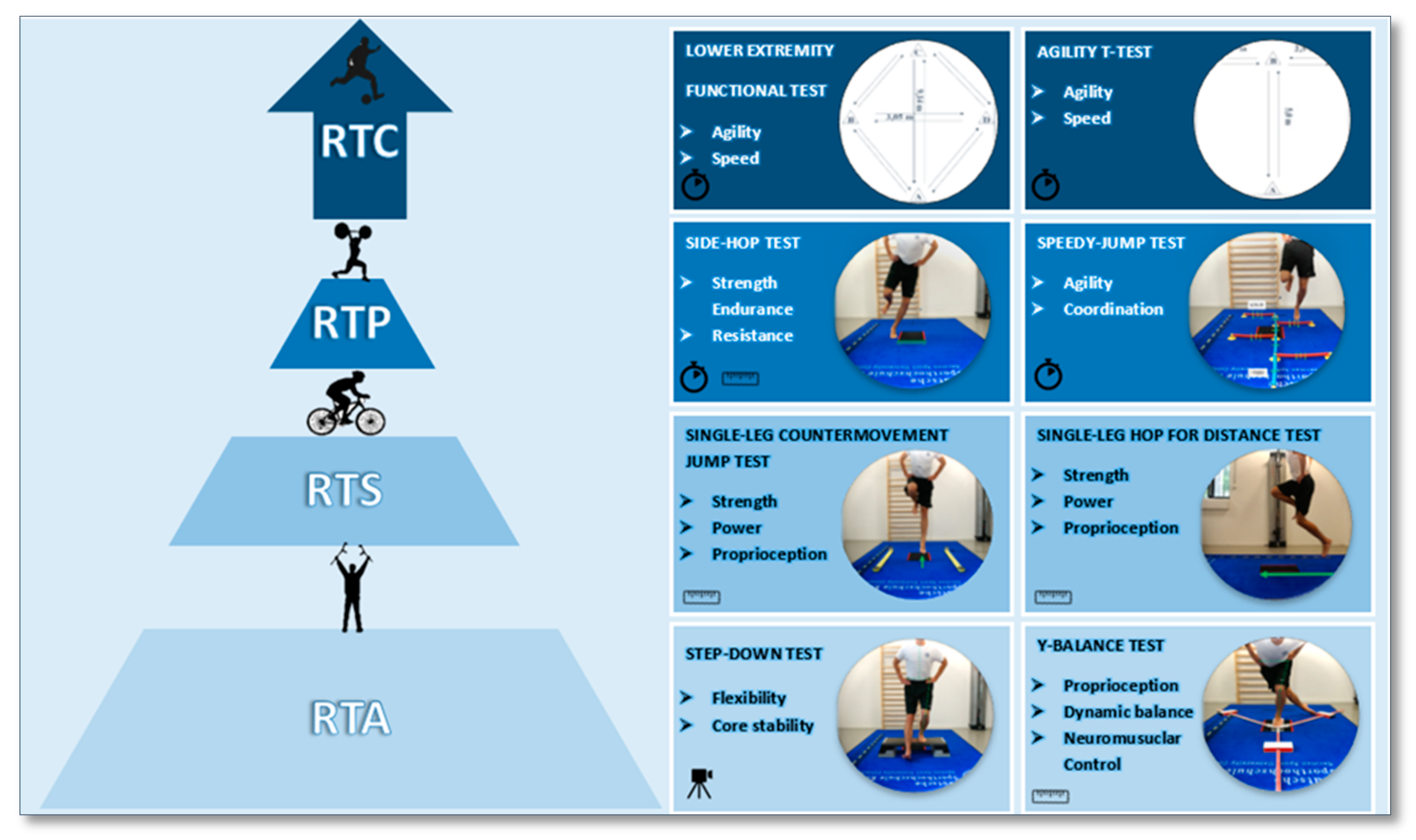
2.4. Test Battery Standardization and Description
2.4.1. Step-Down Test (SD)
2.4.2. Y-Balance Test (YBT)
2.4.3. Single-Leg Countermovement Jump Test (SLCMJ)
2.4.4. Single Leg Hop for Distance Test (SLH)
2.4.5. Side-Hop Test (SH)
2.4.6. Speedy-Jump Test (SJ)
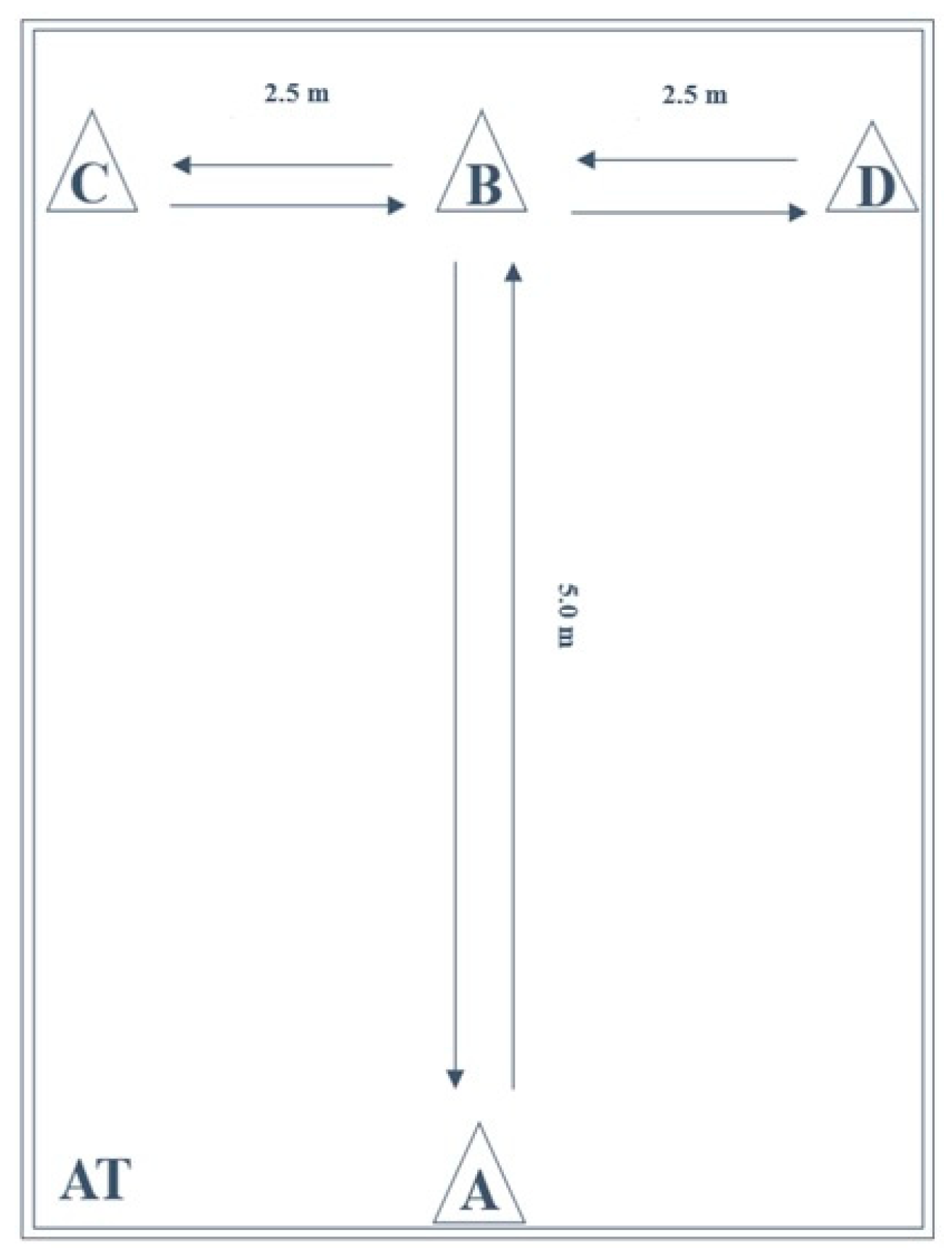
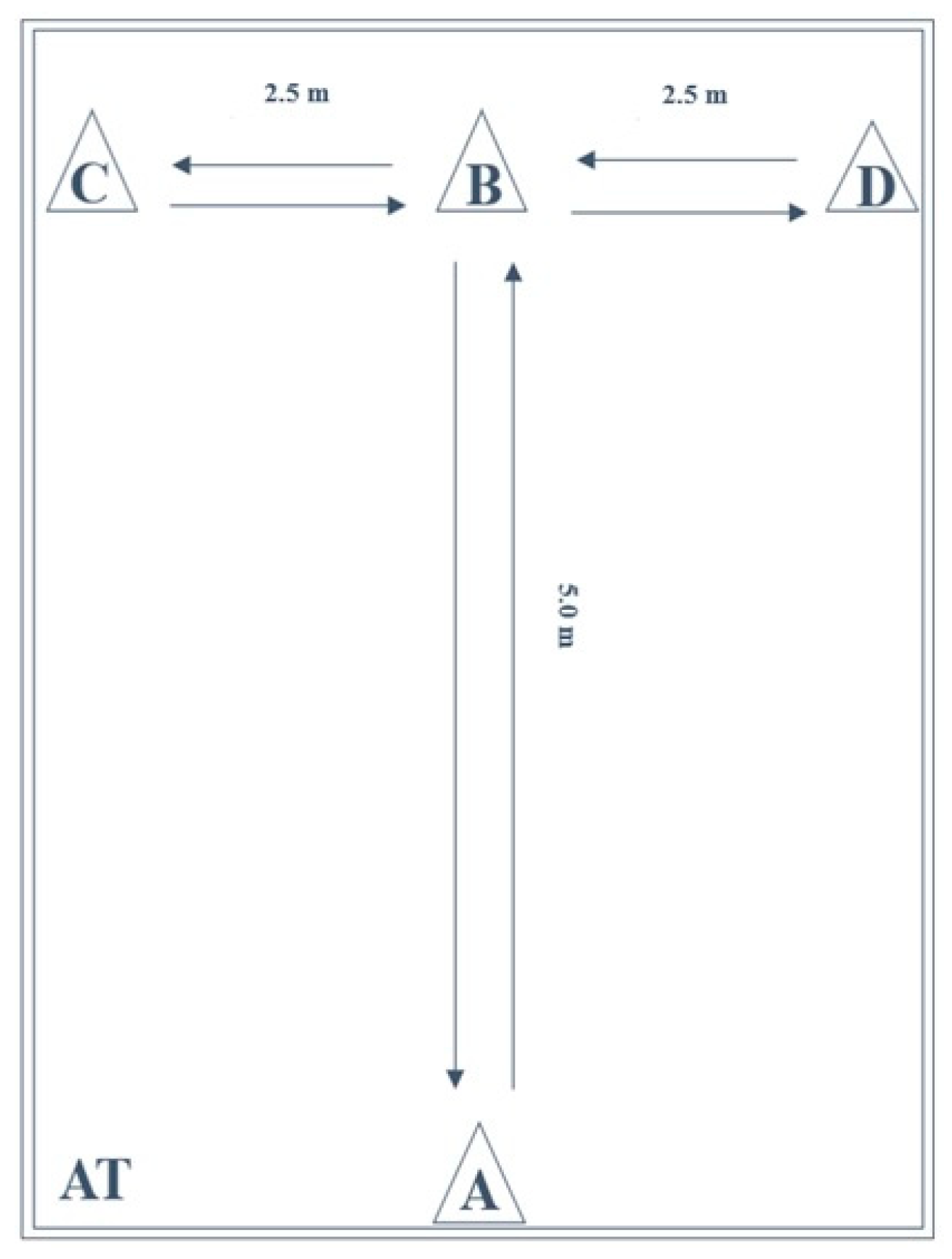
2.4.7. Agility T-Test (AT)
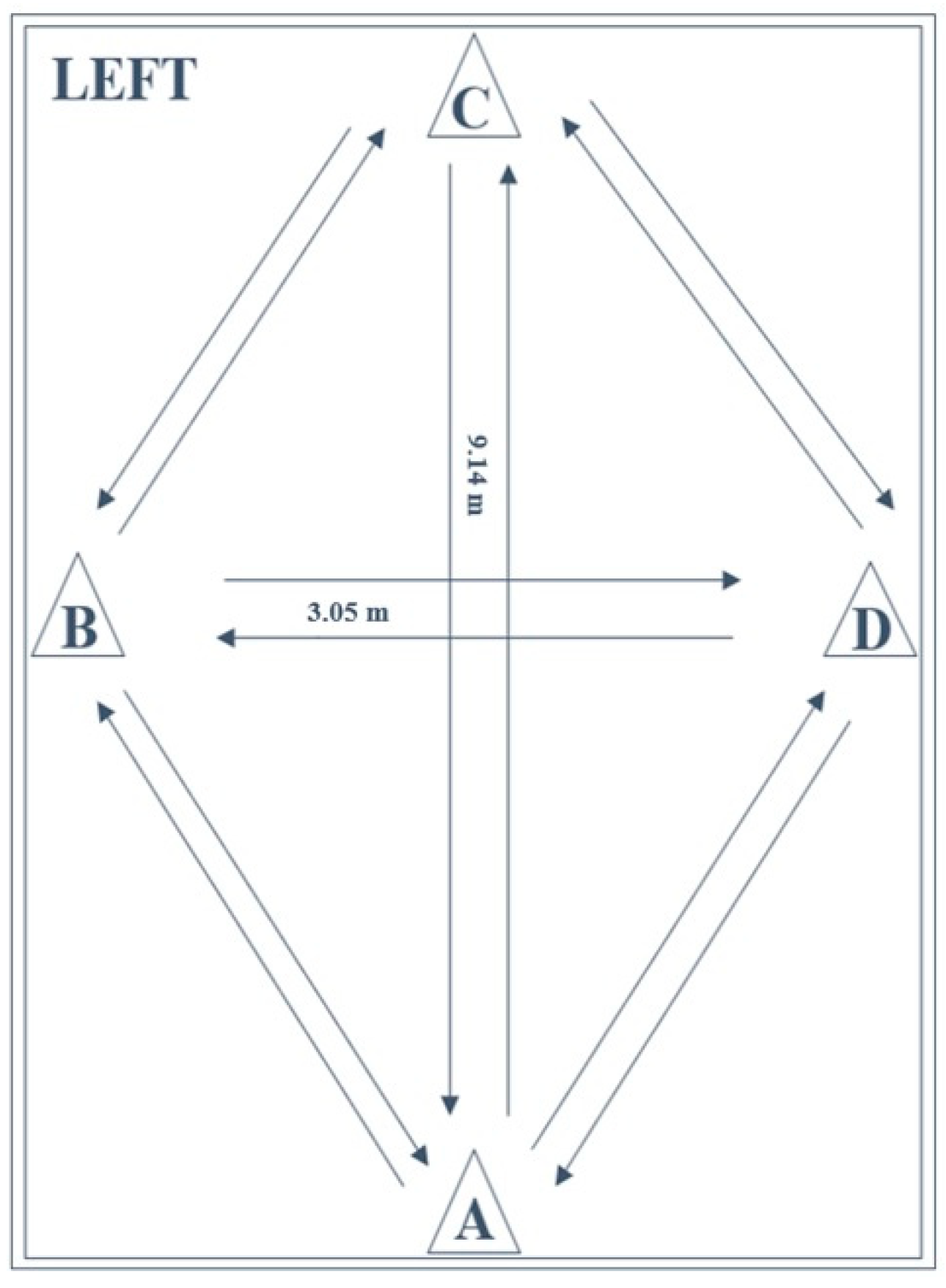
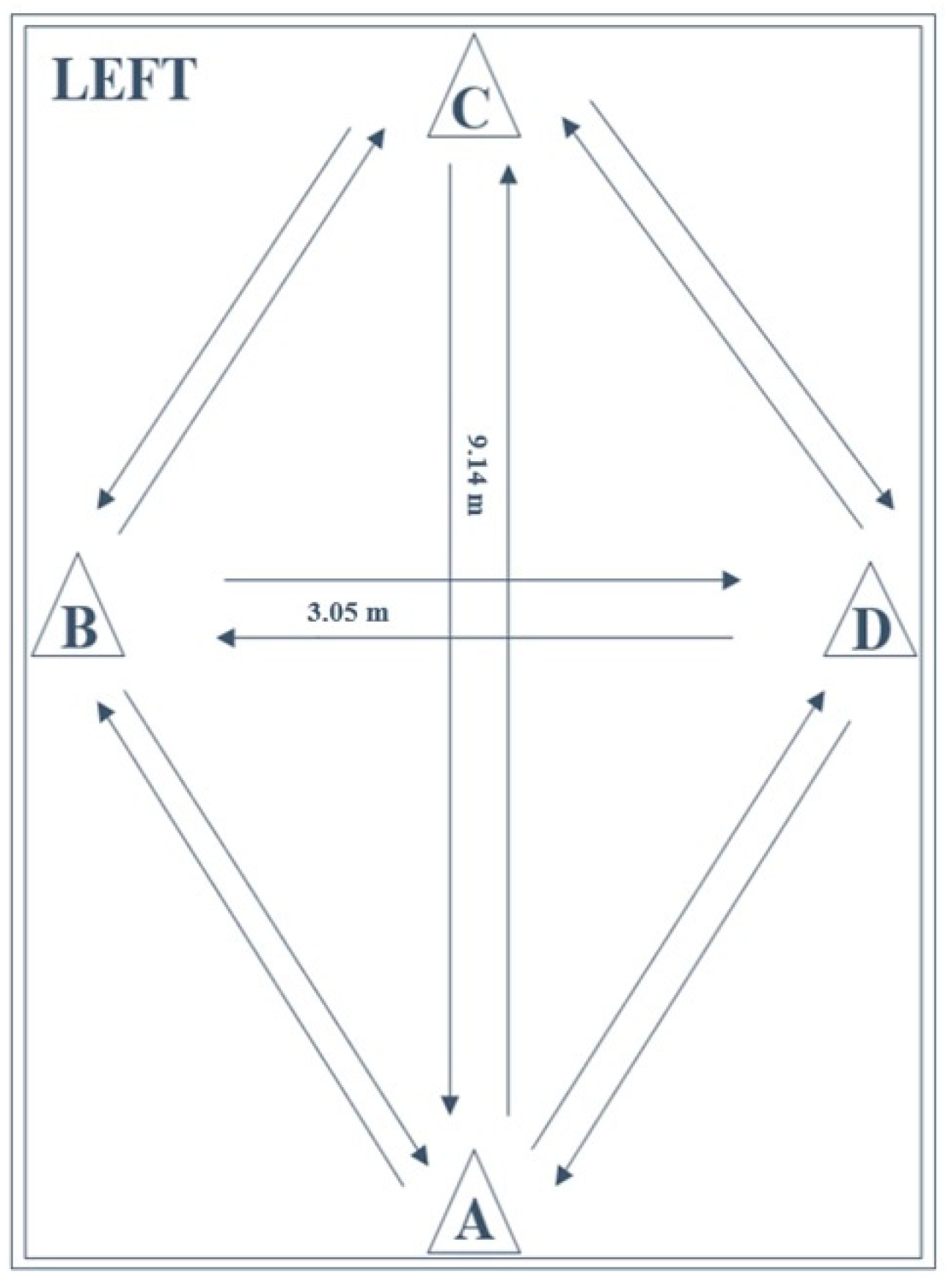
2.4.8. Lower Extremity Functional Test (LEFT)
2.5. Test–Retest Reliability
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hildebrandt, C.; Müller, L.; Zisch, B.; Huber, R.; Fink, C.; Raschner, C. Functional assessments for decision-making regarding return to sports following ACL reconstruction. Part I: Development of a new test battery. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1273–1281. [Google Scholar] [CrossRef] [Green Version]
- Manske, R.; Reiman, M. Functional performance testing for power and return to sports. Sports Health 2013, 5, 244–250. [Google Scholar] [CrossRef] [Green Version]
- Herbst, E.; Hoser, C.; Hildebrandt, C.; Raschner, C.; Hepperger, C.; Pointner, H.; Fink, C. Functional assessments for decision-making regarding return to sports following ACL reconstruction. Part II: Clinical application of a new test battery. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1283–1291. [Google Scholar] [CrossRef] [Green Version]
- Moser, N.; Bloch, H. Return-to-Competition: Testmanual zur Beurteilung der Spielfähigkeit nach Ruptur des vorderen Kreuzbands; Version 1.0; Ihre gesetzliche Unfallversicherung (VBG): Hamburg, Germany, 2015. [Google Scholar]
- Shultz, S.J.; Schmitz, R.J.; Cameron, K.L.; Ford, K.R.; Grooms, D.R.; Lepley, L.K.; Myer, G.D.; Pietrosimone, B. Anterior Cruciate Ligament Research Retreat VIII Summary Statement: An Update on Injury Risk Identification and Prevention Across the Anterior Cruciate Ligament Injury Continuum, March 14-16, 2019, Greensboro, NC. J. Athl. Train. 2019, 54, 970–984. [Google Scholar] [CrossRef] [Green Version]
- Petersen, W.; Diermeier, T.; Mehl, J.; Stöhr, A.; Ellermann, A.; Müller, P.; Höher, J.; Herbort, M.; Akoto, R.; Zantop, T.; et al. Prevention of knee and ACL injuries. Guidelines of the ligament commitee of the DKG (German Knee Society). OUP 2016, 10, 542–550. [Google Scholar] [CrossRef]
- Loturco, I.; Pereira, L.A.; Kobal, R.; Abad, C.C.C.; Komatsu, W.; Cunha, R.; Arliani, G.; Ejnisman, B.; Pochini, A.D.C.; Nakamura, F.Y.; et al. Functional screening tests: Interrelationships and ability to predict vertical jump performance. Int. J. Sports Med. 2018, 39, 189–197. [Google Scholar] [CrossRef]
- Hughes, T.; Sergeant, J.C.; Parkes, M.J.; Callaghan, M.J. Prognostic factors for specific lower extremity and spinal musculoskeletal injuries identified through medical screening and training load monitoring in professional football (soccer): A systematic review. BMJ Open Sport Exerc. Med. 2017, 3. [Google Scholar] [CrossRef]
- McCall, A.; Carling, C.; Davison, M.; Nedelec, M.; Le Gall, F.; Berthoin, S.; Dupont, G. Injury risk factors, screening tests and preventative strategies: A systematic review of the evidence that underpins the perceptions and practices of 44 football (soccer) teams from various premier leagues. Br. J. Sports Med. 2015, 49, 583–589. [Google Scholar] [CrossRef]
- Swart, E.; Redler, L.; Fabricant, P.D.; Mandelbaum, B.R.; Ahmad, C.S.; Wang, Y.C. Prevention and screening programs for anterior cruciate ligament injuries in young athletes: A cost-effectiveness analysis. J. Bone Jt. Surg. 2014, 96, 705–711. [Google Scholar] [CrossRef] [Green Version]
- Wilke, C.; Scinicarelli, G.; Schoser, D.S.; Offerhaus, C.; Froböse, I. Limb symmetry index and pre-injury performance level after anterior cruciate ligament reconstruction: A case report on a female gymnast. Sports Orthop. Traumatol 2021, in press. [Google Scholar] [CrossRef]
- Wilke, C.; Grimm, L.; Hoffmann, B.; Froböse, I. Funktionelle Tests als Entscheidungskriterium für die Rückkehr von Spielsportlern nach einer Ruptur des vorderen Kreuzbandes. Sportverletz. Sportschaden. 2018, 32, 171–186. [Google Scholar] [CrossRef]
- Wilke, C.; Pfeiffer, L.; Froböse, I. Return to sports after lower extremity injuries: Assessment of movement quality. Health 2017, 9, 1416–1426. [Google Scholar] [CrossRef] [Green Version]
- Keller, M.; Kurz, E.; Schmidtlein, O.; Welsch, G.; Anders, C. Interdisziplinäre Beurteilungskriterien für die Rehabilitation nach Verletzungen an der unteren Extremität: Ein funktionsbasierter Return to Activity Algorithmus. Sportverletz. Sportschaden. 2016, 30, 38–49. [Google Scholar] [CrossRef]
- Lambert, C.; Pfeiffer, T.; Lambert, M.; Brozat, B.; Lachmann, D.; Shafizadeh, S.; Akoto, R. Side differences regarding the Limb Symmetry Index in healthy professional athletes. Int. J. Sports Med. 2020, 41, 729–735. [Google Scholar] [CrossRef]
- Nagai, T.; Schilaty, N.D.; Laskowski, E.R.; Hewett, T.E. Hop tests can result in higher limb symmetry index values than isokinetic strength and leg press tests in patients following ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 816–822. [Google Scholar] [CrossRef]
- Lustosa, L.S.; Pereira, N.D.C.; de Almeida Ferreira, J.J.; de Andrade, P.R.; Honorato dos Santos, H. Lower limb symmetry index (LLSI) pre- and post-reconstruction of the ACL: A controlled study. Man. Ther. Posturol Rehabil. J. 2018, 16, 597. [Google Scholar] [CrossRef]
- Steidl-Müller, L.; Hildebrandt, C.; Müller, E.; Fink, C.; Raschner, C. Limb symmetry index in competitive alpine ski racers: Reference values and injury risk identification according to age-related performance levels. J. Sport Health Sci. 2018, 7, 405–415. [Google Scholar] [CrossRef]
- Rohman, E.; Steubs, J.T.; Tompkins, M. Changes in involved and uninvolved limb function during rehabilitation after anterior cruciate ligament reconstruction: Implications for Limb Symmetry Index measures. Am. J. Sports Med. 2015, 43, 1391–1398. [Google Scholar] [CrossRef]
- Bishop, C.; Read, P.; McCubbine, J.; Turner, A. Vertical and horizontal asymmetries are related to slower sprinting and jump performance in elite youth female soccer players. J. Strength Cond. Res. 2018, 35, 56–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, C.; Read, P.; Lake, J.; Chavda, S.; Turner, A. Inter-limb asymmetries: Understanding how to calculate differences from bilateral and unilateral tests. Strength Cond. J. 2018, 40, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Adams, D.; Logerstedt, D.S.; Hunter-Giordano, A.; Axe, M.J.; Snyder-Mackler, L. Current concepts for anterior cruciate ligament reconstruction: A criterion-based rehabilitation progression. J. Orthop. Sports Phys. Ther. 2012, 42, 601–614. [Google Scholar] [CrossRef] [Green Version]
- Ortiz, A.; Micheo, W. Biomechanical evaluation of the athlete’s knee: From basic science to clinical application. PM&R 2011, 3, 365–371. [Google Scholar] [CrossRef]
- Distefano, L.J.; Padua, D.A.; Blackburn, J.T.; Garrett, W.E.; Guskiewicz, K.M.; Marshall, S.W. Integrated injury prevention program improves balance and vertical jump height in children. J. Strength Cond. Res. 2010, 24, 332–342. [Google Scholar] [CrossRef]
- Gokeler, A.; Welling, W.; Zaffagnini, S.; Seil, R.; Padua, D. Development of a test battery to enhance safe return to sports after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 192–199. [Google Scholar] [CrossRef] [Green Version]
- Haitz, K.; Shultz, R.; Hodgins, M.; Matheson, G.O. Test-retest and interrater reliability of the functional lower extremity evaluation. J. Orthop. Sports Phys. Ther. 2014, 44, 947–954. [Google Scholar] [CrossRef] [Green Version]
- Plisky, P.J.; Gorman, P.P.; Butler, R.J.; Kiesel, K.B.; Underwood, F.B.; Elkins, B. The reliability of an instrumented device for measuring components of the Star Excursion Balance Test. N. Am. J. Sports Phys. Ther. 2009, 4, 92–99. [Google Scholar] [PubMed]
- Plisky, P.J.; Rauh, M.J.; Kaminski, T.W.; Underwood, F.B. Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players. J. Orthop. Sports Phys. Ther. 2006, 36, 911–919. [Google Scholar] [CrossRef]
- Kockum, B.; Heijne, A.I.L.M. Hop performance and leg muscle power in athletes: Reliability of a test battery. Phys. Ther. Sport. 2015, 16, 222–227. [Google Scholar] [CrossRef]
- Gustavsson, A.; Neeter, C.; Thomeé, P.; Silbernagel, K.G.; Augustsson, J.; Thomeé, R.; Karlsson, J. A test battery for evaluating hop performance in patients with an ACL injury and patients who have undergone ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 778–788. [Google Scholar] [CrossRef]
- Neeter, C.; Gustavsson, A.; Thomeé, P.; Augustsson, J.; Thomeé, R.; Karlsson, J. Development of a strength test battery for evaluating leg muscle power after anterior cruciate ligament injury and reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 571–580. [Google Scholar] [CrossRef]
- Brumitt, J.; Heiderscheit, B.C.; Manske, R.C.; Niemuth, P.; Rauh, M.J. Lower extremity functional tests and risk of injury in division iii collegiate athletes. Int. J. Sports Phys. Ther. 2013, 8, 2016–2027. [Google Scholar]
- Munro, A.G.; Herrington, L.C. Between-session reliability of four hop tests and the agility T-test. J. Strength Cond. Res. 2011, 25, 1470–1477. [Google Scholar] [CrossRef]
- Tabor, M.A.; Davies, G.J.; Kernozek, T.W.; Negrete, R.J.; Hudson, V. A multicenter study of the test–retest reliability of the lower extremity functional test. J. Sport Rehabil. 2002, 11, 190–201. [Google Scholar] [CrossRef]
- Pauole, K.; Madole, K.; Garhammer, J.; Lacourse, M.; Rozenek, R. Reliability and validity of the T-Test as a measure of agility, leg power, and leg speed in college-aged men and women. J. Strength Cond. Res. 2000, 14, 443–450. [Google Scholar] [CrossRef]
- Schelin, L.; Tengman, E.; Ryden, P.; Häger, C. A statistically compiled test battery for feasible evaluation of knee function after rupture of the anterior cruciate ligament—Derived from long-term follow-up data. PLoS ONE. 2017, 12, e0176247. [Google Scholar] [CrossRef]
- van Melick, N.; van Cingel, R.E.H.; Brooijmans, F.; Neeter, C.; van Tienen, T.; Hullegie, W.; Nijhuis-van der Sanden, M.W.G. Evidence-based clinical practice update: Practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br. J. Sports Med. 2016, 50, 1506–1515. [Google Scholar] [CrossRef] [Green Version]
- Leppink, J.; Pérez-Fuster, P. We need more replication research—A case for test-retest reliability. Perspect. Med. Educ. 2017, 6, 158–164. [Google Scholar] [CrossRef] [Green Version]
- Bishop, C.; Read, P.; Chavda, S.; Jarvis, P.; Turner, A. Using unilateral strength, power and reactive strength tests to detect the magnitude and direction of asymmetry: A test-retest design. Sports 2019, 7, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadhi, T.; Rauch, J.T.; Tamulevicius, N.; Andersen, J.C.; Souza, E.O. Validity and reliability of the GymAware linear position transducer for squat jump and counter-movement jump height. Sports 2018, 6, 177. [Google Scholar] [CrossRef] [Green Version]
- Thomas, C.; Dos’Santos, T.; Comfort, P.; Jones, P.A. Between-session reliability of common strength- and power-related measures in adolescent athletes. Sports 2017, 5, 15. [Google Scholar] [CrossRef]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Bruton, A.; Conway, J.H.; Holgate, S.T. Reliability: What is it, and how is it measured? Physiotherapy 2000, 86, 94–99. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Machin, D.; Campbell, M.J.; Walters, S.J. Medical Statistics: A Textbook for the Health Sciences, 4th ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2007. [Google Scholar]
- Chen, H.M.; Chen, C.C.; Hsueh, I.P.; Huang, S.L.; Hsieh, C.L. Test-retest reproducibility and smallest real difference of 5 hand function tests in patients with stroke. Neurorehabil. Neural Repair. 2009, 23, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.G.; Menezes, A.; Horovitz, L.; Jones, E.C.; Warren, R.F. A comparison of two-time intervals for test-retest reliability of health status instruments. J. Clin. Epidemiol. 2003, 56, 730–735. [Google Scholar] [CrossRef]
- Reid, A.; Birmingham, T.B.; Stratford, P.W.; Alcock, G.K.; Giffin, J.R. Hop testing provides a reliable and valid outcome measure during rehabilitation after anterior cruciate ligament reconstruction. Phys. Ther. 2007, 87, 337–349. [Google Scholar] [CrossRef] [Green Version]
- van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.G.; van Cingel, R.E.H. How to determine leg dominance: The agreement between self-reported and observed performance in healthy adults. PLoS ONE 2017, 12, e0189876. [Google Scholar] [CrossRef] [Green Version]
- Butler, R.J.; Lehr, M.E.; Fink, M.L.; Kiesel, K.B.; Plisky, P.J. Dynamic balance performance and noncontact lower extremity injury in college football players: An initial study. Sports Health 2013, 5, 417–422. [Google Scholar] [CrossRef] [Green Version]
- Hubbard, T.J.; Kramer, L.C.; Denegar, C.R.; Hertel, J. Contributing factors to chronic ankle instability. Foot Ankle Int. 2007, 28, 343–354. [Google Scholar] [CrossRef]
- Park, K.M.; Cynn, H.S.; Choung, S.D. Musculoskeletal predictors of movement quality for the forward step-down test in asymptomatic women. J. Orthop. Sports Phys. Ther. 2013, 43, 504–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holsgaard-Larsen, A.; Jensen, C.; Aagaard, P. Subjective vs objective predictors of functional knee joint performance in anterior cruciate ligament-reconstructed patients—Do we need both? Knee 2014, 21, 1139–1144. [Google Scholar] [CrossRef] [PubMed]
- Born, D.P.; Kunz, P.; Sperlich, B. Reliability and validity of an agility-like incremental exercise test with multidirectional change-of-direction movements in response to a visual stimulus. Physiol. Rep. 2017, 5. [Google Scholar] [CrossRef] [PubMed]
- Raya, M.A.; Gailey, R.S.; Gaunaurd, I.A.; Jayne, D.M.; Campbell, S.M.; Gagne, E.; Manrique, P.G.; Muller, D.G.; Tucker, C. Comparison of three agility tests with male servicemembers: Edgren Side Step Test, T-Test, and Illinois Agility Test. J. Rehabil. Res. Dev. 2013, 50, 951–960. [Google Scholar] [CrossRef]
- Bishop, C.; Read, P.; Chavda, S.; Turner, A. Asymmetries of the lower limb: The calculation conundrum in strength training and conditioning. Strength Cond. J. 2016, 38, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Hayen, A.; Dennis, R.J.; Finch, C.F. Determining the intra- and inter-observer reliability of screening tools used in sports injury research. J. Sci. Med. Sport 2007, 10, 201–210. [Google Scholar] [CrossRef] [Green Version]
- McGrath, T.M.; Waddington, G.; Scarvell, J.M.; Ball, N.B.; Creer, R.; Woods, K.; Smith, D. The effect of limb dominance on lower limb functional performance: A systematic review. J. Sports Sci. 2016, 34, 289–302. [Google Scholar] [CrossRef]
- Bishop, C.; Turner, A.; Read, P. Effects of inter-limb asymmetries on physical and sports performance: A systematic review. J. Sports Sci. 2017, 36, 1135–1144. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Male (Mean ± SD) | Female (Mean ± SD) | Total (Mean ± SD) | |
|---|---|---|---|
| Number | 14 | 8 | 22 |
| Age (years) | 23.6 ± 2.9 | 22.8 ± 5.4 | 23.3 ± 3.9 |
| Mass (kg) | 78.4 ± 6.1 | 65.9 ± 7.3 | 73.8 ± 8.6 |
| Height (m) | 1.80 ± 0.1 | 1.71 ± 0.1 | 1.77 ± 0.1 |
| BMI (kg/m2) | 24.1 ± 1.5 | 22.6 ± 2.3 | 23.6 ± 1.9 |
| Limb length (cm) | N-Dom 100.9 ± 4.3 | N-Dom 97.3 ± 4.9 | N-Dom 99.6 ± 4.8 |
| Dom 100.9 ± 4.3 | Dom 97.3 ± 4.7 | Dom 99.6 ± 4.7 |
| Test | Session 1 (Mean ± SD) | Session 2 (Mean ± SD) | ANOVA (p < 0.05) | Cronbach’s Alpha (α) | ICC (95% CI) | CV | SEM | SRD |
|---|---|---|---|---|---|---|---|---|
| YBT (cs) | ||||||||
| Dom | 86.8 ± 4.7 | 87.4 ± 4.1 | 0.273 | 0.92 | 0.89 (0.86–0.92) | 5.05 | 1.46 | 4.03 |
| N-Dom | 85.8 ± 4.6 | 87.2 ± 3.5 | 0.081 | 0.80 | 0.71 (0.62–0.80) | 4.74 | 2.21 | 6.11 |
| LSI (%) | 99.0 ± 5.6 | 99.9 ± 4.6 | 0.393 | 0.70 | 0.62 (0.53–0.70) | 5.13 | 3.14 | 8.68 |
| SLCMJ (cm) | ||||||||
| Dom | 15.5 ± 4.3 | 15.8 ± 4.2 | 0.380 | 0.96 | 0.95 (0.93–0.96) | 26.92 | 0.94 | 2.60 |
| N-Dom | 15.5 ± 4.5 | 16.2 ± 4.1 | 0.078 | 0.95 | 0.93 (0.90–0.95) | 27.04 | 1.14 | 3.15 |
| LSI (%) | 101.3 ± 14.1 | 104.4 ± 12.5 | 0.164 | 0.83 | 0.76 (0.70–0.82) | 12.94 | 6.52 | 18.02 |
| SLH (cm) | ||||||||
| Dom | 139.6 ± 24.2 | 143.5 ± 23.3 | 0.071 | 0.96 | 0.93 (0.91–0.95) | 16.68 | 6.24 | 17.24 |
| N-Dom | 134.0 ± 25.0 | 139.4 ± 23.8 | 0.015 * | 0.96 | 0.93 (0.90–0.95) | 17.78 | 6.45 | 17.83 |
| LSI (%) | 95.9 ± 6.7 | 97.2 ± 6.9 | 0.289 | 0.80 | 0.73 (0.66–0.80) | 7.04 | 3.53 | 9.76 |
| SH (no.) | ||||||||
| Dom | 54.7 ± 15.2 | 57.3 ± 13.0 | 0.116 | 0.94 | 0.90 (0.85–0.92) | 25.00 | 4.46 | 12.33 |
| N-Dom | 54.9 ± 11.0 | 58.0 ± 11.6 | 0.007 * | 0.95 | 0.92 (0.90–0.94) | 19.87 | 3.19 | 8.82 |
| LSI (%) | 108.6 ± 45.3 | 102.3 ± 9.8 | 0.447 | 0.50 | 0.41 (0.31–0.50) | 30.90 | 25.04 | 69.20 |
| SJ (s) | ||||||||
| Dom | 7.9 ± 1.7 | 7.7 ± 2.1 | 0.180 | 0.98 | 0.97 (0.96–0.98) | 24.36 | 0.33 | 0.91 |
| N-Dom | 8.3 ± 2.8 | 7.8 ± 2.4 | 0.011 * | 0.98 | 0.96 (0.95–0.97) | 32.50 | 0.52 | 1.44 |
| LSI (%) | 103.4 ± 13.8 | 100.7 ± 8.3 | 0.246 | 0.74 | 0.67 (0.60–0.73) | 11.17 | 6.54 | 18.07 |
| AT (s) | 11.6 ± 1.2 | 11.7 ± 1.0 | 0.528 | 0.96 | 0.95 (0.93–0.96) | 9.40 | 0.25 | 0.69 |
| LEFT (s) | 110.8 ± 11.4 | 107.7 ± 10.3 | 0.009 * | 0.94 | 0.90 (0.86–0.92) | 9.97 | 3.45 | 9.53 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scinicarelli, G.; Trofenik, M.; Froböse, I.; Wilke, C. The Reliability of Common Functional Performance Tests within an Experimental Test Battery for the Lower Extremities. Sports 2021, 9, 100. https://doi.org/10.3390/sports9070100
Scinicarelli G, Trofenik M, Froböse I, Wilke C. The Reliability of Common Functional Performance Tests within an Experimental Test Battery for the Lower Extremities. Sports. 2021; 9(7):100. https://doi.org/10.3390/sports9070100
Chicago/Turabian StyleScinicarelli, Giordano, Marko Trofenik, Ingo Froböse, and Christiane Wilke. 2021. "The Reliability of Common Functional Performance Tests within an Experimental Test Battery for the Lower Extremities" Sports 9, no. 7: 100. https://doi.org/10.3390/sports9070100
APA StyleScinicarelli, G., Trofenik, M., Froböse, I., & Wilke, C. (2021). The Reliability of Common Functional Performance Tests within an Experimental Test Battery for the Lower Extremities. Sports, 9(7), 100. https://doi.org/10.3390/sports9070100